
The Direct Anterior Approach to Primary Total Hip Replacement: Radiological Analysis in Comparison to Other Approaches

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
Assessment of Methodological Quality
3. Results
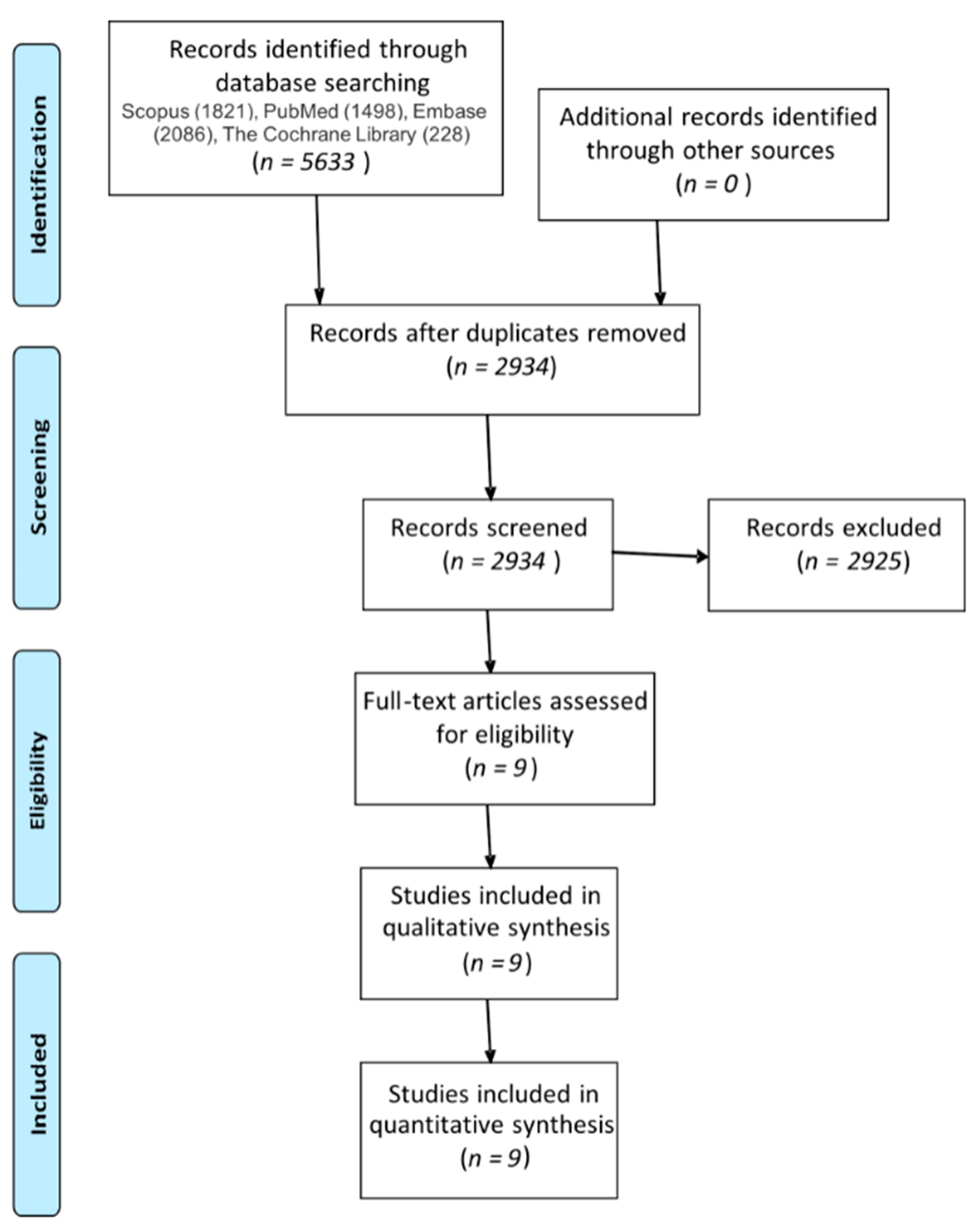
3.1. Literature Selection
3.1.1. Study Characteristics
3.1.2. Participants
3.1.3. Risk of Bias within Studies
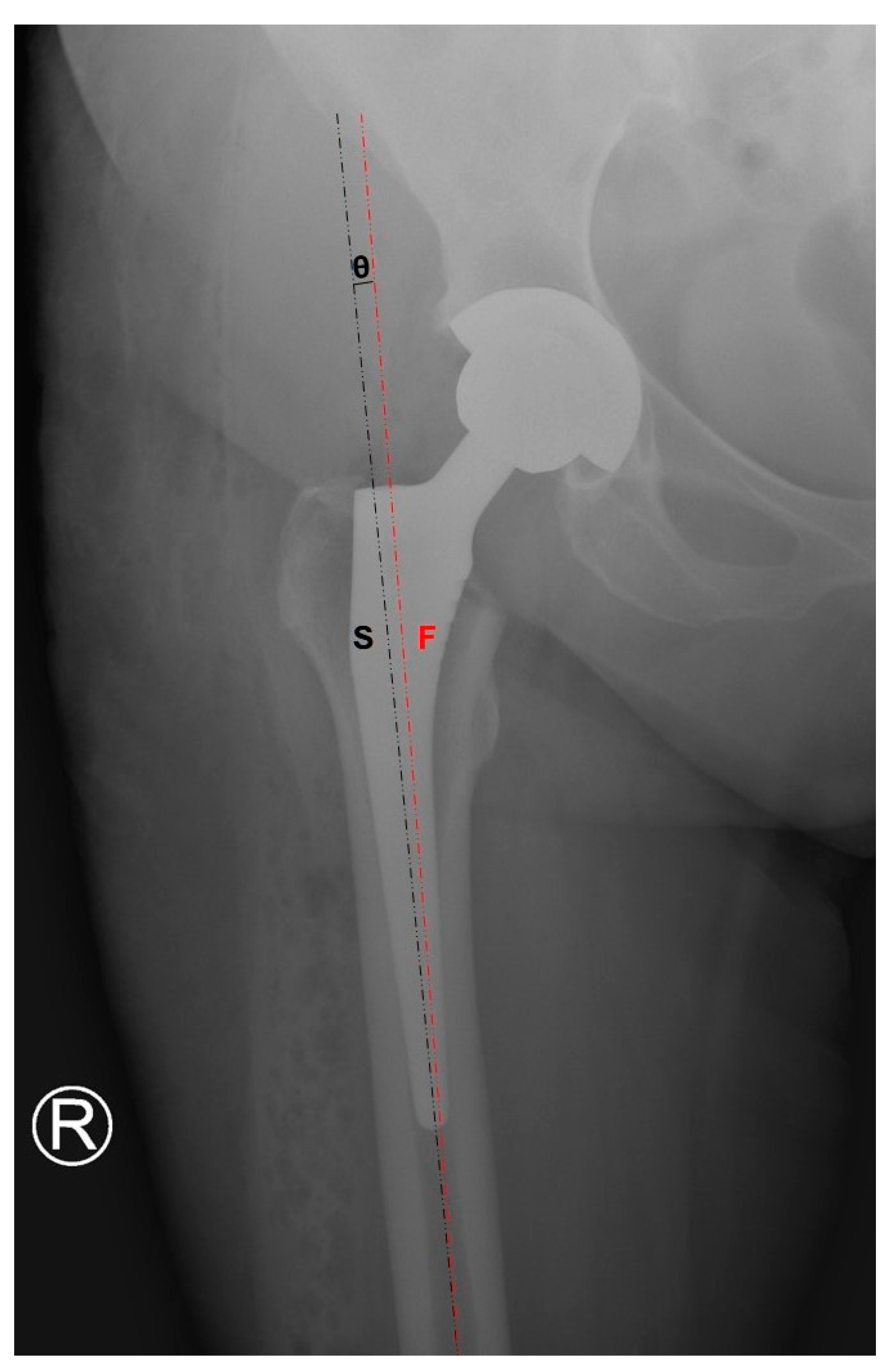
3.2. Femoral Stem Alignment
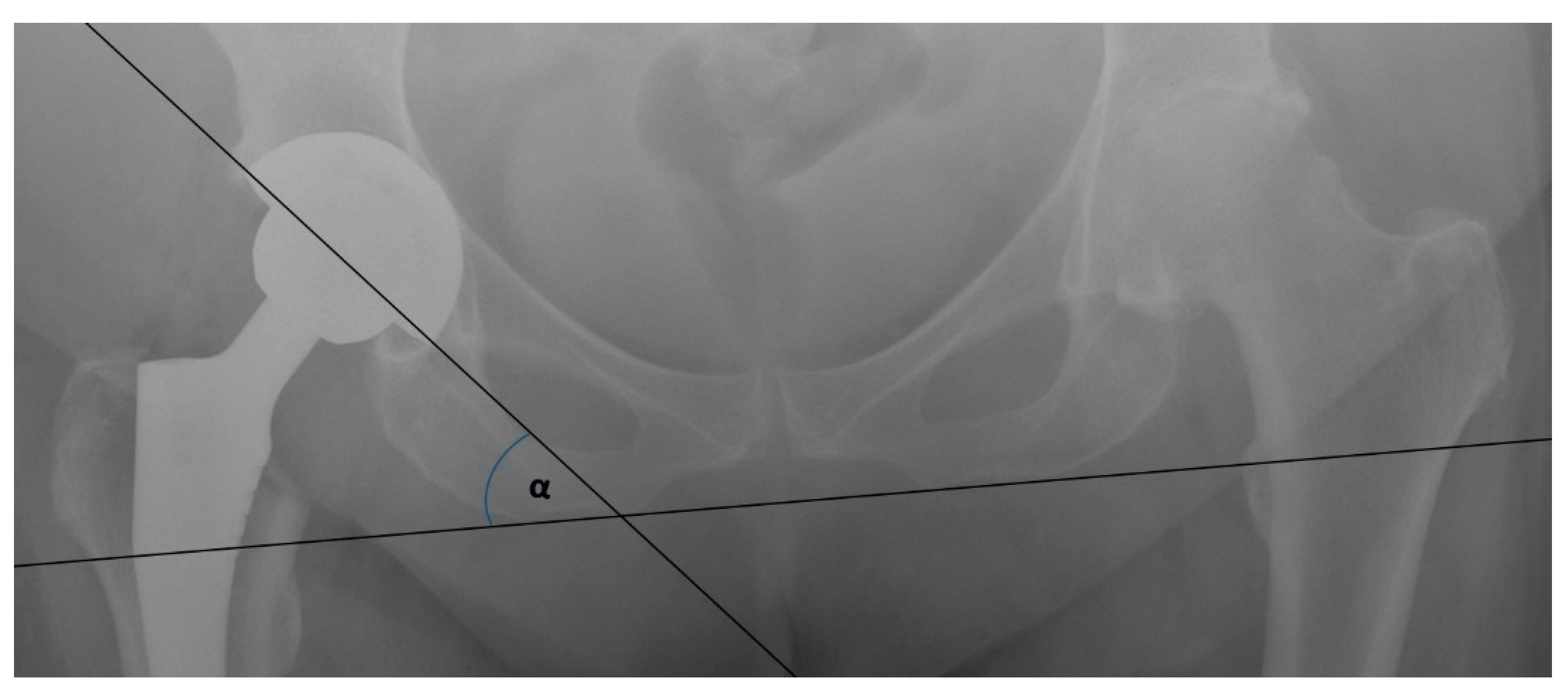
3.3. Mean Radiographic Cup Inclination
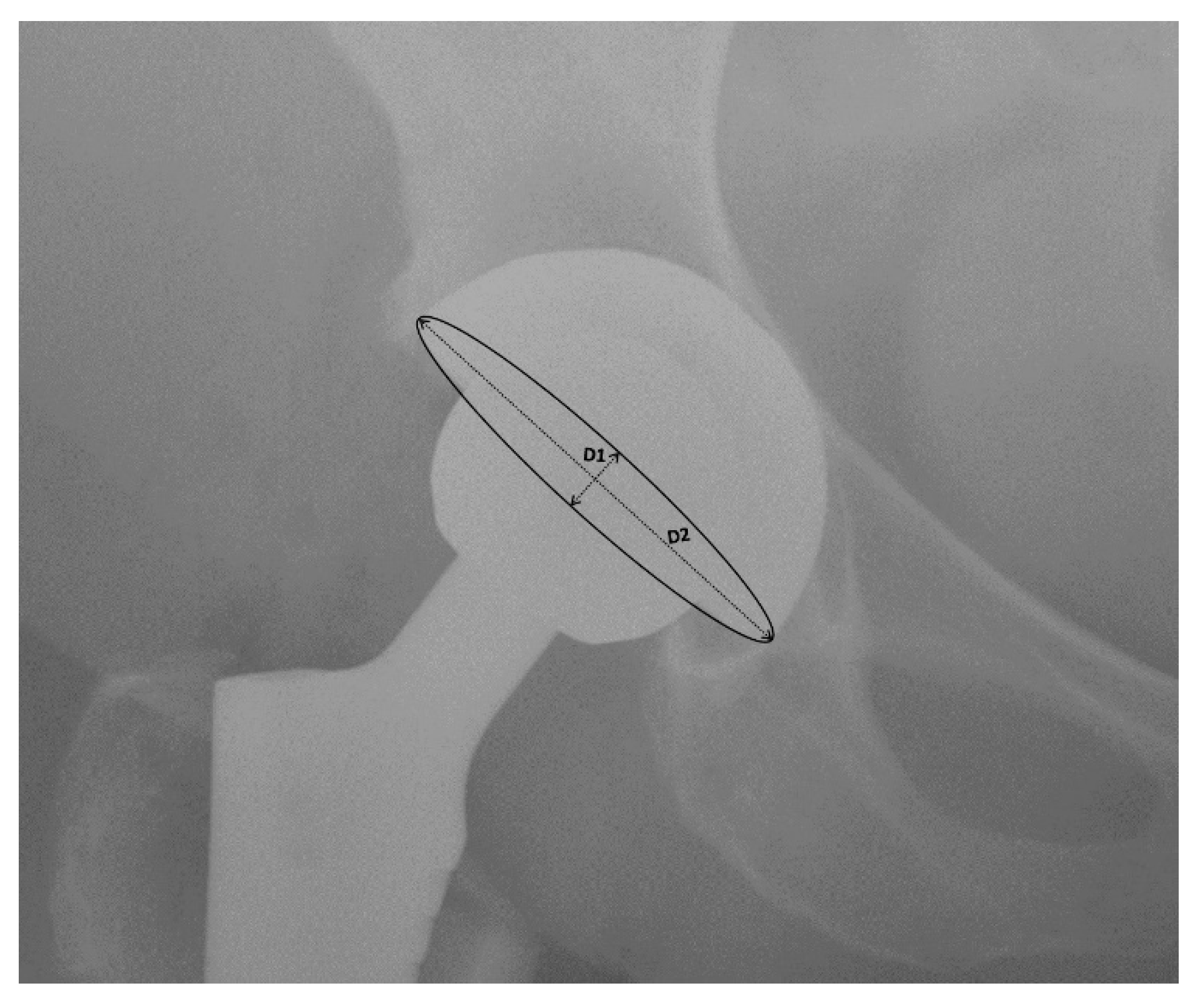
3.4. Mean Radiographic Cup Anteversion
3.5. Leg Length
3.6. DAA vs. LA
3.7. DAA vs. PA
3.8. DAA vs. PLA
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Learmonth, I.D.; Young, C.; Rorabeck, C. The operation of the century: Total hip replacement. Lancet 2007, 370, 1508–1519. [Google Scholar] [CrossRef]
- Chechik, O.; Khashan, M.; Lador, R.; Salai, M.; Amar, E. Surgical approach and prosthesis fixation in hip arthroplasty world wide. Arch. Orthop. Trauma Surg. 2013, 133, 1595–1600. [Google Scholar] [CrossRef]
- Kwon, M.S.; Kuskowski, M.; Mulhall, K.J.; Macaulay, W.E.; Brown, T.; Saleh, K.J. Does Surgical Approach Affect Total Hip Arthroplasty Dislocation Rates? Clin. Orthop. Relat. Res. 2006, 447, 34–38. [Google Scholar] [CrossRef]
- Kucukdurmaz, F.; Sukeik, M.; Parvizi, J. A meta-analysis comparing the direct anterior with other approaches in primary total hip arthroplasty. Surgeon 2019, 17, 291–299. [Google Scholar] [CrossRef]
- Ilchmann, T. Approaches for primary total hip replacement. Hip Int. 2014, 24, S2–S6. [Google Scholar] [CrossRef]
- Graves, S.C.; Dropkin, B.M.; Keeney, B.J.; Lurie, J.D.; Tomek, I.M. Does Surgical Approach Affect Patient-reported Function After Primary THA? Clin. Orthop. Relat. Res. 2016, 474, 971–981. [Google Scholar] [CrossRef]
- Smith-Petersen, M.N. A new supra-articular subperiosteal approach to the hip joint. J. Bone Joint Surg. Am. 1917, 2, 592–595. [Google Scholar]
- Nistor, D.V.; Caterev, S.; Bolboacă, S.D.; Cosma, D.; Lucaciu, D.O.G.; Todor, A. Transitioning to the direct anterior approach in total hip arthroplasty. Is it a true muscle sparing approach when performed by a low volume hip replacement surgeon? Int. Orthop. 2017, 41, 2245–2252. [Google Scholar] [CrossRef]
- Post, Z.D.; Orozco, F.; Diaz-Ledezma, C.; Hozack, W.J.; Ong, A. Direct anterior approach for total hip arthroplasty: Indications; technique; and results. J. Am. Acad. Orthop. Surg. 2014, 22, 595–603. [Google Scholar] [CrossRef]
- Jelsma, J.; Pijnenburg, R.; Boons, H.W.; Eggen, P.J.; Kleijn, L.L.; Lacroix, H.; Noten, H.J. Limited benefits of the direct anterior approach in primary hip arthroplasty: A prospective single centre cohort study. J. Orthop. 2017, 14, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Kyriakopoulos, G.; Poultsides, L.; Christofilopoulos, P. Total hip arthroplasty through an anterior approach. EFORT Open Rev. 2018, 3, 574–583. [Google Scholar] [CrossRef]
- Wang, Z.; Hou, J.-Z.; Wu, C.-H.; Zhou, Y.-J.; Gu, X.-M.; Wang, H.-H.; Feng, W.; Cheng, Y.-X.; Sheng, X.; Bao, H.-W. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total hip arthroplasty. J. Orthop. Surg. Res. 2018, 13. [Google Scholar] [CrossRef]
- Connolly, K.P.; Kamath, A.F. Direct anterior total hip arthroplasty: Comparative outcomes and contemporary results. World J. Orthop. 2016, 7, 94. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, J.A.; Deshmukh, A.J.; Rathod, P.A. Does the direct anterior approach in THA offer faster rehabilitation and com-parable safety to the posterior approach? Clin. Orthop. Relat. Res. 2014, 472, 455–463. [Google Scholar] [CrossRef]
- Lewinnek, G.E.; Lewis, J.L.; Tarr, R.; Compere, C.L.; Zimmerman, J.R. Dislocations after total hip replacement arthroplasties. J. Bone Jt. Surg. Am. 1978, 60, 217–220. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.0 (updated July 2019). Cochrane. 2019. Available online: www.training.cochrane.org/handbook (accessed on 8 February 2021).
- Yue, C.; Kang, P.; Pei, F. Comparison of Direct Anterior and Lateral Approaches in Total Hip Arthroplasty: A Systematic Review and Meta-Analysis (PRISMA). Medicine 2015, 94, e2126. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. Cochrane Bias Methods Group, Cochrane Statistical Methods Group The cochrane collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Reichert, J.C.; Von Rottkay, E.; Roth, F.; Renz, T.; Hausmann, J.; Kranz, J.; Rackwitz, L.; Nöth, U.; Rudert, M. A prospective randomized comparison of the minimally invasive direct anterior and the transgluteal approach for primary total hip arthroplasty. BMC Musculoskelet. Disord. 2018, 19, 241. [Google Scholar] [CrossRef]
- Dienstknecht, T.; Luring, C.; Tingart, M.; Grifka, J.; Sendtner, E. Total hip arthroplasty through the mini-incision (mi-cro-hip) approach versus the standard transgluteal (Bauer) approach: A prospective; randomised study. J. Orthop. Surg. 2014, 22, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.E.; Wallis, J.A.; Taylor, N.F.; Holden, C.T.; Marks, P.; Smith, C.L.; Armstrong, M.S.; Singh, P.J. A Prospective Randomized Clinical Trial in Total Hip Arthroplasty—Comparing Early Results Between the Direct Anterior Approach and the Posterior Approach. J. Arthroplast. 2017, 32, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Taunton, M.J.; Bohannon, M.J.; Odum, S.M.; Springer, B.D. Direct Anterior THA yields more rapid voluntary cessation of all walking aids: A Prospective; Randomized Clinical Trial. J. Arthroplast. 2014, 29, 169–172. [Google Scholar] [CrossRef]
- Barrett, W.P.; Turner, S.E.; Leopold, J.P. Prospective Randomized Study of Direct Anterior vs Postero-Lateral Approach for Total Hip Arthroplasty. J. Arthroplast. 2013, 28, 1634–1638. [Google Scholar] [CrossRef]
- Zhao, H.-Y.; Kang, P.-D.; Xia, Y.-Y.; Shi, X.-J.; Nie, Y.; Pei, F.-X. Comparison of early functional recovery following total hip ar-throplasty using a direct anterior or posterolateral approach: A randomized controlled trial. J. Arthroplast. 2017, 32, 3421–3428. [Google Scholar] [CrossRef]
- Taunton, M.J.; Trousdale, R.T.; Sierra, R.J.; Kaufman, K.P.; Pagnano, M.W. Randomized Clinical Trial of Anterior and Miniposterior Approach THA: Which Provides Better Functional Recovery? Clin. Orthop. Relat. Res. 2018, 476, 216–229. [Google Scholar] [CrossRef]
- Brun, O.C.L.; Sund, H.N.; Nordsletten, L.; Rohrl, S.M.; Mjaaland, K.E. Component Placement in Direct Lateral vs. Minimally In-vasive Anterior Approach in Total Hip Arthroplasty: Radiographic Outcomes from a Prospective Randomized Controlled Trial. J. Arthroplast. 2019, 34, 1718. [Google Scholar] [CrossRef]
- Harrison, C.L.; Thomson, A.I.; Cutts, S.; Rowe, P.J.; Riches, P.E. Research Synthesis of Recommended Acetabular Cup Orientations for Total Hip Arthroplasty. J. Arthroplast. 2014, 29, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Board, T.; Bhaskar, D.; Rajpura, A. Current concepts in acetabular positioning in total hip arthroplasty. Indian J. Orthop. 2017, 51, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Scheerlinck, T. Cup positioning in total hip arthroplasty. Acta Orthop. Belg. 2014, 80, 336–347. [Google Scholar] [PubMed]
- Reikerås, O.; Gunderson, R. Components anteversion in primary cementless THA using straight stem and hemispherical cup: A prospective study in 91 hips using CT-scan measurements. Orthop. Traumatol. Surg. Res. 2011, 97, 615–621. [Google Scholar] [CrossRef]
- Angadji, A.; Royle, M.; Collins, S.N.; Shelton, J.C. Influence of cup orientation on the wear performance of metal-on-metal hip replacements. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2009, 223, 449–457. [Google Scholar] [CrossRef] [PubMed]
- De Haan, R.; Pattyn, C.; Gill, H.S.; Murray, D.W.; Campbell, P.A.; De Smet, K. Correlation between inclination of the acetabular component and metal ion levels in metal-on-metal hip resurfacing replacement. J. Bone Jt. Surg. Br. 2008, 90, 1291–1297. [Google Scholar] [CrossRef] [PubMed]
- Hart, A.J.; Ilo, K.; Underwood, R.; Cann, P.; Henckel, J.; Lewis, A.; Cobb, J.; Skinner, J. The relationship between the angle of version and rate of wear of retrieved met-al-onmetal resurfacings: A prospective; CT-based study. J. Bone Jt. Surg. Br. 2011, 93, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Langton, D.J.; Jameson, S.S.; Joyce, T.J.; Webb, J.; Nargol, A.V.F. The effect of component size and orientation on the concentra-tions of metal ions after resurfacing arthroplasty of the hip. J. Bone Jt. Surg. Br. 2008, 90, 1143–1151. [Google Scholar] [CrossRef]
- Abdel, M.P.; von Roth, P.; Jennings, M.T.; Hanssen, A.D.; Pagnano, M.W. What Safe Zone? The Vast Majority of Dislocated THAs Are Within the Lewinnek Safe Zone for Acetabular Component Position. Clin. Orthop. Relat. Res. 2016, 474, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Tezuka, T.; Heckmann, N.D.; Bodner, R.J.; Dorr, L.D. Functional Safe Zone Is Superior to the Lewinnek Safe Zone for Total Hip Arthroplasty: Why the Lewinnek Safe Zone Is Not Always Predictive of Stability. J. Arthroplast. 2019, 34, 3–8. [Google Scholar] [CrossRef]
- Takada, R.; Jinno, T.; Miyatake, K.; Hirao, M.; Kimura, A.; Koga, D.; Yagishita, K.; Okawa, A. Direct anterior versus anterolateral approach in one-stage supine total hip arthroplasty. Focused on nerve injury: A prospective, randomized, controlled trial. J. Orthop. Sci. 2018, 23, 783–787. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Patients Undergoing Total Hip Replacement for Treatment of End-Stage Primary Hip Osteoarthritis |
|---|---|
| Intervention | Total hip replacement with use of one of the surgical approaches to the hip joint (anterolateral, posterior, or direct lateral) |
| Comparisons | Patients undergoing total hip replacement via direct anterior approach to the hip joint |
| Outcomes | Radiographic analysis (femoral stem alignment, mean radiographic cup inclination, mean radiographic cup anteversion, mean radiographic cup abduction, position in Lewinnek’s safe zone) |
| Study design | Randomized controlled trial |
| References, Year Compared Approaches | Number of Participants in Each Group (Females/Males, Left/Right Hips) | Patients’ Characteristics Age (years); BMI (kg/m2) | Implants Used |
|---|---|---|---|
| Nistor [8], 2017 DAA vs. LA | DAA: 35 (F/M: 26: 9, L/R: 19: 16) LA: 35 (F/M: 16: 19, L/R: 18: 17) | DAA: 67 (53.5, 72.5); 27.45 ± 3.76 LA: 64 (54.5, 67.5); 28.63 ± 3.12 | Metabloc™ uncemented femoral stem system, cobalt–chrome Versys® 32 mm diameter femoral head, polyethylene liner form Trilogy® acetabular system, and Trilogy® uncemented acetabular system shell, with acetabular self-tapping bone screws if needed (Zimmer Warsaw, IN 46,580, USA). |
| Reichert [21], 2018 DAA vs. LA | DAA: 73 (F/M: 32: 45, L/R: NA) LA: 50 (F/M: 32: 49, L/R: NA) | DAA 63.2 (44–77); 28.1 ± 3.7 LA: 61.9 (50–78); 28.3 ± 3.4 | Trilogy or Allofit cups (Trilogy® Acetabular Hip System; Allofit® Acetabular Cup System), the non-cemented M/L Taper stem, or the cemented M. E. Müller straight stem. Overall, the anterior group included four cemented stems, while the lateral group included five cemented stems. |
| Dienstknecht [22], 2014 DAA vs. LA | DAA: 55 (F/M 33: 22, L/R: 27:28) LA: 88 (F/M 47: 41, L/R: 47:41) | DAA: 61.9 ± 12.1 (33–85); 27.6 ± 6.0 (15.7–42.0) LA: 61.3 ± 11.6 (35–89); 30.1 ± 5.6 (17.6–48.8) | Pressfit acetabular components and cement-free hydroxyapatite-coated stems with metal heads were used. Five patients in the Bauer group and one patient in the Micro-hip group received a cemented stem because of poor bone stock. |
| Cheng [23], 2017 DAA vs. PA | DAA: 35 (F/M: 20: 15, L/R: NA) LA: 38 (F/M: 20: 18, L/R: NA) | DAA: 59 (IQR54, 69); 27.7 (25.8, 30.0) LA: 62.5 (IQR55, 69); 28.3 (24.8, 31.1) | R3 acetabular system and Anthology femoral stem. |
| Taunton [24], 2014 DAA vs. PA | DAA: 27 (F/M: 15: 12, L/R: NA) LA: 27 (F/M: 14: 13, L/R: NA) | DAA: 62.05; 27.7 PA: 66.4; 29.2 | The same femoral component design (Corail; DePuy, Warsaw, Indiana) and the same acetabular component design (Pinnacle; DePuy) were used in every case. |
| Barret [25], 2013 DAA vs. PLA | DAA: 43 (F/M: 14: 29, L/R: 21:22) PLA: 44 (F/M: 25: 19, L/R: 20:24) | DAA: 61.4 ± 9.2; 30.7 ± 5.4 PLA: 63.2 ± 7.7; 29.1 ± 5.0 | Corail Total Hip System femoral stem, a Pinnacle Acetabular Cup System cup, an AltrX cross-linked polyethylene liner, and a cobalt chromium-molybdenum femoral head with size 28, 32, or 36 mm. |
| Zhao [26], 2017 DAA vs. PLA | DAA: 60 (F/M: 36: 24, L/R: NA) PLA: 60 (F/M: 34: 26, L/R: NA) | DAA: 64.88 ± 12.13; 25.58 ± 2.83 PLA:62.18 ± 14.72; 24.35 ± 3.10 | N/A |
| Brun [28], 2019 DAA vs. LA | DAA: 84 (F/M: 59: 25, L/R: NA) LA: 80 (F/M: 50: 30, L/R: NA) | DAA: 67.2 ± 8.6; 27.7 ± 3.6 LA:65.6 ± 8.6; 27.6 ± 3.9 | Cemented cup (Marathon; DePuy, Warsaw, IN, USA), uncemented stem (Corail; DePuy), and ceramic head with a diameter of 32 mm (BIOLOX Forte; CeramTec, Plochingen, Germany). |
| Taunton [27], 2018 DAA vs. PA | DAA: 52 PA: 49 | DAA: 65 ± 10 (38–84); 29 ± 22 (19–39) PA: 64 ± 11 (37–85); 30 ± 4 (22–39) | Hemispherical uncemented acetabular component (Pinnacle®; DePuy Orthopaedics Inc, Warsaw, IN, USA), hydroxyapatite-coated femoral stem (Corail®; DePuy Orthopaedics Inc), and Biolox® delta ceramic femoral head (CeramTec GmbH, Plochingen, Germany). |
| References | Randomization Process | Deviations from Intended Interventions | Missing Outcome Data | Measurement of the Outcome | Selection of the Reported Result | Overall Bias |
|---|---|---|---|---|---|---|
| Nistor [8] | + | + | + | + | + | + |
| Reichert [21] | + | + | + | + | + | + |
| Dienstknecht [22] | + | + | + | Not stated | + | + |
| Cheng [23] | + | + | + | - | + | + |
| Taunton [24] | + | + | + | - | + | + |
| Barret [25] | + | + | + | - | + | + |
| Zhao [26] | + | + | + | + | + | + |
| Taunton [27] | + | + | + | - | + | + |
| Brun [28] | + | + | + | + | + | + |
| References, Year Compared Approaches | DAA | LA | PA | PLA |
|---|---|---|---|---|
| Nistor [8], 2017 DAA vs. LA | 1.40° (SD 0.99°) varus | 1.29° (SD 1.13°) varus | ||
| Reichert [21], 2018 DAA vs. LA | 5.5% varus 2% valgus 92.5% neutral | 4% varus 2% valgus 94% neutral | ||
| Dienstknecht [22], 2014 DAA vs. LA | 2.6° (SD 2.1°) varus | 2.8° (SD 2.2°) varus | ||
| Cheng [23], 2017 DAA vs. PA | 1.09° varus | 1.62° varus | ||
| Barret [25], 2013 DAA vs. PLA | 2% varus 0% valgus 98% neutral | 26% varus 0% valgus 74% neutral | ||
| Taunton [24], 2014 DAA vs. PA | 4 varus/52 operated | 6 varus, 2 valgus/49 operated | ||
| Brun [28],2019 DAA vs. LA | 3.1° (SD 1.5°) varus | 2.9° (SD 1.1°) varus |
| References, Year Compared Approaches | DAA | LA | PA | PLA |
|---|---|---|---|---|
| Nistor [8], 2017 DAA vs. LA | 36.97° (SD 1.85°) | 39.63° (SD 2.88°) | ||
| Reichert [21], 2018 DAA vs. LA | 38.6° (SD 5.7°) | 40.3° (SD 6.2°) | ||
| Dienstknecht [22], 2014 DAA vs. LA | 48.1° (SD 6.0°) | 49.7° (SD 6.0°) | ||
| Cheng [23], 2017 DAA vs. PA | 46.07° | 45.86° | ||
| Taunton [24], 2014 DAA vs. PA | 38.0° | 40.0° | ||
| Barret [25], 2013 DAA vs. PLA | 47.1° (SD 6.1°) | 42.4° (SD 7.6°) | ||
| Zhao [26], 2017 DAA vs. PLA | 41.3° | 40.8° | ||
| Taunton [27], 2018 DAA vs. PA | 37° (SD 5°) | 39° (SD 6°) | ||
| Brun [28],2019 DAA vs. LA | 49.5° (SD 7.4°) | 47.0° (SD 6.0°) |
| References, Year Compared Approaches | DAA | LA | PA | PLA |
|---|---|---|---|---|
| Cheng [23], 2017 DAA vs. PA | 24.57° | 20.34° | ||
| Taunton [24], 2014 DAA vs. PA | 26° | 29° | ||
| Barret [25], 2013 DAA vs. PLA | 20.1° (SD 5.9°) | 25.8° (SD 8.1°) | ||
| Zhao [26], 2017 DAA vs. PLA | 17.1° | 21.3° | ||
| Taunton [27], 2018 DAA vs. PA | 23° (SD 4°) | 25° (SD 6°) | ||
| Brun [28], 2019 DAA vs. LA | 9.4° (SD 4.8°) | 5.8° (SD 4.3°) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stolarczyk, A.; Stolarczyk, M.; Stępiński, P.; Dorocińska, M.K.; Świercz, M.; Szymczak, J.; Żarnovsky, K.; Żuchniewicz, A.; Maciąg, B.M. The Direct Anterior Approach to Primary Total Hip Replacement: Radiological Analysis in Comparison to Other Approaches. J. Clin. Med. 2021, 10, 2246. https://doi.org/10.3390/jcm10112246
Stolarczyk A, Stolarczyk M, Stępiński P, Dorocińska MK, Świercz M, Szymczak J, Żarnovsky K, Żuchniewicz A, Maciąg BM. The Direct Anterior Approach to Primary Total Hip Replacement: Radiological Analysis in Comparison to Other Approaches. Journal of Clinical Medicine. 2021; 10(11):2246. https://doi.org/10.3390/jcm10112246
Chicago/Turabian StyleStolarczyk, Artur, Magda Stolarczyk, Piotr Stępiński, Monika K. Dorocińska, Maciej Świercz, Jakub Szymczak, Krystian Żarnovsky, Albert Żuchniewicz, and Bartosz M. Maciąg. 2021. "The Direct Anterior Approach to Primary Total Hip Replacement: Radiological Analysis in Comparison to Other Approaches" Journal of Clinical Medicine 10, no. 11: 2246. https://doi.org/10.3390/jcm10112246
APA StyleStolarczyk, A., Stolarczyk, M., Stępiński, P., Dorocińska, M. K., Świercz, M., Szymczak, J., Żarnovsky, K., Żuchniewicz, A., & Maciąg, B. M. (2021). The Direct Anterior Approach to Primary Total Hip Replacement: Radiological Analysis in Comparison to Other Approaches. Journal of Clinical Medicine, 10(11), 2246. https://doi.org/10.3390/jcm10112246