
Atypical Clinical Presentation of Laryngopharyngeal Reflux: A 5-Year Case Series

 ,
, 
 ,
,  and
and
Abstract
1. Introduction
2. Methods
2.1. Design, Data Collection, and Setting
2.2. 24 h HEMII-pH
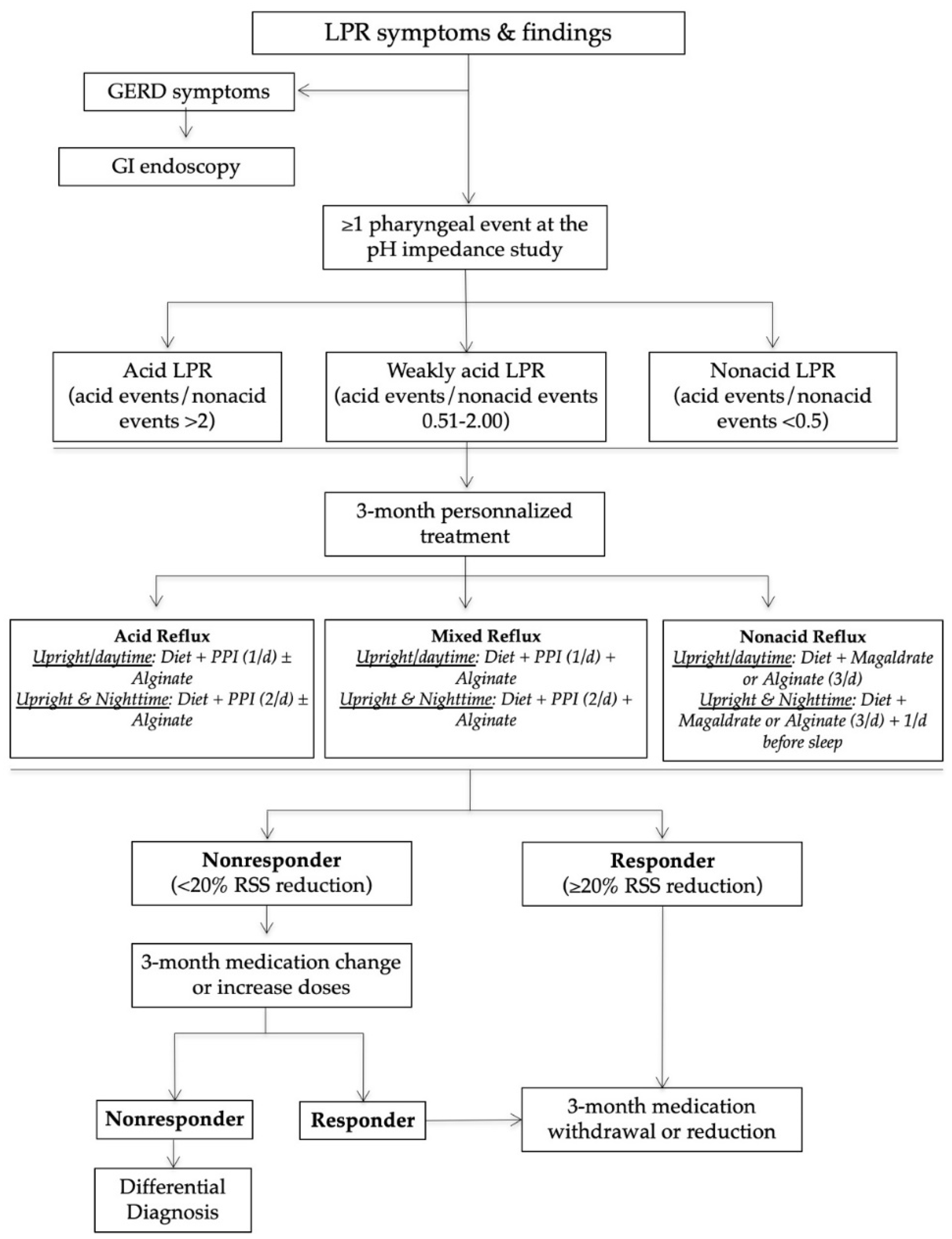
2.3. Finding Evolution, Treatment, and Management of Atypical Clinical Presentations
3. Results
3.1. Oral Atypical Manifestations
3.2. Otological and Nasal Atypical Manifestations
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lechien, J.R.; Akst, L.M.; Hamdan, A.L.; Schindler, A.; Karkos, P.D.; Barillari, M.R.; Calvo-Henriquez, C.; Crevier-Buchman, L.; Finck, C.; Eun, Y.G.; et al. Evaluation and Management of Laryngopharyngeal Reflux Disease: State of the Art Review. Otolaryngol. Head Neck Surg. 2019, 160, 762–782. [Google Scholar] [CrossRef]
- Klimara, M.J.; Randall, D.R.; Allen, J.; Figueredo, E.; Johnston, N. Proximal reflux: Biochemical mediators, markers, therapeutic targets, and clinical correlations. Ann. N. Y. Acad. Sci. 2020, 1481, 127–138. [Google Scholar] [CrossRef] [PubMed]
- Samuels, T.L.; Johnston, N. Pepsin as a marker of extraesophageal reflux. Ann. Otol. Rhinol. Laryngol. 2010, 119, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Ren, J.J.; Zhao, Y.; Wang, J.; Ren, X.; Xu, Y.; Tang, W.; He, Z. PepsinA as a Marker of Laryngopharyngeal Reflux Detected in Chronic Rhinosinusitis Patients. Otolaryngol. Head Neck Surg. 2017, 156, 893–900. [Google Scholar] [CrossRef]
- Pawar, S.; Lim, H.J.; Gill, M.; Smith, T.L.; Merati, A.; Toohill, R.J.; Loehrl, T.A. Treatment of postnasal drip with proton pump inhibitors: A prospective, randomized, placebo-controlled study. Am. J. Rhinol. 2007, 21, 695–701. [Google Scholar] [CrossRef]
- Lechien, J.R.; Hans, S.; Simon, F.; Horoi, M.; Calvo-Henriquez, C.; Chiesa-Estomba, C.M.; Mayo-Yáñez, M.; Bartel, R.; Piersiala, K.; Nguyen, Y.; et al. Association between Laryngopharyngeal Reflux and Media Otitis: A Systematic Review. Otol. Neurotol. 2021. [Google Scholar] [CrossRef]
- Lechien, J.R.; Akst, L.M.; Saussez, S.; Crevier-Buchman, L.; Hans, S.; Barillari, M.R.; Calvo-Henriquez, C.; Bock, J.M.; Carroll, T.L. Involvement of Laryngopharyngeal Reflux in Select Nonfunctional Laryngeal Diseases: A Systematic Review. Otolaryngol. Head Neck Surg. 2020, 194599820933209. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J.P.; Parikh, S.; Orlando, R.C.; Johnston, N.; Allen, J.; Tinling, S.P.; Belafsky, P.; Arevalo, L.F.; Sharma, N.; Castell, D.O.; et al. Review article: Reflux and its consequences—The laryngeal, pulmonary and oesophageal manifestations. In Proceedings of the 9th International Symposium on Human Pepsin (ISHP), Kingston-upon-Hull, UK, 21–23 April 2010. [Google Scholar]
- Lechien, J.R.; Bobin, F.; Muls, V.; Saussez, S.; Remacle, M.; Hans, S. Reflux clinic: Proof-of-concept of a Multidisciplinary European Clinic. Eur. Arch. Otorhinolaryngol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Bobin, F.; Muls, V.; Mouawad, F.; Dequanter, D.; Horoi, M.; Thill, M.P.; Rodriguez Ruiz, A.; Saussez, S. The efficacy of a personalised treatment depending on the characteristics of reflux at multichannel intraluminal impedance-pH monitoring in patients with acid, non-acid and mixed laryngopharyngeal reflux. Clin. Otolaryngol. 2021, 46, 602–613. [Google Scholar] [CrossRef]
- Lechien, J.R.; Rodriguez Ruiz, A.; Dequanter, D.; Bobin, F.; Mouawad, F.; Muls, V.; Huet, K.; Harmegnies, B.; Remacle, S.; Finck, C.; et al. Validity and Reliability of the Reflux Sign Assessment. Ann. Otol. Rhinol. Laryngol. 2020, 129, 313–325. [Google Scholar] [CrossRef]
- Lechien, J.R.; Saussez, S.; Schindler, A.; Karkos, P.D.; Hamdan, A.L.; Harmegnies, B.; De Marrez, L.G.; Finck, C.; Journe, F.; Paesmans, M.; et al. Clinical outcomes of laryngopharyngeal reflux treatment: A systematic review and meta-analysis. Laryngoscope 2019, 129, 1174–1187. [Google Scholar] [CrossRef]
- Hoppo, T.; Sanz, A.F.; Nason, K.S.; Carroll, T.L.; Rosen, C.; Normolle, D.P.; Shaheen, N.J.; Luketich, J.D.; Jobe, B.A. How much pharyngeal exposure is “normal”? Normative data for laryngopharyngeal reflux events using hypopharyngeal multichannel intraluminal impedance (HMII). J. Gastrointest. Surg. 2012, 16, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Bobin, F.; Muls, V.; Horoi, M.; Thill, M.P.; Dequanter, D.; Rodriguez, A.; Saussez, S. Patients with acid, high-fat and low-protein diet have higher laryngopharyngeal reflux episodes at the impedance-pH monitoring. Eur. Arch. Otorhinolaryngol. 2020, 277, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Allen, J.E.; Barillari, M.R.; Karkos, P.D.; Jia, H.; Ceccon, F.P.; Imamura, R.; Metwaly, O.; Chiesa-Estomba, C.M.; Bock, J.M.; et al. Management of Laryngopharyngeal Reflux Around the World: An International Study. Laryngoscope 2020. [Google Scholar] [CrossRef]
- Howden, G.F. Erosion as the presenting symptom in hiatus hernia. A case report. Br. Dent. J. 1971, 131, 455–456. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Chiesa-Estomba, C.M.; Calvo Henriquez, C.; Mouawad, F.; Ristagno, C.; Barillari, M.R.; Schindler, A.; Nacci, A.; Bouland, C.; Laino, L.; et al. Laryngopharyngeal reflux, gastroesophageal reflux and dental disorders: A systematic review. PLoS ONE 2020, 15, e0237581. [Google Scholar] [CrossRef]
- Preetha, A.; Sujatha, D.; Patil, B.A.; Hegde, S. Oral manifestations in gastroesophageal reflux disease. Gen. Dent. 2015, 63, e27–e31. [Google Scholar]
- Hakeem, A.; Fitzpatrick, S.G.; Bhattacharyya, I.; Islam, M.N.; Cohen, D.M. Clinical characterization and treatment outcome of patients with burning mouth syndrome. Gen. Dent. 2018, 66, 41–47. [Google Scholar]
- Cheung, D.; Trudgill, N. Managing a patient with burning mouth syndrome. Frontline Gastroenterol. 2015, 6, 218–222. [Google Scholar] [CrossRef]
- Lechien, J.R.; Hans, S.; De Marrez, L.G.; Dequanter, D.; Rodriguez, A.; Muls, V.; Ben Abdelouahed, F.; Evrard, L.; Maniaci, A.; Saussez, S.; et al. Prevalence and Features of Laryngopharyngeal Reflux in Patients with Primary Burning Mouth Syndrome. Laryngoscope 2021. [Google Scholar] [CrossRef]
- Brunworth, J.D.; Mahboubi, H.; Garg, R.; Johnson, B.; Brandon, B.; Djalilian, H.R. Nasopharyngeal acid reflux and Eustachian tube dysfunction in adults. Ann. Otol. Rhinol. Laryngol. 2014, 123, 415–419. [Google Scholar] [CrossRef]
- Brunworth, J.D.; Garg, R.; Mahboubi, H.; Johnson, B.; Djalilian, H.R. Detecting nasopharyngeal reflux: A novel pH probe technique. Ann. Otol. Rhinol. Laryngol. 2012, 121, 427–430. [Google Scholar] [CrossRef]
- Lechien, J.R.; Bobin, F.; Dapri, G.; Eisendrath, P.; Salem, C.; Mouawad, F.; Horoi, M.; Thill, M.P.; Dequanter, D.; Rodriguez, A.; et al. Hypopharyngeal-Esophageal Impedance-pH Monitoring Profiles of Laryngopharyngeal Reflux Patients. Laryngoscope 2021, 131, 268–276. [Google Scholar] [CrossRef] [PubMed]
- Lei, L.; Yu, Z.; Yu, R.; Yang, H.; Zou, J.; Ren, J.; Zhang, J.; Zhong, D. Correlation of pathogenic effects of laryngopharyngeal reflux and bacterial infection in COME of children. Acta Otolaryngol. 2021, 1–5. [Google Scholar] [CrossRef]
- O’Reilly, R.C.; Soundar, S.; Tonb, D.; Bolling, L.; Yoo, E.; Nadal, T.; Grindle, C.; Field, E.; He, Z. The role of gastric pepsin in the inflammatory cascade of pediatric otitis media. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 350–357. [Google Scholar] [CrossRef]
- Hamizan, A.W.; Choo, Y.Y.; Loh, P.V.; Abd Talib, N.F.; Mohd Ramli, M.F.; Zahedi, F.D.; Husain, S. The association between the reflux symptoms index and nasal symptoms among patients with non-allergic rhinitis. J. Laryngol. Otol. 2021, 135, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, S.M.; Kanmaz, M.A.; Disikirik, I.; Karadeniz, P.G. Peak nasal inspiratory airflow measurements for assessing laryngopharyngeal reflux treatment. Clin. Otolaryngol. 2021. [Google Scholar] [CrossRef]
- Magliulo, G.; Pace, A.; Plateroti, R.; Plateroti, A.M.; Cascella, R.; Solito, C.; Rossetti, V.; Iannella, G. Laryngopharyngeal reflux disease in adult patients: Tears and pepsin. J. Biol. Regul. Homeost. Agents 2020, 34, 715–720. [Google Scholar] [CrossRef]
- Samuels, T.L.; Johnston, N. Pepsin in gastroesophageal and extraesophageal reflux: Molecular pathophysiology and diagnostic utility. Curr. Opin. Otolaryngol. Head Neck Surg. 2020, 28, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Lechien, J.R.; Saussez, S.; Harmegnies, B.; Finck, C.; Burns, J.A. Laryngopharyngeal Reflux and Voice Disorders: A Multifactorial Model of Etiology and Pathophysiology. J. Voice 2017, 31, 733–752. [Google Scholar] [CrossRef]
- Blumin, J.H.; Johnston, N. Evidence of extraesophageal reflux in idiopathic subglottic stenosis. Laryngoscope 2011, 121, 1266–1273. [Google Scholar] [CrossRef]
- Lechien, J.R.; De Vos, N.; Everard, A.; Saussez, S. Laryngopharyngeal reflux: The microbiota theory. Med. Hypotheses 2021, 146, 110460. [Google Scholar] [CrossRef] [PubMed]
- Biagi, E.; Candela, M.; Turroni, S.; Garagnani, P.; Franceschi, C.; Brigidi, P. Ageing and gut microbes: Perspectives for health maintenance and longevity. Pharmacol. Res. 2013, 69, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Motta, J.P.; Wallace, J.L.; Buret, A.G.; Deraison, C.; Vergnolle, N. Gastrointestinal biofilms in health and disease. Nat. Rev. Gastroenterol. Hepatol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Hillel, A.T.; Tang, S.S.; Carlos, C.; Skarlupka, J.H.; Gowda, M.; Yin, L.X.; Motz, K.; Currie, C.R.; Suen, G.; Thibeault, S.L. Laryngotracheal Microbiota in Adult Laryngotracheal Stenosis. mSphere 2019, 4, e00211–e00219. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.H.F.; Teo, S.M.; Sly, P.D.; Holt, P.G.; Inouye, M. The intersect of genetics, environment, and microbiota in asthma-perspectives and challenges. J. Allergy Clin. Immunol. 2021, 147, 781–793. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| PN | G | Age | Baseline Features | Post-Treatment Features | ||||
|---|---|---|---|---|---|---|---|---|
| Atypical Presentation | HEMII-pH/RSS | Treatment | RSS/RSA | Presentation Evolution | Long-Term Follow-Up | |||
| 1 | M | 36 | Recurrent aphthosis and burning mouth | Upright acid reflux (58) * | Strict diet | RSS: 13 | Resolution of aphthosis and | Long-term diet |
| Dental check-up: normal | GI: normal | PPIs | RSA: 10 | burning mouth | No recurrence (3-y) | |||
| RSS: 48–RSA: 26 | Magaldrate | |||||||
| 2 | F | 55 | Recurrent aphthosis and burning mouth | Upright acid reflux (22) * | Strict diet | RSS: 5 | Resolution of aphthosis and | Long-term diet |
| Dental check-up: normal | GI: not performed | PPIs | RSA: NP | burning mouth | No recurrence (6-m) | |||
| RSS: 50–RSA: 26 | Alginate | |||||||
| 3 | M | 31 | Mouth burning and severe anorexia | Upright nonacid reflux (11) | Histamine-free | RSS: 64 | Resolution of pain and | Long-term histamine-free |
| GI/dental check-up: normal | GI: normal | Diet | RSA: NP | weight gain | diet. | |||
| Nutritionist: Histamine intolerance | RSS: 148–RSA: 14 | No recurrence (1-y) | ||||||
| 4 | M | 38 | Tongue burning | Upright weakly acid reflux (15) | Strict diet | RSS: 16 | Resolution of tongue | Long-term diet |
| Dental check-up: normal | GI: normal | PPIs | RSA: 23 | burning | No recurrence (1-y) | |||
| RSS: 131–RSA: 37 | Alginate | |||||||
| 5 | M | 55 | Tongue burning | Upright acid reflux (27) | Strict diet | RSS: 48 | Reduction of tongue | Long-term diet |
| Dental check-up: normal | GI: GERD, hiatal hernia | PPIs | RSA: 21 | burning | Long-term PPIs and | |||
| RSS: 76–RSA: 24 | Magaldrate | Magaldrate (1-y) | ||||||
| 6 | F | 53 | Tongue burning and fissured tongue | Upright acid reflux (19) | Strict diet | RSS: 135 | Reduction of tongue | Long-term diet |
| Dental check-up: normal | GI: GERD, esophagitis | PPIs | RSA: 22 | Burning but no change | Long-term intermittent | |||
| RSS: 247–RSA: 28 | Magaldrate | in fissured tongue | Magaldrate (9-m) | |||||
| 7 | F | 54 | Tongue and mouth burning | Upright acid reflux (38) * | Strict diet | RSS: 19 | Resolution of tongue | Long-term diet |
| Dental check-up: normal | GI: GERD | PPIs | RSA: 13 | burning | No recurrence (3-y) | |||
| RSS: 88–RSA: 26 | Magaldrate | |||||||
| 8 | F | 62 | Tongue and mouth burning | Upright acid reflux | Strict diet | RSS: 19 | Resolution of tongue | Long-term diet |
| Dental check-up: normal | GI: GERD, esophagitis | PPIs | RSA: 32 | burning | One recurrence controlled | |||
| RSS: 203–RSA: 22 | Alginate | with alginate (3-y) | ||||||
| 9 | F | 64 | Tongue and mouth burning | Upright acid reflux (7) | Strict alkaline | RSS: 12 | Resolution of tongue | Long-term diet |
| Dental check-up: normal | GI: normal | Diet | RSA: NP | burning | No recurrence (6-m) | |||
| RSS: 124–RSA: 32 | ||||||||
| 10 | F | 31 | Recurrent burps and abdominal pain | Upright acid reflux (18) | Gluten-free | RSS: 40 | Resolution of burps and | Long-term gluten-free |
| GI check-up: gluten intolerance | GI: bulbitis | Diet | RSA: 17 | Abdominal pain | diet. | |||
| RSS: 167–RSA: 20 | No recurrence (4-y) | |||||||
| 11 | F | 36 | Recurrent burps and abdominal pain | Upright nonacid reflux (2) | Lactose-free | RSS: 16 | Resolution of burps and | Long-term lactosis-free |
| GI check-up: lactose intolerance | GI: normal | Diet | RSA: 21 | Abdominal pain | diet. | |||
| RSS: 111–RSA: 31 | No recurrence (4-y) | |||||||
| PN | G | Age | Baseline Features | Post-Treatment Features | ||||
|---|---|---|---|---|---|---|---|---|
| Atypical Presentation | HEMII-pH/RSS | Treatment | RSS/RSA | Presentation Evolution | Long-Term Follow-Up | |||
| 12 | F | 64 | Resistant chronic nasal obstruction # | Upright weakly acid reflux (12) | Strict diet | RSS: 67 | Resolution of nasal | Long-term diet |
| Nasosinusal check-up: hypertrophy of | GI: normal | PPIs | RSA: NP | obstruction | No recurrence (6 months) | |||
| the posterior part of the inferior turbine | RSS: 250–RSA: 29 | Alginate | ||||||
| 13 | F | 50 | Resistant chronic nasal obstruction # | Upright acid reflux (24) | Strict diet | RSS: 43 | Resolution of nasal | Long-term diet |
| Nasosinusal check-up: hypertrophy of | GI: not performed | PPIs | RSA: NP | obstruction | No recurrence (6 months) | |||
| the posterior part of the inferior turbine | RSS: 58–RSA: 12 | Alginate | Septoplasty not required | |||||
| 14 | F | 66 | Resistant chronic nasal obstruction | Upright weakly acid reflux (9) * | Strict alkaline | RSS: 184 | Resolution of nasal | Long-term diet and alginate |
| and tearing | GI: not performed | Diet | RSA: NP | obstruction and tearing | No recurrence (6-m) of | |||
| Nasosinusal check-up: hypertrophy of | RSS: 210–RSA: 32 | Resolution of edema of | tear and nasal symptoms | |||||
| the posterior part of the inferior turbine | inferior and middle meatus | Chronic throat symptoms | ||||||
| 15 | F | 35 | Recurrent suppurative media otitis and | Upright acid reflux (4) * | Strict alkaline | RSS: 2 | Resolution of media | Long-term diet |
| Ear pressure and pain | GI: not performed | Diet | RSA: 7 | otitis | No recurrence (1-y) of | |||
| Nasosinusal check-up: normal | RSS: 11–RSA: 20 | symptoms or tympanic | ||||||
| Otological check-up: retraction pocket | membrane findings. | |||||||
| 16 | M | 37 | Chronic media otitis | Upright acid reflux (3) | Strict alkaline | RSS: 48 | Improvement of nasal | Long-term diet and short |
| Nasosinusal check-up: obstruction and | GI: not performed | Diet | RSA: NP | obstruction | period of alginate | |||
| erythema of the Eustachian tube. ** | RSS: 73–RSA: 36 | No recurrence (1-y) | ||||||
| 17 | M | 36 | Recurrent rhinopharyngitis/otitis | Upright weakly acid reflux (11) | Strict diet | RSS: 52 | Resolution of rhino- | Long-term diet |
| Otological check-up: normal | GI: not performed | PPIs | RSA: 20 | pharyngitis posttreatment | No recurrence (6 months) | |||
| Nasal check-up: controlled dust allergy | RSS: 107–RSA: 29 | Alginate | ||||||
| PN | G | Age | Baseline Features | Post-Treatment Features | ||||
|---|---|---|---|---|---|---|---|---|
| Atypical Presentation | HEMII-pH/RSS | Treatment | RSS/RSA | Presentation Evolution | Long-Term Follow-Up | |||
| 18 | F | 34 | Severe idiopathic vocal fold dysplasia | Upright acid reflux (11) | Strict alkaline | RSS: 9 | Resolution of dysplasia | Long-term diet |
| Laryngeal check-up: normal | GI: not performed | Alginate | RSA: 20 | within 6 months | No recurrence (6 months) | |||
| No tobacco/toxic exposition history | RSS: 34–RSA: 39 | Diet | ||||||
| 19 | M | 45 | Severe idiopathic vocal fold dysplasia | Upright acid reflux (22) | Strict alkaline | RSS: 16 | Resolution of dysplasia | Long-term diet |
| Laryngeal check-up: normal | GI: not performed | Diet | RSA: 18 | within 6 months | No recurrence (9 months) | |||
| No tobacco/toxic exposition history | RSS: 73–RSA: 23 | |||||||
| 20 | M | 38 | Daily aspirations and pneumonia | Upright acid reflux (39) * | Strict alkaline | RSS: 81 | Resolution of dysplasia | Long-term diet |
| Lung/swallowing check-up: normal | GI: esophagitis | Diet | RSA: 18 | within 6 months | No recurrence (6 months) | |||
| RSS: 156–RSA: 27 | Alginate | |||||||
| 21 | F | 65 | Recurrent tracheobronchitis | Upright weakly acid reflux (34) * | Strict diet | RSS: 110 | Resolution of tracheo- | Long-term diet |
| Lung check-up: normal | GI: LES insufficiency | Magaldrate | RSA: 19 | bronchitis within 6 months | Magaldrate (sometimes) | |||
| No tobacco/asthma history | RSS: 415–RSA: 24 | No recurrence (6 months) | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lechien, J.R.; Hans, S.; Bobin, F.; Calvo-Henriquez, C.; Saussez, S.; Karkos, P.D. Atypical Clinical Presentation of Laryngopharyngeal Reflux: A 5-Year Case Series. J. Clin. Med. 2021, 10, 2439. https://doi.org/10.3390/jcm10112439
Lechien JR, Hans S, Bobin F, Calvo-Henriquez C, Saussez S, Karkos PD. Atypical Clinical Presentation of Laryngopharyngeal Reflux: A 5-Year Case Series. Journal of Clinical Medicine. 2021; 10(11):2439. https://doi.org/10.3390/jcm10112439
Chicago/Turabian StyleLechien, Jerome R., Stéphane Hans, Francois Bobin, Christian Calvo-Henriquez, Sven Saussez, and Petros D. Karkos. 2021. "Atypical Clinical Presentation of Laryngopharyngeal Reflux: A 5-Year Case Series" Journal of Clinical Medicine 10, no. 11: 2439. https://doi.org/10.3390/jcm10112439
APA StyleLechien, J. R., Hans, S., Bobin, F., Calvo-Henriquez, C., Saussez, S., & Karkos, P. D. (2021). Atypical Clinical Presentation of Laryngopharyngeal Reflux: A 5-Year Case Series. Journal of Clinical Medicine, 10(11), 2439. https://doi.org/10.3390/jcm10112439