Abstract
In addition to more narrow criteria such as safety, effectiveness and cost-effectiveness, vaccines can also be evaluated based on broader criteria such as their economic impact, contribution to disease eradication objectives, caregiver aspects, financial protection offered, equity or social acceptability. We summarize a survey executed in a sample of the population (n = 1000) in Flanders, Belgium, in which we investigated support for using these broader criteria to evaluate vaccines for funding decisions. By means of both favourable and unfavourable framings of a hypothetical vaccine across 40 value dimensions, we find support for the view that people indeed consider a broad range of medical and socio-economic criteria relevant. Several of these are not incorporated in standard evaluation frameworks for vaccines. The different results we find for different framings highlight the importance of developing a consistent a priori value framework for vaccine evaluation, rather than evaluating vaccines on an ad hoc basis.
1. Introduction
Since the discovery of the first smallpox vaccine in the eighteenth century, public health policy makers now have at least fifty safe and effective vaccines at their disposal to prevent infectious diseases in their population [1]. However, as vaccine schedules cannot become overcrowded and budgets are finite, priority-setting between these vaccines is an inevitable reality of policy-making. To assist governments in making these difficult but inevitable choices, various decision-aid frameworks have been developed. These frameworks can be broadly categorized into two groups. On the one hand there are deliberative frameworks in which a structured set of general evaluation principles are defined for vaccines [2,3,4,5,6,7,8]. Examples of this deliberative approach were developed in 2014 by the WHO or in 2010 by the Health Council of the Netherlands. In the WHO framework, vaccines are evaluated based on the medical burden of the disease (its clinical aspects as well as its perception and alignment with national health policy goals), the performance, availability and economic impact of the vaccine and the impact of the vaccination program on the healthcare system (e.g., in terms of operational challenges) [3]. In the Dutch example a vaccine is evaluated on five dimensions: severity and size of the disease burden, effectiveness and safety of the vaccine, acceptability of the vaccine, efficiency of the vaccine and its priority relative to other vaccines [4]. The alternative is to adopt an algorithmic approach in which a scoring formula is used to estimate a vaccine’s value. The most elaborate representative of this approach is cost-utility analysis (CUA), expressing the value-for-money of a vaccine in a ratio of incremental costs per quality-adjusted life year (QALY) gained [9,10]. Criteria that are considered relevant in CUA are direct vaccine and disease treatment costs, indirect productivity losses and net health gains in QALYs due to vaccination, as well as the timing of the occurrence of the costs and effects. A concrete example of how a CUA-approach can produce rankings for vaccine priority setting can be found in the report “Vaccines for the 21st century” from the National Academy of Sciences (NAS) of the United States [11]. An updated and improved multiple criteria decision analysis (MCDA) framework from the NAS is “Smart Vaccines” [12,13].
Common to all these decision-aid frameworks for vaccine evaluation is the difficulty to define the right “evaluation space” for vaccines: the dimensions on which the performance of a vaccine should be evaluated. Vaccines have been shown to result in a broad range of potential consequences, beyond their rather narrow, clinically defined effects or their short-term healthcare costs and impact on labour productivity [14,15,16,17,18]. The COVID-19 crisis highlighted this fact and showed how infectious diseases can have enormous broader social, economic, political, psychological and ethical consequences. Before the pandemic, substantial literature had emerged highlighting how these broader consequences of infectious diseases are neglected in existing vaccine evaluation frameworks (see e.g., [17,19,20,21,22,23,24,25]).
At the same time it seems reasonable, in the first place for pragmatic reasons of a lack of reliable data or science, that not all consequences of vaccination can be included in vaccine evaluation (e.g., through health technology assessment). Certain criteria may be considered irrelevant for more fundamental reasons than pragmatism; because they are judged as irrelevant to the decision context. For instance, vaccines can be produced domestically by local vaccine manufacturers and funding a new vaccine might therefore affect employment and economic development. Anti-vaccination lobbies can fight the introduction of a particular vaccine and this might affect the broader public support for other vaccines as well [26]. Such consequences might be considered less relevant (or irrelevant) as a foundation to decide whether the vaccine should receive funding priority or not. Therefore, a good value framework for vaccines must find a balanced set of evaluation criteria that are “individually necessary and jointly sufficient” to assess the benefits offered relative to their costs.
To contribute to our understanding of which criteria are essential to be included in such a vaccine value framework, we set up a survey to investigate which criteria the general public considers most relevant to be used in vaccine funding decisions. Although, of course, lay people’s opinions are no substitute for the more technical judgment of experts, they can be an insightful “common sense” complement to it [27]. Moreover, it is important that decisions about which vaccine deserves funding are (at least partly) in line with public preferences. An unsupported vaccine evaluation framework that excludes important aspects or that includes (seemingly) less relevant aspects might increase mistrust in the decision-making process for vaccine funding, e.g., by creating perceptions propagated by anti-vaccination lobbies that governments are tied to pharmaceutical industries.
2. Materials and Methods
2.1. Survey
We constructed 40 criteria with potential relevance to vaccine evaluation, ranging from more obvious criteria such as safety or effectiveness to less obvious criteria such as contribution to disease eradication or impact on patient caregiving by family members. Of these criteria, 17 involved epidemiological and clinical aspects of the disease and the vaccine and 22 had a broader socio-economic nature. A respondent sample had to rate how relevant each criterion was to the decision whether a vaccine should be funded or not.
First, we familiarized respondents with the problem of budget scarcity and with the government’s challenge of setting vaccine priorities. Respondents received the following background: “The Flemish government has a fixed annual budget for vaccinations for the Flemish population. However, there are too many vaccines on the market and the budget is too small to pay for all possible vaccines. In other words, the government must choose and prioritize among the available vaccines. However, the question is: how should she do this? Based on which arguments?”
Next, we presented respondents with a fictitious vaccine that was candidate for public funding and invited them to assist the government in making a funding decision. More specifically, we asked respondents whether the vaccine’s performance on any of the 40 dimensions was relevant or not for the ultimate funding decision: “Imagine that the government is faced with the choice of either reimbursing a certain vaccine (called “VACCINEX”) or not reimbursing it. If she chooses VACCINEX, it means that there is less money available to pay for other vaccines. In the following, we will each time show you an argument that may be either important or unimportant for the funding decision”.
A simplistic example:
- -
- If we tell you that VACCINEX is a safe or unsafe vaccine, that is probably a relevant argument.
- -
- If we tell you that VACCINEX is in a nice or ugly package, that is probably not a relevant argument.
QUESTION: Should the government take this argument into account when deciding whether or not to reimburse VACCINEX? Or do you think this argument is irrelevant and should not play a role?
Respondents had to indicate the relevance to vaccine funding of each of the 40 value propositions on a Likert scale from 1 to 10. As the particular framing of the value proposition can affect people’s judgment [28], we decided to present criteria in two ways: through a favourable and an unfavourable framing. In the favourable version, the vaccine under evaluation scored well on the particular criterion. If this specific dimension is deemed relevant, then the vaccine would become more attractive for funding. In the unfavourable version, the vaccine scored poorly on the particular criterion. When the criterion is considered relevant, it becomes less attractive for funding. Both framings are important to understand the relevance of an overarching criterion. For example, the “vaccine safety” dimension could be deemed extremely important to guide decisions in case a vaccine induces a risk of serious side effects. But when a vaccine has no side effects at all, people might consider safety more self-evident and attribute lower importance to a vaccine’s safety profile. Table 1 shows all statements in their two formulations. We chose a “between subjects” design: each respondent evaluated either only 40 favourable or 40 unfavourable framings. All 40 statements were presented in random order to each respondent to avoid any order effects.

Table 1.
Value propositions, favourably and unfavourably framed.
2.2. Sample
Via a market research agency (Research Now SSI–RN SSI) we collected two quasi-representative samples of 500 respondents, one for the favourable set of value propositions and one for the unfavourable one. Initially a stratified random sample of in total 1580 respondents was recruited from an online panel of 250,000 Flemish members (4% of the population), based on quotas for the Flemish population for the characteristics gender, age, educational level and geographical spread. Panel members received small incentives for participating in the research (e.g., vouchers). All these respondents completed our survey. The research agency then applied strict criteria and implemented tests to guarantee high data quality for our final sample. First, it excluded all “speedsters” (respondents who finish the survey in less than a third of the median time to complete the survey for the entire sample) and “straight-liners” (respondents who consistently give the same answer throughout the entire survey). Second, a test was added to the survey to be able to exclude those respondents who gave thoughtless answers. Two of the value propositions were repeated throughout the survey (so respondents completed 42 rating exercises in total). When there was more than 2 points difference between the scores given to both pairs of value propositions, respondents were automatically excluded from the final sample. For example, a score of 5/10 and 9/10 on one of the two repeated value propositions, and one of 5/10 and 8/10 on the other, led to automatic exclusion of the respondent. In total 580 respondents were excluded, leading to 1000 survey responses that were considered sufficiently valid and reliable for our analysis. Sample size calculation for comparing the means of two groups showed that a sample size of 500 respondents per group was more than sufficient to find significant differences of 0.5 in the mean respondent scores with a 95% power. Table 2 lists the main demographic characteristics of the included respondents.
Table 2.
Sample characteristics.
3. Results
Figure 1 shows boxplots with the distributions of the respondent scores across the sample for the favourable and unfavourable statements. The asterisks on the boxplots denote the averages.
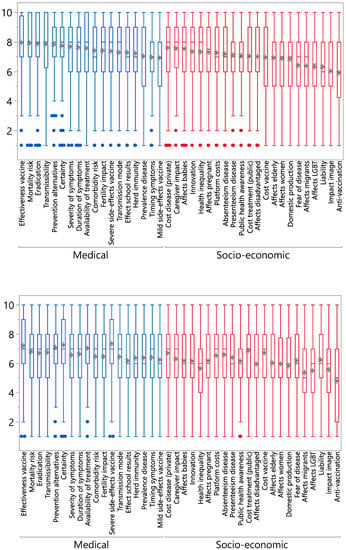
Figure 1.
Boxplots with respondent scores on the favourable and unfavourable propositions. Upper panel: favourable propositions, lower panel: unfavourable propositions.
Three overall observations can be made. First, none of the 40 dimensions was dismissed as completely irrelevant by our sample, i.e., obtaining an average score below 5 in both positive and negative framings. The average of the positive items ranged from 5.9 (for the anti-vaccination proposition) to 7.9 (for the mortality proposition). The average of the negative items ranged from 4.8 (for the anti-vaccination proposition) to 7.3 (for the severe side-effects proposition). Only the negatively phrased anti-vaccination proposition had an average relevance score below 5. This indicates that our sample considers a broad range of criteria relevant to evaluate vaccines. Table 3 presents a ranking of the average scores of all statements in their positive and negative variants and connects them by means of letters. Statements with the same letter indicate that the average scores’ 95% confidence intervals overlap. This means that these average scores do not significantly differ from each other at the 5% level. The most relevant aspects were vaccine effectiveness, mortality risk, eradication potential, transmissibility, prevention alternatives, scientific certainty, severity of symptoms, duration of symptoms, cost disease (private), availability of treatment, caregiver impact, severe side-effects of the vaccine and whether the disease affects babies. The least relevant dimensions were whether the disease mainly affects migrants or LGBT members, legal liability for the state, impact on the country’s image and response by anti-vaccination groups.
Table 3.
Analysis of variance (ANOVA) for analysing differences in the mean scores for the 40 statements.
Second, Table 3 shows that, overall, socio-economic aspects were considered less relevant than medical aspects related to (broader) safety and effectiveness. There were, however, a few notable exceptions. Whether the disease had high or low private and public treatment costs, whether there was a large impact on informal caregiving, a high vaccine cost and whether babies were particularly affected by the disease were all deemed of high relevance. Amongst the medical statements mild side-effects and timing of symptoms obtained lower scores.
Third, for all evaluation criteria, scores were markedly lower in the unfavourably phrased versions. This means that respondents judged a criterion as overall less relevant when the vaccine under evaluation was not scoring well on it. Vice versa, a criterion was judged as more relevant when the vaccine under evaluation obtained a favourable score on it. For instance, when vaccinex was considered to be protecting against a disease that is not very contagious, the criterion of transmissibility obtained an average score of 6.7. When the disease was contagious, the average score of transmissibility was 7.8.
We investigated whether there were groups of items for which the respondent scores were correlated. A factor analysis revealed two factors in each of the samples. Table 4 shows the factor loadings or correlation coefficients explaining how these factors load on, or correlate with the items’ scores. The first factor mainly describes the medical propositions and the second factor describes the socio-economic criteria. However, important exceptions to this classification were the socio-economic items about the private and public treatment cost of the disease, the caregiver impact of an infection, absenteeism, platform costs and the equity item whether the disease affects babies (or pregnant women). These socio-economic statements varied more alongside the factor of medical aspects. Likewise, the medical items of timing of symptoms and risk of mild side-effects of the vaccine varied more alongside the socio-economic factor. As can be seen in Table 4, the first factor obtained higher overall relevance scores than the second factor.
Table 4.
Factor loadings from a factor analysis on the respondent scores for the favourable and unfavourable statements.
We constructed a general linear model to predict the respondent scores using item and framing (favourable and unfavourable) as categorical explanatory variables including the interaction between them. With an R-square of 95%, the model has a very high prediction power, where the predicted scores are the average scores from the boxplots in Figure 1. Figure 2 presents the predicted scores and their 95% confidence intervals. We clearly observe the relatively high scores of some socio-economic variables, such as caregiver impact and impact on babies. We also notice the systematically lower scores of the negative variants, except for a few items where scores overlap: risk of severe side-effects of the vaccine, treatment cost for the health system, vaccine cost, fear of the disease and legal liability.
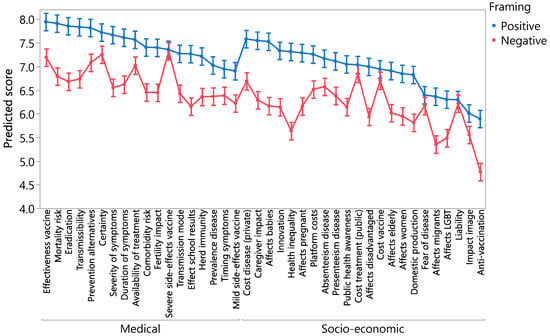
Figure 2.
Predicted scores.
4. Discussion
An important research challenge is to develop adequate evaluation frameworks for vaccines that manage to incorporate the broad range of consequences they can sort. In this study we investigated public support for various of these broader criteria. This is important because vaccine funding decisions are impactful for population health and, as such, they can affect everyone, directly or indirectly. By recommending funding priorities, they determine which infectious disease risks we, as a society, consider a priority to prevent but also which diseases we choose to tolerate. To be “procedurally fair”, these frameworks must be based on “relevant” criteria only: priorities may neither be based on irrelevant information nor on partial, incomplete evaluation only. This is for instance acknowledged in the ethical “Accountability for Reasonableness” (A4R) framework for fair priority setting in healthcare [29].
Our sample did not limit itself to a narrow set of basic criteria (safety, effectiveness, cost-effectiveness) but instead considered the relevance of a broad range of salient and less salient aspects. All the studied criteria, except perhaps the anti-vaccination movement’s response, were considered important (average relevance score above 5/10). Certain socio-economic aspects were considered of particular relevance. For instance, a vaccine’s impact in terms of affecting caregiver burden, treatment cost for the disease, and whether newborns are the main target group played a similar role in regard to the impact of medical aspects such as duration, type or severity of disease symptoms. Amongst the medical aspects, our sample attributed a remarkably high importance to the disease eradication potential of a vaccine and the degree of scientific certainty around the vaccine’s effects.
How do these findings relate to available decision-aid frameworks? Whereas many of the criteria that we studied (disease burden in infected patients, infectivity, duration of symptoms, treatment options, but also the effectiveness of the vaccine and the risk of severe side-effects) are included in deliberative frameworks [5] as well as in CUA [10], several of the considerations that were deemed important are neglected in those evaluation frameworks. For instance, the impact on informal caregiving was considered an important criterion, but this is often given insufficient attention in vaccine evaluation [30]. The potential for disease eradication and the degree of scientific certainty regarding the effect of the vaccine were deemed relevant evaluation criteria. Specific guidelines exist for taking into account uncertainty [31], but they are often not fully followed. Broader aspects of health that can be affected by infectious diseases, such as cognition and fertility (both not included in QALYs [32]) were also found to be more or less relevant by a large proportion of the sample.
A second finding is the large difference that was found in the relevance of a criterion depending on whether the vaccine was presented as more or less favourable. The relevance score of a criterion for vaccine funding decisions was systematically considered lower when the vaccine was presented in a less favourable way. This finding highlights the importance of developing a consistent value framework for vaccines in which the weight of an exhaustive list of criteria is established a priori, rather than evaluating vaccines on an ad hoc basis where the weight or relevance of criteria is determined during the vaccine evaluation process itself. Our study suggests that without using pre-established value frameworks, there is a risk that the focus will be disproportionally on those characteristics that are considered to be most relevant by policy makers to the vaccine under evaluation. Other important criteria that are nonetheless important to other vaccines, which are competing for the same resources, can as such be neglected.
Our study had limitations. We investigated lay people’s opinion regarding a complicated subject. Answers are merely indicative of which criteria matter to the public in vaccine evaluation and are meant to be used in discussions about what an “optimal” value framework for vaccines looks like. We used an online panel for this study and we think this is sufficient for our purpose, but panel membership may be associated with particular characteristics that reduce representativeness (e.g., internet access). Although we did make many efforts to exclude respondents that did not provide thoughtful answers, we still cannot fully distinguish between better and worse informed respondents.
5. Conclusions
In conclusion, vaccines can sort a broad range of consequences but it is not always clear which of these must be incorporated in funding decisions. Our study suggests that people indeed consider many broader aspects of vaccines as relevant and this suggests that they support a broad value framework for vaccines. Our study also indicates that it is important to determine the elements of this framework beforehand. These insights can be valuable to researchers in the fields of health technology assessment, MCDA or evidence-based decision-making who aim to capture the value of vaccines in new evaluation frameworks.
Author Contributions
Conceptualization, all authors; formal analysis, R.K. and J.L.; methodology, all authors; supervision, C.V. and P.B.; writing—original draft, J.L.; writing—review & editing, R.K, C.V. and P.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Flemish government—Agency of Health and Care.
Acknowledgments
We thank the Agency of Health and Care of the Flemish Government for supporting this study. R.K. thanks the JMP Division of SAS Institute for her research fellowship.
Conflicts of Interest
J.L. and R.K. have no conflicts of interest to declare. C.V. has been principal investigator of vaccine clinical trials for G.S.K., M.S.D. and Pfizer, for which the university received a grant. C.V. did not receive any personal payments nor is she a member of any advisory boards. P.B. declares that his university received compensation for time spent on ad-hoc consultation (short duration of ∼2 days) for Pfizer in 2019–2020.
References
- Plotkin, S.L.; Plotkin, S.A. A Short History of Vaccination. In Plotkin’s Vaccines, 7th ed.; Elsevier: Amsterdam, The Netherlands, 2018; pp. 1–15.e8. [Google Scholar]
- Gonzalez-Lorenzo, M.; Piatti, A.; Coppola, L.; Gramegna, M.; Demicheli, V.; Melegaro, A.; Tirani, M.; Parmelli, E.; Auxilia, F.; Moja, L. Conceptual frameworks and key dimensions to support coverage decisions for vaccines. Vaccine 2015, 33, 1206–1217. [Google Scholar] [CrossRef]
- WHO. Choosing Interventions That Are Cost-Effective. 2014. Available online: http://www.who.int/choice/en (accessed on 22 October 2020).
- Houweling, H.; Verweij, M.; Ruitenberg, E.J. Criteria for inclusion of vaccinations in public programmes. Vaccine 2010, 28, 2924–2931. [Google Scholar] [CrossRef] [PubMed]
- Burchett, H.; Mounier-Jack, S.; Griffiths, U.K.; Mills, A. National decision-making on adopting new vaccines: A systematic review. Health Policy Plan. 2011, 27, ii62–ii76. [Google Scholar] [CrossRef]
- Mantel, C.F.; Wang, S.A. The privilege and responsibility of having choices: Decision-making for new vaccines in developing countries. Health Policy Plan. 2012, 27, ii1–ii4. [Google Scholar] [CrossRef]
- Nolan, T. The Australian model of immunization advice and vaccine funding. Vaccine 2010, 28, A76–A83. [Google Scholar] [CrossRef]
- Kimman, T.G.; Boot, H.J.; Berbers, G.A.M.; Bondt, P.E.V.-D.; De Wit, G.A.; Demelker, H. Developing a vaccination evaluation model to support evidence-based decision making on national immunization programs. Vaccine 2006, 24, 4769–4778. [Google Scholar] [CrossRef] [PubMed]
- Drummond, M.F.; Sculpher, M.J.; Claxton, K.; Stoddart, G.L.; Torrance, G.W. Methods for the Economic Evaluation of Health Care Programmes; Oxford University Press.: Oxford, UK, 2005; Volume 3. [Google Scholar]
- Walker, D.G.; Hutubessy, R.; Beutels, P. WHO Guide for standardisation of economic evaluations of immunization programmes. Vaccine 2010, 28, 2356–2359. [Google Scholar] [CrossRef]
- IOM. Vaccines for the 21st Century: A Tool for Decisionmaking; Stratton, K.R., Durch, J.S., Lawrence, R.S., Eds.; The National Academies Press: Washington, DC, USA, 2000; p. 472. [Google Scholar]
- Knobler, S.L.; Bok, K.; Gellin, B. Informing vaccine decision-making: A strategic multi-attribute ranking tool for vaccines—SMART Vaccines 2.0. Vaccine 2017, 35, A43–A45. [Google Scholar] [CrossRef] [PubMed]
- Phelps, C.; Madhavan, G.; Sangha, K.; Rappuoli, R.; Colwell, R.R.; Martinez, R.M.; Kelley, P.; King, L. A priority-setting aid for new vaccine candidates. Proc. Natl. Acad. Sci. USA 2014, 111, 3199–3200. [Google Scholar] [CrossRef]
- Van Der Putten, I.; Hiligsmann, M.; Paulus, A.; Hutubessy, R.; Evers, S.M.A. Identifying the Broader Value of Vaccines in Low and Middle Income Countries. Value Health 2014, 17, A548. [Google Scholar] [CrossRef][Green Version]
- Bärnighausen, T.; Berkley, S.; Bhutta, Z.A.; Bishai, D.M.; Black, M.M.; Bloom, D.E.; Constenla, D.; Driessen, J.; Edmunds, J.; Evans, D.; et al. Reassessing the value of vaccines. Lancet Glob. Health 2014, 2, e251–e252. [Google Scholar] [CrossRef]
- Sevilla, J.P.; Bloom, D.E.; Cadarette, D.; Jit, M.; Lipsitch, M. Toward economic evaluation of the value of vaccines and other health technologies in addressing AMR. Proc. Natl. Acad. Sci. USA 2018, 115, 12911–12919. [Google Scholar] [CrossRef] [PubMed]
- Jit, M.; Hutubessy, R.; Png, M.E.; Sundaram, N.; Audimulam, J.; Salim, S.; Yoong, J. The broader economic impact of vaccination: Reviewing and appraising the strength of evidence. BMC Med. 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Luyten, J.; Beutels, P.; Beutels, P. Costing Infectious Disease Outbreaks for Economic Evaluation. PharmacoEconomics 2009, 27, 379–389. [Google Scholar] [CrossRef]
- Barnighausen, T. Valuing vaccination. Proc. Natl. Acad. Sci. USA 2014, 111, 12313–12319. [Google Scholar] [CrossRef]
- Bloom, D.E.; Fan, V.Y.; Sevilla, J.P. The broad socioeconomic benefits of vaccination. Sci. Transl. Med. 2018, 10, eaaj2345. [Google Scholar] [CrossRef]
- Bloom, D.E.; Brenzel, L.; Cadarette, D.; Sullivan, J. Moving beyond traditional valuation of vaccination: Needs and opportunities. Vaccine 2017, 35, A29–A35. [Google Scholar] [CrossRef]
- Luyten, J.; Beutels, P. The Social Value Of Vaccination Programs: Beyond Cost-Effectiveness. Health Aff. 2016, 35, 212–218. [Google Scholar] [CrossRef]
- Beutels, P.; Scuffham, P.A.; MacIntyre, C.R. Funding of drugs: Do vaccines warrant a different approach? Lancet Infect. Dis. 2008, 8, 727–733. [Google Scholar] [CrossRef]
- Luyten, J.; Kessels, R.; Goos, P.; Beutels, P. Public Preferences for Prioritizing Preventive and Curative Health Care Interventions: A Discrete Choice Experiment. Value Health 2015, 18, 224–233. [Google Scholar] [CrossRef]
- Luyten, J.; Dorgali, V.; Hens, N.; Beutels, P. Public preferences over efficiency, equity and autonomy in vaccination policy: An empirical study. Soc. Sci. Med. 2013, 77, 84–89. [Google Scholar] [CrossRef] [PubMed]
- Luyten, J.; Bruyneel, L.; Van Hoek, A.J. Assessing vaccine hesitancy in the UK population using a generalized vaccine hesitancy survey instrument. Vaccine 2019, 37, 2494–2501. [Google Scholar] [CrossRef] [PubMed]
- Luyten, J.; Kessels, R.; Atkins, K.E.; Jit, M.; van Hoek, A.J. Quantifying the public’s view on social value judgments in vaccine decision-making: A discrete choice experiment. Soc. Sci. Med. 2019, 228, 181–193. [Google Scholar] [CrossRef]
- Gong, J.; Zhang, Y.; Yang, Z.; Huang, Y.; Feng, J.; Zhang, W. The framing effect in medical decision-making: A review of the literature. Psychol. Health Med. 2013, 18, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Daniels, N.; Sabin, J. Setting Limits Fairly: Learning How to Share Resources for Health; Oxford University Press.: Oxford, UK, 2008. [Google Scholar]
- Annemans, L.; Beutels, P.; Bloom, D.; Debacker, W.; Ethgen, O.; Luyten, J.; Van Wilder, P.; Van Laethem, Y.; Willem, L.; Simoens, S. Economic evaluation of vaccines: Belgian reflections on the need for a broader perspective. Value Health 2020, in press. [Google Scholar]
- Bilcke, J.; Beutels, P.; Brisson, P.M.; Jit, M. Accounting for Methodological, Structural, and Parameter Uncertainty in Decision-Analytic Models. Med. Decis. Mak. 2011, 31, 675–692. [Google Scholar] [CrossRef]
- Brazier, J.; Ratcliffe, J.; Saloman, J.; Tsuchiya, A. Measuring and Valuing Health Benefits for Economic Evaluation; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).