
Immunogenicity of BNT162b2, BBIBP-CorV, Gam-COVID-Vac and ChAdOx1 nCoV-19 Vaccines Six Months after the Second Dose: A Longitudinal Prospective Study

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
Inclusion and Exclusion Criteria
2.2. Sample Collection and Measurement of IgG Antibody Levels against SARS-CoV-2 Spike Protein
2.3. Statistical Analyses
2.4. Ethical Considerations
3. Results
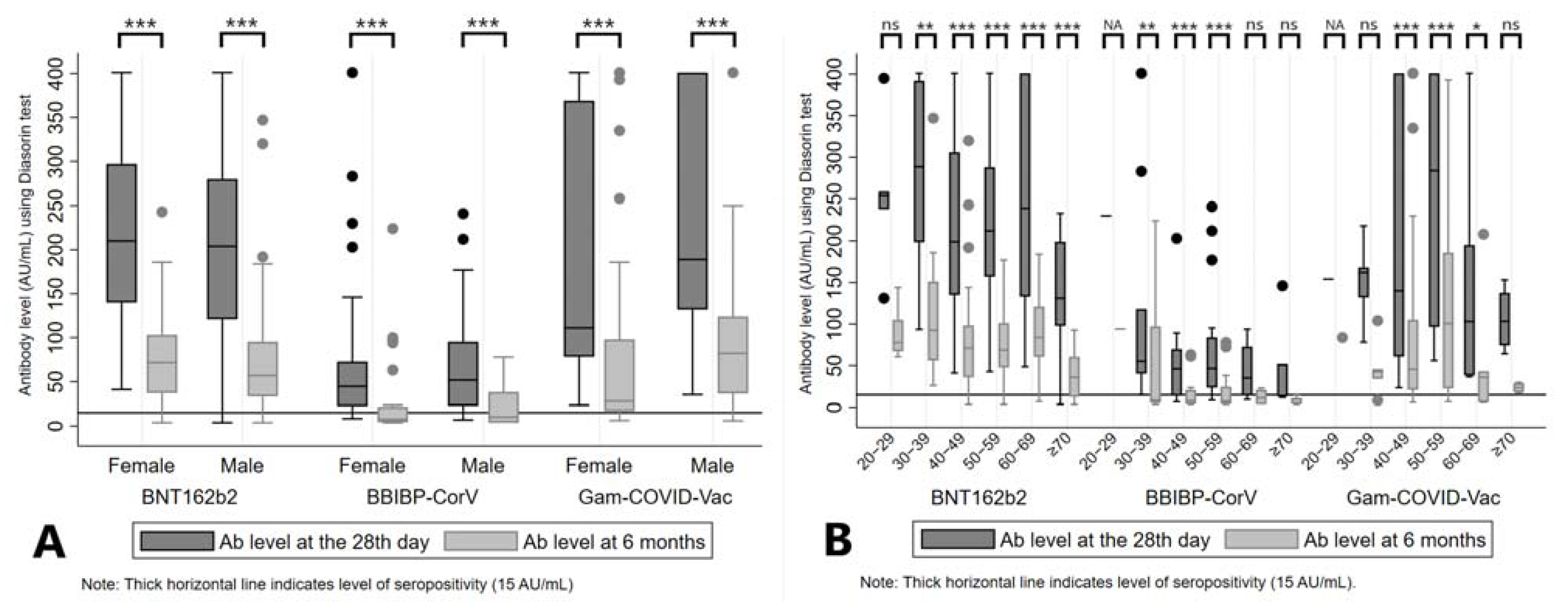
3.1. Longitudinal Course of the SARS-CoV-2 IgG Levels after Vaccination
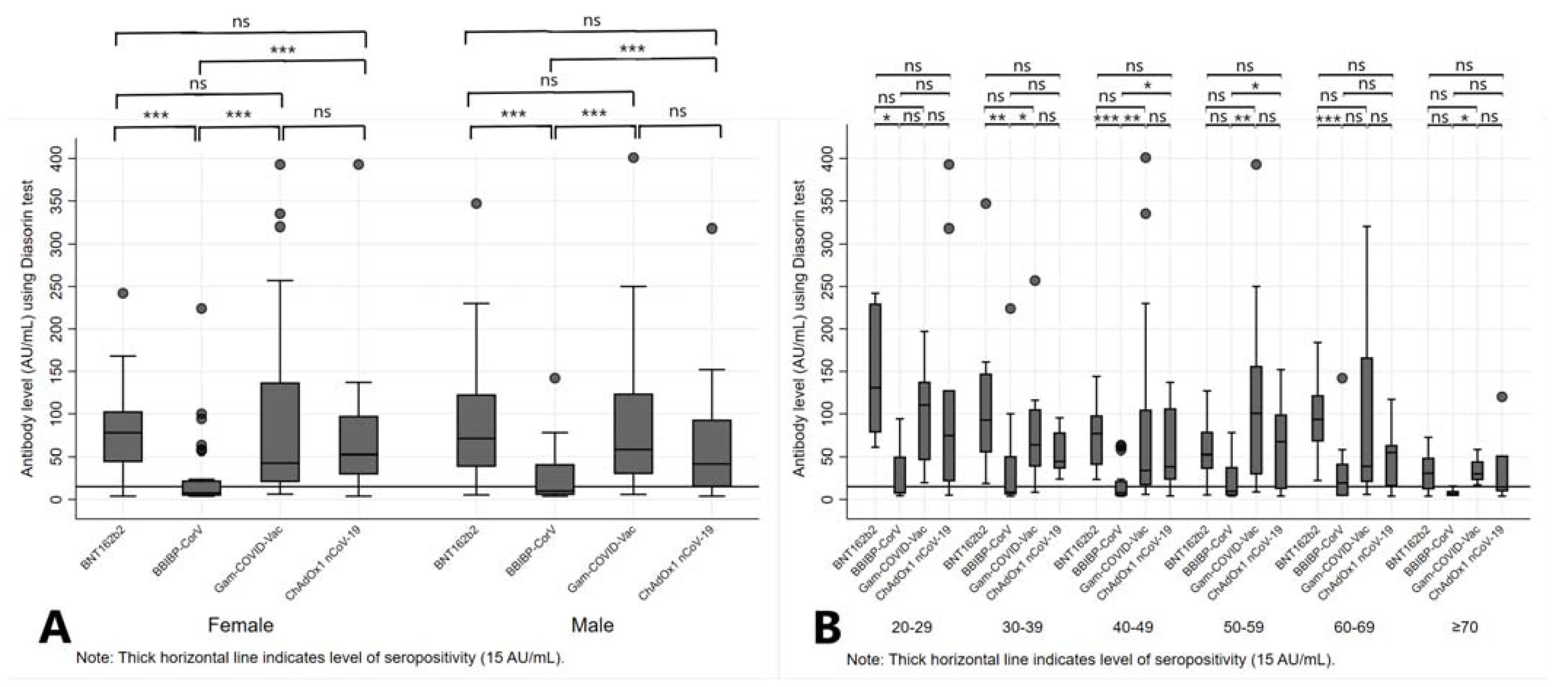
3.2. SARS-CoV-2 IgG Levels at Six Months after the Second Dose of Vaccine


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| BNT162b2 Vaccine | BBIBP-CorV Vaccine | Gam-COVID-Vac Vaccine | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean (SD), %-Change | Median, %-Change | IQR (25–75) | p-Value 1 | Mean (SD), %-Change | Median, %-Change | IQR (25–75) | p-Value 1 | Mean (SD), %-Change | Median, %-Change | IQR (25–75) | p-Value 1 | ||||
| Total | −66.64 (17.18) | −68.43 | −78.53 | −59.34 | NA | −69.47 (17.22) | −71.07 | −81.12 | −60.40 | NA | −61.93 (25.65) | −69.57 | −79.61 | −44.15 | NA |
| Sex | |||||||||||||||
| Female | −66.60 (15.66) | −68.72 | −79.05 | −58.80 | 0.68 | −70.29 (15.36) | −69.61 | −80.51 | −60.40 | 0.91 | −62.69 (26.73) | −70.07 | −81.71 | −53.62 | 0.62 |
| Male | −66.70 (19.21) | −68.35 | −78.45 | −59.34 | −68.00 (20.50) | −73.66 | −81.98 | −57.42 | −60.56 (24.29) | −69.08 | −77.90 | −42.64 | |||
| Age category | |||||||||||||||
| 20–29 | −63.13 (9.89) | −63.54 | −69.41 | −59.46 | 0.74 | −59.13 | −59.13 | 0.69 | −45.65 | −45.65 | 0.47 | ||||
| 30–39 | −59.87 (20.67) | −67.74 | −73.82 | −48.36 | −63.90 (24.87) | −75.07 | −81.12 | −44.14 | −70.31 (20.74) | −79.04 | −79.70 | −67.73 | |||
| 40–49 | −68.73 (16.67) | −70.07 | −79.27 | −64.32 | −66.72 (19.14) | −69.28 | −78.46 | −59.80 | −52.39 (30.19) | −61.03 | −75.93 | −38.50 | |||
| 50–59 | −66.97 (14.90) | −66.77 | −78.53 | −57.48 | −74.37 (12.67) | −76.86 | −83.85 | −62.95 | −62.42 (26.44) | −69.57 | −79.53 | −40.20 | |||
| 60–69 | −65.95 (14.41) | −72.12 | −74.51 | −50.15 | −69.71 (9.10) | −69.53 | −77.37 | −62.05 | −73.79 (13.65) | −77.90 | −83.78 | −65.15 | |||
| ≥70 | −67.18 (22.48) | −68.43 | −85.11 | −58.80 | −75.60 (11.06) | −71.07 | −80.43 | −69.57 | −73.68 (15.50) | −75.44 | −86.76 | −60.60 | |||
3.3. Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pollard, C.A.; Morran, M.P.; Nestor-Kalinoski, A.L. The COVID-19 pandemic: A global health crisis. Physiol. Genomics 2020, 52, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Gebru, A.A.; Birhanu, T.; Wendimu, E.; Ayalew, A.F.; Mulat, S.; Abasimel, H.Z.; Kazemi, A.; Tadesse, B.A.; Gebru, B.A.; Deriba, B.S.; et al. Global burden of COVID-19: Situational analyis and review. Hum. Antibodies 2021, 29, 139–148. [Google Scholar] [CrossRef] [PubMed]
- Jeyanathan, M.; Afkhami, S.; Smaill, F.; Miller, M.S.; Lichty, B.D.; Xing, Z. Immunological considerations for COVID-19 vaccine strategies. Nat. Rev. Immunol. 2020, 20, 615–632. [Google Scholar] [CrossRef] [PubMed]
- Papadopoli, R.; De Sarro, C.; Palleria, C.; Gallelli, L.; Pileggi, C.; De Sarro, G. Serological Response to SARS-CoV-2 Messenger RNA Vaccine: Real-World Evidence from Italian Adult Population. Vaccines 2021, 9, 1494. [Google Scholar] [CrossRef]
- Creech, C.B.; Walker, S.C.; Samuels, R.J. SARS-CoV-2 Vaccines. JAMA 2021, 325, 1318. [Google Scholar] [CrossRef]
- Krammer, F. A correlate of protection for SARS-CoV-2 vaccines is urgently needed. Nat. Med. 2021, 27, 1147–1148. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control (ECDC). Key Aspects Regarding the Introduction and Prioritisation of COVID-19 Vaccination in the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/en/publications-data/key-aspects-regarding-introduction-and-prioritisation-covid-19-vaccination (accessed on 30 October 2022).
- Subbarao, K. The success of SARS-CoV-2 vaccines and challenges ahead. Cell Host Microbe 2021, 29, 1111–1123. [Google Scholar] [CrossRef]
- Khan, M.; Adil, S.F.; Alkhathlan, H.Z.; Tahir, M.N.; Saif, S.; Khan, M.; Khan, S.T. COVID-19: A Global Challenge with Old History, Epidemiology and Progress So Far. Molecules 2020, 26, 39. [Google Scholar] [CrossRef]
- Earle, K.A.; Ambrosino, D.M.; Fiore-Gartland, A.; Goldblatt, D.; Gilbert, P.B.; Siber, G.R.; Dull, P.; Plotkin, S.A. Evidence for antibody as a protective correlate for COVID-19 vaccines. Vaccine 2021, 39, 4423–4428. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Henry, B.; Pighi, L.; De Nitto, S.; Lippi, G. Total Anti-SARS-CoV-2 Antibodies Measured 6 Months After Pfizer-BioNTech COVID-19 Vaccination in Healthcare Workers. J. Med. Biochem. 2021, 41, 199–203. [Google Scholar] [CrossRef]
- Đaković Rode, O.; Bodulić, K.; Zember, S.; Cetinić Balent, N.; Novokmet, A.; Čulo, M.; Rašić, Ž.; Mikulić, R.; Markotić, A. Decline of Anti-SARS-CoV-2 IgG Antibody Levels 6 Months after Complete BNT162b2 Vaccination in Healthcare Workers to Levels Observed Following the First Vaccine Dose. Vaccines 2022, 10, 153. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef] [PubMed]
- Levin, E.G.; Lustig, Y.; Cohen, C.; Fluss, R.; Indenbaum, V.; Amit, S.; Doolman, R.; Asraf, K.; Mendelson, E.; Ziv, A.; et al. Waning Immune Humoral Response to BNT162b2 Covid-19 Vaccine over 6 Months. N. Engl. J. Med. 2021, 385, e84. [Google Scholar] [CrossRef] [PubMed]
- Groß, R.; Zanoni, M.; Seidel, A.; Conzelmann, C.; Gilg, A.; Krnavek, D.; Erdemci-Evin, S.; Mayer, B.; Hoffmann, M.; Pöhlmann, S.; et al. Heterologous ChAdOx1 nCoV-19 and BNT162b2 prime-boost vaccination elicits potent neutralizing antibody responses and T cell reactivity against prevalent SARS-CoV-2 variants. EBioMedicine 2022, 75, 103761. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch Institut. Epidemiologisches Bulletin 2021; Robert Koch Institut: Berlin, Germany, 2021. [Google Scholar]
- Klasse, P.J.; Nixon, D.F.; Moore, J.P. Immunogenicity of clinically relevant SARS-CoV-2 vaccines in nonhuman primates and humans. Sci. Adv. 2021, 7, eabe8065. [Google Scholar] [CrossRef] [PubMed]
- Herzberg, J.; Fischer, B.; Lindenkamp, C.; Becher, H.; Becker, A.-K.; Honarpisheh, H.; Guraya, S.Y.; Strate, T.; Knabbe, C. Persistence of Immune Response in Health Care Workers After Two Doses BNT162b2 in a Longitudinal Observational Study. Front. Immunol. 2022, 13, 839922. [Google Scholar] [CrossRef]
- Delbrück, M.; Hoehl, S.; Toptan, T.; Schenk, B.; Grikscheit, K.; Metzler, M.; Herrmann, E.; Ciesek, S. Characterization of the humoral immune response to BNT162b2 in elderly residents of long-term care facilities five to seven months after vaccination. medRxiv 2021. [Google Scholar] [CrossRef]
- Bayart, J.-L.; Douxfils, J.; Gillot, C.; David, C.; Mullier, F.; Elsen, M.; Eucher, C.; Van Eeckhoudt, S.; Roy, T.; Gerin, V.; et al. Waning of IgG, Total and Neutralizing Antibodies 6 Months Post-Vaccination with BNT162b2 in Healthcare Workers. Vaccines 2021, 9, 1092. [Google Scholar] [CrossRef]
- Ministry of Health of the Republic of Serbia and Institute of Public Health of Serbia “Dr Milan Jovanović Batut”. Stručno-Metodološko Uputsuvo za Srovođenje Vanredne Preporučene Imunizacije Protiv COVID-19 u Republici Srbiji Vakcinama: Pfizer-BioNTech COVID-19 Vaccine (Comirnaty), Gam-KOVID-Vak, SARS-CoV-2 Vaccine (Vero Cell), Inactivated, ChAdOx1 nCoV-19 Corona Virus Vaccine (Recombinant) COVISHIELD/AstraZeneca SKBio AZD1222-COVID-19 Vaccine (ChAdOx1-S(Recombinant))/COVID-19 Vaccine AstraZeneca (Vaxzevria) i SPIKEVAX (Ranije COVID-19 Vaccine Moderna). 2022. Available online: https://www.batut.org.rs/download/smuZaVanrednuPreporucenuImunizacijuProtivCOVID19.pdf (accessed on 30 October 2022).
- Petrović, V.; Vuković, V.; Marković, M.; Ristić, M. Early Effectiveness of Four SARS-CoV-2 Vaccines in Preventing COVID-19 among Adults Aged ≥60 Years in Vojvodina, Serbia. Vaccines 2022, 10, 389. [Google Scholar] [CrossRef]
- Petrović, V.; Vuković, V.; Patić, A.; Marković, M.; Ristić, M. Immunogenicity of BNT162b2, BBIBP-CorV and Gam-COVID-Vac vaccines and immunity after natural SARS-CoV-2 infection—A comparative study from Novi Sad, Serbia. PLoS ONE 2022, 17, e0263468. [Google Scholar] [CrossRef]
- Hodcroft, E.B. CoVariants: SARS-CoV-2 Mutations and Variants of Interest. Available online: https://covariants.org/per-country (accessed on 30 October 2022).
- DiaSorin—The Diagnostic Specialist. LIAISON ® SARS-CoV-2 S1/S2 IgG The Fully Automated Serology Test for the Detection of SARS-CoV-2 IgG Antibodies; DiaSorin—The Diagnostic Specialist: Saluggia, Italy, 2021. [Google Scholar]
- Morales-Núñez, J.J.; Muñoz-Valle, J.F.; Torres-Hernández, P.C.; Hernández-Bello, J. Overview of Neutralizing Antibodies and Their Potential in COVID-19. Vaccines 2021, 9, 1376. [Google Scholar] [CrossRef] [PubMed]
- Eberhardt, K.A.; Dewald, F.; Heger, E.; Gieselmann, L.; Vanshylla, K.; Wirtz, M.; Kleipass, F.; Johannis, W.; Schommers, P.; Gruell, H.; et al. Evaluation of a New Spike (S)-Protein-Based Commercial Immunoassay for the Detection of Anti-SARS-CoV-2 IgG. Microorganisms 2021, 9, 733. [Google Scholar] [CrossRef] [PubMed]
- Tian, L.; Elsheikh, E.B.; Patrone, P.N.; Kearsley, A.J.; Gaigalas, A.K.; Inwood, S.; Lin-Gibson, S.; Esposito, D.; Wang, L. Towards Quantitative and Standardized Serological and Neutralization Assays for COVID-19. Int. J. Mol. Sci. 2021, 22, 2723. [Google Scholar] [CrossRef]
- Younes, S.; Al-Jighefee, H.; Shurrab, F.; Al-Sadeq, D.W.; Younes, N.; Dargham, S.R.; Al-Dewik, N.; Qotba, H.; Syed, M.; Alnuaimi, A.; et al. Diagnostic Efficiency of Three Fully Automated Serology Assays and Their Correlation with a Novel Surrogate Virus Neutralization Test in Symptomatic and Asymptomatic SARS-COV-2 Individuals. Microorganisms 2021, 9, 245. [Google Scholar] [CrossRef]
- Dolscheid-Pommerich, R.; Bartok, E.; Renn, M.; Kümmerer, B.M.; Schulte, B.; Schmithausen, R.M.; Stoffel-Wagner, B.; Streeck, H.; Saschenbrecker, S.; Steinhagen, K.; et al. Correlation between a quantitative anti-SARS-CoV-2 IgG ELISA and neutralization activity. J. Med. Virol. 2022, 94, 388–392. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Zirou, C.; Sklirou, A.D.; Apostolakou, F.; Gumeni, S.; Charitaki, I.; Papanagnou, E.-D.; Bagratuni, T.; Liacos, C.-I.; et al. Comparative kinetics of SARS-CoV-2 anti-spike protein RBD IgGs and neutralizing antibodies in convalescent and naïve recipients of the BNT162b2 mRNA vaccine versus COVID-19 patients. BMC Med. 2021, 19, 208. [Google Scholar] [CrossRef] [PubMed]
- Salvagno, G.L.; Henry, B.M.; di Piazza, G.; Pighi, L.; De Nitto, S.; Bragantini, D.; Gianfilippi, G.L.; Lippi, G. Anti-SARS-CoV-2 Receptor-Binding Domain Total Antibodies Response in Seropositive and Seronegative Healthcare Workers Undergoing COVID-19 mRNA BNT162b2 Vaccination. Diagnostics 2021, 11, 832. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.-S.; Phua, S.K.; Liang, Y.-L.; Oh, H.M.-L.; Aw, T.-C. Robust SARS-CoV-2 Antibody Responses in Asian COVID-Naïve Subjects 180 Days after Two Doses of BNT162b2 mRNA COVID-19 Vaccine. Vaccines 2021, 9, 1241. [Google Scholar] [CrossRef]
- Nomura, Y.; Sawahata, M.; Nakamura, Y.; Koike, R.; Katsube, O.; Hagiwara, K.; Niho, S.; Masuda, N.; Tanaka, T.; Sugiyama, K. Attenuation of Antibody Titers from 3 to 6 Months after the Second Dose of the BNT162b2 Vaccine Depends on Sex, with Age and Smoking Risk Factors for Lower Antibody Titers at 6 Months. Vaccines 2021, 9, 1500. [Google Scholar] [CrossRef]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef]
- Taminato, M.; Paula Cunha Chaves, A.; Borges de Morais, R.; Vinicius Leão Moreira, L.; Dias Conte, D.; Soares Faico Filho, K.; Cristina Gabrielloni, M.; Alexandrino de Medeiros, E.; Bellei, N.; Paulo, S. Waning of SARS-CoV-2 Antibody levels response to inactivated cellular vaccine over 6 months among healthcare workers. medRxiv 2022. [Google Scholar] [CrossRef]
- Lijeskić, O.; Klun, I.; Stamenov Djaković, M.; Gligorić, N.; Štajner, T.; Srbljanović, J.; Djurković-Djaković, O. Prospective Cohort Study of the Kinetics of Specific Antibodies to SARS-CoV-2 Infection and to Four SARS-CoV-2 Vaccines Available in Serbia, and Vaccine Effectiveness: A 3-Month Interim Report. Vaccines 2021, 9, 1031. [Google Scholar] [CrossRef] [PubMed]
- Israel, A.; Shenhar, Y.; Green, I.; Merzon, E.; Golan-Cohen, A.; Schäffer, A.A.; Ruppin, E.; Vinker, S.; Magen, E. Large-Scale Study of Antibody Titer Decay following BNT162b2 mRNA Vaccine or SARS-CoV-2 Infection. Vaccines 2021, 10, 64. [Google Scholar] [CrossRef] [PubMed]
- Di Resta, C.; Ferrari, D.; Viganò, M.; Moro, M.; Sabetta, E.; Minerva, M.; Ambrosio, A.; Locatelli, M.; Tomaiuolo, R. The Gender Impact Assessment among Healthcare Workers in the SARS-CoV-2 Vaccination-An Analysis of Serological Response and Side Effects. Vaccines 2021, 9, 522. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, M.; Balena, A.; Tuccinardi, D.; Tozzi, R.; Risi, R.; Masi, D.; Caputi, A.; Rossetti, R.; Spoltore, M.E.; Filippi, V.; et al. Central obesity, smoking habit, and hypertension are associated with lower antibody titres in response to COVID-19 mRNA vaccine. Diabetes Metab. Res. Rev. 2022, 38, e3465. [Google Scholar] [CrossRef] [PubMed]
- Frasca, D.; Diaz, A.; Romero, M.; Landin, A.M.; Phillips, M.; Lechner, S.C.; Ryan, J.G.; Blomberg, B.B. Intrinsic defects in B cell response to seasonal influenza vaccination in elderly humans. Vaccine 2010, 28, 8077–8084. [Google Scholar] [CrossRef] [PubMed]
- Frasca, D.; Diaz, A.; Romero, M.; Blomberg, B.B. The generation of memory B cells is maintained, but the antibody response is not, in the elderly after repeated influenza immunizations. Vaccine 2016, 34, 2834–2840. [Google Scholar] [CrossRef]
- Wei, J.; Stoesser, N.; Matthews, P.C.; Ayoubkhani, D.; Studley, R.; Bell, I.; Bell, J.I.; Newton, J.N.; Farrar, J.; Diamond, I.; et al. Antibody responses to SARS-CoV-2 vaccines in 45,965 adults from the general population of the United Kingdom. Nat. Microbiol. 2021, 6, 1140–1149. [Google Scholar] [CrossRef]
- Szebeni, G.J.; Gémes, N.; Honfi, D.; Szabó, E.; Neuperger, P.; Balog, J.Á.; Nagy, L.I.; Szekanecz, Z.; Puskás, L.G.; Toldi, G.; et al. Humoral and Cellular Immunogenicity and Safety of Five Different SARS-CoV-2 Vaccines in Patients with Autoimmune Rheumatic and Musculoskeletal Diseases in Remission or With Low Disease Activity and in Healthy Controls: A Single Center Study. Front. Immunol. 2022, 13, 846248. [Google Scholar] [CrossRef]
- Quast, I.; Tarlinton, D. B cell memory: Understanding COVID-19. Immunity 2021, 54, 205–210. [Google Scholar] [CrossRef]
- Khodadadi, L.; Cheng, Q.; Radbruch, A.; Hiepe, F. The Maintenance of Memory Plasma Cells. Front. Immunol. 2019, 10, 721. [Google Scholar] [CrossRef]
- Dashdorj, N.J.; Wirz, O.F.; Röltgen, K.; Haraguchi, E.; Buzzanco, A.S.; Sibai, M.; Wang, H.; Miller, J.A.; Solis, D.; Sahoo, M.K.; et al. Direct comparison of antibody responses to four SARS-CoV-2 vaccines in Mongolia. Cell Host Microbe 2021, 29, 1738–1743. [Google Scholar] [CrossRef]
- Stoma, I.; Korsak, K.; Voropaev, E.; Osipkina, O.; Kovalev, A. Comparative study of immunogenicity and safety of Gam-COVID-Vac and Sinopharm BBIBP-CorV vaccines in Belarus. medRxiv 2022. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Doria-Rose, N.; Suthar, M.S.; Makowski, M.; O’Connell, S.; McDermott, A.B.; Flach, B.; Ledgerwood, J.E.; Mascola, J.R.; Graham, B.S.; Lin, B.C.; et al. Antibody Persistence through 6 Months after the Second Dose of mRNA-1273 Vaccine for Covid-19. N. Engl. J. Med. 2021, 384, 2259–2261. [Google Scholar] [CrossRef]
- Terpos, E.; Trougakos, I.P.; Apostolakou, F.; Charitaki, I.; Sklirou, A.D.; Mavrianou, N.; Papanagnou, E.-D.; Liacos, C.-I.; Gumeni, S.; Rentziou, G.; et al. Age-dependent and gender-dependent antibody responses against SARS-CoV-2 in health workers and octogenarians after vaccination with the BNT162b2 mRNA vaccine. Am. J. Hematol. 2021, 96, E257–E259. [Google Scholar] [CrossRef]
- Alqassieh, R.; Suleiman, A.; Abu-Halaweh, S.; Santarisi, A.; Shatnawi, O.; Shdaifat, L.; Tarifi, A.; Al-Tamimi, M.; Al-Shudifat, A.-E.; Alsmadi, H.; et al. Pfizer-BioNTech and Sinopharm: A Comparative Study on Post-Vaccination Antibody Titers. Vaccines 2021, 9, 1223. [Google Scholar] [CrossRef]
- Lo Sasso, B.; Giglio, R.V.; Vidali, M.; Scazzone, C.; Bivona, G.; Gambino, C.M.; Ciaccio, A.M.; Agnello, L.; Ciaccio, M. Evaluation of Anti-SARS-Cov-2 S-RBD IgG Antibodies after COVID-19 mRNA BNT162b2 Vaccine. Diagnostics 2021, 11, 1135. [Google Scholar] [CrossRef]
- Bignucolo, A.; Scarabel, L.; Mezzalira, S.; Polesel, J.; Cecchin, E.; Toffoli, G. Sex Disparities in Efficacy in COVID-19 Vaccines: A Systematic Review and Meta-Analysis. Vaccines 2021, 9, 825. [Google Scholar] [CrossRef]
- Fodor, E.; Olmos Calvo, I.; Kuten-Pella, O.; Hamar, E.; Bukva, M.; Madár, Á.; Hornyák, I.; Hinsenkamp, A.; Hetényi, R.; Földes, F.; et al. Comparison of immune activation of the COVID vaccines: ChAdOx1, BNT162b2, mRNA-1273, BBIBP-CorV, and Gam-COVID-Vac from serological human samples in Hungary showed higher protection after mRNA-based immunization. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 5297–5306. [Google Scholar] [CrossRef]
- Mudd, P.A.; Minervina, A.A.; Pogorelyy, M.V.; Turner, J.S.; Kim, W.; Kalaidina, E.; Petersen, J.; Schmitz, A.J.; Lei, T.; Haile, A.; et al. SARS-CoV-2 mRNA vaccination elicits a robust and persistent T follicular helper cell response in humans. Cell 2022, 185, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Gustafson, C.E.; Kim, C.; Weyand, C.M.; Goronzy, J.J. Influence of immune aging on vaccine responses. J. Allergy Clin. Immunol. 2020, 145, 1309–1321. [Google Scholar] [CrossRef] [PubMed]
- Naaber, P.; Tserel, L.; Kangro, K.; Sepp, E.; Jürjenson, V.; Adamson, A.; Haljasmägi, L.; Rumm, A.P.; Maruste, R.; Kärner, J.; et al. Dynamics of antibody response to BNT162b2 vaccine after six months: A longitudinal prospective study. Lancet Reg. Heal.-Eur. 2021, 10, 100208. [Google Scholar] [CrossRef] [PubMed]
- Swadźba, J.; Anyszek, T.; Panek, A.; Martin, E. Anti-Spike SARS-CoV-2 IgG Assessment with a Commercial Assay during a 4-Month Course after COVID-19 Vaccination. Vaccines 2021, 9, 1367. [Google Scholar] [CrossRef] [PubMed]
- Jordan, S.C. Innate and adaptive immune responses to SARS-CoV-2 in humans: Relevance to acquired immunity and vaccine responses. Clin. Exp. Immunol. 2021, 204, 310–320. [Google Scholar] [CrossRef]
- Goel, R.R.; Painter, M.M.; Apostolidis, S.A.; Mathew, D.; Meng, W.; Rosenfeld, A.M.; Lundgreen, K.A.; Reynaldi, A.; Khoury, D.S.; Pattekar, A.; et al. mRNA Vaccination Induces Durable Immune Memory to SARS-CoV-2 with Continued Evolution to Variants of Concern. bioRxiv 2021. [Google Scholar] [CrossRef]
- Jo, D.-H.; Minn, D.; Lim, J.; Lee, K.-D.; Kang, Y.-M.; Choe, K.-W.; Kim, K.-N. Rapidly Declining SARS-CoV-2 Antibody Titers within 4 Months after BNT162b2 Vaccination. Vaccines 2021, 9, 1145. [Google Scholar] [CrossRef]
- Peluso, M.J.; Takahashi, S.; Hakim, J.; Kelly, J.D.; Torres, L.; Iyer, N.S.; Turcios, K.; Janson, O.; Munter, S.E.; Thanh, C.; et al. SARS-CoV-2 antibody magnitude and detectability are driven by disease severity, timing, and assay. Sci. Adv. 2021, 7. [Google Scholar] [CrossRef]
- Salazar, E.; Kuchipudi, S.V.; Christensen, P.A.; Eagar, T.; Yi, X.; Zhao, P.; Jin, Z.; Long, S.W.; Olsen, R.J.; Chen, J.; et al. Convalescent plasma anti–SARS-CoV-2 spike protein ectodomain and receptor-binding domain IgG correlate with virus neutralization. J. Clin. Investig. 2020, 130, 6728–6738. [Google Scholar] [CrossRef]
- Gerges, D.; Kapps, S.; Hernández-Carralero, E.; Freire, R.; Aiad, M.; Schmidt, S.; Winnicki, W.; Reiter, T.; Pajenda, S.; Schmidt, A.; et al. Vaccination with BNT162b2 and ChAdOx1 nCoV-19 Induces Cross-Reactive Anti-RBD IgG against SARS-CoV-2 Variants including Omicron. Viruses 2022, 14, 1181. [Google Scholar] [CrossRef]
- Dejnirattisai, W.; Huo, J.; Zhou, D.; Zahradník, J.; Supasa, P.; Liu, C.; Duyvesteyn, H.M.E.; Ginn, H.M.; Mentzer, A.J.; Tuekprakhon, A.; et al. SARS-CoV-2 Omicron-B.1.1.529 leads to widespread escape from neutralizing antibody responses. Cell 2022, 185, 467–484.e15. [Google Scholar] [CrossRef]
- Stosic, M.; Milic, M.; Markovic, M.; Kelic, I.; Bukumiric, Z.; Veljkovic, M.; Kisic Tepavcevic, D.; Saponjic, V.; Plavsa, D.; Jovanovic, S.; et al. Immunogenicity and Reactogenicity of the Booster Dose of COVID-19 Vaccines and Related Factors: A Panel Study from the General Population in Serbia. Vaccines 2022, 10, 838. [Google Scholar] [CrossRef]



| Vaccine | At the 28th Day after the Second Dose | At 6 Months after the Second Dose | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | Mean (AU/mL) | SD | Median (AU/mL) | IQR (25–75) | Mean (AU/mL) | SD | Median (AU/mL) | IQR (25–75) | p-Value 1 | |||
| BNT162b2 | |||||||||||||
| Total | 130 | 100 | 216.55 | 105.7 | 209 | 135 | 288 | 75.67 | 57.3 | 67.95 | 37.3 | 101 | <0.001 |
| Sex | |||||||||||||
| Female | 75 | 57.7 | 219.24 | 102.2 | 210 | 140 | 297 | 76.54 | 49.24 | 71.6 | 37.3 | 103 | <0.001 |
| Male | 55 | 42.3 | 212.88 | 111.3 | 204 | 121 | 280 | 74.48 | 67.23 | 56.9 | 33.5 | 95.2 | <0.001 |
| Age category | |||||||||||||
| 20–29 | 5 | 3.85 | 255.4 | 93.92 | 254 | 238 | 259 | 90.9 | 34.18 | 77.7 | 67.2 | 105 | 0.063 |
| 30–39 | 12 | 9.23 | 276.46 | 108 | 288.5 | 198.5 | 392 | 117.28 | 88.45 | 92.5 | 56.1 | 151 | 0.002 |
| 40–49 | 41 | 31.5 | 217.8 | 114.6 | 199 | 135 | 306 | 76.45 | 65.31 | 70.9 | 36 | 98.2 | <0.001 |
| 50–59 | 35 | 26.9 | 222.21 | 82.61 | 212 | 157 | 288 | 75.12 | 41.68 | 68.7 | 47.7 | 101 | <0.001 |
| 60–69 | 15 | 11.5 | 255.24 | 125.2 | 239 | 133 | 401 | 88.08 | 50.57 | 83.8 | 60.5 | 121 | <0.001 |
| ≥70 | 22 | 16.9 | 137.32 | 65.34 | 131 | 97.8 | 199 | 40.47 | 27.48 | 35.8 | 12.7 | 60.6 | <0.001 |
| BBIBP-CorV | |||||||||||||
| Total | 53 | 100 | 72.74 | 80.04 | 48.1 | 22.7 | 78.6 | 24.43 | 38.43 | 8.13 | 4.37 | 21.9 | <0.001 |
| Sex | |||||||||||||
| Female | 34 | 64.2 | 72.29 | 87.2 | 44.7 | 22.3 | 72.7 | 24.94 | 44.4 | 7.61 | 4.37 | 21.4 | <0.001 |
| Male | 19 | 35.9 | 73.55 | 67.55 | 51.8 | 22.7 | 95.2 | 23.52 | 25.52 | 10 | 3.79 | 38.2 | <0.001 |
| Age category | |||||||||||||
| 20–29 | 1 | 1.89 | 230 | 230 | 94 | 94 | NA | ||||||
| 30–39 | 9 | 17 | 120.89 | 132.7 | 55.1 | 40.3 | 118 | 56.95 | 74.4 | 8.48 | 5.57 | 97.1 | 0.004 |
| 40–49 | 18 | 34 | 50.87 | 46.57 | 46.1 | 13.9 | 69.7 | 16.08 | 18.19 | 7.98 | 4.22 | 20.7 | <0.001 |
| 50–59 | 16 | 30.2 | 73.39 | 72.96 | 46.4 | 23.5 | 84 | 19.05 | 24.01 | 7.61 | 4.39 | 24.6 | <0.001 |
| 60–69 | 4 | 7.55 | 43.37 | 38.17 | 35.1 | 13.99 | 72.8 | 12.37 | 10.06 | 11.3 | 3.79 | 20.95 | 0.125 |
| ≥70 | 5 | 9.43 | 54.74 | 54.59 | 51.1 | 13.1 | 51.6 | 8.94 | 4.99 | 10 | 4.23 | 11 | 0.063 |
| Gam-COVID-Vac | |||||||||||||
| Total | 48 | 100 | 194.38 | 140.2 | 147 | 85.8 | 401 | 90.53 | 111.3 | 36.3 | 19.75 | 112 | <0.001 |
| Sex | |||||||||||||
| Female | 31 | 64.6 | 176.38 | 139.4 | 111 | 78.2 | 369 | 81.44 | 113.8 | 28 | 17 | 97.9 | <0.001 |
| Male | 17 | 35.4 | 227.21 | 140 | 189 | 132 | 401 | 107.11 | 108.1 | 82.1 | 36.7 | 124 | <0.001 |
| Age category | |||||||||||||
| 20–29 | 1 | 2.08 | 154 | 154 | 83.7 | 83.7 | NA | ||||||
| 30–39 | 5 | 10.4 | 151.64 | 51.38 | 162 | 132 | 168 | 46.96 | 35.09 | 42.6 | 34.1 | 45.7 | 0.063 |
| 40–49 | 17 | 35.4 | 201.02 | 158.5 | 140 | 60.8 | 401 | 114.36 | 138.6 | 45.5 | 21 | 105 | <0.001 |
| 50–59 | 14 | 29.2 | 257.58 | 148.4 | 284 | 96.6 | 401 | 117.51 | 117.6 | 100.55 | 22.6 | 186 | <0.001 |
| 60–69 | 7 | 14.6 | 138.71 | 129.5 | 103 | 38.1 | 195 | 49.11 | 71.89 | 35.9 | 6.18 | 43.1 | 0.016 |
| ≥70 | 4 | 8.33 | 105.9 | 39.49 | 103.2 | 74.3 | 138 | 23.48 | 6.31 | 23.6 | 18.1 | 28.85 | 0.125 |
| BNT162b2 Vaccine | BBIBP-CorV Vaccine | Gam-COVID-Vac Vaccine | ChAdOx1 nCoV-19 Vaccine | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n (%) | Mean (SD), AU/mL | Median (IQR, 25–75), AU/mL | p-Value 1 | n (%) | Mean (SD), AU/mL | Median (IQR, 25–75), AU/mL | p-Value 1 | n (%) | Mean (SD), AU/mL | Median (IQR, 25–75), AU/mL | p-Value 1 | n (%) | Mean (SD), AU/mL | Median (IQR, 25–75), AU/mL | p-Value 1 | p-Value 2 | |
| Total | 70 (100) | 85.25 (60.02) | 74.55 (42.70–109.00) | NA | 70 (100) | 25.26 (36.92) | 8.18 (4.37–27.40) | NA | 70 (100) | 91.28 (95.96) | 44.85 (25.00–127.00) | NA | 70 (100) | 64.22 (65.30) | 50.60 (19.00–93.20) | NA | <0.01 |
| Sex | |||||||||||||||||
| Female | 35 (50.00) | 81.47 (47.87) | 77.70 (43.80–103.00) | 0.91 | 35 (50.00) | 24.86 (42.68) | 7.59 (4.22–22.40) | 0.52 | 35 (50.00) | 90.44 (103.47) | 42.70 (20.30–137.00) | 0.47 | 35 (50.00) | 68.12 (69.11) | 52.40 (29.20–97.70) | 0.47 | <0.01 |
| Male | 35 (50.00) | 89.03 (70.64) | 70.90 (38.20–123.00) | 35 (50.00) | 25.65 (30.72) | 9.95 (5.20–41.60) | 35 (50.00) | 92.11 (89.33) | 57.90 (29.70–124.00) | 35 (50.00) | 60.32 (62.00) | 41.70 (14.50–93.20) | <0.01 | ||||
| Age category | |||||||||||||||||
| 20–29 | 6 (8.57) | 145.30 (79.72) | 130.75 (77.70–230.00) | <0.01 | 6 (8.57) | 28.44 (36.64) | 7.45 (7.04–50.50) | 0.69 | 8 (11.43) | 100.65 (61.23) | 110.35 (46.00–138.00) | 0.45 | 10 (14.29) | 118.10 (133.92) | 74.35 (21.10–128.00) | 0.61 | 0.06 |
| 30–39 | 12 (17.15) | 113.06 (88.31) | 92.50 (54.20–147.50) | 12 (17.15) | 40.99 (64.81) | 8.47 (5.65–51.05) | 12 (17.15) | 79.95 (65.90) | 63.40 (38.35–105.50) | 14 (20.00) | 53.44 (22.88) | 44.60 (36.10–78.30) | 0.01 | ||||
| 40–49 | 18 (25.71) | 74.38 (35.68) | 76.70 (40.40–98.20) | 18 (25.71) | 18.37 (20.67) | 7.98 (4.22–21.90) | 18 (25.71) | 93.58 (119.76) | 34.05 (16.60–105.00) | 12 (17.14) | 61.16 (47.13) | 38.35 (22.95–106.50) | <0.01 | ||||
| 50–59 | 12 (17.15) | 56.56 (35.50) | 52.40 (35.75–79.00) | 14 (20.00) | 24.86 (26.81) | 9.54 (4.40–38.20) | 12 (17.15) | 118.89 (113.21) | 100.55 (29.15–156.50) | 14 (20.00) | 64.87 (51.82) | 67.20 (12.10–99.40) | <0.01 | ||||
| 60–69 | 16 (22.85) | 95.19 (45.83) | 93.40 (67.25–122.00) | 12 (17.14) | 30.50 (40.08) | 19.30 (3.79–42.10) | 16 (22.85) | 86.17 (100.15) | 38.85 (20.30–166.50) | 14 (20.00) | 50.73 (37.65) | 54.25 (15.20–63.30) | <0.01 | ||||
| ≥70 | 6 (8.57) | 33.02 (24.99) | 30.65 (11.70–49.10) | 8 (11.43) | 7.58 (4.26) | 6.64 (3.79–10.15) | 4 (5.71) | 33.73 (17.32) | 30.00 (22.50–44.95) | 6 (8.57) | 35.67 (44.66) | 14.60 (9.25–51.80) | 0.04 | ||||
| Total | BNT162b2 Vaccine (n = 70) | BBIBP-CorV Vaccine (n = 70) | Gam-COVID-Vac Vaccine (n = 70) | ChAdOx1 nCoV-19 Vaccine (n = 70) | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sero-Negative | Equi-Vocal | Sero-Positive | p-Value 1 | Sero-Negative | Equi-Vocal | Sero-Positive | p-Value 1 | Sero-Negative | Equi-Vocal | Sero-Positive | p-Value 1 | Sero-Negative | Equi-vocal | Sero-Positive | p-Value 1 | ||
| Total,n(%) | 280 (100) | 4 (5.71) | 0 | 66 (94.29) | NA | 42 (60.00) | 0 | 28 (40.00) | NA | 10 (14.29) | 0 | 60 (85.71) | NA | 11 (15.71) | 4 (5.72) | 55 (78.57) | NA |
| Sex, n (%) | |||||||||||||||||
| Female | 140 (100) | 2 (5.71) | 0 | 33 (94.29) | 1 | 22 (62.86) | 0 | 13 (37.14) | 0.81 | 5 (14.29) | 0 | 30 (85.71) | 1 | 4 (11.43) | 2 (5.71) | 29 (82.86) | 0.69 |
| Male | 140 (100) | 2 (5.71) | 0 | 33 (94.29) | 20 (57.14) | 0 | 15 (42.86) | 5 (14.29) | 0 | 30 (85.71) | 7 (20.00) | 2 (5.71) | 26 (74.29) | ||||
| Age (years), mean (SD) | 49.17 (14.34) | 66.75 (14.68) | NA | 48.88 (14.68) | 0.02 | 50.26 (15.60) | NA | 49.54 (13.86) | 0.84 | 52.30 (9.06) | NA | 47.90 (13.76) | 0.33 | 54.00 (16.30) | 55.25 (12.95) | 46.62 (13.98) | 0.8 |
| Age category, n (%) | |||||||||||||||||
| 20–29 | 30 (100) | 0 | 0 | 6 (100) | <0.01 | 4 (66.67) | 0 | 2 (33.33) | 0.51 | 0 | 0 | 8 (100) | 0.76 | 2 (20.00) | 0 | 8 (80.00) | 0.16 |
| 30–39 | 50 (100) | 0 | 0 | 12 (100) | 7 (58.33) | 0 | 5 (41.67) | 1 (8.33) | 0 | 11 (91.67) | 0 | 0 | 14 (100) | ||||
| 40–49 | 66 (100) | 0 | 0 | 18 (100) | 11 (61.11) | 0 | 7 (38.89) | 4 (22.22) | 0 | 14 (77.78) | 1 (8.33) | 1 (8.33) | 10 (83.34) | ||||
| 50–59 | 52 (100) | 2 (16.67) | 0 | 10 (83.33) | 8 (57.14) | 0 | 6 (42.86) | 2 (16.67) | 0 | 10 (83.33) | 3 (21.43) | 2 (14.28) | 9 (64.29) | ||||
| 60–69 | 58 (100) | 0 | 0 | 16 (100) | 5 (41.67) | 0 | 7 (58.33) | 3 (18.75) | 0 | 13 (81.25) | 3 (21.43) | 0 | 11 (78.57) | ||||
| ≥70 | 24 (100) | 2 (33.33) | 0 | 4 (66.67) | 7 (87.50) | 0 | 1 (12.50) | 0 | 0 | 4 (100) | 2 (33.33) | 1 (16.67) | 3 (50.00) | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrović, V.; Vuković, V.; Patić, A.; Marković, M.; Ristić, M. Immunogenicity of BNT162b2, BBIBP-CorV, Gam-COVID-Vac and ChAdOx1 nCoV-19 Vaccines Six Months after the Second Dose: A Longitudinal Prospective Study. Vaccines 2023, 11, 56. https://doi.org/10.3390/vaccines11010056
Petrović V, Vuković V, Patić A, Marković M, Ristić M. Immunogenicity of BNT162b2, BBIBP-CorV, Gam-COVID-Vac and ChAdOx1 nCoV-19 Vaccines Six Months after the Second Dose: A Longitudinal Prospective Study. Vaccines. 2023; 11(1):56. https://doi.org/10.3390/vaccines11010056
Chicago/Turabian StylePetrović, Vladimir, Vladimir Vuković, Aleksandra Patić, Miloš Marković, and Mioljub Ristić. 2023. "Immunogenicity of BNT162b2, BBIBP-CorV, Gam-COVID-Vac and ChAdOx1 nCoV-19 Vaccines Six Months after the Second Dose: A Longitudinal Prospective Study" Vaccines 11, no. 1: 56. https://doi.org/10.3390/vaccines11010056
APA StylePetrović, V., Vuković, V., Patić, A., Marković, M., & Ristić, M. (2023). Immunogenicity of BNT162b2, BBIBP-CorV, Gam-COVID-Vac and ChAdOx1 nCoV-19 Vaccines Six Months after the Second Dose: A Longitudinal Prospective Study. Vaccines, 11(1), 56. https://doi.org/10.3390/vaccines11010056