
No Waning of Pneumococcal Vaccine Responses over Time in People with Inflammatory Arthritis: Findings from a Single Centre Cohort

 , ,
, ,
Abstract
1. Background
2. Methods
2.1. Study Design and Population
2.2. Primary Outcome
2.3. Statistical Methodology
2.4. Ethics
3. Results
3.1. Characteristics of Cohort
3.2. Time between Pneumococcal Vaccine Administration and Serological Assessment
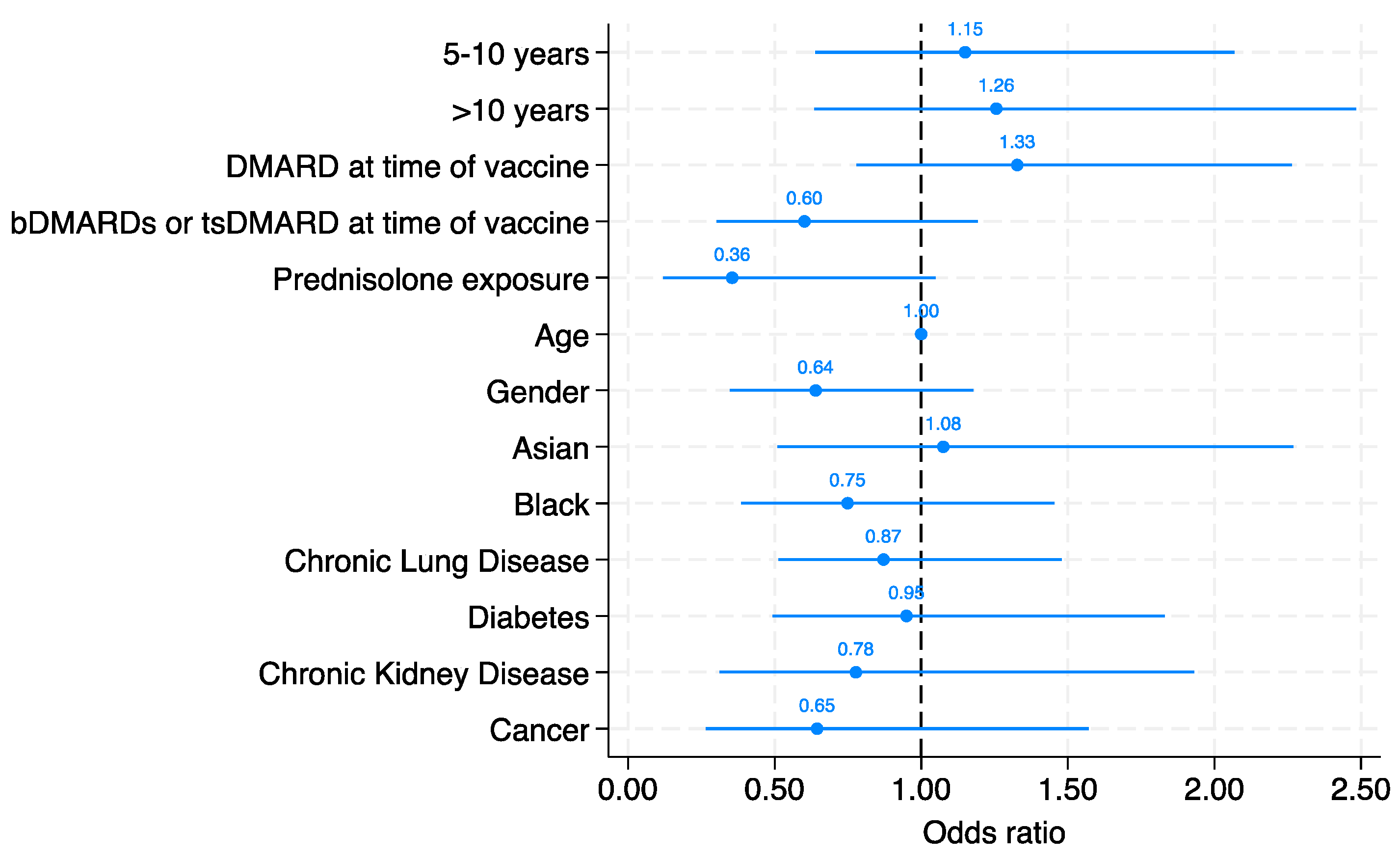
3.3. Serological Response
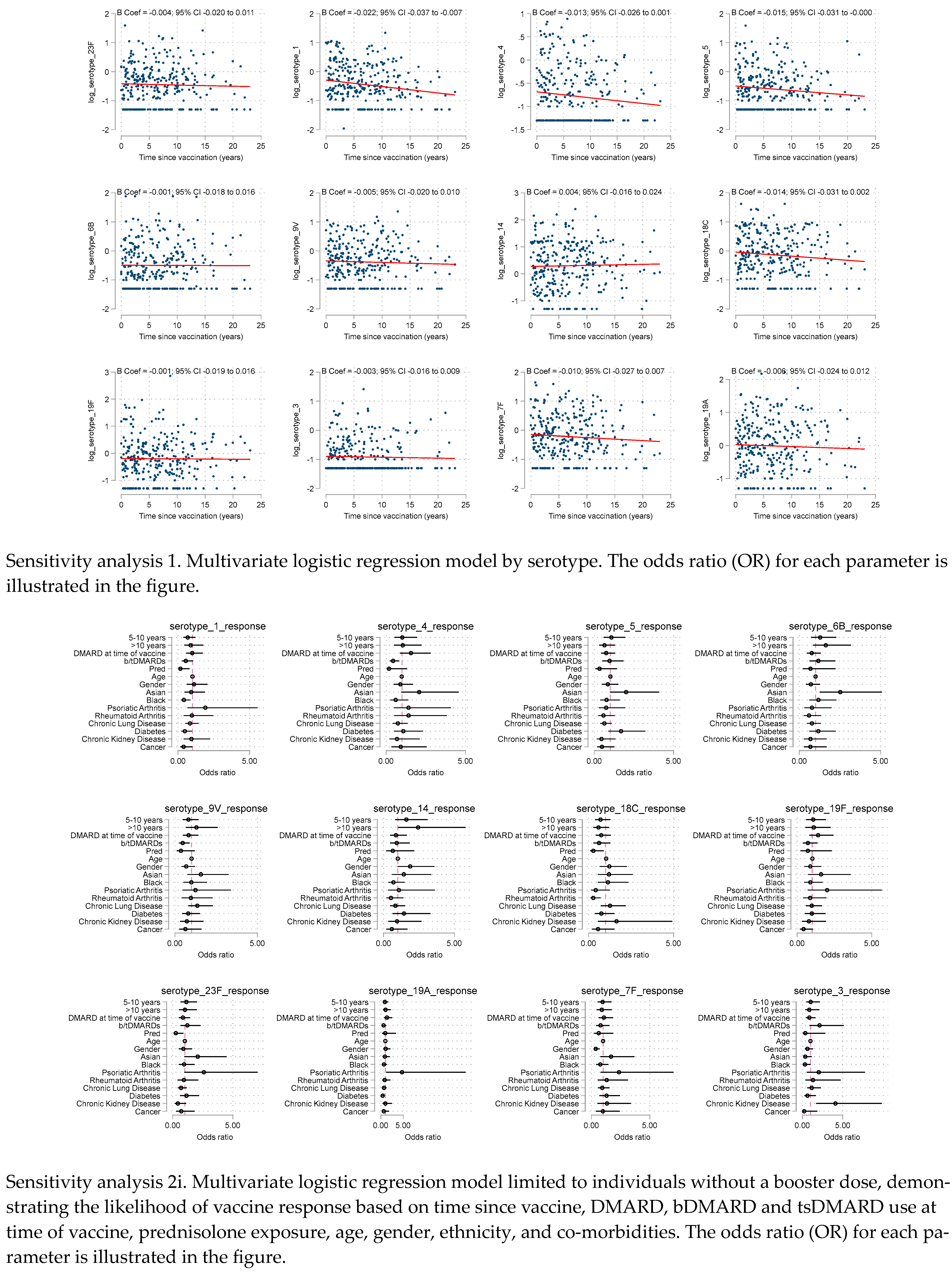
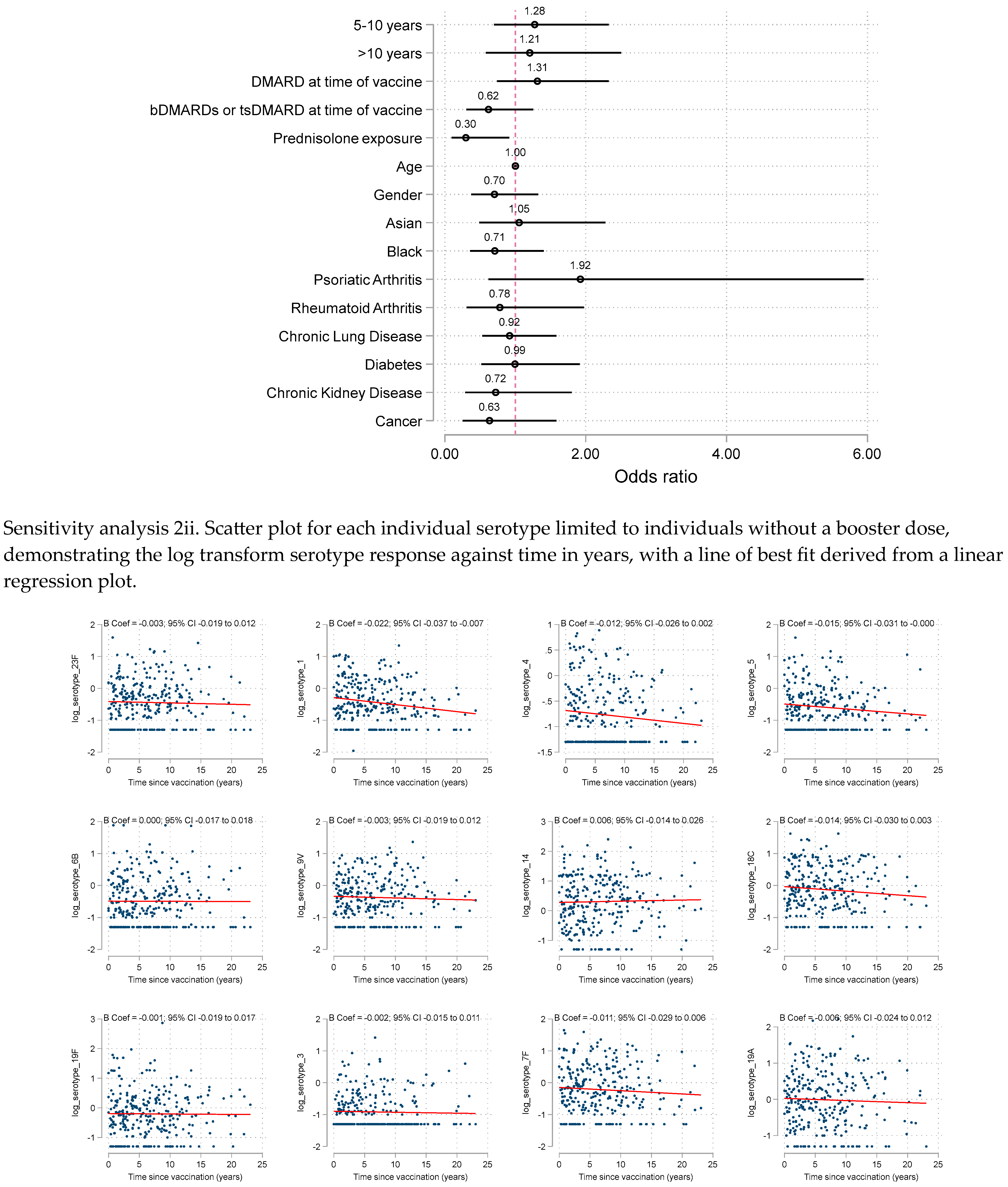
3.4. Sensitivity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Doran, M.F.; Crowson, C.S.; Pond, G.R.; O’Fallon, W.M.; Gabriel, S.E. Frequency of infection in patients with rheumatoid arthritis compared with controls: A population-based study. Arthritis Rheum. 2002, 46, 2287–2293. [Google Scholar] [CrossRef]
- van Aalst, M.; Lötsch, F.; Spijker, R.; van der Meer, J.T.; Langendam, M.W.; Goorhuis, A.; Grobusch, M.P.; de Bree, G.J. Incidence of invasive pneumococcal disease in immunocompromised patients: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2018, 24, 89–100. [Google Scholar] [CrossRef]
- Chen, H.; Matsumoto, H.; Horita, N.; Hara, Y.; Kobayashi, N.; Kaneko, T. Prognostic factors for mortality in invasive pneumococcal disease in adult: A system review and meta-analysis. Sci. Rep. 2021, 11, 11865. [Google Scholar] [CrossRef] [PubMed]
- Welte, T.; Torres, A.; Nathwani, D. Clinical and economic burden of community-acquired pneumonia among adults in Europe. Thorax 2012, 67, 71–79. [Google Scholar] [CrossRef]
- Mackenzie, G.A.; Hill, P.C.; Jeffries, D.J.; Ndiaye, M.; Sahito, S.M.; Hossain, I.; Uchendu, U.; Ameh, D.; Adeyemi, O.; Pathirana, J.; et al. Impact of the introduction of pneumococcal conjugate vaccination on invasive pneumococcal disease and pneumonia in The Gambia: 10 years of population-based surveillance. Lancet Infect. Dis. 2021, 21, 1293–1302. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Douiri, A.; Gulliford, M. Pneumonia incidence trends in UK primary care from 2002 to 2017: Population-based cohort study. Epidemiol. Infect. 2019, 147, e263. [Google Scholar] [CrossRef]
- Chen, Z.; Cox, K.S.; Tang, A.; Roman, J.; Fink, M.; Kaufhold, R.M.; Guan, L.; Xie, A.; Boddicker, M.A.; Mcguinness, D.; et al. Human monoclonal antibodies isolated from a primary pneumococcal conjugate Vaccinee demonstrates the expansion of an antigen-driven Hypermutated memory B cell response. BMC Infect. Dis. 2018, 18, 613. [Google Scholar] [CrossRef] [PubMed]
- Papadatou, I.; Tzovara, I.; Licciardi, P.V. The Role of Serotype-Specific Immunological Memory in Pneumococcal Vaccination: Current Knowledge and Future Prospects. Vaccines 2019, 7, 13. [Google Scholar] [CrossRef]
- Agency UHS. Pneumococcal: The Green Book, Chapter 25. 2023. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1178054/Green_Book_Chapter_25_Pneumococcal_27_7_23.pdf (accessed on 22 September 2023).
- Constantinou, C.A.; Ziogas, D.C.; Venetsanopoulou, A.; Gamaletsou, M.N.; Koutsogeorgopoulou, L.; Barbouni, A.; Tzioufas, A.G.; Sipsas, N.V. A clinical audit of pneumococcal vaccination among patients with autoimmune rheumatic diseases living in Greece: The power of awareness. Vaccine 2021, 39, 1593–1597. [Google Scholar] [CrossRef]
- Nagra, D.; Bechman, K.; Adas, M.; Yang, Z.; Alveyn, E.; Subesinghe, S.; Rutherford, A.; Allen, V.; Patel, S.; Russell, M.D.; et al. A Systematic Review and Meta-Analysis of Anti-Rheumatic Drugs and Pneumococcal Vaccine Immunogenicity in Inflammatory Arthritis. Vaccines 2023, 11, 1680. [Google Scholar] [CrossRef]
- Jacobsen, H.; Sitaras, I.; Katzmarzyk, M.; Cobos Jiménez, V.; Naughton, R.; Higdon, M.M.; Deloria Knoll, M. Systematic review and meta-analysis of the factors affecting waning of post-vaccination neutralizing antibody responses against SARS-CoV-2. NPJ Vaccines 2023, 8, 159. [Google Scholar] [CrossRef] [PubMed]
- Essink, B.; Sabharwal, C.; Cannon, K.; Frenck, R.; Lal, H.; Xu, X.; Sundaraiyer, V.; Peng, Y.; Moyer, L.; Pride, M.W.; et al. Pivotal Phase 3 Randomized Clinical Trial of the Safety, Tolerability, and Immunogenicity of 20-Valent Pneumococcal Conjugate Vaccine in Adults Aged ≥ 18 Years. Clin. Infect. Dis. 2022, 75, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Wolf, A.-S.; Mitsi, E.; Jones, S.; Jochems, S.P.; Roalfe, L.; Thindwa, D.; Meiring, J.E.; Msefula, J.; Bonomali, F.; Jere, T.M.; et al. Quality of antibody responses by adults and young children to 13-valent pneumococcal conjugate vaccination and Streptococcus pneumoniae colonisation. Vaccine 2022, 40, 7201–7210. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune Correlates Analysis of the mRNA-1273 COVID-19 Vaccine Efficacy Trial. medRxiv 2021. [Google Scholar] [CrossRef]
- de Gier, B.; Huiberts, A.J.; Hoeve, C.E.; den Hartog, G.; van Werkhoven, H.; van Binnendijk, R.; Hahné, S.J.; de Melker, H.E.; van den Hof, S.; Knol, M.J. Effects of COVID-19 vaccination and previous infection on Omicron SARS-CoV-2 infection and relation with serology. Nat. Commun. 2023, 14, 4793. [Google Scholar] [CrossRef]
- Jackson, L.A.; Gurtman, A.; van Cleeff, M.; Jansen, K.U.; Jayawardene, D.; Devlin, C.; Scott, D.A.; Emini, E.A.; Gruber, W.C.; Schmoele-Thoma, B. Immunogenicity and safety of a 13-valent pneumococcal conjugate vaccine compared to a 23-valent pneumococcal polysaccharide vaccine in pneumococcal vaccine-naive adults. Vaccine 2013, 31, 3577–3584. [Google Scholar] [CrossRef]
- Wernette, C.M.; Frasch, C.E.; Madore, D.; Carlone, G.; Goldblatt, D.; Plikaytis, B.; Benjamin, W.; Quataert, S.A.; Hildreth, S.; Sikkema, D.J.; et al. Enzyme-linked immunosorbent assay for quantitation of human antibodies to pneumococcal polysaccharides. Clin. Vaccine Immunol. 2003, 10, 514–519. [Google Scholar] [CrossRef]
- LaFon, D.C.; Nahm, M.H. Measuring immune responses to pneumococcal vaccines. J. Immunol. Methods 2018, 461, 37–43. [Google Scholar] [CrossRef]
- Groenwold, R.H.; White, I.R.; Donders, A.R.T.; Carpenter, J.R.; Altman, D.G.; Moons, K.G. Missing covariate data in clinical research: When and when not to use the missing-indicator method for analysis. CMAJ 2012, 184, 1265–1269. [Google Scholar] [CrossRef]
- Mufson, M.A. Antibody response of pneumococcal vaccine: Need for booster dosing? Int. J. Antimicrob. Agents 2000, 14, 107–112. [Google Scholar] [CrossRef]
- Mufson, M.A.; Krause, H.E.; Schiffman, G.; Hughey, D.F. Pneumococcal antibody levels one decade after immunization of healthy adults. Am. J. Med. Sci. 1987, 293, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Balmer, P.; Cant, A.J.; Borrow, R. Anti-pneumococcal antibody titre measurement: What useful information does it yield? J. Clin. Pathol. 2007, 60, 345–450. [Google Scholar] [CrossRef]
- Swarthout, T.D.; Henrion, M.Y.R.; Thindwa, D.; Meiring, J.E.; Mbewe, M.; Kalizang’oma, A.; Brown, C.; Msefula, J.; Moyo, B.; Mataya, A.A.; et al. Waning of antibody levels induced by a 13-valent pneumococcal conjugate vaccine, using a 3 + 0 schedule, within the first year of life among children younger than 5 years in Blantyre, Malawi: An observational, population-level, serosurveillance study. Lancet Infect. Dis. 2022, 22, 1737–1747. [Google Scholar] [CrossRef] [PubMed]
- Van Westen, E.; Knol, M.J.; Wijmenga-Monsuur, A.J.; Tcherniaeva, I.; Schouls, L.M.; Sanders, E.A.; Van Els, C.A.; Berbers, G.A.; Rots, N.Y. Serotype-Specific IgG Antibody Waning after Pneumococcal Conjugate Primary Series Vaccinations with either the 10-Valent or the 13-Valent Vaccine. Vaccines 2018, 6, 82. [Google Scholar] [CrossRef]
- Garcia Garrido, H.M.; Vollaard, A.; D’haens, G.R.; Spuls, P.I.; Bemelman, F.J.; Tanck, M.W.; de Bree, G.J.; Meek, B.; Grobusch, M.P.; Goorhuis, A. Immunogenicity of the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) Followed by the 23-Valent Pneumococcal Polysaccharide Vaccine (PPSV23) in Adults with and without Immunosuppressive Therapy. Vaccines 2022, 10, 795. [Google Scholar] [CrossRef] [PubMed]
- Azzolini, E.; Pozzi, C.; Germagnoli, L.; Oresta, B.; Carriglio, N.; Calleri, M.; Selmi, C.; De Santis, M.; Finazzi, S.; Carlo-Stella, C.; et al. mRNA COVID-19 vaccine booster fosters B- and T-cell responses in immunocompromised patients. Life Sci. Alliance 2022, 5, e202201381. [Google Scholar] [CrossRef] [PubMed]
- Paramithiotis, E.; Sugden, S.; Papp, E.; Bonhomme, M.; Chermak, T.; Crawford, S.Y.; Demetriades, S.Z.; Galdos, G.; Lambert, B.L.; Mattison, J.; et al. Cellular Immunity Is Critical for Assessing COVID-19 Vaccine Effectiveness in Immunocompromised Individuals. Front. Immunol. 2022, 13, 880784. [Google Scholar] [CrossRef]
- Amodio, D.; Ruggiero, A.; Sgrulletti, M.; Pighi, C.; Cotugno, N.; Medri, C.; Morrocchi, E.; Colagrossi, L.; Russo, C.; Zaffina, S.; et al. Humoral and Cellular Response Following Vaccination with the BNT162b2 mRNA COVID-19 Vaccine in Patients Affected by Primary Immunodeficiencies. Front. Immunol. 2021, 12, 727850. [Google Scholar] [CrossRef]
- Intongkam, S.; Samakarnthai, P.; Pakchotanon, R.; Narongroeknawin, P.; Assavatanabodee, P.; Chaiamnuay, S. Efficacy and Safety of Hepatitis B Vaccination in Rheumatoid Arthritis Patients Receiving Disease-Modifying Antirheumatic Drugs and/or Biologics Therapy. J. Clin. Rheumatol. 2019, 25, 329–334. [Google Scholar] [CrossRef]
- Paris, K.; Sorensen, R.U. Assessment and clinical interpretation of polysaccharide antibody responses. Ann. Allergy Asthma Immunol. 2007, 99, 462–464. [Google Scholar] [CrossRef]
- Beck, S.C. Making sense of serotype-specific pneumococcal antibody measurements. Ann. Clin. Biochem. 2013, 50, 517–519. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.Y.; Immermann, F.W.; Sebastian, S.; Pride, M.W.; Pavliakova, D.; Belanger, K.A.; Watson, W.; Scott, D.A.; Sidhu, M.; Jansen, K.U.; et al. Evaluation of a Validated Luminex-Based Multiplex Immunoassay for Measuring Immunoglobulin G Antibodies in Serum to Pneumococcal Capsular Polysaccharides. mSphere 2018, 3, e00127-18. [Google Scholar] [CrossRef] [PubMed]
- Daly, T.M.; Hill, H.R. Use and clinical interpretation of pneumococcal antibody measurements in the evaluation of humoral immune function. Clin. Vaccine Immunol. 2015, 22, 148–152. [Google Scholar] [CrossRef] [PubMed]
- Agency, E.M. Prevenar 13 Suspension for Injection Pneumococcal Polysaccharide Conjugate Vaccine (13-valent, Adsorbed). Available online: https://www.ema.europa.eu/en/documents/product-information/prevenar-13-epar-product-information_en.pdf (accessed on 1 December 2023).
- Winthrop, K.L.; Silverfield, J.; Racewicz, A.; Neal, J.; Lee, E.B.; Hrycaj, P.; Gomez-Reino, J.; Soma, K.; Mebus, C.; Wilkinson, B.; et al. The effect of tofacitinib on pneumococcal and influenza vaccine responses in rheumatoid arthritis. Ann. Rheum. Dis. 2016, 75, 687–695. [Google Scholar] [CrossRef]
- Menni, C.; May, A.; Polidori, L.; Louca, P.; Wolf, J.; Capdevila, J.; Hu, C.; Ourselin, S.; Steves, C.J.; Valdes, A.M.; et al. COVID-19 vaccine waning and effectiveness and side-effects of boosters: A prospective community study from the ZOE COVID Study. Lancet Infect. Dis. 2022, 22, 1002–1010. [Google Scholar] [CrossRef]
- Strehl, C.; Ehlers, L.; Gaber, T.; Buttgereit, F. Glucocorticoids-All-Rounders Tackling the Versatile Players of the Immune System. Front. Immunol. 2019, 10, 1744. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Time Since Vaccination | ||||
|---|---|---|---|---|
| <5 Years | 5–10 Years | >10 Years | Total | |
| N = 127 | N = 97 | N = 72 | N = 296 | |
| Baseline Characteristics | ||||
| Age | 51.0 (14.9) | 56.1 (14.8) | 61.7 (15.9) | 55.3 (15.6) |
| Female | 87 (69.0%) | 77 (79.4%) | 55 (77.5%) | 219 (74.5%) |
| Ethnic Group | ||||
| Asian | 21 (16.5%) | 10 (10.3%) | 8 (11.1%) | 39 (13.2%) |
| Black | 24 (18.9%) | 16 (16.5%) | 11 (15.3%) | 51 (17.2%) |
| White | 82 (64.6%) | 71 (73.2%) | 53 (73.6%) | 206 (69.6%) |
| Rheumatic Diseases Comorbidity Index | 1.7 (1.8) | 2.0 (2.0) | 2.4 (1.8) | 2.0 (1.9) |
| Chronic Lung Disease | 41 (32.3%) | 37 (38.1%) | 26 (36.1%) | 104 (35.1%) |
| Heart Attack | 18 (14.2%) | 12 (12.4%) | 17 (23.6%) | 47 (15.9%) |
| Ischaemic Heart Disease | 15 (11.8%) | 8 (8.2%) | 15 (20.8%) | 38 (12.8%) |
| Stroke | 2 (1.6%) | 1 (1.0%) | 0 (0.0%) | 3 (1.0%) |
| Hypertension | 32 (25.2%) | 32 (33.0%) | 37 (51.4%) | 101 (34.1%) |
| Previous Fracture | 9 (7.1%) | 4 (4.1%) | 5 (6.9%) | 18 (6.1%) |
| Depression | 27 (21.4%) | 18 (18.6%) | 20 (27.8%) | 65 (22.0%) |
| Diabetes | 17 (13.4%) | 16 (16.5%) | 21 (29.2%) | 54 (18.2%) |
| Cancer | 6 (4.7%) | 9 (9.3%) | 7 (9.7%) | 22 (7.4%) |
| Peptic Ulcer Disease | 25 (19.7%) | 23 (24.0%) | 13 (18.1%) | 61 (20.7%) |
| Chronic Kidney Disease | 6 (4.7%) | 10 (10.3%) | 9 (12.5%) | 25 (8.4%) |
| Diagnosis | ||||
| Axial Spondylarthritis | 20 (15.7%) | 11 (11.3%) | 7 (9.7%) | 38 (12.8%) |
| Psoriatic Arthritis | 20 (15.7%) | 12 (12.4%) | 6 (8.3%) | 38 (12.8%) |
| Rheumatoid Arthritis | 87 (68.5%) | 74 (76.3%) | 59 (81.9%) | 220 (74.3%) |
| Rheumatoid arthritis patients only | ||||
| Seronegative | 20 (23.0%) | 25 (33.8%) | 18 (30.5%) | 63 (28.6%) |
| RF only | 11 (12.6%) | 8 (10.8%) | 11 (18.6%) | 30 (13.6%) |
| CCP only | 10 (11.5%) | 7 (9.5%) | 4 (6.8%) | 21 (9.5%) |
| Double (RF & CCP) antibody positive | 46 (52.9%) | 34 (45.9%) | 26 (44.1%) | 106 (48.2%) |
| Treatment at time of vaccine | ||||
| Prednisolone at time of vaccine | 10 (7.9%) | 5 (5.2%) | 0 (0.0%) | 15 (5.1%) |
| DMARD at time of vaccine | 62 (48.8%) | 49 (50.5%) | 15 (20.8%) | 126 (42.6%) |
| Biologic at time of vaccine | 36 (28.3%) | 16 (16.5%) | 6 (8.3%) | 58 (19.6%) |
| 21 (16.5%) | 8 (8.2%) | 3 (4.2%) | 32 (10.8%) |
| 15 (11.8%) | 8 (8.2%) | 3 (4.2%) | 26 (8.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagra, D.; Bechman, K.; Russell, M.D.; Yang, Z.; Adas, M.; Subesinghe, S.; Rutherford, A.; Alveyn, E.; Patel, S.; Wincup, C.; et al. No Waning of Pneumococcal Vaccine Responses over Time in People with Inflammatory Arthritis: Findings from a Single Centre Cohort. Vaccines 2024, 12, 69. https://doi.org/10.3390/vaccines12010069
Nagra D, Bechman K, Russell MD, Yang Z, Adas M, Subesinghe S, Rutherford A, Alveyn E, Patel S, Wincup C, et al. No Waning of Pneumococcal Vaccine Responses over Time in People with Inflammatory Arthritis: Findings from a Single Centre Cohort. Vaccines. 2024; 12(1):69. https://doi.org/10.3390/vaccines12010069
Chicago/Turabian StyleNagra, Deepak, Katie Bechman, Mark D. Russell, Zijing Yang, Maryam Adas, Sujith Subesinghe, Andrew Rutherford, Edward Alveyn, Samir Patel, Chris Wincup, and et al. 2024. "No Waning of Pneumococcal Vaccine Responses over Time in People with Inflammatory Arthritis: Findings from a Single Centre Cohort" Vaccines 12, no. 1: 69. https://doi.org/10.3390/vaccines12010069
APA StyleNagra, D., Bechman, K., Russell, M. D., Yang, Z., Adas, M., Subesinghe, S., Rutherford, A., Alveyn, E., Patel, S., Wincup, C., Mahto, A., Baldwin, C., Karafotias, I., Cope, A., Norton, S., & Galloway, J. (2024). No Waning of Pneumococcal Vaccine Responses over Time in People with Inflammatory Arthritis: Findings from a Single Centre Cohort. Vaccines, 12(1), 69. https://doi.org/10.3390/vaccines12010069