Exploring Vaccination Challenges among Syrian Refugees in Jordan: Insights from Camps and Communities, and Perceived Parental Barriers to Childhood Vaccination Uptake


Abstract
1. Introduction
2. Methods
2.1. Design
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Participants
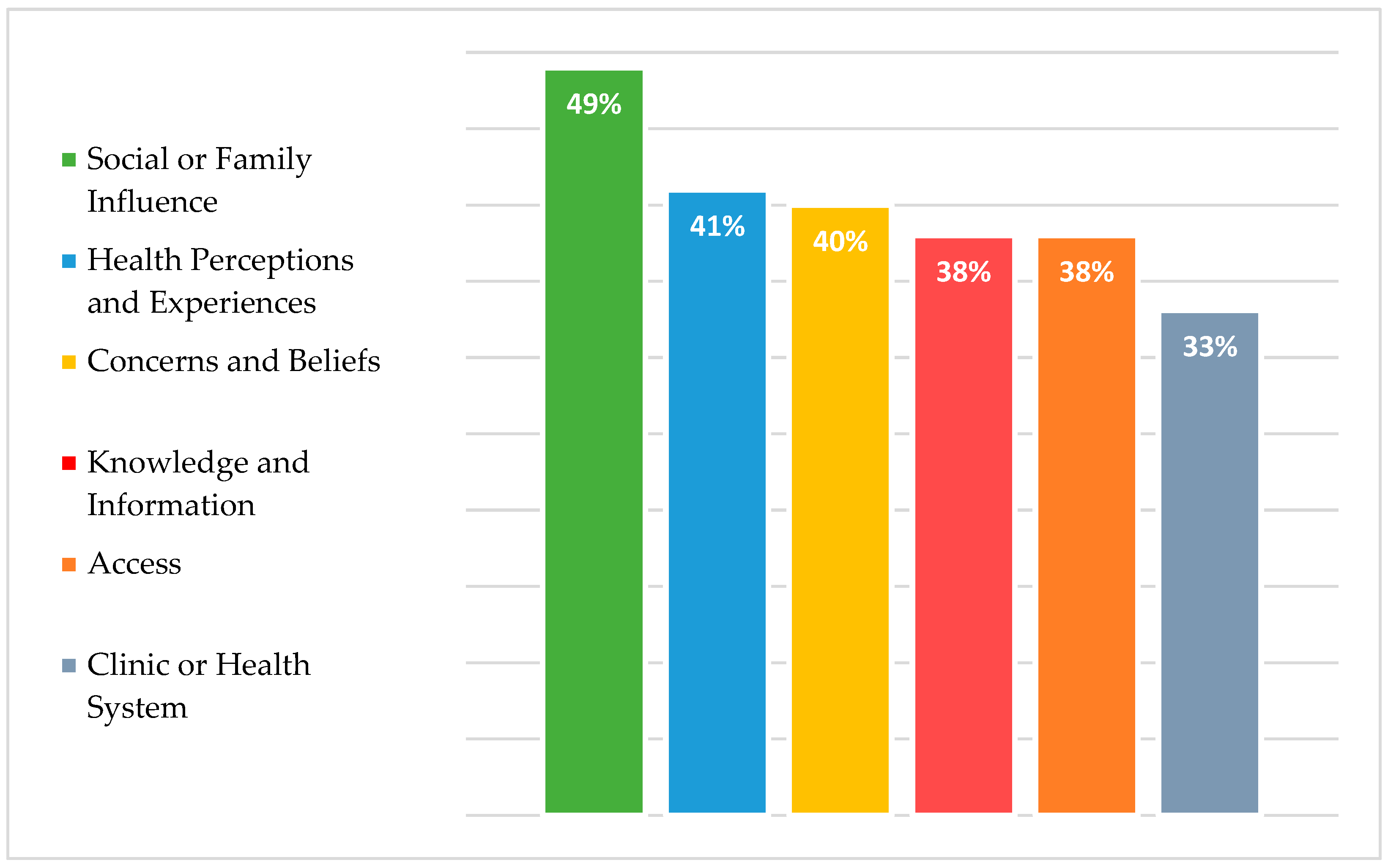
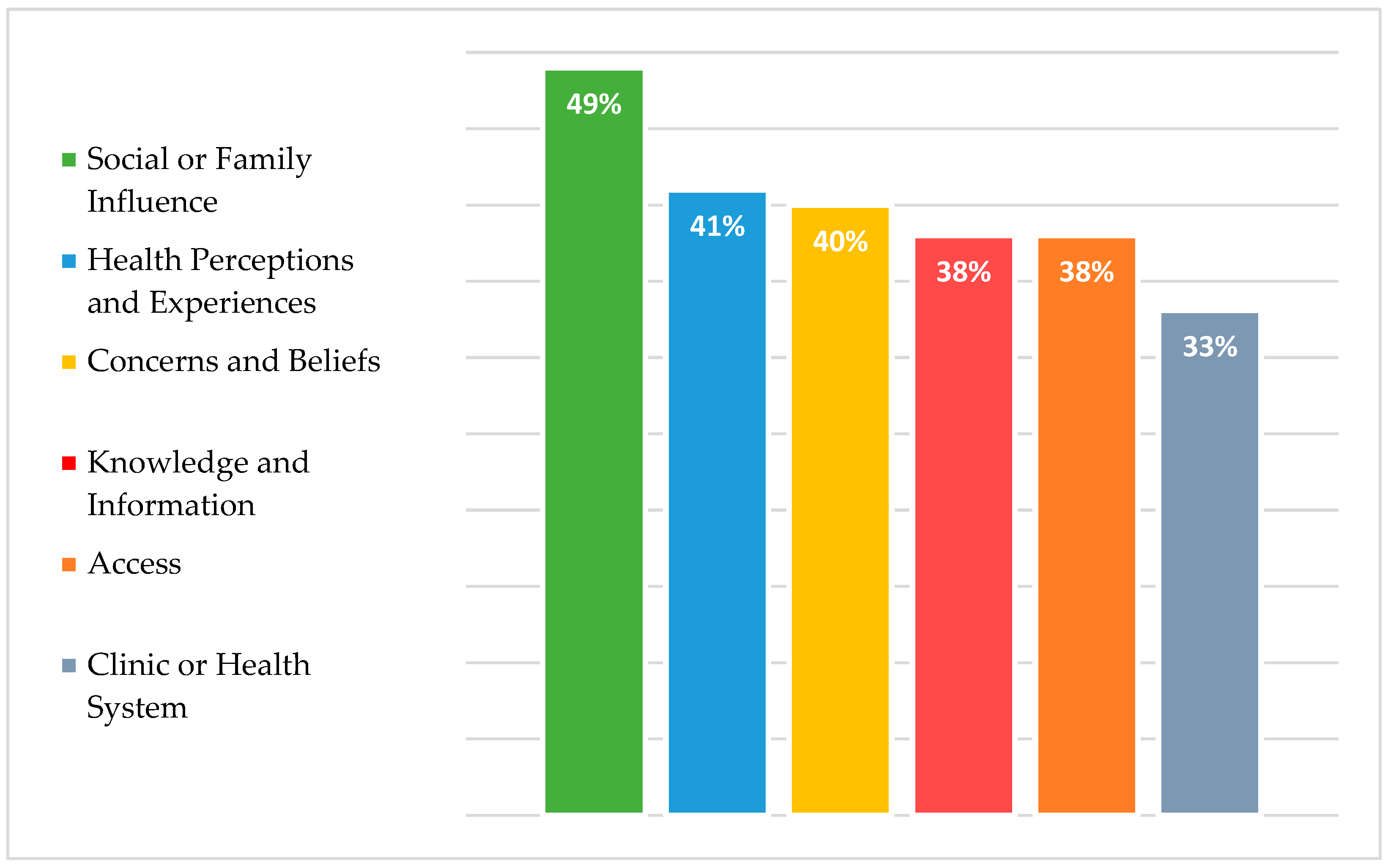
3.2. Barriers to Vaccinations
3.3. Sociodemographic Differences in Barrier Perception
3.4. Psychological Antecedents of Vaccination Adoption
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- UNHCR—Refugee Statistics. UNHCR. Available online: https://www.unhcr.org/refugee-statistics/ (accessed on 8 October 2022).
- Napoli, C.; Dente, M.G.; Kärki, T.; Riccardo, F.; Rossi, P.; Declich, S.; Network for the Control of Cross-border Health Threats in the Mediterranean Basin and Black Sea. Screening for Infectious Diseases among Newly Arrived Migrants: Experiences and Practices in Non-EU Countries of the Mediterranean Basin and Black Sea. Int. J. Environ. Res. Public Health 2015, 12, 15550–15558. [Google Scholar] [CrossRef]
- UNHCR. UNHCR: Global Displacement Hits Another Record, Capping Decade-Long Rising Trend. UNHCR. Available online: https://www.unhcr.org/news/press/2022/6/62a9d2b04/unhcr-global-displacement-hits-record-capping-decade-long-rising-trend.html (accessed on 8 October 2022).
- Murphy, A.; Woodman, M.; Roberts, B.; McKee, M. The neglected refugee crisis. BMJ 2016, 352, i484. [Google Scholar] [CrossRef]
- Al-Hussaini, M.; Al-Ani, A.; Hammouri, M.; Al-Huneidy, L.; Mansour, A. Investigating the impact of COVID-19 on patients with cancer from areas of conflict within the MENA region treated at King Hussein Cancer Center. Front. Oncol. 2023, 13, 1088000. [Google Scholar] [CrossRef] [PubMed]
- Lam, E.; Diaz, M.; Maina, A.G.K.; Brennan, M. Displaced populations due to humanitarian emergencies and its impact on global eradication and elimination of vaccine-preventable diseases. Confl. Health 2016, 10, 27. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.A.; Bacci, S.; Shadwick, R.; Tillmann, T.; Rechel, B.; Noori, T.; Suk, J.E.; Odone, A.; Ingleby, J.D.; Mladovsky, P.; et al. Measles among migrants in the European Union and the European Economic Area. Scand. J. Public Health 2016, 44, 6–13. [Google Scholar] [CrossRef] [PubMed]
- Charania, N.A.; Gaze, N.; Kung, J.Y.; Brooks, S. Vaccine-preventable diseases and immunisation coverage among migrants and non-migrants worldwide: A scoping review of published literature, 2006 to 2016. Vaccine 2019, 37, 2661–2669. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.T.; Sue, E.; Zola, J.; So, S.K. 3 for Life: A Model Pilot Program to Prevent Hepatitis B Virus Infection and Liver Cancer in Asian and Pacific Islander Americans. Am. J. Health Promot. 2009, 23, 176–181. [Google Scholar] [CrossRef]
- Kowal, S.P.; Jardine, C.G.; Bubela, T.M. “If they tell me to get it, I’ll get it. If they don’t....”: Immunization decision-making processes of immigrant mothers. Can. J. Public Health 2015, 106, e230–e235. [Google Scholar] [CrossRef] [PubMed]
- Chao, S.D.; Chang, E.T.; Le, P.V.; Prapong, W.; Kiernan, M.; So, S.K.S. The Jade Ribbon Campaign: A Model Program for Community Outreach and Education to Prevent Liver Cancer in Asian Americans. J. Immigr. Minor. Health 2009, 11, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Boulton, M.L.; Wagner, A.L. Advancing Global Vaccination Equity. Am. J. Prev. Med. 2021, 60, S1–S3. [Google Scholar] [CrossRef]
- Bonu, S.; Rani, M.; Baker, T.D. The impact of the national polio immunization campaign on levels and equity in immunization coverage: Evidence from rural North India. Soc. Sci. Med. 2003, 57, 1807–1819. [Google Scholar] [CrossRef] [PubMed]
- Farag, N.H.; Wannemuehler, K.; Weldon, W.; Arbaji, A.; Belbaisi, A.; Khuri-Bulos, N.; Ehrhardt, D.; Surour, M.R.; ElhajQasem, N.S.; Al-Abdallat, M.M. Estimating population immunity to poliovirus in Jordan’s high-risk areas. Hum. Vaccin. Immunother. 2020, 16, 548–553. [Google Scholar] [CrossRef]
- Al Rousan, T.; Schwabkey, Z.; Jirmanus, L.; Nelson, B.D. Health needs and priorities of Syrian refugees in camps and urban settings in Jordan: Perspectives of refugees and health care providers. East. Mediterr. Health J. 2018, 24, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Abdo, N.; Sweidan, F.; Batieha, A. Quality-of-life among Syrian refugees residing outside camps in Jordan relative to Jordanians and other countries. PeerJ 2019, 7, e6454. [Google Scholar] [CrossRef] [PubMed]
- Obi, C.T. How Refugees’ Decision to Live in or Outside a Camp Affects Their Quality of Life. 2021. Available online: https://blogs.worldbank.org/dev4peace/how-refugees-decision-live-or-outside-camp-affects-their-quality-life (accessed on 1 October 2023).
- Aguilera, A.; Krishnan, N.; Muñoz, J.; Riva, F.R.; Sharma, D.; Vishwanath, T. Sampling for Representative Surveys of Displaced Populations. In Data Collection in Fragile States; Hoogeveen, J., Pape, U., Eds.; Palgrave Macmillan: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Statistical Report on UNHCR Registered Refugees and Asylum-Seekers Jordan. Available online: https://data.unhcr.org/en/documents/details/99989 (accessed on 13 December 2023).
- Kaufman, J.; Tuckerman, J.; Bonner, C.; Durrheim, D.N.; Costa, D.; Trevena, L.; Thomas, S.; Danchin, M. Parent-level barriers to uptake of childhood vaccination: A global overview of systematic reviews. BMJ Glob. Health 2021, 6, e006860. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed]
- ElHafeez, S.A.; Elbarazi, I.; Shaaban, R.; ElMakhzangy, R.; Aly, M.O.; Alnagar, A.; Yacoub, M.; El Saeh, H.M.; Eltaweel, N.; Alqutub, S.T.; et al. Arabic validation and cross-cultural adaptation of the 5C scale for assessment of COVID-19 vaccines psychological antecedents. PLoS ONE 2021, 16, e0254595. [Google Scholar]
- Abdou, M.S.; Kheirallah, K.A.; Aly, M.O.; Ramadan, A.; Elhadi, Y.A.M.; Elbarazi, I.; Deghidy, E.A.; El Saeh, H.M.; Salem, K.M.; Ghazy, R.M. The coronavirus disease 2019 (COVID-19) vaccination psychological antecedent assessment using the Arabic 5c validated tool: An online survey in 13 Arab countries. PLoS ONE 2021, 16, e0260321. [Google Scholar] [CrossRef]
- Roberton, T.; Weiss, W.; Doocy, S. Challenges in Estimating Vaccine Coverage in Refugee and Displaced Populations: Results From Household Surveys in Jordan and Lebanon. Vaccines 2017, 5, 22. [Google Scholar] [CrossRef]
- Wilson, L.; Rubens-Augustson, T.; Murphy, M.; Jardine, C.; Crowcroft, N.; Hui, C.; Wilson, K. Barriers to immunization among newcomers: A systematic review. Vaccine 2018, 36, 1055–1062. [Google Scholar] [CrossRef]
- Murray, S.B.; Skull, S.A. Hurdles to health: Immigrant and refugee health care in Australia. Aust. Health Rev. 2005, 29, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Abdi, I.; Menzies, R.; Seale, H. Barriers and facilitators of immunisation in refugees and migrants in Australia: An east-African case study. Vaccine 2019, 37, 6724–6729. [Google Scholar] [CrossRef] [PubMed]
- Deal, A.; Crawshaw, A.F.; Carter, J.; Knights, F.; Iwami, M.; Darwish, M.; Hossain, R.; Immordino, P.; Kaojaroen, K.; Severoni, S.; et al. Defining drivers of under-immunization and vaccine hesitancy in refugee and migrant populations. J. Travel. Med. 2023, 30, taad084. [Google Scholar] [CrossRef]
- Salibi, N.; Abdulrahim, S.; El Haddad, M.; Bassil, S.; El Khoury, Z.; Ghattas, H.; McCall, S.J. COVID-19 vaccine acceptance in older Syrian refugees: Preliminary findings from an ongoing study. Preventive Medicine Reports. Prev. Med. Rep. 2021, 24, 101606. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8523309/ (accessed on 30 September 2023). [CrossRef] [PubMed]
- Tomlinson, N.; Redwood, S. Health beliefs about preschool immunisations: An exploration of the views of Somali women resident in the UK. Divers. Equal. Health Care 2013, 10, 101–113. [Google Scholar]
- Ganczak, M.; Bielecki, K.; Drozd-Dąbrowska, M.; Topczewska, K.; Biesiada, D.; Molas-Biesiada, A.; Dubiel, P.; Gorman, D. Vaccination concerns, beliefs and practices among Ukrainian migrants in Poland: A qualitative study. BMC Public Health 2021, 21, 93. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.; Saliba, V.; Ramsay, M.; Mounier-Jack, S. What have we learnt from measles outbreaks in 3 English cities? A qualitative exploration of factors influencing vaccination uptake in Romanian and Roma Romanian communities. BMC Public Health 2020, 20, 381. [Google Scholar] [CrossRef] [PubMed]
- Deal, A.; Halliday, R.; Crawshaw, A.F.; E Hayward, S.; Burnard, A.; Rustage, K.; Carter, J.; Mehrotra, A.; Knights, F.; Campos-Matos, I.; et al. Migration and outbreaks of vaccine-preventable disease in Europe: A systematic review. Lancet Infect. Dis. 2021, 21, e387–e398. [Google Scholar] [CrossRef]
- Jalloh, M.F.; Bennett, S.D.; Alam, D.; Kouta, P.; Lourenço, D.; Alamgir, M.; Feldstein, L.R.; Ehlman, D.C.; Abad, N.; Kapil, N.; et al. Rapid behavioral assessment of barriers and opportunities to improve vaccination coverage among displaced Rohingyas in Bangladesh, January 2018. Vaccine 2019, 37, 833–838. [Google Scholar] [CrossRef]
- Glatman-Freedman, A.; Nichols, K. The effect of social determinants on immunization programs. Hum. Vaccin. Immunother. 2012, 8, 293–301. [Google Scholar] [CrossRef]
- Ganczak, M.; Dmytrzyk-Daniłów, G.; Karakiewicz, B.; Korzeń, M.; Szych, Z. Determinants influencing self-paid vaccination coverage, in 0–5 years old Polish children. Vaccine 2013, 31, 5687–5692. [Google Scholar] [CrossRef]
- Hughes, A.; Mesher, D.; White, J.; Soldan, K. Coverage of the English National human papillomavirus (HPV) Immunisation Programme among 12 to 17 year-old females by area-level deprivation score, England, 2008 to 2011. Eurosurveillance 2014, 19, 20677. [Google Scholar] [CrossRef]
- Louka, C.; Chandler, E.; Ranchor, A.V.; Broer, H.; Pournaras, S.; Ravensbergen, S.J.; Stienstra, Y. Asylum seekers’ perspectives on vaccination and screening policies after their arrival in Greece and The Netherlands. PLoS ONE 2019, 14, e0226948. [Google Scholar] [CrossRef] [PubMed]
- Rubens-Augustson, T.; Wilson, L.A.; Murphy, M.S.; Jardine, C.; Pottie, K.; Hui, C.; Stafström, M.; Wilson, K. Healthcare provider perspectives on the uptake of the human papillomavirus vaccine among newcomers to Canada: A qualitative study. Hum. Vaccin. Immunother. 2018, 15, 1697–1707. [Google Scholar] [CrossRef]
- Arnaout, M. Caring for Children with Cancer in a Country Conflicted with Massive Refugee Migration: Jordan as an Example. In Cancer Care in Countries and Societies in Transition; Springer: Cham, Switzerland, 2016; pp. 105–116. Available online: https://link.springer.com/chapter/10.1007/978-3-319-22912-6_8 (accessed on 1 October 2023).
- Abu-Sliah, A. Impact of Syrian Refugees on Jordan’s Health Sector. UNHCR Operational Data Portal (ODP). Available online: https://data.unhcr.org/en/documents/details/39516 (accessed on 1 October 2023).
- Lyles, E. Syrian Refugee Health Access Survey in Jordan. UNHCR Operational Data Portal (ODP). Available online: https://data2.unhcr.org/en/documents/details/45809 (accessed on 1 October 2023).
- Obi, C.T. The Impact of Living Arrangements (In-Camp versus Out-of-Camp) on the Quality of Life: Case Study of Syrian Refugees in Jordan. World Bank Group. Available online: https://www.jointdatacenter.org/literature_review/the-impact-of-living-arrangements-in-camp-versus-out-of-camp-on-the-quality-of-life-case-study-of-syrian-refugees-in-jordan/ (accessed on 30 September 2023).
- Murshidi, M.M.; Hijjawi, M.Q.B.; Jeriesat, S.; Eltom, A. Syrian refugees and Jordan’s health sector. Lancet 2013, 382, 206–207. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Rothman, A.J.; Leask, J.; Kempe, A. Increasing Vaccination: Putting Psychological Science Into Action. Psychol. Sci. Public Interest 2017, 18, 149–207. [Google Scholar] [CrossRef]
- Bedford, H.; Attwell, K.; Danchin, M.; Marshall, H.; Corben, P.; Leask, J. Vaccine hesitancy, refusal and access barriers: The need for clarity in terminology. Vaccine 2018, 36, 6556–6558. [Google Scholar] [CrossRef]
- Ay, M.; Arcos González, P.; Castro Delgado, R. The Perceived Barriers of Access to Health Care Among a Group of Non-camp Syrian Refugees in Jordan. Int. J. Health Serv. 2016, 46, 566–589. [Google Scholar] [CrossRef] [PubMed]
- Crawshaw, A.F.; Deal, A.; Rustage, K.; Forster, A.S.; Campos-Matos, I.; Vandrevala, T.; Würz, A.; Pharris, A.; Suk, J.E.; Kinsman, J.; et al. What must be done to tackle vaccine hesitancy and barriers to COVID-19 vaccination in migrants? J. Travel Med. 2021, 28, taab048. [Google Scholar] [CrossRef] [PubMed]
- Kaji, A.; Parker, D.M.; Chu, C.S.; Thayatkawin, W.; Suelaor, J.; Charatrueangrongkun, R.; Salathibuppha, K.; Nosten, F.H.; McGready, R. Immunization Coverage in Migrant School Children along the Thailand-Myanmar Border. J. Immigr. Minor. Health 2016, 18, 1038–1045. [Google Scholar] [CrossRef]
- Rossi, C.; Schwartzman, K.; Oxlade, O.; Klein, M.B.; Greenaway, C. Hepatitis B Screening and Vaccination Strategies for Newly Arrived Adult Canadian Immigrants and Refugees: A Cost-Effectiveness Analysis. PLoS ONE 2013, 8, e78548. [Google Scholar] [CrossRef]
- Peak, C.M.; Reilly, A.L.; Azman, A.S.; Buckee, C.O. Prolonging herd immunity to cholera via vaccination: Accounting for human mobility and waning vaccine effects. PLoS Neglected Trop. Dis. 2018, 12, e0006257. [Google Scholar] [CrossRef]
- El-Halabi, S.; Khader, Y.S.; Khdeir, M.A.; Hanson, C.; Alfvén, T.; El-Khatib, Z. Children Immunization App (CIMA): A Non-randomized Controlled Trial Among Syrian Refugees in Zaatari Camp, Jordan. J. Prev. 2023, 44, 239–252. [Google Scholar] [CrossRef]
- Khader, Y.S.; Laflamme, L.; Schmid, D.; El-Halabi, S.; Abu Khdair, M.; Sengoelge, M.; Atkins, S.; Tahtamouni, M.; Derrough, T.; El-Khatib, Z. Children Immunization App (CImA) Among Syrian Refugees in Zaatari Camp, Jordan: Protocol for a Cluster Randomized Controlled Pilot Trial Intervention Study. JMIR Res. Protoc. 2019, 8, e13557. [Google Scholar] [CrossRef]
- Mellou, K.; Silvestros, C.; Saranti-Papasaranti, E.; Koustenis, A.; Pavlopoulou, I.D.; Georgakopoulou, T.; Botsi, C.; Terzidis, A. Increasing childhood vaccination coverage of the refugee and migrant population in Greece through the European programme PHILOS, April 2017 to April 2018. Eurosurveillance 2019, 24, 1800326. [Google Scholar] [CrossRef] [PubMed]
- Charania, N.A.; Gaze, N.; Kung, J.Y.; Brooks, S. Interventions to reduce the burden of vaccine-preventable diseases among migrants and refugees worldwide: A scoping review of published literature, 2006–2018. Vaccine 2020, 38, 7217–7225. [Google Scholar] [CrossRef] [PubMed]
- Dardas, L.A.; Al-leimon, O.; Jaber, A.R.; Saadeh, M.; Al-leimon, A.; Al-Hurani, A.; Jaber, A.-R.; Aziziye, O.; Al-salieby, F.; Aljahalin, M.; et al. Flu Shots Unveiled: A Global Systematic Review of Healthcare Providers’ Uptake of, Perceptions, and Attitudes toward Influenza Vaccination. Vaccines 2023, 11, 1760. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristic | n (%) |
|---|---|
| Gender | |
| Male | 58 (17.5%) |
| Female | 274 (82.5%) |
| Mean age | 32.7 ± 10 |
| Marital status | |
| Married | 311 (93.7%) |
| Divorced | 8 (2.4%) |
| Widowed | 13 (3.9%) |
| Educational level | |
| No schooling | 31 (9.3%) |
| 11th grade or less | 196 (59%) |
| 12th grade | 53 (16%) |
| Diploma | 16 (4.8%) |
| Bachelor’s degree or higher | 36 (10.8%) |
| Income (in JD *) | |
| Less than 150 | 240 (72.3%) |
| 150–300 | 62 (18.7%) |
| 301–500 | 25 (7.5%) |
| 501–1000 | 2 (0.6%) |
| 1001–1500 | 3 (0.9%) |
| 1501–2000 | 0 (0%) |
| Number of children | |
| 0 | 8 (2.4%) |
| 1–3 | 165 (49.5%) |
| 4–6 | 132 (39.6%) |
| >6 | 27 (8.1%) |
| Residence | |
| Inside a camp | 167 (50.3%) |
| Outside a camp | 165 (49.7%) |
| Occupation | |
| Unemployed | 271 (81.3%) |
| Employed | 61 (18.3%) |
| Health problems | |
| Have a health problem | 75 (22.5%) |
| Does not have a health problem | 257 (77.1%) |
| Child health problems | |
| Has a health problem | 44 (13.2%) |
| Does not have a health problem | 288 (86.4%) |
| Seeking help before | |
| Yes | 19 (5.7%) |
| No | 313 (93.9%) |
| Items Classified by Barrier Category | Disagree n (%) | Neutral n (%) | Agree n (%) | |||
|---|---|---|---|---|---|---|
| Access Barriers | ||||||
| (1) I don’t have enough time to get vaccinated. | 261 | (78.6%) | 26 | (7.8%) | 45 | (13.6%) |
| (2) I have trouble affording financial vaccinations. | 243 | (73.2%) | 26 | (7.8%) | 63 | (19.0%) |
| (3) I am facing a problem with transportation, and this prevents me from taking vaccinations. | 239 | (72.0%) | 22 | (6.6%) | 71 | (21.4%) |
| (4) I have a problem because there is no comprehensive health system. | 222 | (66.9%) | 28 | (8.4%) | 82 | (24.7%) |
| (5) I have a problem with waiting a long time when I receive the vaccine. | 220 | (66.3%) | 30 | (9.0%) | 82 | (24.7%) |
| (6) I have trouble securing care for my other children when we will get vaccinated | 208 | (62.7%) | 32 | (9.6%) | 92 | (27.7%) |
| (7) I have a problem with impermanent residence and frequent commuting | 244 | (73.5%) | 25 | (7.5%) | 63 | (19.0%) |
| (8) I receive inadequate healthcare support due to social exclusion | 266 | (80.1%) | 31 | (9.3%) | 35 | (10.5%) |
| (9) I have a problem with vaccines availability. | 278 | (83.7%) | 25 | (7.5%) | 29 | (8.7%) |
| (10) I have appointment time difficulties related to get vaccines. | 280 | (84.3%) | 20 | (6.0%) | 32 | (9.6%) |
| (11) I don’t have health insurance, and this is preventing me from getting vaccinations. | 260 | (78.3%) | 23 | (6.9%) | 49 | (14.8%) |
| (12) I have trouble relating to the cost of transportation to a healthcare facility | 243 | (73.2%) | 23 | (6.9%) | 66 | (19.9%) |
| (13) I have trouble accessing vaccinations for other reasons that have not been mentioned. | 269 | (81.0%) | 35 | (10.5%) | 28 | (8.4%) |
| Clinic or Health System Barriers | ||||||
| (14) Health providers poor communication constitute an obstacle to obtaining vaccinations | 166 | (94.3%) | 1 | (0.6%) | 9 | (5.1%) |
| (15) There is no vaccination reminder system. | 277 | (83.4%) | 35 | (10.5%) | 20 | (6.0%) |
| (16) There is a delay in the clinic and disorganization in its health facilities. | 257 | (77.4%) | 21 | (6.3%) | 54 | (16.3%) |
| (17) I was not informed enough about vaccination recommendation. | 253 | (76.2%) | 34 | (10.2%) | 45 | (13.6%) |
| (18) The poor buildings and equipment makes me afraid of exposure to pathogens | 252 | (75.9%) | 27 | (8.1%) | 53 | (16.0%) |
| (19) Health centers are not adequately funded and monitored. | 239 | (72.0%) | 47 | (14.2%) | 46 | (13.9%) |
| (20) Lack of culturally appropriate healthcare or linguistic barriers is an obstacle to getting vaccines. | 235 | (70.8%) | 44 | (13.3%) | 53 | (16.0%) |
| (21) Healthcare providers have negative attitudes and they do not have enough health knowledge. | 285 | (85.8%) | 26 | (7.8%) | 21 | (6.3%) |
| (22) I can’t get another appointment to get vaccinated when I miss my appointment. | 282 | (84.9%) | 29 | (8.7%) | 21 | (6.3%) |
| (23) Poor relationship with providers reduces the possibility of going to get vaccinations. | 265 | (79.8%) | 37 | (11.1%) | 30 | (9.0%) |
| (24) Providers hesitate or are lazy to administer vaccinations. | 281 | (84.6%) | 27 | (8.1%) | 24 | (7.2%) |
| Concerns and Beliefs | ||||||
| (25) I am concerned about the safety of the vaccines and I’m afraid of their possible damage. | 268 | (80.7%) | 31 | (9.3%) | 33 | (9.9%) |
| (26) I mistrust vaccinations, their providers, or the health policies in force. | 254 | (76.5%) | 33 | (9.9%) | 45 | (13.6%) |
| (27) I believe having illnesses strengthen a child’s immune system better than vaccinations. | 247 | (74.4%) | 36 | (10.8%) | 49 | (14.8%) |
| (28) I believe that vaccinations compromise the immune system. | 266 | (80.1%) | 32 | (9.6%) | 34 | (10.2%) |
| (29) I believe that there is immune system response variation among children. | 177 | (53.3%) | 38 | (11.4%) | 117 | (35.2%) |
| (30) I think vaccines are provided when children are too young. | 211 | (63.6%) | 32 | (9.6%) | 89 | (26.8%) |
| (31) I believe that parents have the full right to accept or reject the vaccination. | 167 | (50.3%) | 39 | (11.7%) | 126 | (38.0%) |
| (32) I believe that combination vaccines (triple, quintuple) are harmful effects on the body. | 220 | (66.3%) | 34 | (10.2%) | 78 | (23.5%) |
| (33) I believe that multiple vaccinations and doses are unsafe for the child. | 240 | (72.3%) | 62 | (18.7%) | 30 | (9.0%) |
| (34) As a mother, I do not have the capacity to take my child to receive vaccines. | 224 | (67.5%) | 48 | (14.5%) | 60 | (18.1%) |
| (35) I believe that vaccinations have a role in the child’s autism. | 261 | (78.6%) | 29 | (8.7%) | 42 | (12.7%) |
| (36) I believe that epidemics and vaccinations are an external conspiracy. | 279 | (84.0%) | 40 | (12.0%) | 13 | (3.9%) |
| (37) I am worried about injection site pain. | 211 | (63.6%) | 47 | (14.2%) | 74 | (22.3%) |
| (38) I feel regret and guilt if vaccine side-effects occurred. | 200 | (60.2%) | 30 | (9.0%) | 102 | (30.7%) |
| (39) I believe that there is no flexibility to adapt a vaccine schedule to a child. | 234 | (70.5%) | 29 | (8.7%) | 69 | (20.8%) |
| (40) I am concerned about vaccinations in general. | 243 | (73.2%) | 45 | (13.6%) | 44 | (13.3%) |
| Health Perceptions and Experiences | ||||||
| (41) The child has a contraindication on appointment day prevented me from vaccination. | 131 | (39.5%) | 35 | (10.5%) | 166 | (50.0%) |
| (42) I believe that there is no need to take the vaccine because the disease is not severe. | 203 | (61.1%) | 29 | (8.7%) | 100 | (30.1%) |
| (43) I am concerned about potential allergies after taking the vaccine. | 229 | (69.0%) | 35 | (10.5%) | 68 | (20.5%) |
| (44) I think that vaccines are not effective | 222 | (66.9%) | 33 | (9.9%) | 77 | (23.2%) |
| (45) I prefer alternative healthcare (such as herbal remedies) instead of vaccinations. | 270 | (81.3%) | 42 | (12.7%) | 20 | (6.0%) |
| (46) I have personal objections to vaccinations. | 281 | (84.6%) | 31 | (9.3%) | 20 | (6.0%) |
| (47) My child’s fear of needles is an obstacle to getting immunized. | 254 | (76.5%) | 48 | (14.5%) | 30 | (9.0%) |
| (48) Poor past experiences with health services constitute an obstacle to vaccination. | 251 | (75.6%) | 28 | (8.4%) | 53 | (16.0%) |
| Knowledge and Information | ||||||
| (49) I believe that there is insufficient knowledge of the importance of receiving all vaccines dose. | 260 | (78.3%) | 38 | (11.4%) | 34 | (10.2%) |
| (50) I believe that there is insufficient quantity and quality of information related to vaccines. | 238 | (71.7%) | 36 | (10.8%) | 58 | (17.5%) |
| (51) Insufficient knowledge about the vaccination dose schedule made me not adherent to them. | 236 | (71.1%) | 35 | (10.5%) | 61 | (18.4%) |
| (52) What I read of vaccine-related information in the media made me not adhere to it. | 241 | (72.6%) | 48 | (14.5%) | 43 | (13.0%) |
| (53) The available information about the content of the vaccines is not adequate. | 249 | (75.0%) | 35 | (10.5%) | 48 | (14.5%) |
| (54) Unawareness of vaccination services, clinic location, or the timing, made me not adhere to it. | 241 | (72.6%) | 25 | (7.5%) | 66 | (19.9%) |
| (55) Uncertainty about the importance of vaccinations made me not adhere to it. | 263 | (79.2%) | 35 | (10.5%) | 34 | (10.2%) |
| (56) Forgetting the appointments (schedule) for vaccinations made me not adhere to them. | 246 | (74.1%) | 28 | (8.4%) | 58 | (17.5%) |
| (57) The available information about vaccinations is not appropriate for all education levels. | 248 | (74.7%) | 32 | (9.6%) | 52 | (15.7%) |
| Social or Family Influence | ||||||
| (58) Religious beliefs regarding vaccinations made me not adhere to them. | 246 | (74.1%) | 40 | (12.0%) | 46 | (13.9%) |
| (59) I believe that vaccination is a societal duty for community protection. | 135 | (40.7%) | 32 | (9.6%) | 165 | (49.7%) |
| (60) Following up on vaccination schedules is the mother’s responsibility only. | 141 | (42.5%) | 22 | (6.6%) | 169 | (50.9%) |
| (61) Diseases can be treated through alternative methods such as going to the clergy. | 251 | (75.6%) | 23 | (6.9%) | 58 | (17.5%) |
| Measures Domains | Gender | Age | Income (in JD +) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | p-Value | <32 | >32 | p-Value | <150 | >150 | p-Value | ||
| Barrier | Access | 45.3 + 19.1 | 32.4 + 13.7 | <0.001 * | 28.5 + 11.7 | 39.7 + 16.3 | <0.001 * | 37.1 + 16.8 | 28.1 + 8.7 | <0.001 * |
| System | 32.3 + 13.7 | 24.0 + 9.6 | <0.001 * | 21.7 + 8.3 | 28.7 + 11.6 | <0.001 * | 26.4 + 11.7 | 23.1 + 7.9 | 0.014 * | |
| Concerns and Beliefs | 56.9 + 19.8 | 42.7 + 16.7 | <0.001 * | 39.7 + 15.2 | 49.4 + 18.8 | <0.001 * | 46.9 + 19.6 | 40.7 + 12.5 | 0.005 * | |
| Perceptions | 33.1 + 11.6 | 23.9 + 9.6 | <0.001 * | 22.2 + 9.3 | 28.4 + 10.9 | <0.001 * | 26.6 + 11.3 | 22.7 + 7.7 | 0.003 * | |
| Knowledge | 28.1 + 12.4 | 20.0 + 9.6 | <0.001 * | 18.3 + 8.8 | 23.9 + 11.4 | <0.001 * | 22.5 + 11.3 | 18.6 + 7.7 | 0.003 * | |
| Social and Family | 15.3 + 4.2 | 13.3 + 3.8 | 0.001 * | 12.5 + 3.6 | 14.7 + 3.9 | <0.001 * | 14.0 + 4.1 | 12.8 + 3.3 | 0.013 * | |
| Construct | Confidence | 6.7 + 0.2 | 6.7 + 0.4 | 0.921 | 6.7 + 0.4 | 6.6 + 0.3 | 0.293 | 6.7 + 0.3 | 6.7 + 0.4 | 0.518 |
| Complacency | 1.0 + 0.1 | 1.6 + 0.7 | <0.001 * | 1.8 + 0.7 | 1.3 + 0.6 | <0.001 * | 1.5 + 0.7 | 1.6 + 0.5 | 0.112 | |
| Constraints | 1.7 + 0.3 | 1.9 + 0.7 | 0.027 * | 2.0 + 0.8 | 1.7 + 0.5 | <0.001 * | 1.8 + 0.6 | 2.0 + 0.8 | 0.005 * | |
| Calculation | 2.1 + 0.4 | 3.0 + 1.5 | <0.001 * | 3.4 + 1.6 | 2.4 + 1.0 | <0.001 * | 2.7 + 1.3 | 3.3 + 1.6 | 0.001 * | |
| Collective responsibility | 4.7 + 0.2 | 4.5 + 0.8 | 0.203 | 4.5 + 0.8 | 4.6 + 0.6 | 0.421 | 4.6 + 0.7 | 4.5 + 0.8 | 0.473 | |
| Measures Domains | Educational Level | Living Arrangement | Marital Status | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No Education | Less Than 12th Grade | Secondary Education | Graduate or Higher | p-Value | In Camp | Outside Camp | p-Value | Married | Divorced or Widowed | p-Value | ||
| Barrier | Access | 39.3 + 16.7 | 31.8 + 13.6 | 41.3 + 19.7 | 35.6 + 14.4 | <0.001 * | 26.6 + 7.9 | 42.9 + 17.0 | <0.001 * | 34.1 + 15.3 | 42.2 + 17.9 | 0.056 |
| System | 28.6 + 10.9 | 23.0 + 9.1 | 29.2 + 13.9 | 29.3 + 11.0 | <0.001 * | 19.8 + 5.2 | 31.4 + 11.9 | <0.001 * | 25.0 + 10.6 | 33.4 + 11.7 | 0.004 * | |
| Concerns and Beliefs | 47.6 + 16.9 | 41.6 + 16.0 | 53.1 + 22.2 | 49.2 + 18.4 | <0.001 * | 35.3 + 9.0 | 55.2 + 19.5 | <0.001 * | 44.3 + 17.4 | 57.9 + 23.4 | 0.001 * | |
| Perceptions | 28.1 + 10.8 | 23.4 + 9.6 | 28.6 + 11.9 | 28.7 + 10.9 | <0.001 * | 19.4 + 5.4 | 31.7 + 11.0 | <0.001 * | 25.0 + 10.4 | 32.2 + 10.6 | 0.006 * | |
| Knowledge | 22.5 + 10.1 | 19.3 + 9.2 | 24.9 + 13.1 | 25.0 + 11.2 | <0.001 * | 15.7 + 5.7 | 27.2 + 11.3 | <0.001 * | 20.9 + 10.3 | 28.5 + 11.8 | 0.009 * | |
| Social and Family | 14.3 + 4.5 | 13.0 + 3.7 | 14.8 + 4.1 | 14.7 + 4.0 | 0.003 * | 12.3 + 3.1 | 15.2 + 4.1 | <0.001 * | 13.6 + 3.9 | 15.1 + 4.1 | 0.118 | |
| Construct | Confidence | 6.5 + 0.4 | 6.7 + 0.4 | 6.6 + 0.4 | 6.6 + 0.2 | 0.009 * | 6.7 + 0.5 | 6.6 + 0.2 | 0.589 | 6.7 + 0.4 | 6.6 + 0.2 | 0.609 |
| Complacency | 1.7 + 0.7 | 1.6 + 0.7 | 1.3 + 0.6 | 1.3 + 0.4 | <0.001 * | 1.9 + 0.7 | 1.1 + 0.3 | <0.001 * | 1.6 + 0.7 | 1.1 + 0.3 | 0.003 * | |
| Constraints | 2.1 + 0.7 | 1.9 + 0.8 | 1.7 + 0.4 | 1.6 + 0.3 | 0.003 * | 2.0 + 0.8 | 1.7 + 0.4 | <0.001 * | 1.8 + 0.7 | 1.8 + 0.5 | 0.678 | |
| Calculation | 2.4 + 1.1 | 3.1 + 1.5 | 2.7 + 1.4 | 2.5 + 1.1 | 0.013 * | 3.6 + 1.6 | 2.2 + 0.6 | <0.001 * | 2.9 + 1.5 | 2.1 + 0.3 | 0.001 * | |
| Collective responsibility | 4.2 + 1.0 | 4.6 + 0.6 | 4.4 + 0.8 | 4.6 + 0.5 | 0.004 * | 4.5 + 0.9 | 4.6 + 0.3 | 0.075 | 4.6 + 0.7 | 4.6 + 0.4 | 0.871 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abdulhaq, B.; Hammouri, M.; Abu Hawas, D.; Dardas, L.A. Exploring Vaccination Challenges among Syrian Refugees in Jordan: Insights from Camps and Communities, and Perceived Parental Barriers to Childhood Vaccination Uptake. Vaccines 2024, 12, 133. https://doi.org/10.3390/vaccines12020133
Abdulhaq B, Hammouri M, Abu Hawas D, Dardas LA. Exploring Vaccination Challenges among Syrian Refugees in Jordan: Insights from Camps and Communities, and Perceived Parental Barriers to Childhood Vaccination Uptake. Vaccines. 2024; 12(2):133. https://doi.org/10.3390/vaccines12020133
Chicago/Turabian StyleAbdulhaq, Bayan, Muhammad Hammouri, Dania Abu Hawas, and Latefa Ali Dardas. 2024. "Exploring Vaccination Challenges among Syrian Refugees in Jordan: Insights from Camps and Communities, and Perceived Parental Barriers to Childhood Vaccination Uptake" Vaccines 12, no. 2: 133. https://doi.org/10.3390/vaccines12020133
APA StyleAbdulhaq, B., Hammouri, M., Abu Hawas, D., & Dardas, L. A. (2024). Exploring Vaccination Challenges among Syrian Refugees in Jordan: Insights from Camps and Communities, and Perceived Parental Barriers to Childhood Vaccination Uptake. Vaccines, 12(2), 133. https://doi.org/10.3390/vaccines12020133