
Gender Differences of the Effect of Vaccination on Perceptions of COVID-19 and Mental Health in Japan


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Ethical Considerations
2.3. Measurements
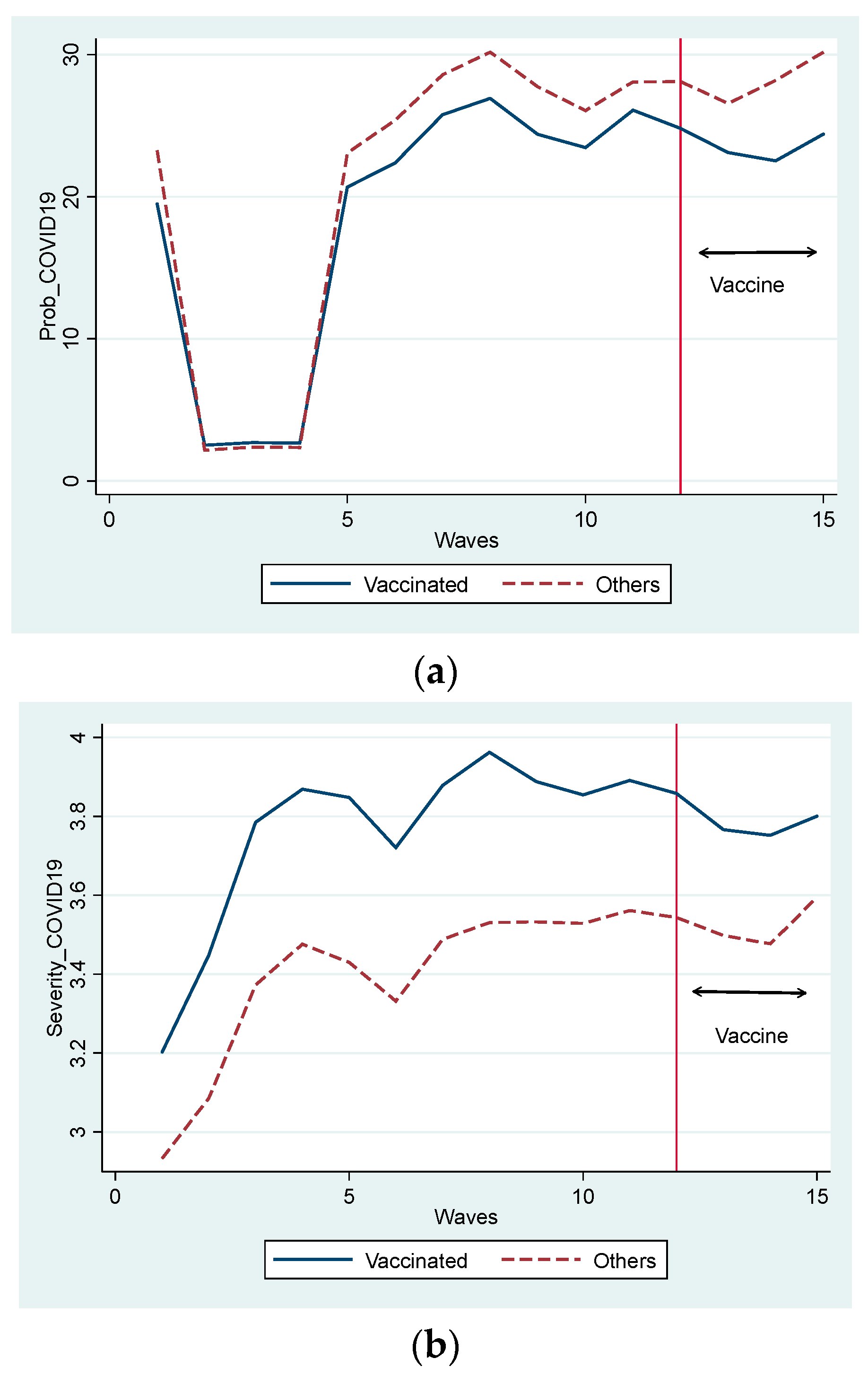
According to you, what is the probability (%) of you getting infected with SARS-COV-2 within a month from now? “What percentage do you think is the probability of your contracting COVID-19? Choose a percentage from 0 to 100 (%).”
“How serious are your symptoms if you are infected with the novel coronavirus?
Choose from six choices: 1 (very small influence) to 6 (death).”
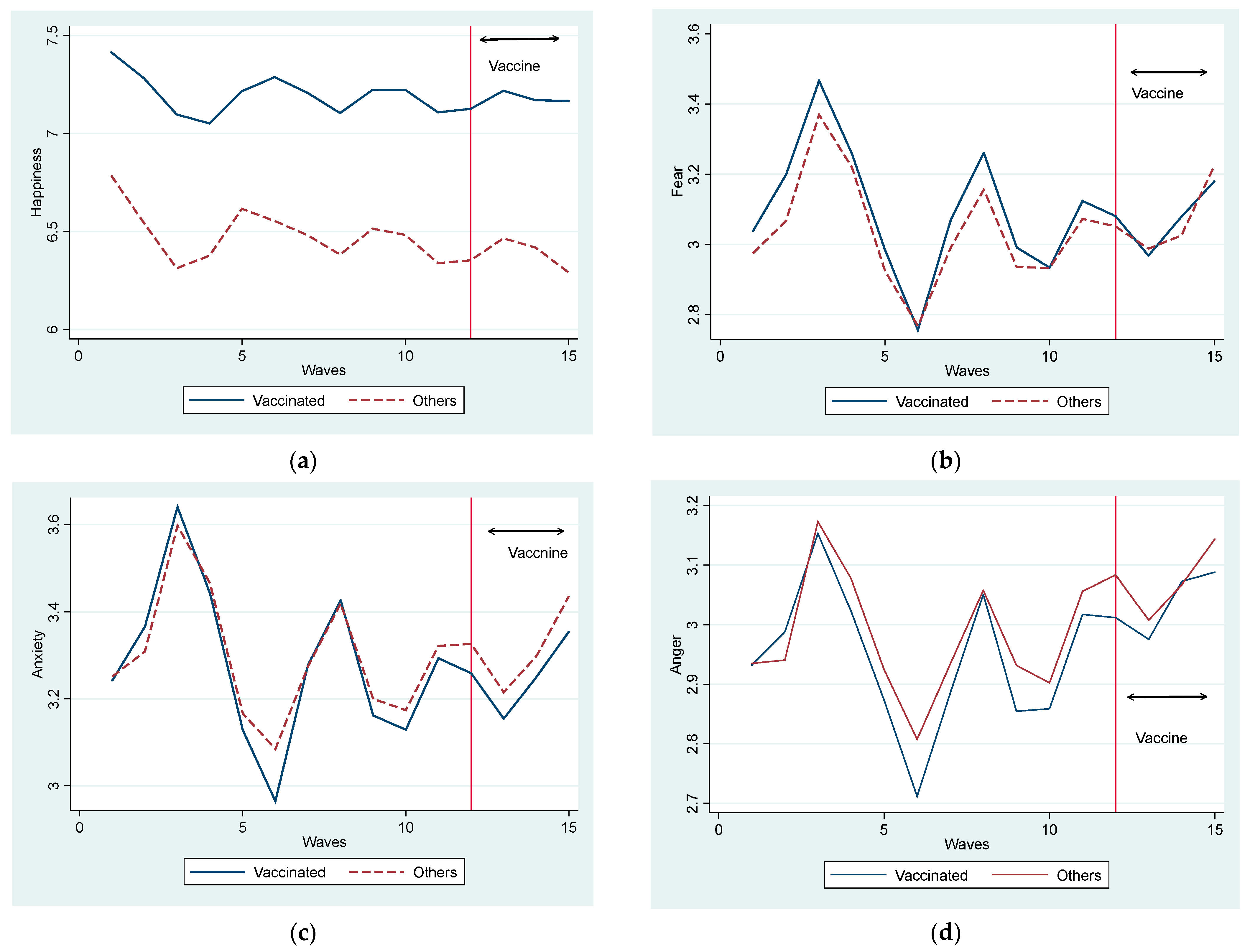
“How happy do you feel now?
Please answer on a scale from 1 (very unhappy) to 11 (very happy).”
In the last two weeks, to what extent have you felt anger, fear, and anxiety? Please indicate from 1 (I have not felt the emotion in the slightest) to 5 (I have felt the emotion stronger than ever).
2.4. Regression Model
3. Results
3.1. Full Sample Estimations
3.2. Subsample Estimations (Male vs. Female Groups)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. WHO Coronavirus (COVID-19) Dashboard WHO Coronavirus Disease (COVID-19). Available online: https://covid19.who.int/ (accessed on 20 August 2021).
- Randolph, H.E.; Barreiro, L.B. Herd Immunity: Understanding COVID-19. Immunity 2020, 52, 737–741. [Google Scholar] [CrossRef] [PubMed]
- Machingaidze, S.; Wiysonge, C.S. Understanding COVID-19 Vaccine Hesitancy. Nat. Med. 2021, 27, 1338–1339. [Google Scholar] [CrossRef] [PubMed]
- Lucia, V.C.; Kelekar, A.; Afonso, N.M. COVID-19 Vaccine Hesitancy among Medical Students. J. Public Health 2021, 43, 445–449. [Google Scholar] [CrossRef] [PubMed]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 Vaccine Acceptance and Hesitancy in Low- and Middle-Income Countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Murphy, J.; Vallières, F.; Bentall, R.P.; Shevlin, M.; McBride, O.; Hartman, T.K.; McKay, R.; Bennett, K.; Mason, L.; Gibson-Miller, J.; et al. Psychological Characteristics Associated with COVID-19 Vaccine Hesitancy and Resistance in Ireland and the United Kingdom. Nat. Commun. 2021, 12, 29. [Google Scholar] [CrossRef]
- Almaghaslah, D.; Alsayari, A.; Kandasamy, G.; Vasudevan, R. COVID-19 Vaccine Hesitancy among Young Adults in Saudi Arabia: A Cross-Sectional Web-Based Study. Vaccines 2021, 9, 330. [Google Scholar] [CrossRef]
- Mottaleb, K.A.; Mainuddin, M.; Sonobe, T. COVID-19 Induced Economic Loss and Ensuring Food Security for Vulnerable Groups: Policy Implications from Bangladesh. PLoS ONE 2020, 15, e0240709. [Google Scholar] [CrossRef]
- Inoue, H.; Murase, Y.; Todo, Y. Do Economic Effects of the Anti-COVID-19 Lockdowns in Different Regions Interact through Supply Chains? PLoS ONE 2021, 16, e0255031. [Google Scholar] [CrossRef]
- Chinna, K.; Sundarasen, S.; Khoshaim, H.B.; Kamaludin, K.; Nurunnabi, M.; Baloch, G.M.; Hossain, S.F.A.; Sukayt, A.; Dalina, N.; Rajagopalan, U.; et al. Psychological Impact of COVID-19 and Lock down Measures: An Online Cross-Sectional Multicounty Study on Asian University Students. PLoS ONE 2021, 16, e0253059. [Google Scholar] [CrossRef]
- Fiorenzato, E.; Zabberoni, S.; Costa, A.; Cona, G. Cognitive and Mental Health Changes and Their Vulnerability Factors Related to COVID-19 Lockdown in Italy. PLoS ONE 2021, 16, e0246204. [Google Scholar] [CrossRef]
- Greyling, T.; Rossouw, S.; Adhikari, T. The Good, the Bad and the Ugly of Lockdowns during COVID-19. PLoS ONE 2021, 16, e0245546. [Google Scholar] [CrossRef]
- Ogden, R. Distortions to the Passage of Time during England’s Second National Lockdown: A Role for Depression. PLoS ONE 2021, 16, e0250412. [Google Scholar] [CrossRef]
- Yamamura, E.; Tsutsui, Y. Impact of the State of Emergency Declaration for COVID-19 on Preventive Behaviours and Mental Conditions in Japan: Difference in Difference Analysis Using Panel Data. COVID Econ. Vetted Real-Time Pap. 2020, 23, 303–324. [Google Scholar]
- Watanabe, T.; Yabu, T. Japan’s Voluntary Lockdown. PLoS ONE 2021, 16, e0252468. [Google Scholar] [CrossRef]
- Muto, K.; Yamamoto, I.; Nagasu, M.; Tanaka, M.; Wada, K. Japanese Citizens’ Behavioral Changes and Preparedness against COVID-19: An Online Survey during the Early Phase of the Pandemic. PLoS ONE 2020, 15, e0234292. [Google Scholar] [CrossRef]
- Yamamura, E.; Tsutsui, Y. School Closures and Mental Health during the COVID-19 Pandemic in Japan. J. Popul. Econ. 2021, 34, 1261–1298. [Google Scholar] [CrossRef]
- Nagasu, M.; Yamamoto, I. Impact of Socioeconomic- And Lifestyle-Related Risk Factors on Poor Mental Health Conditions: A Nationwide Longitudinal 5-Wave Panel Study in Japan. PLoS ONE 2020, 15, e0240240. [Google Scholar] [CrossRef]
- Siva, N. Severe Mental Illness: Reassessing COVID-19 Vaccine Priorities. Lancet 2021, 397, 657. [Google Scholar] [CrossRef]
- Mazereel, V.; van Assche, K.; Detraux, J.; de Hert, M. COVID-19 Vaccination for People with Severe Mental Illness: Why, What, and How? Lancet Psychiatry 2021, 8, 444–450. [Google Scholar] [CrossRef]
- Warren, N.; Kisely, S.; Siskind, D. Maximizing the Uptake of a COVID-19 Vaccine in People with Severe Mental Illness: A Public Health Priority. JAMA Psychiatry 2021, 78, 589–590. [Google Scholar] [CrossRef]
- Maliki, I.; Elmsellem, H.; Hafez, B.; El Moussaoui, A.; Kachmar, M.R.; Ouahbi, A. The Psychological Properties of the Arabic BDI-II and the Psychological State of the General Moroccan Population during the Mandatory Quarantine Due to the COVID-19 Pandemic. Casp. J. Environ. Sci. 2021, 19, 139–150. [Google Scholar]
- Perez-Arce, F.; Angrisani, M.; Bennett, D.; Darling, J.; Kapteyn, A.; Thomas, K. COVID-19 Vaccines and Mental Distress. PLoS ONE 2021, 16, e0256406. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Aruldass, A.R.; Cardinal, R.N. Mental Health Outcomes after SARS-CoV-2 Vaccination in the United States: A National Cross-Sectional Study. J. Affect. Disord. 2022, 298, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, M. The Psychological Benefits of COVID-19 Vaccination. Adv Public Health 2021, 2021, 1718800. [Google Scholar] [CrossRef]
- Chaudhuri, K.; Howley, P. The Impact of COVID-19 Vaccination for Mental Well-Being. Eur. Econ. Rev. 2022, 150, 104293. [Google Scholar] [CrossRef]
- Singh, G.P.; Jaswal, S. COVID Vaccination and Mental Health: An Indian Perspective. Asian J. Psychiatr. 2022, 67, 102950. [Google Scholar] [CrossRef]
- Wisnivesky, J.P.; Govindarajulu, U.; Bagiella, E.; Goswami, R.; Kale, M.; Campbell, K.N.; Meliambro, K.; Chen, Z.; Aberg, J.A.; Lin, J.J. Association of Vaccination with the Persistence of Post-COVID Symptoms. J. Gen. Intern. Med. 2022, 37, 1748–1753. [Google Scholar] [CrossRef]
- Lee, S.-E.; Shim, S.-R.; Youn, J.-H.; Han, H.-W. COVID-19 Vaccination Is Not Associated with Psychiatric Adverse Events: A Meta-Analysis. Vaccines 2023, 11, 194. [Google Scholar] [CrossRef]
- Allcott, H. Social Norms and Energy Conservation. J. Public Econ. 2011, 95, 1082–1095. [Google Scholar] [CrossRef]
- Allcott, H.; Knittel, C. Are Consumers Poorly Informed about Fuel Economy? Evidence from Two Experiments. Am. Econ. J. Econ. Policy 2019, 11, 1–37. [Google Scholar] [CrossRef]
- Sasaki, S.; Kurokawa, H.; Ohtake, F. Effective but Fragile? Responses to Repeated Nudge-Based Messages for Preventing the Spread of COVID-19 Infection. Jpn. Econ. Rev. 2021, 72, 371–408. [Google Scholar] [CrossRef]
- Sasaki, S.; Saito, T.; Ohtake, F. Nudges for COVID-19 Voluntary Vaccination: How to Explain Peer Information? Soc. Sci. Med. 2021, 292, 114561. [Google Scholar] [CrossRef]
- Roy, B.; Kumar, V.; Venkatesh, A. Health Care Workers’ Reluctance to Take the COVID-19 Vaccine: A Consumer-Marketing Approach to Identifying and Overcoming Hesitency. NEJM Catal 2020, 1. Available online: https://catalyst.nejm.org/doi/full/10.1056/CAT.20.0676 (accessed on 20 August 2021).
- Feleszko, W.; Lewulis, P.; Czarnecki, A.; Waszkiewicz, P. Flattening the Curve of COVID-19 Vaccine Rejection-An International Overview. Vaccines 2021, 9, 44. [Google Scholar] [CrossRef]
- Yamamura, E.; Tsustsui, Y. The Impact of Closing Schools on Working from Home during the COVID-19 Pandemic: Evidence Using Panel Data from Japan. Rev. Econ. Househ. 2021, 19, 41–60. [Google Scholar] [CrossRef]
- Mohapatra, S. Gender Differentiated Economic Responses to Crises in Developing Countries: Insights for COVID-19 Recovery Policies. Rev. Econ. Househ. 2021, 19, 291–306. [Google Scholar] [CrossRef]
- Yerkes, M.A.; André, S.C.H.; Besamusca, J.W.; Kruyen, P.M.; Remery, C.L.H.S.; van der Zwan, R.; Beckers, D.G.J.; Geurts, S.A.E. ‘Intelligent’ Lockdown, Intelligent Effects? Results from a Survey on Gender (in)Equality in Paid Work, the Division of Childcare and Household Work, and Quality of Life among Parents in the Netherlands during the COVID-19 Lockdown. PLoS ONE 2020, 15, e0242249. [Google Scholar] [CrossRef]
- Barber, B.M.; Odean, T. Boys Will Be Boys: Gender, Overconfidence, and Common Stock Investment. Q. J. Econ. 2001, 116, 261–292. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ghaznavi, C.; Ueda, P. Assessment of Suicide in Japan During the COVID-19 Pandemic vs Previous Years. JAMA Netw. Open 2021, 4, e2037378. [Google Scholar] [CrossRef]
- Vaccination of Health Care Workers to Begin in Japan, with Older People Slated for April. Available online: https://www.japantimes.co.jp/news/2021/02/16/national/health-care-worker-vaccination-begin/ (accessed on 20 August 2021).
- Japan Times 75% of Japan’s Older Residents Have Received First COVID-19 Vaccine Shot. Available online: https://www.japantimes.co.jp/news/2021/07/11/national/coronavirus-vaccinations-japan-tally/ (accessed on 20 August 2021).
- Japan to Start COVID-19 Vaccinations at Workplaces and Universities on June 21. Available online: https://www.japantimes.co.jp/news/2021/06/01/national/vaccinations-in-workplaces/ (accessed on 20 August 2021).
- Transition of COVID-19 Vaccination Rates by Country. Available online: https://web.sapmed.ac.jp/canmol/coronavirus/vaccine_e.html?a=1&f=y&c=1&s=y (accessed on 20 August 2021).



{kind=link}
{kind=link}
| Variables | Definition | Male (1) | Female (2) | (2)–(1) |
|---|---|---|---|---|
| PROB_ COVID19 | What percentage do you think is the probability of your getting COVID-19? 0 to 100 (%) | 18.9 | 22.0 | 3.11 *** |
| SEVER_ COVID19 | How serious are your symptoms if you are infected with the novel coronavirus? Choose from 6 choices: 1 (very small influence); 6 (death) | 3.53 | 3.62 | 0.09 *** |
| HAPPYNESS | To what degree are you currently feeling happiness? Please answer on a scale from 1 (very unhappy) to 11 (very happy) | 6.59 | 7.04 | 0.45 *** |
| FEAR | How much have you felt the emotion of fear? Please answer on a scale from 1 (I have not felt this emotion at all) to 5 (I have felt this emotion strongly). | 2.94 | 3.20 | 0.25 *** |
| ANXIETY | How much have you felt the emotion of anxiety? Please answer on a scale from 1 (I have not felt this emotion at all) to 5 (I have felt this emotion strongly). | 3.15 | 3.43 | 0.29 *** |
| ANGER | How much have you felt the emotion of anger? Please answer in a scale from 1 (I have not felt this emotion at all) to 5 (I have felt this emotion strongly). | 2.94 | 3.03 | 0.09 *** |
| VACCINE FIRST | Did you take the first shot (but not yet the second one)? 1 (Yes) or 0 (No) | 0.38 | 0.38 | 0.002 |
| VACCINE SECOND | Did you take the second shot? 1 (Yes) or 0 (No) | 0.06 | 0.06 | 0.001 |
| VACCINE SECOND_1 | 1 if they took the second shot this month; 0 otherwise | 0.03 | 0.03 | 0.0002 |
| VACCINE SECOND_2 | 1 if they took the second shot the last month; 0 otherwise | 0.02 | 0.02 | 0.001 |
| VACCINE SECOND_3 | 1 if they took the second shot two months ago; 0 otherwise | 0.006 | 0.006 | −0.0003 |
| VACCINE SECOND_4 | 1 if they took the second shot three months ago; 0 otherwise | 0.001 | 0.001 | 0.00003 |
| Nubmer of Surveys | Dates | All % | Males % | Females % | First Shot % | Second Shot% |
|---|---|---|---|---|---|---|
| 1 | 13–16 March 2020 | 0 | 0 | 0 | ||
| 2 | 27–30 March 2020 | 0 | 0 | 0 | ||
| 3 | 10–13 April 2020 | 0 | 0 | 0 | ||
| 4 | 8–11 May 2020 | 0 | 0 | 0 | ||
| 5 | 12–15 June, 2020 | 0 | 0 | 0 | ||
| 6 | 23–28 October 2020 | 0 | 0 | 0 | ||
| 7 | 4–8 December 2020 | 0 | 0 | 0 | ||
| 8 | 15–19 January 2021 | 0 | 0 | 0 | ||
| 9 | 17–22 February 2021 | 0 | 0 | 0 | ||
| 10 | 24–29 March 2021 | 0 | 0 | 0 | ||
| 11 | 23–26 April 2021 | 0.2 | 0.2 | 0.2 | 0.2 | 0 |
| 12 | 28–31 May 2021 | 8.2 | 8.2 | 8.2 | 5.2 | 0.6 |
| 13 | 25–30 June 2021 | 25.1 | 24.3 | 25.9 | 19.6 | 8.0 |
| 14 | 30 July–4 August 2021 | 50.0 | 48.5 | 51.4 | 39.5 | 26.9 |
| 15 | 27 August–1 September 2021 | 64.2 | 63.7 | 64.7 | 51.3 | 91.2 |
| (1) PROB_ COVID19 | (2) SEVER_ COVID19 | (3) HAPPY | (4) FEAR | (5) ANXIETY | (6) ANGER | |
|---|---|---|---|---|---|---|
| VACCINE FIRST | −1.248 *** | −0.044 ** | 0.024 | −0.041 ** | −0.026 | −0.011 |
| VACCINE SECOND_1 | −4.369 *** | −0.173 *** | 0.063 ** | −0.078 *** | −0.059 *** | −0.023 |
| VACCINE SECOND_2 | −5.084 *** | −0.181 *** | 0.042 | −0.092 *** | −0.064 ** | 0.029 |
| VACCINE SECOND_3 | −4.980 *** | −0.142 * | 0.160 ** | −0.129 *** | −0.139 *** | −0.008 |
| VACCINE SECOND_4 | −4.821 *** | 0.041 | −0.188 | −0.017 * | −0.073 | −0.124 |
| EMERGENT | −0.007 | −0.005 | −0.015 | 0.039 ** | 0.039 *** | 0.013 ** |
| SURVEY 1 | <Default> | |||||
| SURVEY 2 | −19.385 *** | 0.184 *** | −0.173 *** | 0.119 *** | 0.083 *** | 0.023 |
| SURVEY 3 | −19.033 *** | 0.494 *** | −0.383 *** | 0.390 *** | 0.349 *** | 0.215 *** |
| SURVEY 4 | −19.107 *** | 0.582 *** | −0.349 *** | 0.181 *** | 0.155 *** | 0.081 *** |
| SURVEY 5 | 0.497 | 0.532 *** | −0.149 *** | −0.061 ** | −0.106 *** | −0.036 |
| SURVEY 6 | 2.622 *** | 0.416 *** | −0.140 *** | −0.253 *** | −0.227 *** | −0.179 *** |
| SURVEY 7 | 5.726 *** | 0.563 *** | −0.216 *** | −0.011 | 0.017 | −0.034 |
| SURVEY 8 | 6.957 *** | 0.627 *** | −0.326 *** | 0.175 *** | 0.146 *** | 0.094 *** |
| SURVEY 9 | 4.486 *** | 0.597 *** | −0.180 *** | −0.076 *** | −0.101 *** | −0.066 *** |
| SURVEY 10 | 3.474 *** | 0.588 *** | −0.194 *** | −0.084 *** | −0.109 *** | −0.061 ** |
| SURVEY 11 | 5.647 *** | 0.609 *** | −0.308 *** | 0.070 *** | 0.036 * | 0.081 *** |
| SURVEY 12 | 5.074 *** | 0.588 *** | −0.294 *** | 0.035 | 0.018 *** | 0.097 *** |
| SURVEY 13 | 4.125 *** | 0.551 *** | −0.231 *** | −0.018 | −0.057 *** | 0.058 *** |
| SURVEY 14 | 5.624 *** | 0.579 *** | −0.298 *** | 0.069 ** | 0.035 *** | 0.121 *** |
| SURVEY 15 | 7.934 *** | 0.674 *** | −0.343 *** | 0.221 *** | 0.150 *** | 0.143 *** |
| Adj R2 Obs. | 0.57 54,007 | 0.67 54,007 | 0.76 54,007 | 0.56 54,007 | 0.57 54,007 | 0.50 54,007 |
| (1) PROB_ COVID19 | (2) SEVER_ COVID19 | (3) HAPPY | (4) FEAR | (5) ANXIETY | (6) ANGER | |
|---|---|---|---|---|---|---|
| VACCINE FIRST | −1.253 *** | −0.044 ** | 0.023 | −0.040 ** | −0.025 | −0.009 |
| VACCINE SECOND_1 | −4.676 *** | −0.169 *** | 0.058 ** | −0.085 *** | −0.064 *** | −0.004 |
| Adj R2 Obs. | 0.57 54,007 | 0.67 54,007 | 0.76 54,007 | 0.56 54,007 | 0.57 54,007 | 0.50 54,007 |
| (1) PROB_ COVID19 | (2) SEVER_ COVID19 | (3) HAPPY | (4) FEAR | (5) ANXIETY | (6) ANGER | |
|---|---|---|---|---|---|---|
| VACCINE FIRST | −1.876 *** | −0.017 | 0.005 | 0.001 | 0.006 | 0.009 |
| VACCINE SECOND_1 | −3.684 *** | −0.163 *** | 0.019 | −0.038 | −0.052 * | −0.016 |
| VACCINE SECOND_2 | −5.018 *** | −0.193 *** | −0.043 | −0.044 | −0.032 | 0.040 |
| VACCINE SECOND_3 | −4.890 *** | −0.174 * | 0.133 | −0.023 | −0.063 | 0.104 |
| VACCINE SECOND_4 | −4.123 ** | −0.045 | −0.207 | −0.059 | −0.055 | −0.143 |
| Adj R2 Obs. | 0.57 27,316 | 0.65 27,316 | 0.77 27,316 | 0.56 27,316 | 0.57 27,316 | 0.57 27,316 |
| (1) PROB_ COVID19 | (2) SEVER_ COVID19 | (3) HAPPY | (4) FEAR | (5) ANXIETY | (6) ANGER | |
|---|---|---|---|---|---|---|
| VACCINE FIRST | −0.617 | −0.072 ** | 0.047 | −0.084 *** | −0.060 ** | −0.030 |
| VACCINE SECOND_1 | −5.068 *** | −0.184 *** | 0.112 *** | −0.116 *** | −0.066 ** | −0.029 |
| VACCINE SECOND_2 | −5.245 *** | −0.171 *** | 0.131 ** | −0.139 *** | −0.097 *** | 0.017 |
| VACCINE SECOND_3 | −5.043 *** | −0.109 | 0.189 * | −0.241 *** | −0.217 *** | −0.127 * |
| VACCINE SECOND_4 | −5.521 ** | 0.125 | −0.157 | −0.280 | −0.098 | −0.106 |
| Adj R2 Obs. | 0.56 26,691 | 0.68 26,691 | 0.73 26,691 | 0.54 26,691 | 0.55 26,691 | 0.48 26,691 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yamamura, E.; Kohsaka, Y.; Tsutsui, Y.; Ohtake, F. Gender Differences of the Effect of Vaccination on Perceptions of COVID-19 and Mental Health in Japan. Vaccines 2023, 11, 822. https://doi.org/10.3390/vaccines11040822
Yamamura E, Kohsaka Y, Tsutsui Y, Ohtake F. Gender Differences of the Effect of Vaccination on Perceptions of COVID-19 and Mental Health in Japan. Vaccines. 2023; 11(4):822. https://doi.org/10.3390/vaccines11040822
Chicago/Turabian StyleYamamura, Eiji, Youki Kohsaka, Yoshiro Tsutsui, and Fumio Ohtake. 2023. "Gender Differences of the Effect of Vaccination on Perceptions of COVID-19 and Mental Health in Japan" Vaccines 11, no. 4: 822. https://doi.org/10.3390/vaccines11040822
APA StyleYamamura, E., Kohsaka, Y., Tsutsui, Y., & Ohtake, F. (2023). Gender Differences of the Effect of Vaccination on Perceptions of COVID-19 and Mental Health in Japan. Vaccines, 11(4), 822. https://doi.org/10.3390/vaccines11040822