
Lessons from Recent Measles Post-Campaign Coverage Surveys Worldwide

 ,
,  , , and
, , and
Abstract
1. Background
2. Methods
3. Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shattock, A.J.; Johnson, H.C.; Sim, S.Y.; Carter, A.; Lambach, P.; Hutubessy, R.C.W.; Thompson, K.M.; Badizadegan, K.; Lambert, B.; Ferrari, M.J.; et al. Contribution of vaccination to improved survival and health: Modelling 50 years of the Expanded Programme on Immunization. Lancet 2024, 403, 2307–2316. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Measles vaccines: WHO position paper. Wkly. Epidemiol. Rec. 2017, 92, 205–227. [Google Scholar]
- World Health Organization. Planning and Implementing High-Quality Supplementary Immunization Activities for Injectable Vaccines: Using an Example of Measles-Rubella Vaccines—Field Guide; WHO: Geneva, Switzerland, 2016; Available online: https://www.who.int/publications/i/item/9789241511254 (accessed on 15 October 2024).
- Strebel, P.; Grabowsky, M.; Hoekstra, E.; Gay, A.; Cochi, S. Evolution and Contribution of a Global Partnership against Measles and Rubella, 2001–2023. Vaccines 2024, 12, 693. [Google Scholar] [CrossRef] [PubMed]
- De Quadros, C.A.; Hersh, B.S.; Nogueira, A.C.; A Carrasco, P.; Da Silveira, C.M. Measles eradication: Experience in the Americas. Bull. World Health Organ. 1998, 76 (Suppl. 2), 47–52. [Google Scholar] [PubMed]
- Verguet, S.; Johri, M.; Morris, S.K.; Gauvreau, C.L.; Jha, P.; Jit, M. Controlling measles using supplemental immunization activities: A mathematical model to inform optimal policy. Vaccine 2015, 33, 1291–1296. [Google Scholar] [CrossRef]
- Prada, J.; Metcalf, C.; Takahashi, S.; Lessler, J.; Tatem, A.; Ferrari, M. Demographics, epidemiology and the impact of vaccination campaigns in a measles-free world—Can elimination be maintained? Vaccine 2017, 35, 1488–1493. [Google Scholar] [CrossRef]
- Auzenbergs, M.; Fu, H.; Abbas, K.; Procter, S.R.; Cutts, F.T.; Jit, M. Health effects of routine measles vaccination and supplementary immunisation activities in 14 high-burden countries: A Dynamic Measles Immunization Calculation Engine (DynaMICE) modelling study. Lancet Glob. Health 2023, 11, e1194–e1204. [Google Scholar] [CrossRef]
- Portnoy, A.; Jit, M.; Helleringer, S.; Verguet, S. Comparative Distributional Impact of Routine Immunization and Supplementary Immunization Activities in Delivery of Measles Vaccine in Low- and Middle-Income Countries. Value Health 2020, 23, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Portnoy, A.; Jit, M.; Helleringer, S.; Verguet, S. Impact of measles supplementary immunization activities on reaching children missed by routine programs. Vaccine 2018, 36, 170–178. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rosenfeld, K.A.; Frey, K.; McCarthy, K.A. Optimal Timing Regularly Outperforms Higher Coverage in Preventative Measles Supplementary Immunization Campaigns. Vaccines 2024, 12, 820. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yan, L.; Jing, M.; Dapeng, Y. Rubella vaccines: WHO position paper. Wkly. Epidemiol. Rec. 2020, 95, 27. [Google Scholar]
- Ou, A.C.; Zimmerman, L.A.; Alexander, J.P.; Crowcroft, N.S.; O’connor, P.M.; Knapp, J.K. Progress Toward Rubella and Congenital Rubella Syndrome Elimination—Worldwide, 2012–2022. Mmwr-Morb. Mortal. Wkly. Rep. 2024, 73, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Minta, A.A.; Ferrari, M.; Antoni, S.; Portnoy, A.; Sbarra, A.; Lambert, B.; Hatcher, C.; Hsu, C.H.; Ho, L.L.; Steulet, C.; et al. Progress Toward Measles Elimination—Worldwide, 2000–2022. Mmwr-Morbidity Mortal. Wkly. Rep. 2023, 72, 1262–1268. [Google Scholar] [CrossRef] [PubMed]
- Rachlin, A.; Danovaro-Holliday, M.C.; Murphy, P.; Sodha, S.V.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2021. Mmwr-Morbidity Mortal. Wkly. Rep. 2022, 71, 1396–1400. [Google Scholar] [CrossRef]
- Muhoza, P.; Danovaro-Holliday, M.C.; Diallo, M.S.; Murphy, P.; Sodha, S.V.; Requejo, J.H.; Wallace, A.S. Routine Vaccination Coverage—Worldwide, 2020. Mmwr-Morbidity Mortal. Wkly. Rep. 2021, 70, 1495–1500. [Google Scholar] [CrossRef]
- Ho, L.L.; Gurung, S.; Mirza, I.; Nicolas, H.D.; Steulet, C.; Burman, A.L.; Danovaro-Holliday, M.C.; Sodha, S.V.; Kretsinger, K. Impact of the SARS-CoV-2 pandemic on vaccine-preventable disease campaigns. Int. J. Infect. Dis. 2022, 119, 201–209. [Google Scholar] [CrossRef]
- CDC. Global Measles Outbreaks. Global Measles Vaccination. Published 13 May 2024. Available online: https://www.cdc.gov/global-measles-vaccination/data-research/global-measles-outbreaks/index.html (accessed on 15 October 2024).
- e Clinical Medicine Concerning global rise in measles cases. eClinicalMedicine 2024, 68, 102502. [CrossRef]
- Parums, D.V. A Review of the Resurgence of Measles, a Vaccine-Preventable Disease, as Current Concerns Contrast with Past Hopes for Measles Elimination. Med. Sci. Monit. 2024, 30, e944436-1–e944436-10. [Google Scholar] [CrossRef]
- Cutts, F.T.; Danovaro-Holliday, M.C.; Rhoda, D.A. Challenges in measuring supplemental immunization activity coverage among measles zero-dose children. Vaccine 2021, 39, 1359–1363. [Google Scholar] [CrossRef]
- World Health Organization. Vaccination Coverage Cluster Surveys: Reference Manual; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Measles and Measles-Rubella Vaccine Support. Available online: https://www.gavi.org/types-support/vaccine-support/measles-and-measles-rubella (accessed on 15 October 2024).
- Luman, E.T.; Cairns, K.L.; Perry, R.; Dietz, V.; Gittelman, D. Use and abuse of rapid mnitoring to assess coverage during mass vaccination campaigns. Bull. World Health Organ. 2007, 85, 651. [Google Scholar] [CrossRef]
- Kaiser, R.; E Shibeshi, M.; Chakauya, J.M.; Dzeka, E.; Masresha, B.G.; Daniel, F.; Shivute, N. Surveys of measles vaccination coverage in eastern and southern Africa: A review of quality and methods used. Bull. World Health Organ. 2015, 93, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Cutts, F.T.; Izurieta, H.S.; Rhoda, D.A. Measuring Coverage in MNCH: Design, Implementation, and Interpretation Challenges Associated with Tracking Vaccination Coverage Using Household Surveys. PLoS Med. 2013, 10, e1001404. [Google Scholar] [CrossRef] [PubMed]
- Utazi, C.E.; Wagai, J.; Pannell, O.; Cutts, F.T.; Rhoda, D.A.; Ferrari, M.J.; Dieng, B.; Oteri, J.; Danovaro-Holliday, M.C.; Adeniran, A.; et al. Geospatial variation in measles vaccine coverage through routine and campaign strategies in Nigeria: Analysis of recent household surveys. Vaccine 2020, 38, 3062–3071. [Google Scholar] [CrossRef] [PubMed]
- Danovaro-Holliday, M.C.; Dansereau, E.; Rhoda, D.A.; Brown, D.W.; Cutts, F.T.; Gacic-Dobo, M. Collecting and using reliable vaccination coverage survey estimates: Summary and recommendations from the “Meeting to share lessons learnt from the roll-out of the updated WHO Vaccination Coverage Cluster Survey Reference Manual and to set an operational research agenda around vaccination coverage surveys”, Geneva, 18–21 April 2017. Vaccine 2018, 36, 5150–5159. [Google Scholar] [CrossRef] [PubMed]
- Biostat Global Consulting. Vaccination Coverage Quality Indicators (VCQI)—Resources [Internet]. 2024. Available online: http://www.biostatglobal.com/VCQI_RESOURCES.HTML (accessed on 23 August 2024).
- Prier, M.L.; Rhoda, D.A. Organ Pipe Plots for Clustered Datasets—Visualize Disparities in Cluster-Level Coverage [Internet]. Stata Conference 2018; Columbus, Ohio. Available online: https://github.com/BiostatGlobalConsulting/organ-pipe-plots/blob/master/opplot_presentation.pptx (accessed on 23 August 2024).
- Cutts, F.T.; Ferrari, M.J.; Krause, L.K.; Tatem, A.J.; Mosser, J.F. Vaccination strategies for measles control and elimination: Time to strengthen local initiatives. BMC Med. 2021, 19, 2. [Google Scholar] [CrossRef]
- World Health Organization. Measles and Rubella Strategic Framework 2021–2030; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Measles Cases in the AFRO Region. South Sudan. Available online: https://www.afro.who.int/sites/default/files/2024-06/Measles%20Outbreak%20and%20Response%20Weekly%20Situation%20Update_Week%2019%2C%202024.pdf (accessed on 23 August 2024).
- Behavioral and Social Drivers of Immunization. Available online: https://www.who.int/teams/immunization-vaccines-and-biologicals/essential-programme-on-immunization/demand (accessed on 15 October 2024).
- Akpan, G.U.; Mohammed, H.F.; Touray, K.; Kipterer, J.; Bello, I.M.; Ngofa, R.; Stein, A.; Seaman, V.; Mkanda, P.; Cabore, J. Conclusions of the African Regional GIS Summit (2019): Using geographic information systems for public health decision-making. BMC Proc. 2022, 16 (Suppl. 1), 3. [Google Scholar] [CrossRef]
- Utazi, C.E.; Aheto, J.M.; Wigley, A.; Tejedor-Garavito, N.; Bonnie, A.; Nnanatu, C.C.; Wagai, J.; Williams, C.; Setayesh, H.; Tatem, A.J.; et al. Mapping the distribution of zero-dose children to assess the performance of vaccine delivery strategies and their relationships with measles incidence in Nigeria. Vaccine 2022, 41, 170–181. [Google Scholar] [CrossRef]
- Arambepola, R.; Yang, Y.; Hutchinson, K.; Mwansa, F.D.; Doherty, J.A.; Bwalya, F.; Ndubani, P.; Musukwa, G.; Moss, W.J.; Wesolowski, A.; et al. Using geospatial models to map zero-dose children: Factors associated with zero-dose vaccination status before and after a mass measles and rubella vaccination campaign in Southern province, Zambia. BMJ Glob. Health 2021, 6, e007479. [Google Scholar] [CrossRef] [PubMed]
- Gebreslasie, M.T. A review of spatial technologies with applications for malaria transmission modelling and control in Africa. Geospat. Health 2015, 10, 239–247. [Google Scholar] [CrossRef] [PubMed]
- Fatima, M.; O’keefe, K.J.; Wei, W.; Arshad, S.; Gruebner, O. Geospatial Analysis of COVID-19: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 2336. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Seidenberg, A.B.; Moser, R.P.; West, B.T. Preferred Reporting Items for Complex Sample Survey Analysis (PRICSSA). J. Surv. Stat. Methodol. 2023, 11, 743–757. [Google Scholar] [CrossRef]

{kind=link}
| Measles Supplementary Immunization Activities (SIAs) | Post-Campaign Coverage Surveys (PCCSs) | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Basics | Basics | Sampling | |||||||||||||||||||||
| # | Year of PCCS | Country | WHO Region | Target Age Group in Months | Estimated Target Population | Admin Coverage % | SIA Month/Year | Month/Year of Field Work | Delay Between SIA & PCCS (in Months) | Lead Implementer | Ethical Clearance Mentioned | Questionnaire/Data Collection Form Included in Report | # of Clusters Selected/Included | # of Households Interviewed | # of Children Included | Description of Response Rates of Clusters | Description of Response Rates of Households | Primary Sampling Units | Household Enumeration Done | Involvement of NBS/CSO | Data Collection Tools | GPS Coordinates Collected | Software Used for Analysis |
| 1 | 2019 | Democratic People’s Republic of Korea | SEAR | 9 months-15 years old | 5,873,914 | 99.7 | Oct-19 | Winter | NA | Country-led | Yes | Yes | 41 | 1312 (31 HH in each cluster) | 1180 | Yes | Yes | Census enumeration blocks | Yes | Yes | CSPro | No | SPSS |
| 2 | 2019 | Zimbabwe | AFR | 9–59 months | 1,776,546 | 91 | Sep-19 | Nov-19 | 2 months | Not specified | Yes | Yes | 470 | 8110 planned *actual number included missing | 3796 planned *actual number included missing | No | No | Enumeration areas | Yes | Yes | ODK | NR | Stata |
| 3 | 2020 | Burkina Faso | AFR | 9–59 months | 3,078,334 | 106 | Nov-19 | Aug–Sept 2020 | 9–10 months | Independent consultant | Yes | No | 548 | 17,650 | 8457 | Yes | Yes | Enumeration areas | Not mentioned | Sampling frame from NBS | ODK | NA | SPSS and Stata |
| 4 | 2020 | Cameroon | AFR | 9–59 months | 3,339,090 | 92 | Dec-19 | June–July 2020 | 6–7 months | Research Organization | Not mentioned. Informed consent was obtained. | Yes | 396 | 4866 | 4671 | Yes | Yes | Enumeration areas | Yes | Sampling frame from NBS | ODK | Yes | SPSS |
| 5 | 2020 | Ethiopia | AFR | 9–59 months | 14,181,143 | 102.8 | June–July 2020 | Oct 2020–Jan 2021 | 4–6 months | Research Organization | Yes | Yes | 1016 Tigray was excluded | 10,143 | 12,867 | Yes | Yes | Enumeration areas | Yes | Sampling frame from NBS | CSPro | Yes | Stata, VCQI |
| 6 | 2020 | Uganda | AFR | 9 months to less than 15 years old | 18,200,970 | 107 | Oct-19 | Dec 2019–Jan 2020 | 2–3 months | Academic Institution | Yes | No | 363 | 5174 | 12,025 | Yes (written as coverage rate) | Yes | Enumeration areas | Yes | Sampling frame from NBS | ODK | NA | Stata |
| 7 | 2021 | Central African Republic † | AFR | 6–59 months 5–10 years | 1,209,256 | 102 for 6–59 m 85.5 for 5–10 yrs | Phase 1: Mar-2020 Phase 2: Aug-2020 | Dec 2020 Bangui, March–April 2021 rest | 8–11 months | Independent consultant | Yes | Yes | 240 | 3172 | 5674 | Yes | Yes | Enumeration areas | Yes | Sampling frame from NBS | ODK | Yes (difficulties noted) | SPSS |
| 8 | 2021 | Chad | AFR | 9–59 months | 1,792,830 (Phase1) 1,623,518 (Phase2) | 108.8 (Phase1) 107.5 (Phase2) | Jan- 2021 (Phase1) Mar-2021 (Phase2) | Mar–April 2022 | ~1 year | Independent consultant | The survey technical committe considered that the survey was not reasearch and thus it was not needed to present the protocol to an ethical comittee. Informed consent was obtained. | Yes | 695 | 15,793 | 11,601 | Yes | Yes | Enumeration areas, with segmentation | Yes | Yes | ODK | Yes, at least for clusters | SPSS and Stata |
| 9 | 2021 | Democratic Republic of the Congo | AFR | 6–59 months | 18,167,926 | 101.6 | Oct-Dec 2019 | Nov–Dec 2021 | ~2 years | Independent consultant | Yes | Yes | 728 | 81,740 | 21,575 | Yes | Yes | Enumeration areas | Yes | Yes | CSPro | Yes | SPSS, EpIInfo |
| 10 | 2021 | Kenya ‡ | AFR | 9–59 months | 3,374,464 | 111 | June–July 2021 | Jul-21 | <3 months | NBS | Considered programmatic evaluation. No ethical clearance was sought. Informed consent was obtained. | No | 477 | 4404 | 5409 | Yes, but by Region | Yes | Enumeration areas | Not for the PCCS. Sample was from available up-to-date sampling frame maintained by NBS. | Yes | Survey Solution application with digitization of the questionnaire and integration of maps. | Yes | Not mentioned |
| 11 | 2021 | Nepal | SEAR | 9–59 months | 2,548,336 | 101 | Feb–Mar 2020 (Phase 1) Mar–July 2020 (Phase 2) | Sept–Nov 2021 | >1 year | Family Welfare Division Department of Health Services MOH | Yes | Yes | 342 | 7180 | 3715 | Yes | Yes | List of wards (some were merged or segmented) | Yes | Yes | CSPro | Yes | SPSS |
| 12 | 2021 | Pakistan | EMR | 9 months-15 years old | 90,262,980 | 105 | Nov-21 | Nov 2021–Jan 2022 | <3 months | Contech International Health Consultants | Yes | Yes | 1584 | 15,840 | 31,871 | Yes | Yes | Enumeration areas | Yes | Yes. Technical and sampling frame | Proprietary android-based CAPI application from implementing partner | No | Stata, VCQI |
| 13 | 2021 | Zambia | AFR | 9–59 months | 3,398,230 | 91.3 | Nov-20 | Oct-21 | >1 year | Not specified | No | No | 272 | 5155 | 4590 | No | Yes | Enumeration areas | Yes | Yes | The questionnaire was programmed into a CAPI application using survey solutions, a World Bank software application | Not mentioned? | |
| 14 | 2022 | Burundi | AFR | 9–59 months | 1,683,300 | 93 | Jan-22 | Oct–Nov 2022 | 10–11 months | NBS | Not mentioned | Yes | 540 | 32,177 | 20,618 | Yes | Yes | Ennumeration areas | Yes | Yes | KoboCollect | Yes | SPSS and Stata |
| 15 | 2022 | Madagascar | AFR | 6–59 months | 4,355,433 | 95.11 | May–June 2022 | Aug–Sept 2022 | 3 months | International consultant with Directorate of Demography and Social Statistics (DDSS) of the NBS | Yes | Yes | 123 | 3055 | 1421 | Yes | Yes | Enumeration areas | Yes | Yes | CSPro | Yes | SPSS and Stata |
| 16 | 2022 | Somalia | EMR | children of 0–59 months for tOPV, 06–59 months for MCV and Vitamin A and 12–59 months for deworming | 2,566,955 | 90 | Nov-22 | Feb-23 | 3 months | Independent consultant/cabinet | Yes | Yes | 450 | 17,539 | 21,740 | No | No | Lists of accessible areas (not mentioned in detail) | Not mentioned | Not mentioned | Survey123 | Yes | SPSS, Stata, ArcGIS |
| 17 | 2022 or 2023 | Syrian Arab Republic | EMR | 6 months-5 years | 2,494,498 | 75.62 | Oct–Nov 2022 | Dates not provided. 2023? | NA | Independent consultant | Yes | No | 99 | 5982 | 3581 | Yes | Yes | Sub-districts | Yes | Yes, technical advise | Paper-based | No | EpiInfo |
| 18 | 2023 | Cameroon | AFR | 9–59 months | 5,564,940 | 94.38 | Jul-23 | Sept–Oct 2023 | <3 months | NBS | No. Informed consent was obtained. | Yes | 395 | 5711 | 3546 | Yes | Yes | Enumeration areas | Yes | Yes | CSPro | Yes | SPSS, Stata, VCQI |
| 19 | 2023 | Democratic Republic of the Congo | AFR | 6–59 months | 6,454,490 (May) 7,359,339 (August) 5,273,383 (September) | 103.6 (May) 85.7 (August) 101.1 (September) | Three phases: April, June and Aug 2023. | October–December 2023 in Block 1, Phase 2 in Block 2 and part of Block 3 from January to March 2024, then Phase 3 in the rest of the provinces in March–April 2024. | 6 to 10 months | Independent consultant | Yes | Yes | 728 | 10,920 | 9627 | Yes | Yes | Enumeration areas | Yes | Yes | CSPro | Yes | SPSS, EpIInfo |
| 20 | 2023 | Malawi | AFR | 9–59 months | 3,169,522 | 82.4 | May-23 | Jun-23 | <3 months | International consultant and NBS | Yes | Yes | 205 | 4715 | 8485 | Yes | Yes | Enumeration areas | Yes | Yes | CSPro | Yes | Stata, VCQI |
| 21 | 2023 | Niger | AFR | 6–59 m or 9–59 m depending on district | 5,098,682 | 105 | Dec 2022–Jan 2023 | Mar–April 2023 | 3 months | Independent consultant | Yes | Yes | 270 | 5334 | 4655 | Yes | Yes | Ennumeration areas | Yes | Yes | ODK | Yes | SPSS |
| 22 | 2023 | Nigeria | AFR | 9–59 months | 4,298,149 (October) 1,090,330 (November) 5,021,611 (December) | 96.67 (October) 103.95 (November) 4,823,266 (December) | Oct 2023–Jan 2024 | Dec 2023–Jan 2024 | <3 months | NBS | No. Informed consent was obtained. | Yes | 740 (560 in 14 states plus 180 in 6 local area governments in Borno) | 7399 | 6987 | Yes | Yes | Enumeration areas | Yes | Yes | CSPro | Yes | Stata, VCQI |
| 23 | 2023 | Yemen ‡ | EMR | 6–59 months | 1,267,083 | 91 | September–October 2023 | Oct-23 | <3 months | Research Organization | Yes | Yes | 1547 | 18,564 | 29,549 | Yes | Yes | Harahs | No | No | ODK | No | Excel |
| 24 | 2024 | Ethiopia | AFR | 98.7 | Dec 2022–April 2023 | Dec 2023–Jan 2024 | >1 year | Research Organization | Yes | Yes | 1272 | 12,702 | 15,763 | Yes | Yes | Enumeration areas | Yes | Sampling frame from NBS | Kobo Toolbox | Yes | Stata, VCQI | ||
| Results | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| # | Year of PCCS | Country | WHO Region | MCV1 Coverage in Year of Start of SIA | Admin Coverage % | SIA Cards or Finger Marking Seen | SIA Coverage (95% CI) | % Routine Immunization (RI) Cards Seen (Age Group If Not All) | RI MCV1 Coverage % (95% CI) (Age Group If Not All) | SIA Dose Was the First MCV Dose Received by Child % (95%CI) | SIA Coverage Among Zero-Dose % (95%CI) | Child Remained Measles Zero-Dose After SIA % (95%CI) |
| 1 | 2019 | Democratic People’s Republic of Korea | SEAR | 98 | 99.7 | Almost all were verified by record in Primary Health Facility. Only recall were 7 children who had records in a different health facility | 99.9% (99.09–99.87) | NA | 81% yes, 18.6% unsure, 0.4% no | NR | NA | NA |
| 2 | 2019 | Zimbabwe | AFR | 85 | 91 | NR | 78.7% (77.35– 79.98) | NA | NA | NR | NR | NR |
| 3 | 2020 | Burkina Faso | AFR | 88 | 106 | 38.7% (87.8% received one) | 84.4% (83.6–85.2%) | 93% 12–23 months 81% 24–35 months | 87,8% 12–23 m 84.8% 24–35 m | NR | NR | 4.80% |
| 4 | 2020 | Cameroon | AFR | 61 | 92 | 8.30% | 69.7% (68.34–71.01) | NA | NR | 35.70% | NR | NR |
| 5 | 2020 | Ethiopia | AFR | 59 | 102.8 | 81.10% | 81.5% (80.0–83.0%) | NA | 80.30% | NR | 56.70% | 8.10% |
| 6 | 2020 | Uganda | AFR | 87 | 107 | 48.5 (78.4% received one) | 94.4% (93.0–95.5) | 25.30% | 85.40% | 12.00% | NR | 2.60% |
| 7 | 2021 | Central African Republic † | AFR | 41 | 102 for 6–59 m 85.5 for 5–10 yrs | 25% (83% received one) | 94.6% (92.9–96.0%) | NA | 25.2% 12–23 m 15.3% 24–35 m | NR | NR | 3.40% |
| 8 | 2021 | Chad | AFR | 53 | 108.8 (Phase1) 107.5 (Phase2) | 11% (19% reported not having received a card) | 77.4% (74.8–79.8%) | NA | Available as an analysis added later, not in main report. 41.1% 12–23 m 28.2% 24–35 m | NR | 73.5% (IC95%:70.2–76.5%) | 20% (IC95%: 17.6–22.5%) |
| 9 | 2021 | Democratic Republic of the Congo | AFR | 65 | 101.6 | 6.89%; 4.93% (correctly filled in) | 87.52% (87.50–87.53%) | NR | 80.70% | NR | 61.06%. | 7.61% |
| 10 | 2021 | Kenya ‡ | AFR | 90 | 111 | NR | 84.20% | NA | NA | NR | 80.10% | NR |
| 11 | 2021 | Nepal | SEAR | 87 | 101 | 43% | 84% (82–87) Phase 1: 87% (85–89) phase 2: 81% (77–85) | 51.40% | 95.50% | Small sample size of previously zero-dose | Small sample size of previously zero-dose | NR |
| 12 | 2021 | Pakistan | EMR | 81 | 105 | 80% | 93.6% (92.7–94.4) | 47% | 71.5% (and 10% unkown status) 79% for children under 2 years | NR | NR | NR |
| 13 | 2021 | Zambia | AFR | 96 | 91.3 | NA | 68.90% | 63% had documented evidence | 88.5 | NA | NA | NA |
| 14 | 2022 | Burundi | AFR | 89 | 93 | 15% | 88.60% | 91.8% 12–23 m 86.1% 24–35 m | 85.90% | NR | NR | NR |
| 15 | 2022 | Madagascar | AFR | 44 | 95.11 | 56.30% | 65.3% (56.8–72.9) | NA | 69.50% | NR | NR | 19.20% |
| 16 | 2022 | Somalia | EMR | 46 | 90 | NA | 86.0 (83.7–88.0) | 25% 12–23 | 65% | NR | 33.1% 14.1% 12–23 m 37.2% 24–35 m | NR |
| 17 | 2022 or 2023 | Syrian Arab Republic | EMR | 52 | 75.62 | 54.40% | 80.7% (79.35%–81.94%) | NA | 82.8 12–23 m 93.6 24–59 m | NR | 54.30% | NR |
| 18 | 2023 | Cameroon | AFR | 71 | 94.38 | 31.8% (84.9% received a card) | 69.5 (66.4–72.5) | NA | NR | 22.10% | 62.30% | 13.3% |
| 19 | 2023 | Democratic Republic of the Congo | AFR | 52 | 103.6 (May) 85.7 (August) 101.1 (September) | 12.88% | 94.60% (94.60%–94.61%) | ~3.5% (3.47% vaccinated by card seen) | 78.30% | NR | 75.01% | NA |
| 20 | 2023 | Malawi | AFR | 87 | 82.4 | 38.8% | 75.7% (72.3–79.0) | NA | NR | NR | 27.6% for 12–35 m | NR |
| 21 | 2023 | Niger | AFR | 65 | 105 | 71.8% (86.2% received one) | 92.7% (90.8–94.1) | NA | NA | NR | 91.60% | 4.60% |
| 22 | 2023 | Nigeria | AFR | 60 | 96.67 (October) 103.95 (November) 4,823,266 (December) | 47% card and 9.9% finger marking | 87% (84–90) | NR | NR | 12% | NR | NR |
| 23 | 2023 | Yemen ‡ | EMR | 45 | 91 | NA | 84.2% (95% CI: 83.8–84.6) | NA | NR | NR | 12% | NR |
| 24 | 2024 | Ethiopia | AFR | 55 | 98.7 | 16% | 87.10% | 3940 (~25%) | 73.80% | 14.00% | 72% | NR |
| Number of Measles Vaccine Doses Prior to SIA | Vaccinated During SIA (%) | 95% CI (%) | Vaccinated During SIA (Weighted N) | Weighted N |
|---|---|---|---|---|
| Zero | 37.2 | (31.8, 42.8) | 81 | 217 |
| 1 Dose | 92.8 | (89.5, 95.1) | 540 | 582 |
| 2+ Doses | 90.9 | (86.6, 94.0) | 812 | 894 |
| Somalia 2023 (Total) | 84.7 | (81.6, 87.3) | 1433 | 1692 |
| State | % Vac’d During SIA | Total # Children | Total # of Clusters | # Clusters with 100% Children vac’d’ | # Clusters with >50–99.9% Children vac’d | # Clusters with ≤50% Children vac’d | DEFF | ICC |
|---|---|---|---|---|---|---|---|---|
| Banadir | 89.8 | 3604 | 74 | 13 | 57 | 4 | 11.7 | 0.2216 |
| Galmudug | 86.1 | 3338 | 76 | 10 | 61 | 5 | 10.8 | 0.1634 |
| Hirshabelle | 82.6 | 4372 | 76 | 17 | 47 | 12 | 28.5 | 0.4284 |
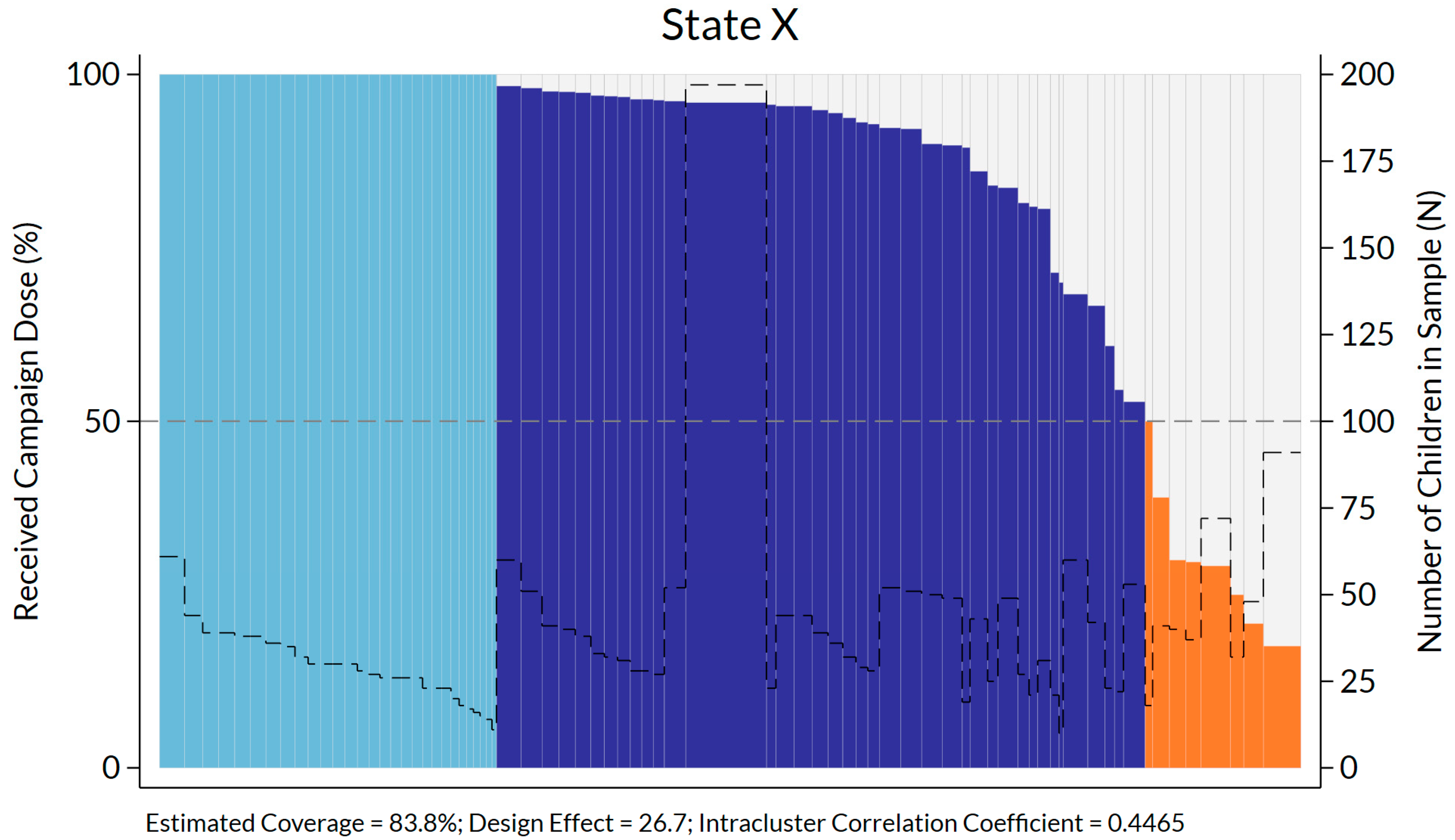
| Jubbaland | 83.8 | 2781 | 76 | 29 | 39 | 8 | 26.7 | 0.4465 |
| Puntland | 88.6 | 3279 | 73 | 18 | 52 | 3 | 14.0 | 0.2361 |
| Southwest | 87 | 3542 | 75 | 20 | 48 | 7 | 17.7 | 0.2791 |
| Total | 87 | 20,916 | 450 | 107 | 304 | 39 | 21.3 | 0.3116 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Danovaro-Holliday, M.C.; Koh, M.; Steulet, C.; Rhoda, D.A.; Trimner, M.K. Lessons from Recent Measles Post-Campaign Coverage Surveys Worldwide. Vaccines 2024, 12, 1257. https://doi.org/10.3390/vaccines12111257
Danovaro-Holliday MC, Koh M, Steulet C, Rhoda DA, Trimner MK. Lessons from Recent Measles Post-Campaign Coverage Surveys Worldwide. Vaccines. 2024; 12(11):1257. https://doi.org/10.3390/vaccines12111257
Chicago/Turabian StyleDanovaro-Holliday, M. Carolina, Mitsuki Koh, Claudia Steulet, Dale A. Rhoda, and Mary Kay Trimner. 2024. "Lessons from Recent Measles Post-Campaign Coverage Surveys Worldwide" Vaccines 12, no. 11: 1257. https://doi.org/10.3390/vaccines12111257
APA StyleDanovaro-Holliday, M. C., Koh, M., Steulet, C., Rhoda, D. A., & Trimner, M. K. (2024). Lessons from Recent Measles Post-Campaign Coverage Surveys Worldwide. Vaccines, 12(11), 1257. https://doi.org/10.3390/vaccines12111257