Abstract
Background: The Measles–Rubella Microarray Patch (MR-MAP) is an important technology that is expected to reduce coverage and equity gaps for measles-containing vaccines (MCVs), reach zero-dose children, and contribute to elimination of measles and rubella. MR-MAPs are anticipated to be easier to deploy programmatically and could be delivered by lesser-trained health workers, thereby increasing immunization coverage. The most advanced MR-MAP has reached clinical proof-of-concept through a Phase I/II trial in the target population of infants and young children. The World Health Organization (WHO) and partners have developed the Phase III clinical trial framework for MR-MAPs presented in this article. Objectives and Methods: The purpose of such framework is to inform the considerations, design and approach for the pivotal clinical trial design, while considering the anticipated data requirements to inform regulatory approval, WHO prequalification, and policy decision. Results: The proposed Phase III trial would compare the immunogenicity and safety of an MR-MAP with MR vaccine delivered subcutaneously in 9- to 10-month-old infants. An analysis of non-inferiority (NI) of immunogenicity would occur six weeks after the first dose. Should regulatory agencies or policy makers require, a proportion of infants could receive a second dose of either the same or alternate MR vaccine presentation six months after the first dose, with those children returning six weeks after the second dose for a descriptive assessment of immunogenicity, and then followed up six months after the second dose for evaluation of safety and immunogenicity. It is anticipated that this proposed pivotal Phase III trial framework would generate the required clinical data for regulatory licensure and WHO prequalification (PQ) of MR-MAPs. However, the trial design would need to be reviewed and confirmed by a national regulatory authority (NRA) that will assess the product for regulatory licensure and the WHO PQ team. Additional research will likely be required to generate data on concomitant vaccine delivery, the safety and immunogenicity of MR-MAPs in other age groups such as children 1–5 years and infants younger than 9 months of age, and the impact of MR-MAPs on coverage and equity. Such studies could be conducted during or after clinical MR-MAP development.
1. Introduction
Between 2021 and 2022, modeled global measles cases increased by 18% from 7,802,000 to 9,232,300, and the number of countries facing large or disruptive outbreaks rose from 22 to 37 [1]. In 2023, approximately 35 million children missed their first or second dose of measles-containing vaccine (MCV1 and MCV2), with 83% receiving MCV1 and 74% receiving both doses [2]. The WHO recommends that countries should strive to attain and sustain a minimum of 95% MCV coverage for both doses [3]. While vaccine effectiveness of a single dose rubella-containing vaccine (RCV) is higher than MCV, it is recommended that RCV in a 2-dose schedule be provided in combination with the measles vaccine, and the goal for rubella vaccination coverage should also be >95% given the common presentation for the vaccine [4]. Despite considerable progress incorporating the RCV into routine immunization programs globally, approximately 25 million infants still do not have access to the RCV every year [5]. Modeled estimates show a 66% decrease in the worldwide burden of congenital rubella syndrome (CRS) from 2010 to 2019; however, over 32,000 infants are still born with CRS annually, nearly all in countries that have not introduced a routine dose of the RCV [6].
Currently available MCVs are in a vial presentation and are lyophilized, requiring reconstitution with diluent prior to immunization use. They are reconstituted with a reuse prevention syringe and administered with an auto-disable needle and syringe (N&S). MCVs are often in a multi-dose vial presentation, which can result in vaccine wastage as any remaining doses in reconstituted open vials must be discarded within 6 h of opening. This has led to vaccinator reluctance in opening multi-dose vials, which results in missed opportunities for vaccination [7,8,9].
There are challenges with N&S-delivered MCV that constrain immunization programs from reaching high vaccine coverage. Examples include the requirements for vaccinators to reconstitute and administer a vaccine, the logistics of reaching remote populations due to limited vaccine thermostability, as well as safe sharps waste disposal [9].
Microarray patches (MAPs) are novel vaccine delivery devices in product development comprising multiple microprojections coated with, or composed of, a vaccine. Upon application to the skin, the vaccine is delivered to the dermis and epidermis in a usually less painful and minimally invasive manner than N&S. This single dose, ready-to-use presentation is expected to be easier to use, will not require vaccine reconstitution, nor require additional supplies such as syringes and, therefore, will reduce open-vial wastage and sharps waste, and is likely to have enhanced thermostability [10,11], when compared to vaccines delivered by N&S. Such attributes are anticipated to bring many opportunities to increase equitable vaccination coverage; for example, a possibility of administration of MR-MAPs by community health workers, immunization of hard-to-reach populations, the potential for partial distribution beyond the cold chain, and fewer missed opportunities for vaccination. The opportunities are likely to translate to public health impact—it has been estimated that between 2030 and 2040, the use of MR-MAPs in routine immunization and supplementary immunization activities (SIAs), partially replacing N&S use, could reduce measles burden by 27–37% in 70 low- and middle-income countries (LMICs) compared to the current N&S-only immunization strategy [12]. The evaluation and further validation of MR-MAP use cases in nine countries highlighted that the use of MR-MAPs in outreach immunization and SIAs would have the highest impact on MR vaccine coverage [9,13]. As such, MR-MAPs are anticipated to play a crucial role in eliminating measles and rubella and have been designated as a priority innovation by global initiatives such as Vaccine Innovation Prioritization Strategy, global stakeholders [14,15,16], and the Measles & Rubella Partnership [17].
There are two MR-MAP candidates that are currently in clinical development. A dissolving MAP from Micron Biomedical Inc has recently been evaluated in a Phase I/II trial in 15-month-old MR vaccinated toddlers and 9-month-old MR naïve infants in the Gambia. The trial reported that MR vaccines delivered by a MAP have comparable safety and immunogenicity to MR vaccines delivered by N&S [18,19]. Another candidate, a high-density vaccine-coated microarray patch (HD-MAP) developed by Vaxxas, has been evaluated in a Phase I trial in previously MR vaccinated, healthy Australian young adults. The trial reported that the MR vaccine delivered by a MAP has similar levels of safety and immunogenicity as the MR vaccine delivered by N&S [20]. Other MR-MAP candidates are in preclinical development. In June 2023, the WHO’s Product Development for Vaccines Advisory Committee (PDVAC) held a meeting to discuss the Phase I/II proof-of-concept clinical trial results presented by Micron Biomedical and provide recommendations for further clinical development and implementation research for MR-MAPs (Box 1) [21].
Box 1. 2023 PDVAC MR-MAP Recommendations [21].
- A regulatory strategy should be developed to allow for the quickest route of product approval and WHO PQ, which would be with WHO prequalified MR vaccines.
- Priority use cases are campaigns and supplementary immunization activities and outbreak response.
- Conduct safety and immunogenicity assessment in naïve 9-month-old infants to optimize dose, wear time and anatomical site.
- Assess an application on the wrist for a 1-min wear time with the dose used in the Phase I/II study, shifting to a 5-min wear time and a different application site out of the reach of the child, depending on the data generated.
- MR-MAP product labeling for a VVM 30 (stability at 37 °C) as well as controlled temperature chain (CTC), which requires thermostability at 40 °C for a minimum of 3 days to allow for the use case in supplemental immunization activities (SIA—campaigns) and outbreak scenarios.
- Evaluate the potential for dose reduction and the possible impact on thermostability.
- In future clinical research, include mild and moderately malnourished infants in a Phase II study and severely malnourished infants in a Phase III study.
- Identify vaccines that could be co-administered with MR-MAPs and related use cases.
- Expanded use/indications for MR-MAPs: inclusion of 6-month old infants, next generation MR vaccines, HIV+ individuals.
- Develop Evidence Considerations for Vaccine Policy (ECVP) for MR-MAPs.
The first MR-MAP for use is anticipated to be available for introduction by 2030, following product design finalization, construction and validation of an initial commercial manufacturing facility, Phase III clinical testing, approval of regulatory applications for marketing authorization, and prequalification (PQ) by the WHO. The initial commercial production lines are anticipated to launch by 2030, with limited supply at product launch until manufacturing scale-up is achieved. Further manufacturing scale-up or scale-out will depend upon demand from end-users and additional investment from vaccine developers.
While the pilot-scale manufacturing facilities are being designed and built, an opportunity exists to refine the MR-MAP design, dose, wear time, and anatomical site for delivery, prepare for future programmatic implementation and to discuss the confirmatory clinical data required to support licensure for MR-MAPs.
Therefore, the purpose of this manuscript is to develop a framework to inform considerations, design, and approach for the Phase III trial for MR-MAPs. Through such framework, this manuscript helps ensure that data on MR-MAPs required to inform regulatory and policy decisions are available, limiting the delay in introducing this important innovation to the immunization programs of countries. To support such goal, the WHO, with support from partners, organized a Global Convening of measles and rubella experts, regulators, policymakers, MAP developers, and vaccine manufacturers on MR-MAPs that occurred in April 2024 in New Delhi, India. Here, we report on the background work, discussions, and recommendations and propose an approach for a pivotal MR-MAP Phase III clinical trial.
2. Phase III Trial Framework—Methods
The following methods and approaches were implemented to develop a Phase III trial framework that describes parameters intended to inform marketing application approval by regulatory authorities and WHO policy and prequalification requirements.
2.1. Desk-Based Research and Stakeholder Interviews
Between November 2023 and February 2024, the WHO team conducted a desk-based review of published literature accessed through PubMed, determined to be relevant to the design of a pivotal Phase III trial for MR-MAPs. The review also included published strategy and policy documents, guidelines, reports, and other grey literature documents (see Table 1): the WHO position papers on measles and rubella, the Technical Report Series on the requirements for measles, mumps, and rubella vaccines and combined vaccine as well as clinical trials for vaccines, the WHO/UNICEF MR-MAP Target Product Profile, the PDVAC report from the MR-MAP meeting held June 2023, past published research on MCV and alternative delivery technologies, studies that led to MCV licensure, MCV indications for use and labeling, with emphasis on WHO PQ MR vaccines, regulatory guidance documents (African Vaccine Regulatory Forum (AVAREF), Central Drugs Standard Control Organization (CDSCO), Drugs Controller General of India (DCGI), European Medicines Agency (EMA), United States Food and Drug Administration (USFDA), WHO) and MR-MAP-related research and strategic documents.

Table 1.
Desk-based Review Documents.
In parallel to the desk-based research review, experts in the fields of measles and rubella vaccination, vaccine product development, and in the development of MR microarray patches, were interviewed on the potential design of a Phase III trial, regulatory licensure strategies, and potential programmatic introduction strategies.
For the desk review and the interviews, the information sources were selected based on their relevance, completeness, and quality to identify data to inform regulatory and policy decisions for MR-MAPs. The review focused on peer-reviewed literature published in reputable journals and incorporated positions, strategies, and guidance from leading international organizations. Additionally, interviews were conducted with top experts in measles, rubella, vaccination, and microarray patches to ensure the accuracy and breadth of data. Although a comprehensive desk review was performed, it is acknowledged that this method could have been strengthened by conducting a systematic review. However, given the limited data published on MR-MAPs, the available information was likely already familiar to the authors, who are experts in the field. Factors beyond the scope of informing regulatory and policy decisions were not included in the review.
2.2. MR-MAP Global Convening
During 16–17 April 2024, a global convening was held in New Delhi, India by the WHO Immunization Vaccines and Biologicals Department, WHO India Country Office, and WHO South-East Asia Regional Office. The convening brought together experts and researchers in measles and rubella vaccines and microarray patches; regulatory representatives from the European Medicines Agency (EMA), United States Food and Drug Administration (USFDA), African Vaccine Regulatory Forum (AVAREF), and Drug Controller General of India (DCGI); global experts including from UNICEF, Gavi, PATH, Médecins Sans Frontières, US Centers for Disease Control and Prevention, and Coalition for Epidemic Preparedness Innovations; funders including the Bill & Melinda Gates Foundation and the RIGHT Foundation; vaccine manufacturers; MAP developers; representatives from the Indian Council of Medical Research; and the WHO HQ, Regional (WPRO, SEARO, AFRO, EMRO), and India Country office. The data obtained from desk-based research and stakeholder interviews were presented at the global convening and discussed in six breakout groups focused on (1) Phase III trial design and appropriate primary endpoint(s); (2) appropriate non-inferiority (NI) margin; (3) priority target populations; (4) concomitant vaccine delivery; (5) manufacturing strategy and shelf life; and (6) evaluation of immune responses. The recommendations reported here were formulated based on the presentations and discussions of the stakeholders and finalized during a closed meeting of the WHO Technical Advisory Group on MR-MAPs and the WHO Secretariat, which was held in April 2024.
3. Phase III Trial Framework—Recommendations
This framework is structured to include key elements required to inform the protocol design of a pivotal Phase III clinical trial for MR-MAPs. The national regulatory authorities (NRAs) and the WHO PQ team will need to define key aspects of a proposed study protocol. The data collected during the pivotal Phase III clinical trial should fulfill the regulatory and WHO PQ requirements and, to the extent feasible, generate evidence that is anticipated to inform a policy decision. The additional policy-related data and evidence that are expected to be needed for an MR-MAP, beyond the clinical outcomes and the chemistry, manufacturing and controls (CMC) data required for regulatory marketing authorization approval, will be described in future guidance in the form of WHO Evidence Considerations for Vaccine Policy (ECVP) [30]. The Phase III clinical trial framework will also inform the development of implementation plans for priority use cases of MR-MAPs. Such an approach, along with potential Phase IV “post-marketing” studies aimed at updating the product label or informing policy decisions (such as use in special populations or co-administration), could accelerate the pathway to programmatic introduction, uptake, and public health impact.
The following Phase III clinical trial framework considers the appropriate comparator arms within the trial design (Table 2) and considerations for non-inferiority (NI) margin (Table 3 and Table 4) for the selected primary endpoint, both of which are critical components that inform the clinical trial study arms, number of participants, and complexity of a clinical trial. The priority populations in which the immunogenicity and safety of MR-MAPs should be evaluated are discussed in Table 5. In Table 6, the administration of non-MR vaccines and other health interventions is discussed. The manufacturing considerations that could impact the design of a Phase III clinical trial are discussed in Table 7. Lastly, the appropriateness and selection of immune assays to be included in a clinical trial are covered in Table 8.
Table 2.
Clinical Trial Design.
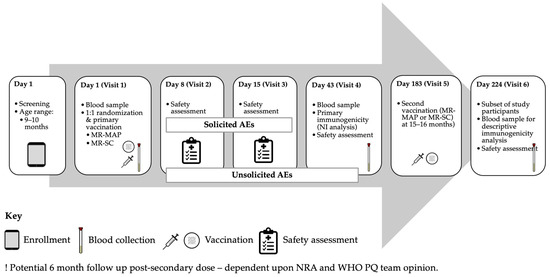
Figure 2.
Illustrative Phase III Trial Flowchart.
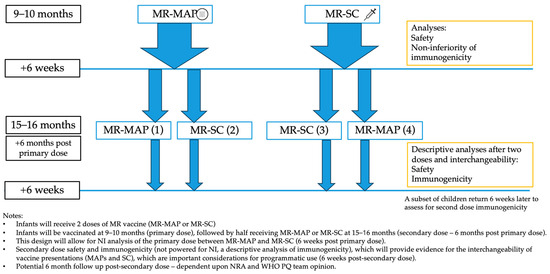
Figure 1.
Proposed Phase III Trial Design.
Table 3.
Non-inferiority margin for seroresponse rates comparison.
Table 4.
NI Margin—Advantages and Disadvantages.
Table 5.
Vaccinated Populations.
Table 6.
Concomitant delivery of vaccines, vitamins, and micronutrients.
Table 7.
Manufacturing and Shelf Life.
Table 8.
Evaluation of Immune Responses.
4. Additional Recommendations to Support the MR-MAP Pathway to Policy Recommendation and Programmatic Use
Additional data and evidence were identified during the stakeholder discussions on the pivotal Phase III trial design. Such evidence would inform and then expand policy recommendations and support programmatic implementation post initial regulatory licensure and policy.
4.1. Other Studies (Descriptive/Post-Market/Implementation)
Given that at least initially, MR-MAPs are expected to be used in outreach delivery and supplementary immunization activities, data pertaining to older ages, beyond 15–18 months, are likely to be required for licensure and policy decisions. Upon agreement with NRAs and WHO PQ, descriptive analyses of safety and immunogenicity in children up to five years of age could be sufficient to inform MR-MAP use in outreach and campaigns for this age range and older and could be added to the product label. After product licensure, safety and immunogenicity data could also be collected in infants younger than nine months or to evaluate interference with concomitantly delivered vaccines (with emphasis on live vaccines such as YF, polio, and JE). As such, MR-MAP developers and global health stakeholders should consider conducting additional informative clinical studies outside of the pivotal Phase III trial. In addition, if moderately to severely malnourished and HIV+ children are excluded from the trial, data demonstrating safety and immunogenicity of MR-MAPs should be collected in parallel research studies to inform a policy decision.
From a programmatic implementation perspective, it is vital to engage with Gavi-supported, self-procuring countries, other countries utilizing MRV, or those interested in the use of MR-MAP early to design and conduct implementation studies (both pre- and post-licensure) to evaluate MR-MAP’s ability to reach zero-dose children and reach other programmatic benefits, key elements of the value proposition. Prior to the Phase III pivotal trial, it is recommended to conduct research studies to evaluate that the anatomical application site or sites are safe, immunogenic, have suitable biomechanical properties to enable efficient MAP delivery, and are acceptable by health workers and caregivers. The MR-MAP application sites could be the wrist, anterolateral thigh, and/or the deltoid, for example. However, this must be confirmed in prior studies. Implementation research in parallel to the Phase III trial is required to provide program design learnings, prospective impact assessment, and other evidence required to inform integration of MR-MAPs into countries’ immunization programs. The completed, ongoing, and planned evaluations of the switch to 5-dose MRV will be an important reference for planning such research for MR-MAPs [82,83,84]. The WHO is leading the work in identifying and prioritizing implementation research questions, which will further enrich the existing knowledge and prepare for programmatic introduction [85].
4.2. Manufacturing, Regulatory and Policy Considerations
Defining the MAHs will be critical to advancing the timeline to regulatory submission, licensure, and commercial manufacture to generate supply for programmatic introduction. The MAH should engage with regulatory authorities and policymakers to align the regulatory and clinical strategies. The MR-MAP is a novel vaccine product, with its unique biologic-device combination configuration, and there are no existing specific guidelines from regulators or from the WHO, which is an important implication for a regulatory pathway.
The WHO Technical Report Series (TRS) includes guidelines about vaccine quality assurance and inform WHO prequalification of vaccines [24], which is required for the use of vaccines in LMICs, financed by Gavi, or procured by UNICEF. There are two WHO TRS documents relevant to the MR-MAP: TRS 840 [22] and TRS 1004 [23]. TRS 840’s manufacturing requirements sections for measles (pages 105–121) and rubella (pages 137–152) may need to be edited to accommodate the different manufacturing processes and platforms for MR-MAPs. Ideally, such revision would occur before manufacturing of Phase III clinical material, to ensure compliance with proposed standards for both the drug product and the device components, as Phase III clinical material are expected to be representative of initial launch material.
Another consideration is the WHO programmatic suitability criteria for the PQ of the vaccine [31], which were developed taking into account vial presentation and syringe reconstitution and delivery. MR-MAP vaccines should meet the mandatory criteria; however, a revision to this document may be valuable in order to take into account specific aspects of MR-MAP devices [31].
The NRAs targeted for initial licensure and for Phase III conduct will need to opine on the overall design of the pivotal Phase III trial, including the critical questions of immunologic endpoints and their NI margins. Those areas not addressed in the Phase III design could be included in additional Phase III studies or research post-licensure as noted above. Discussions with NRAs and WHO PQ need to include aspects related to manufacturing consistency, specifications for lot release, and end-of-shelf life (EOSL) potency. Given that current MR vaccines are primarily produced in India, the CDSCO will likely play a critical role in the regulatory licensure of MR-MAP products. Importantly, if the Phase III trial is conducted in India, a Phase II leading arm might be considered for addition to the trial to address the need for a Phase II/III bridging trial with Indian infants and children for licensure of vaccines imported or from technology transfer (as opposed to domestic development).
After regulatory licensure and pending WHO PQ, MR-MAPs will require a policy recommendation from global or country stakeholders to allow for MR-MAP introduction and use in countries. The WHO, informed by the Strategic Advisory Group of Experts on Immunization (SAGE), can issue a policy decision on MR-MAPs, allowing for their financing by Gavi and procurement by UNICEF. To determine appropriate data to inform policy, SAGE considers the evidence-to-recommendations tables [29] and the ECVP [30]. Data showing MAP impact and cost-effectiveness modeling will likely be required for the policy. However, it is recognized that increased coverage cannot be demonstrated before MAPs are licensed and deployed. Data showing the acceptability and feasibility of health workers’ use of MAPs, acceptability in zero-dose populations, other programmatic benefits, and ability to reach remote populations, together with modeling, could be used to inform policy decisions.
5. Conclusions
It is anticipated that MR-MAPs will play a vital role in immunization programs, particularly in reaching zero-dose children through outreach and campaign efforts, addressing the coverage gap for MRVs, and contributing to MR elimination. The proposed Phase III trial framework attempts to align regulatory, policy, and immunization program needs and is intended to address the recommendations from the MR-MAP TAG, other key stakeholders, regulatory, and WHO PQ and policy requirements. The proposed framework has also been developed to anticipate and prevent potential challenges associated with the design and running of a clinical trial, particularly in LMICs, such as inclusion of appropriate populations, or ensuring that the non-inferiority margin is appropriately defined and measured. This manuscript focuses on aspects related to the design of the Phase III clinical trial for MR-MAPs and other important considerations common to all vaccine trials, such as regulatory and ethical consultations, site selection, staff training, participant recruitment, and logistics, are addressed through adherence to international guidelines, and not discussed here [86].
The pivotal Phase III trial, which should be an individually randomized (1:1), open-label NI trial to receive an MR-MAP or MR-SC at 9–10 months of age to assess safety and non-inferiority of immunogenicity of MR vaccines delivered by a MAP, six weeks after the first dose of the MR vaccine. Dependent upon the NRA and the WHO PQ team review and agreement of the proposed pivotal Phase III trial framework, the trial could continue in a subset of children who would be randomized to receive either the same vaccine presentation or a different vaccine presentation 6 months after the first MR dose, at 15–16 months of age. The trial should be conducted in countries where MR-MAPs are to be utilized programmatically and in representative populations regarding health status, informed by the use cases and projected demand for the product in LMICs.
The relevant NRAs and WHO PQ should confirm the acceptability of the proposed immunogenicity endpoints and their NI margin as part of the overall clinical data set that will be submitted for regulatory approval and should opine on the overall Phase III trial design. Consultations involving both NRAs and the WHO PQ team concurrently should be favored to minimize delays to Phase III start.
In addition to the pivotal Phase III trial, additional clinical studies may be required to meet regulatory, WHO or programmatic needs for MR-MAPs. Such studies could address different age groups outside of the 9 to 16-month-old age group, such as younger infants (down to 6 months old) or older children and adults. The studies could also address the safety and immunogenicity of MR-MAPs in moderately-to-severely malnourished children, should they be excluded from the Phase III trial. Concomitant vaccine administration, with priority live virus vaccines that may present the potential for interference, may also need to be addressed. Such studies may be possible pre- or post-licensure, depending upon the final clinical and regulatory strategy.
Determination of the MAH and Phase III trial sponsor will be vital to advancing MR-MAPs through the regulatory licensure process and WHO PQ, and eventual commercialization, ensuring sufficient supply for programmatic introduction. Ideally, this responsibility should be taken on by a manufacturer of prequalified MR vaccines. The NRAs for initial licensure and WHO PQ team will need to address outstanding questions regarding regulatory requirements for quality aspects (manufacturing, controls) of the biological and the device components of MR-MAPs.
Pathways to facilitate joint NRA and WHO PQ reviews such as the EMA M4-all should be explored to determine alignment with an MR-MAP regulatory and marketing strategy. However, before implementing a pivotal Phase III trial, completing MR-MAP device design development will be critical to address issues such as human factors, application site(s), wear time, and cGMP compliant manufacturing facilities. Validation of manufacturing and controls in such facilities is required to produce the Phase III clinical product and prepare for the regulatory licensure process, WHO PQ, and meeting the initial product demand once it is ready for immunization program use. From a WHO policy perspective, the development of the WHO ECVP should be advanced to identify data and evidence to support policy needs, building upon this Phase III framework that describes the parameters for a pivotal licensure trial.
Author Contributions
M.H.-A. and B.G. secured the funding; D.Z., M.H.-A. and B.G. developed the approach to developing the Phase III trial framework; all authors were involved in the preparation and running of the global convening and breakout groups; D.Z., M.H.-A. and B.G. wrote the first draft. All authors reviewed and approved the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was funded by the Bill & Melinda Gates Foundation grant (INV-005318) and a grant from the Foreign, Commonwealth & Development Office (FCDO), (award HQUHL2221008/1.2.1/68566 to the World Health Organization.
Institutional Review Board Statement
Under WHO procedures, this study was exempt from ethical review because (1) research activities pose minimal risk to participants and (2) participants were asked to provide only objective information or professional opinion on a topic under their direct responsibility or expertise, with their expressed knowledge and consent, and without providing any private individual opinions or opinions on matters outside their direct expertise.
Informed Consent Statement
Not applicable. The study did not involve humans.
Data Availability Statement
The data presented in this study are available in this article.
Acknowledgments
The authors would like to acknowledge the participation of stakeholders interviewed, the global convening attendees, and the MR-MAP TAG for their contributions to the framework design. The authors would like to particularly acknowledge the experts who have reviewed the article and provided feedback: Jon Abramson, Jean-Pierre Amorij, Ben Baker, Marco Cavaleri, Kristen Earle, Matthew Hanson, Ravi Menon, Parag Nagarkar, Mark Papania, Paul Rota, and Tiziana Scarna.
Conflicts of Interest
The authors declare no conflicts of interest.
Author Disclaimer
The findings and conclusions in this article are those of the authors and do not represent the official position of the World Health Organization. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention.
References
- Minta, A.A.; Ferrari, M.; Antoni, S.; Portnoy, A.; Sbarra, A.; Lambert, B.; Hatcher, C.; Hsu, C.H.; Ho, L.L.; Steulet, C.; et al. Progress Toward Measles Elimination—Worldwide, 2000–2022. MMWR Morb. Mortal Wkly. Rep. 2023, 72, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- WHO. Immunization Coverage. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 19 August 2024).
- WHO. Measles Vaccines: WHO Position Paper—2017. Wkly. Epidemiol. Rec. 2017, 92, 205–227. [Google Scholar]
- WHO. Rubella vaccines: WHO position paper—July 2020. Wkly. Epidemiol. Rec. 2020, 95, 27. [Google Scholar]
- Ou, A.C.; Zimmerman, L.A.; Alexander, J.P., Jr.; Crowcroft, N.S.; O’Connor, P.M.; Knapp, J.K. Progress Toward Rubella and Congenital Rubella Syndrome Elimination—Worldwide, 2012–2022. MMWR Morb. Mortal Wkly. Rep. 2024, 73, 162–167. [Google Scholar] [CrossRef]
- Vynnycky, E.; Knapp, J.K.; Papadopoulos, T.; Cutts, F.T.; Hachiya, M.; Miyano, S.; Reef, S.E. Estimates of the global burden of Congenital Rubella Syndrome, 1996–2019. Int. J. Infect. Dis. 2023, 137, 149–156. [Google Scholar] [CrossRef]
- WHO. WHO Policy Statement: Multi-Dose Vial Policy (MDVP). Revision 2014; Handling of Multi-Dose Vaccine Vials After Opening; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- Mvundura, M.; Ng, J.; Reynolds, K.; Theng Ng, Y.; Bawa, J.; Bambo, M.; Bonsu, G.; Payne, J.; Chua, J.; Guerette, J.; et al. Vaccine wastage in Ghana, Mozambique, and Pakistan: An assessment of wastage rates for four vaccines and the context, causes, drivers, and knowledge, attitudes and practices for vaccine wastage. Vaccine 2023, 41, 4158–4169. [Google Scholar] [CrossRef]
- Hasso-Agopsowicz, M. Exploring important attributes, the potential use-cases and feasibility of introduction of measles and rubella microarray patches (MR-MAPs): Insights from nine countries. Vaccines 2024, 12, 1084. [Google Scholar] [CrossRef]
- WHO; UNICEF. Measles-Rubella Microarray Patch (MR–MAP) Target Product Profile; WHO: Geneva, Switzerland, 2019. [Google Scholar]
- Prausnitz, M.R.; Goodson, J.L.; A Rota, P.; A Orenstein, W. A microneedle patch for measles and rubella vaccination: A game changer for achieving elimination. Curr. Opin. Virol. 2020, 41, 68–76. [Google Scholar] [CrossRef]
- Fu, H.; Abbas, K.; Malvolti, S.; Gregory, C.; Ko, M.; Amorij, J.P.; Jit, M. Impact and cost-effectiveness of measles vaccination through microarray patches in 70 low-income and middle-income countries: Mathematical modelling and early-stage economic evaluation. BMJ Glob. Health 2023, 8, e012204. [Google Scholar] [CrossRef]
- Malvolti, S.; Ko, M.; Menozzi-Arnaud, M.; Mantel, C.; Jarrahian, C.; Amorij, J.P.; Giersing, B.; Hasso-Agopsowicz, M. Exploring potential applications of measles and rubella microarray patches (MR-MAPs): Use case identification. Front. Public Health 2023, 11, 1165110. [Google Scholar] [CrossRef]
- Scarnà, T.; Menozzi-Arnaud, M.; Friede, M.; DeMarco, K.; Plopper, G.; Hamer, M.; Chakrabarti, A.; Gilbert, P.A.; Jarrahian, C.; Mistilis, J.; et al. Accelerating the development of vaccine microarray patches for epidemic response and equitable immunization coverage requires investment in microarray patch manufacturing facilities. Expert Opin. Drug Deliv. 2023, 20, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Gavi. Vaccine Microarray Patches (MAPs): Public Summary of the VIPS Alliance Action Plan; Vaccine Innovation Prioritisation Strategy: Geneva, Switzerland, 2021. [Google Scholar]
- Gavi. Vaccine Innovation Prioritisation Strategy (VIPS). 2020. Available online: https://www.gavi.org/our-alliance/market-shaping/vaccine-innovation-prioritisation-strategy (accessed on 19 August 2024).
- Measles & Rubella Partnership. Measles & Rubella Strategic Framework 2021–2030; Measles and Rubella Partnership: Geneva, Switzerland, 2020. [Google Scholar]
- Adigweme, I.; Akpalu, E.; Yisa, M.; Donkor, S.; Jarju, L.B.; Danso, B.; Mendy, A.; Jeffries, D.; Njie, A.; Bruce, A.; et al. Study protocol for a phase 1/2, single-centre, double-blind, double-dummy, randomized, active-controlled, age de-escalation trial to assess the safety, tolerability and immunogenicity of a measles and rubella vaccine delivered by a microneedle patch in healthy adults (18 to 40 years), measles and rubella vaccine-primed toddlers (15 to 18 months) and measles and rubella vaccine-naive infants (9 to 10 months) in The Gambia [Measles and Rubella Vaccine Microneedle Patch Phase 1/2 Age De-escalation Trial]. Trials 2022, 23, 775. [Google Scholar] [PubMed]
- Adigweme, I.; Yisa, M.; Ooko, M.; Akpalu, E.; Bruce, A.; Donkor, S.; Jarju, L.B.; Danso, B.; Mendy, A.; Jeffries, D.; et al. A measles and rubella vaccine microneedle patch in The Gambia: A phase 1/2, double-blind, double-dummy, randomised, active-controlled, age de-escalation trial. Lancet 2024, 403, 1879–1892. [Google Scholar] [CrossRef] [PubMed]
- Baker, B.; Bermingham, I.M.; Leelasena, I.; Hickling, J.; Young, P.R.; Muller, D.A.; Forster, A.H. Safety, Tolerability, and Immunogenicity of Measles and Rubella Vaccine Delivered with a High-Density Microarray Patch: Results from a Randomized, Partially Double-Blinded, Placebo-Controlled Phase I Clinical Trial. Vaccines 2023, 11, 1725. [Google Scholar] [CrossRef]
- WHO. Meeting Report: WHO PDVAC Meeting on MR-MAPs; WHO: Geneva, Switzerland, 2023. [Google Scholar]
- WHO. Requirements for Measles, Mumps and Rubella Vaccines and Combined Vaccine (Live); Technical Report Series; No. 840, Annex 3; WHO: Geneva, Switzerland, 1994. [Google Scholar]
- WHO. Guidelines on Clinical Evaluation of Vaccines: Regulatory Expectations; Technical Report Series; No. 1004, Annex 9; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- WHO. Procedure or Assessing the Acceptability, in Principle, of Vaccines for Purchase by United Nations Agencies; Technical Report Series 978; Annex 6; WHO: Geneva, Switzerland, 2013. [Google Scholar]
- WHO. Guidelines for Independent Lot Release of Vaccines by Regulatory Authorities; Technical Report Series; No. 978, Annex 2; WHO: Geneva, Switzerland, 2010. [Google Scholar]
- WHO. WHO Expert Committee on Biological Standardization; 67th Report: WHO TRS No. 1004; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- SIIL. Measles and Rubella Vaccine. Live, Attenuated (Freeze-Dried) Package Insert. 2021. Available online: https://extranet.who.int/prequal/sites/default/files/vwa_vaccine/pq_138_139_140_141_MR_SII_PI-UNICEF_2022.pdf (accessed on 19 August 2024).
- BiologicalE. Measles and Rubella Vaccine (Live) (Attenuated, Freeze Dried). Package Insert. 2019. Available online: https://extranet.who.int/prequal/sites/default/files/vwa_vaccine/pq_343_344_345_MR_BiolE_PI-2019.pdf (accessed on 19 August 2024).
- WHO. Development of WHO Immunization Policy and Strategic Guidance. Methods and Processes Applied by the Strategic Advisory Group of Experts on Immunization (SAGE) to Develop Evidence-based Recommendations; WHO: Geneva, Switzerland, 2024. [Google Scholar]
- WHO. WHO Evidence Considerations for Vaccine Policy Development (ECVP): Generic Framework for Vaccines/Monoclonal Antibodies in Development; WHO: Geneva, Switzerland, 2022. [Google Scholar]
- WHO. Assessing the Programmatic Suitability of Vaccine Candidates for WHO Prequalification; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- WHO. Prequalification of Medical Products. Vaccines. Guidance Documents. 2024. Available online: https://extranet.who.int/prequal/vaccines/guidance-documents (accessed on 19 August 2024).
- WHO. PQS Independent Type-Testing Protocol. Vaccine Vial Monitor; WHO/PQS/E006/IN05-VP.3; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- WHO. Annex 5. Guidelines on the Stability Evaluation of Vaccines for Use Under Extended Controlled Temperature Conditions; WHO: Geneva, Switzerland, 2016. [Google Scholar]
- EMA. Public Guidance. Parallel Application for EU-M4all (Article 58) Opinion and Centralised Marketing Authorisation Procedure. Promoting EU-Medicines4all; EMA/104275/2021; EMA: Amsterdam, The Netherlands, 2021. [Google Scholar]
- EMA. Guideline on the Choice of the Non-Inferiority Margin; EMA: Amsterdam, The Netherlands, 2005. [Google Scholar]
- EMA. Guideline on Clinical Evaluation of Vaccines; EMAEMA: Amsterdam, The Netherlands, 2023. [Google Scholar]
- EMA. ICH Topic E9 Statistical Principles for Clinical Trials; (CPMP/ICH/363/96); EMA: Amsterdam, The Netherlands, 1998. [Google Scholar]
- EMA. ICH Topic E10 Choice of Control Group in Clinical Trials; (CPMP/ICH/364/96); EMA: Amsterdam, The Netherlands, 2001. [Google Scholar]
- EMA. ICH Guideline E8 (R1) on General Considerations for Clinical Studies; EMA: Amsterdam, The Netherlands, 2021. [Google Scholar]
- CDSCO. Draft Regulatory Guidelines for Development of Vaccines with Special Consideration for COVID-19 Vaccine; CDSCO: New Delhi, India, 2023. [Google Scholar]
- CDSCO. The New Drugs and Clinical Trials Rules, 2019; G.o.I. Ministry of Health and Family Welfare: New Delhi, India, 2023. [Google Scholar]
- USFDA. Non-inferiority Clinical Trials to Establish Effectiveness. Guidance for Industry; USFDA: Silver Spring, MD, USA, 2016. [Google Scholar]
- USFDA. Application of Human Factors Engineering Principles for Combination Products: Questions and Answers. Guidance for Industry and FDA Staff; USFDA: Silver Spring, MD, USA, 2023. [Google Scholar]
- USFDA. Bridging for Drug-Device and Biologic-Device Combination Products. Guidance for Industry; USFDA: Silver Spring, MD, USA, 2019. [Google Scholar]
- USFDA. Guidance for Industry and FDA Staff: Current Good Manufacturing Practice Requirements for Combination Products; USFDA: Silver Spring, MD, USA, 2015. [Google Scholar]
- USFDA. Demonstrating Substantial Evidence of Effectiveness for Human Drug and Biological Products Guidance for Industry; USFDA: Silver Spring, MD, USA, 2019. [Google Scholar]
- AVAREF. African Vaccine Regulatory Forum (AVAREF)—Joint Review Process; AVAREF: Entebbe, Uganda, 2020. [Google Scholar]
- Nic Lochlainn, L.M.; de Gier, B.; van der Maas, N.; Strebel, P.M.; Goodman, T.; van Binnendijk, R.S.; E de Melker, H.; Hahné, S.J.M. Immunogenicity, effectiveness, and safety of measles vaccination in infants younger than 9 months: A systematic review and meta-analysis. Lancet Infect. Dis. 2019, 19, 1235–1245. [Google Scholar] [CrossRef]
- Hasso-Agopsowicz, M.; Crowcroft, N.; Biellik, R.; Gregory, C.J.; Menozzi-Arnaud, M.; Amorij, J.P.; Gilbert, P.A.; Earle, K.; Frivold, C.; Jarrahian, C.; et al. Accelerating the Development of Measles and Rubella Microarray Patches to Eliminate Measles and Rubella: Recent Progress, Remaining Challenges. Front. Public Health 2022, 10, 809675. [Google Scholar] [CrossRef]
- Bavdekar, A.; Oswal, J.; Ramanan, P.V.; Aundhkar, C.; Venugopal, P.; Kapse, D.; Miller, T.; McGray, S.; Zehrung, D.; Kulkarni, P.S.; et al. Immunogenicity and safety of measles-mumps-rubella vaccine delivered by disposable-syringe jet injector in India: A randomized, parallel group, non-inferiority trial. Vaccine 2018, 36, 1220–1226. [Google Scholar] [CrossRef]
- Low, N.; Bavdekar, A.; Jeyaseelan, L.; Hirve, S.; Ramanathan, K.; Andrews, N.J.; Shaikh, N.; Jadi, R.S.; Rajagopal, A.; Brown, K.E.; et al. A Randomized, Controlled Trial of an Aerosolized Vaccine against Measles. N. Engl. J. Med. 2015, 372, 1519–1529. [Google Scholar] [CrossRef]
- Henao-Restrepo, A.M.; Greco, M.L.X.; John, O.; Aguado, T. WHO Product Development Group for Measles Aerosol Project. Measles Aerosol Project; WHO: Geneva, Switzerland, 2010; Volume 2, pp. 147–150. [Google Scholar]
- Castro, J.F.; Bennett, J.V.; Rincon, H.G.; Munoz, M.T.; Sanchez, L.A.; Santos, J.I. Evaluation of immunogenicity and side effects of triple viral vaccine (MMR) in adults, given by two routes: Subcutaneous and respiratory (aerosol). Vaccine 2005, 23, 1079–1084. [Google Scholar] [CrossRef]
- Díaz-Ortega, J.L.; Bennett, J.V.; Castañeda, D.; Martinez, D.; de Castro, J.F. Antibody persistence in young adults 1 year after MMR immunization by aerosol or by subcutaneous route. Vaccine 2010, 28, 7228–7232. [Google Scholar] [CrossRef]
- Diaz-Ortega, J.L.; Bennett, J.V.; Castaneda, D.; Vieyra, J.-R.; Valdespino-Gomez, J.L.; de Castro, J.F. Successful seroresponses to measles and rubella following aerosolized Triviraten vaccine, but poor response to aerosolized mumps (Rubini) component: Comparisons with injected MMR. Vaccine 2010, 28, 692–698. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Ortega, J.-L.; Bennett, J.V.; Castañeda-Desales, D.; Quintanilla, D.-M.A.; Martínez, D.; de Castro, J.F. Booster immune response in children 6–7 years of age, randomly assigned to four groups with two MMR vaccines applied by aerosol or by injection. Vaccine 2014, 32, 3680–3686. [Google Scholar] [CrossRef] [PubMed]
- Wong-Chew, R.M.; García-León, M.L.; Torrija, B.E.-T.; Hernández-Pérez, B.; Cardiel-Marmolejo, L.E.; Beeler, J.A.; Audet, S.; Santos-Preciado, J.I. Increasing the time of exposure to aerosol measles vaccine elicits an immune response equivalent to that seen in 9-month-old Mexican children given the same dose subcutaneously. J. Infect. Dis. 2011, 204, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Wong-Chew, R.M.; Islas-Romero, R.; García-García, M.d.L.; Beeler, J.A.; Audet, S.; Santos-Preciado, J.I.; Gans, H.; Lew-Yasukawa, L.; Maldonado, Y.A.; Arvin, A.M.; et al. Immunogenicity of aerosol measles vaccine given as the primary measles immunization to nine-month-old Mexican children. Vaccine 2006, 24, 683–690. [Google Scholar] [CrossRef]
- Wong-Chew, R.M.; Islas-Romero, R.; García-García, M.d.L.; Beeler, J.A.; Audet, S.; Santos-Preciado, J.I.; Gans, H.; Lew-Yasukawa, L.; Maldonado, Y.A.; Arvin, A.M. Induction of cellular and humoral immunity after aerosol or subcutaneous administration of Edmonston-Zagreb measles vaccine as a primary dose to 12-month-old children. J. Infect. Dis. 2004, 189, 254–257. [Google Scholar] [CrossRef]
- Sepúlveda-Amor, J.; Valdespino-Gómez, J.L.; García-García, M.d.L.; Bennett, J.; Islas-Romero, R.; Echaniz-Aviles, G.; de Castro, J.F. A randomized trial demonstrating successful boosting responses following simultaneous aerosols of measles and rubella (MR) vaccines in school age children. Vaccine 2002, 20, 2790–2795. [Google Scholar] [CrossRef]
- Dilraj, A.; Cutts, F.T.; de Castro, J.F.; Wheeler, J.G.; Brown, D.; Roth, C.; Coovadia, H.M.; Bennett, J.V. Response to different measles vaccine strains given by aerosol and subcutaneous routes to schoolchildren: A randomised trial. Lancet 2000, 355, 798–803. [Google Scholar] [CrossRef]
- Dilraj, A.; Sukhoo, R.; Cutts, F.T.; Bennett, J.V. Aerosol and subcutaneous measles vaccine: Measles antibody responses 6 years after re-vaccination. Vaccine 2007, 25, 4170–4174. [Google Scholar] [CrossRef]
- Klein, N.P.; Abu-Elyazeed, R.; Povey, M.; Parra, M.M.; Diez-Domingo, J.; Ahonen, A.; Korhonen, T.; Tinoco, J.-C.; Weiner, L.; Marshall, G.S.; et al. Immunogenicity and Safety of a Measles-Mumps-Rubella Vaccine Administered as a First Dose to Children Aged 12 to 15 Months: A Phase III, Randomized, Noninferiority, Lot-to-Lot Consistency Study. J. Pediatr. Infect. Dis. Soc. 2020, 9, 194–201. [Google Scholar] [CrossRef]
- Vesikari, T.; Becker, T.; Gajdos, V.; Fiquet, A.; Thomas, S.; Richard, P.; Baudin, M. Immunogenicity and safety of a two-dose regimen of a combined measles, mumps, rubella and varicella live vaccine (ProQuad(®)) in infants from 9 months of age. Vaccine 2012, 30, 3082–3089. [Google Scholar] [CrossRef]
- Sood, A.; Mitra, M.; Joshi, H.A.; Nayak, U.S.; Siddaiah, P.; Babu, T.R.; Mahapatro, S.; Sanmukhani, J.; Gupta, G.; Mittal, R.; et al. Immunogenicity and safety of a novel MMR vaccine (live, freeze-dried) containing the Edmonston-Zagreb measles strain, the Hoshino mumps strain, and the RA 27/3 rubella strain: Results of a randomized, comparative, active controlled phase III clinical trial. Hum. Vaccin. Immunother. 2017, 13, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Santos, E.M.D.; Noronha, T.G.; Alves, I.S.; Cruz, R.L.S.; Ferroco, C.L.V.; Brum, R.C.; Oliveira, P.M.N.; Siqueira, M.M.; Lima, M.C.; Ramos, F.L.P.; et al. Immunogenicity and safety of the combined vaccine for measles, mumps, and rubella isolated or combined with the varicella component administered at 3-month intervals: Randomised study. Mem. Inst. Oswaldo Cruz 2019, 114, e180517. [Google Scholar] [CrossRef] [PubMed]
- Thuluva, S.; Gunneri, S.; Turaga, K.; Mogulla, R.R.; Yerroju, V.; Peta, K.; Suneetha, P.V.; Matur, R.V. A phase II/III randomised, comparative study evaluating the safety and immunogenicity of Biological E’s live, attenuated Measles-Rubella vaccine in 9–12 month old healthy infants. Contemp. Clin. Trials Commun. 2023, 36, 101232. [Google Scholar] [CrossRef] [PubMed]
- USNIH. Division of AIDS (DAIDS) Table for Grading the Severity of Adult and Pediatric Adverse Events; USNIH: Bethesda, MD, USA, 2017. [Google Scholar]
- Donken, R.; de Melker, H.; Rots, N.; Berbers, G.; Knol, M. Comparing vaccines: A systematic review of the use of the non-inferiority margin in vaccine trials. Vaccine 2015, 33, 1426–1432. [Google Scholar] [CrossRef]
- Cavaleri, M. MR-MAP considerations. In WHO Global Convening on Measles-Rubella Microarray Patches (MR-MAPs); WHO: Geneva, Switzerland, 2024. [Google Scholar]
- WHO. Measles. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/measles (accessed on 19 August 2024).
- Mutsaerts, E.A.; Nunes, M.C.; van Rijswijk, M.N.; Klipstein-Grobusch, K.; Grobbee, D.E.; Madhi, S.A. Safety and Immunogenicity of Measles Vaccination in HIV-Infected and HIV-Exposed Uninfected Children: A Systematic Review and Meta-Analysis. EClinicalMedicine 2018, 1, 28–42. [Google Scholar] [CrossRef]
- Seth, A.; Deepa, S.; Dutta, R.; Chandra, J. Evaluation of Immune Response to Measles Component of MMR Vaccine in Children with HIV Infection Receiving Antiretroviral Therapy. Pediatr. Infect. Dis. J. 2016, 35, e8–e11. [Google Scholar] [CrossRef]
- WHO. Guideline: Vitamin A Supplementation in Infants and Children 6–59 Months of Age; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- WHO. WHO Recommendations on Child Health. Guidelines Approved by the WHO Guidelines Review Committee; WHO: Geneva, Switzerland, 2017. [Google Scholar]
- WHO. Vitamin A Supplementation. 2024. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/integration/linking-with-other-health-interventions/vitamin-a#:~:text=%2AVitamin%20A%20can%20be%20stored%20in%20the%20liver%2C,treat%20clinical%20vitamin%20A%20deficiency%20and%20measles%20cases (accessed on 19 August 2024).
- MMR-162 Study Group. Safety and immunogenicity of an upper-range release titer measles-mumps-rubella vaccine in children vaccinated at 12 to 15 months of age: A phase III, randomized study. Hum. Vaccines Immunother. 2018, 14, 2921–2931. [Google Scholar] [CrossRef]
- Jarrahian, C. MR-MAP Phase II; Zehrung, D., Ed.; WHO: Geneva, Switzerland, 2024. [Google Scholar]
- van den Boogaard, J.; de Gier, B.; Lima, P.d.O.B.; Desai, S.; de Melker, H.E.; Hahné, S.J.; Veldhuijzen, I.K. Immunogenicity, duration of protection, effectiveness and safety of rubella containing vaccines: A systematic literature review and meta-analysis. Vaccine 2021, 39, 889–900. [Google Scholar] [CrossRef]
- Coughlin, M.M.; Matson, Z.; Sowers, S.B.; Priest, J.W.; Smits, G.P.; van der Klis, F.R.M.; Mitchell, A.; Hickman, C.J.; Scobie, H.M.; Goodson, J.L.; et al. Development of a Measles and Rubella Multiplex Bead Serological Assay for Assessing Population Immunity. J. Clin. Microbiol. 2021, 59, 889–900. [Google Scholar] [CrossRef]
- Krudwig, K.; Knittel, B.; Karim, A.; Kanagat, N.; Prosser, W.; Phiri, G.; Mwansa, F.; Steinglass, R. The effects of switching from 10 to 5-dose vials of MR vaccine on vaccination coverage and wastage: A mixed-method study in Zambia. Vaccine 2020, 38, 5905–5913. [Google Scholar] [CrossRef]
- Oo, A.N.; Thekkur, P.; Thar, A.M.C.; Htet, K.K.K.; Lin, H.H. Small Session Size and Big Vial Size: Operational Research Assessing Open Vial Vaccine Wastage at the Service Delivery Points in the Mandalay Region of Myanmar During 2018. Trop. Med. Infect. Dis. 2020, 5, 60. [Google Scholar] [CrossRef] [PubMed]
- Wedlock, P.T.; Mitgang, E.A.; Haidari, L.A.; Prosser, W.; Brown, S.T.; Krudwig, K.; Siegmund, S.S.; DePasse, J.V.; Bakal, J.; Leonard, J.; et al. The value of tailoring vial sizes to populations and locations. Vaccine 2019, 37, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Sá Silva, S. MR-MAPs Implementation Research Agenda: A framework to identify priority implementation research questions for MR-MAPs. In MR-MAP Global Convening; WHO: Geneva, Switzerland, 2024. [Google Scholar]
- Saluja, T.; Giri, B.R.; Chaudhary, S.; Tamrakar, D.; Kanodia, P.; Palkar, S.; Vemula, S.; Chinaworapong, S.; Kim, B.; Gupta, B.P.; et al. Challenges and opportunities in setting up a phase III vaccine clinical trial in resource limited settings: Experience from Nepal. Hum. Vaccines Immunother. 2021, 17, 2149–2157. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).