
COVID-19 Vaccination Hesitancy among Healthcare Workers—A Review



Abstract
1. Introduction
2. Methods
3. Pre-COVID-19 Vaccine Hesitancy among Healthcare Workers
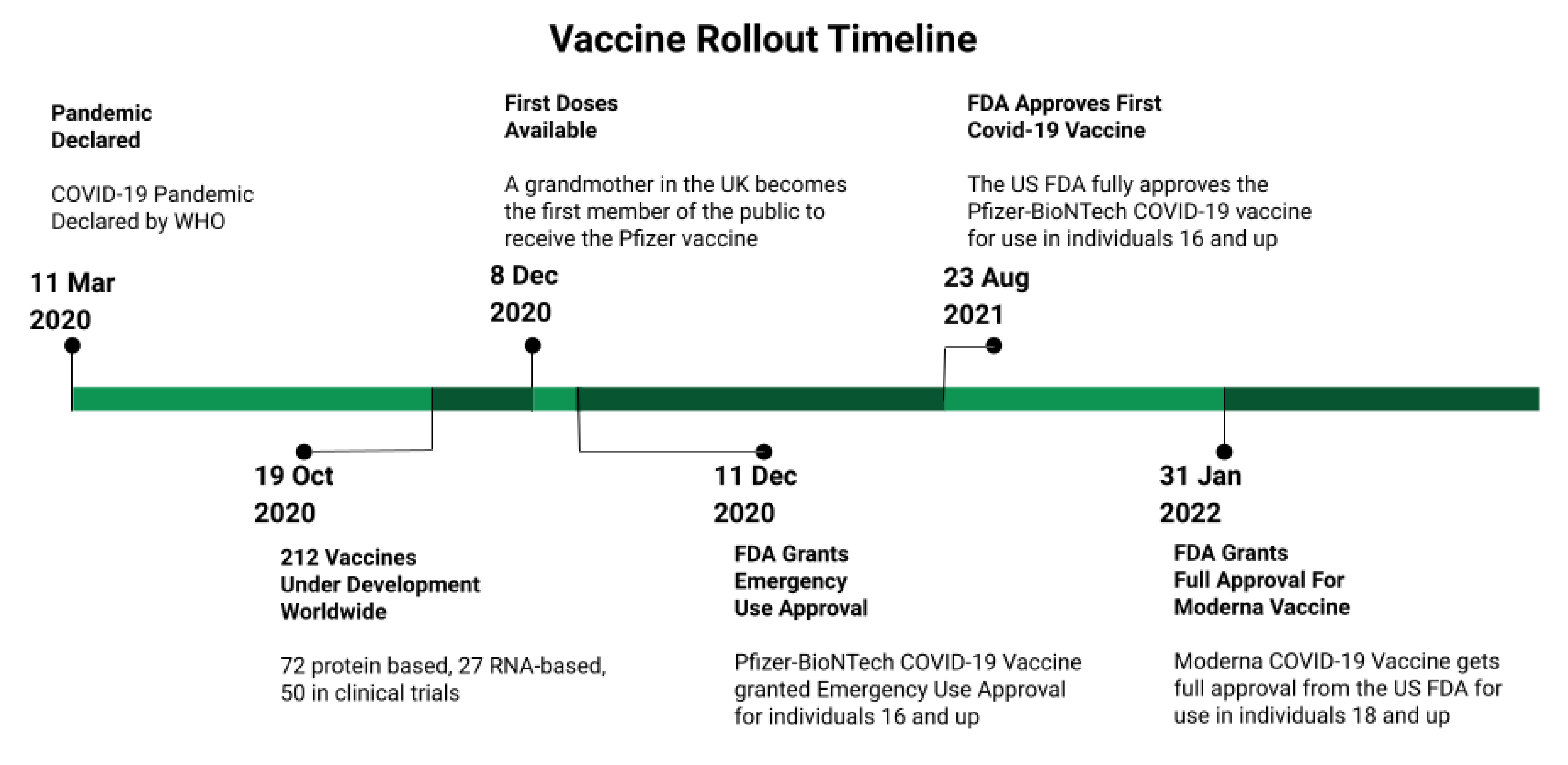
4. The COVID-19 Pandemic and Vaccine Development
5. Demographics of Vaccine Hesitant HCWs
6. Reasons for Hesitancy
6.1. Concerns about Safety and Efficacy
6.2. Waiting for More Data
6.3. Vaccines Developed Too Quickly
6.4. Distrust of Employers, Government, and Healthcare System
6.5. Infringement on Personal Rights
6.6. Vaccination Unnecessary
6.7. Other
7. Towards the Future
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haeder, S.F. Joining the herd? U.S. public opinion and vaccination requirements across educational settings during the COVID-19 pandemic. Vaccine 2021, 39, 2375–2385. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.C. Vaccine Rejection and Hesitancy: A Review and Call to Action. Open Forum Infect. Dis. 2017, 4, ofx146. [Google Scholar] [CrossRef] [PubMed]
- Klompas, M.; Pearson, M.; Morris, C. The Case for Mandating COVID-19 Vaccines for Health Care Workers. Ann. Intern. Med. 2021, 174, 1305–1307. [Google Scholar] [CrossRef] [PubMed]
- Dubé, E.; Laberge, C.; Guay, M.; Bramadat, P.; Roy, R.; Bettinger, J.A. Vaccine hesitancy. Hum. Vaccines Immunother. 2013, 9, 1763–1773. [Google Scholar] [CrossRef]
- Hakim, M.S. SARS-CoV-2, COVID-19, and the debunking of conspiracy theories. Rev. Med. Virol. 2021, 31, e2222. [Google Scholar] [CrossRef]
- Ullah, I.; Khan, K.S.; Tahir, M.J.; Ahmed, A.; Harapan, H. Myths and conspiracy theories on vaccines and COVID-19: Potential effect on global vaccine refusals. Vacunas 2021, 22, 93–97. [Google Scholar] [CrossRef]
- Giubilini, A. Vaccination ethics. Br. Med. Bull. 2020, 137, 4–12. [Google Scholar] [CrossRef]
- Paterson, P.; Meurice, F.; Stanberry, L.R.; Glismann, S.; Rosenthal, S.L.; Larson, H.J. Vaccine hesitancy and healthcare providers. Vaccine 2016, 34, 6700–6706. [Google Scholar] [CrossRef]
- Schmid, P.; Rauber, D.; Betsch, C.; Lidolt, G.; Denker, M.-L. Barriers of Influenza Vaccination Intention and Behavior—A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS ONE 2017, 12, e0170550. [Google Scholar] [CrossRef]
- Hollmeyer, H.; Hayden, F.; Mounts, A.; Buchholz, U. Review: Interventions to increase influenza vaccination among healthcare workers in hospitals. Influenza Other Respir. Viruses 2013, 7, 604–621. [Google Scholar] [CrossRef]
- Da Costa, V.G.; Saivish, M.V.; Santos, D.E.R.; de Lima Silva, R.F.; Moreli, M.L. Comparative epidemiology between the 2009 H1N1 influenza and COVID-19 pandemics. J. Infect. Public Health 2020, 13, 1797–1804. [Google Scholar] [CrossRef]
- Fabry, P.; Gagneur, A.; Pasquier, J.-C. Determinants of A (H1N1) vaccination: Cross-sectional study in a population of pregnant women in Quebec. Vaccine 2011, 29, 1824–1829. [Google Scholar] [CrossRef] [PubMed]
- Al-Tawfiq, J.A. Willingness of health care workers of various nationalities to accept H1N1 (2009) pandemic influenza A vaccination. Ann. Saudi Med. 2012, 32, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Blasi, F.; Aliberti, S.; Mantero, M.; Centanni, S. Compliance with anti-H1N1 vaccine among healthcare workers and general population. Clin. Microbiol. Infect. 2012, 18, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Grohskopf, L.A.; Alyanak, E.; Broder, K.R.; Blanton, L.H.; Fry, A.M.; Jernigan, D.B.; Atmar, R.L. Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2020–2021 Influenza Season. MMWR Recomm. Rep. 2020, 69, 1–24. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention, National Center for Immunization and Respiratory Diseases (NCIRD). Influenza Vaccination Coverage Among Health Care Personnel—United States, 2020–2021 Influenza Season; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2021. [Google Scholar]
- Wilde, J.A.; McMillan, J.A.; Serwint, J.; Butta, J.; O’Riordan, M.A.; Steinhoff, M.C. Effectiveness of Influenza Vaccine in Health Care ProfessionalsA Randomized Trial. JAMA 1999, 281, 908–913. [Google Scholar] [CrossRef]
- Potter, J.; Stott, D.J.; Roberts, M.A.; Elder, A.G.; O’Donnell, B.; Knight, P.V.; Carman, W.F. Influenza Vaccination of Health Care Workers in Long-Term-Care Hospitals Reduces the Mortality of Elderly Patients. J. Infect. Dis. 1997, 175, 1–6. [Google Scholar] [CrossRef]
- Carman, W.F.; Elder, A.G.; Wallace, L.A.; McAulay, K.; Walker, A.; Murray, G.D.; Stott, D.J. Effects of influenza vaccination of health-care workers on mortality of elderly people in long-term care: A randomised controlled trial. Lancet 2000, 355, 93–97. [Google Scholar] [CrossRef]
- Ahmed, F.; Lindley, M.C.; Allred, N.; Weinbaum, C.M.; Grohskopf, L. Effect of Influenza Vaccination of Healthcare Personnel on Morbidity and Mortality Among Patients: Systematic Review and Grading of Evidence. Clin. Infect. Dis. 2013, 58, 50–57. [Google Scholar] [CrossRef]
- Hayward, A.C.; Harling, R.; Wetten, S.; Johnson, A.M.; Munro, S.; Smedley, J.; Murad, S.; Watson, J.M. Effectiveness of an influenza vaccine programme for care home staff to prevent death, morbidity, and health service use among residents: Cluster randomised controlled trial. BMJ 2006, 333, 1241. [Google Scholar] [CrossRef]
- Van den Dool, C.; Bonten, M.J.M.; Hak, E.; Heijne, J.C.M.; Wallinga, J. The Effects of Influenza Vaccination of Health Care Workers in Nursing Homes: Insights from a Mathematical Model. PLoS Med. 2008, 5, e200. [Google Scholar] [CrossRef] [PubMed]
- De Serres, G.; Skowronski, D.M.; Ward, B.J.; Gardam, M.; Lemieux, C.; Yassi, A.; Patrick, D.M.; Krajden, M.; Loeb, M.; Collignon, P.; et al. Influenza Vaccination of Healthcare Workers: Critical Analysis of the Evidence for Patient Benefit Underpinning Policies of Enforcement. PLoS ONE 2017, 12, e0163586. [Google Scholar] [CrossRef] [PubMed]
- Hayward, A.C. Influenza Vaccination of Healthcare Workers Is an Important Approach for Reducing Transmission of Influenza from Staff to Vulnerable Patients. PLoS ONE 2017, 12, e0169023. [Google Scholar] [CrossRef] [PubMed]
- Haviari, S.; Bénet, T.; Saadatian-Elahi, M.; André, P.; Loulergue, P.; Vanhems, P. Vaccination of healthcare workers: A review. Hum. Vaccines Immunother. 2015, 11, 2522–2537. [Google Scholar] [CrossRef]
- Committee On Infectious, D.; Byington, C.L.; Maldonado, Y.A.; Barnett, E.D.; Davies, H.D.; Edwards, K.M.; Lynfield, R.; Munoz, F.M.; Nolt, D.L.; Nyquist, A.-C.; et al. Influenza Immunization for All Health Care Personnel: Keep It Mandatory. Pediatrics 2015, 136, 809–818. [Google Scholar] [CrossRef]
- Desilver, D. States Have Mandated Vaccinations since Long before COVID-19. Available online: https://www.pewresearch.org/fact-tank/2021/10/08/states-have-mandated-vaccinations-since-long-before-covid-19/ (accessed on 4 March 2022).
- Poland, G.A.; Tosh, P.; Jacobson, R.M. Requiring influenza vaccination for health care workers: Seven truths we must accept. Vaccine 2005, 23, 2251–2255. [Google Scholar] [CrossRef]
- Gesser-Edelsburg, A.; Badarna Keywan, H. Physicians’ Perspective on Vaccine-Hesitancy at the Beginning of Israel’s COVID-19 Vaccination Campaign and Public’s Perceptions of Physicians’ Knowledge When Recommending the Vaccine to Their Patients: A Cross-Sectional Study. Front. Public Health 2022, 10, 855468. [Google Scholar] [CrossRef]
- Rodger, D.; Blackshaw, B.P. COVID-19 Vaccination Should not be Mandatory for Health and Social Care Workers. New Bioeth 2022, 28, 27–39. [Google Scholar] [CrossRef]
- Song, Y.; Zhang, T.; Chen, L.; Yi, B.; Hao, X.; Zhou, S.; Zhang, R.; Greene, C. Increasing seasonal influenza vaccination among high risk groups in China: Do community healthcare workers have a role to play? Vaccine 2017, 35, 4060–4063. [Google Scholar] [CrossRef]
- Lorenc, T.; Marshall, D.; Wright, K.; Sutcliffe, K.; Sowden, A. Seasonal influenza vaccination of healthcare workers: Systematic review of qualitative evidence. BMC Health Serv. Res. 2017, 17, 732. [Google Scholar] [CrossRef]
- Pereira, M.; Williams, S.; Restrick, L.; Cullinan, P.; Hopkinson, N.S. Barriers to influenza vaccination in healthcare workers. BMJ 2018, 360, k1141. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.M. Mandatory Vaccination of Health Care Workers. N. Engl. J. Med. 2009, 361, 2015–2017. [Google Scholar] [CrossRef] [PubMed]
- Bechini, A.; Lorini, C.; Zanobini, P.; Mandò Tacconi, F.; Boccalini, S.; Grazzini, M.; Bonanni, P.; Bonaccorsi, G. Utility of Healthcare System-Based Interventions in Improving the Uptake of Influenza Vaccination in Healthcare Workers at Long-Term Care Facilities: A Systematic Review. Vaccines 2020, 8, 165. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, C.G.; McArthur, M.A.; Naus, M.; Abraham, E.; McGeer, A.J. Prevention of influenza and pneumococcal pneumonia in Canadian long-term care facilities: How are we doing? Can. Med. Assoc. J. 2001, 164, 1413–1419. [Google Scholar]
- Thomas, R.E.; Jefferson, T.; Lasserson, T.J. Influenza vaccination for healthcare workers who care for people aged 60 or older living in long-term care institutions. Cochrane Database Syst. Rev. 2016, 2016, CD005187. [Google Scholar] [CrossRef]
- Talbot, T.R.; Schimmel, R.; Swift, M.D.; Rolando, L.A.; Johnson, R.T.; Muscato, J.; Sternberg, P.; Dubree, M.; McGown, P.W.; Yarbrough, M.I.; et al. Expanding mandatory healthcare personnel immunization beyond influenza: Impact of a broad immunization program with enhanced accountability. Infect. Control Hosp. Epidemiol. 2021, 42, 513–518. [Google Scholar] [CrossRef]
- Karlsson, L.C.; Lewandowsky, S.; Antfolk, J.; Salo, P.; Lindfelt, M.; Oksanen, T.; Kivimäki, M.; Soveri, A. The association between vaccination confidence, vaccination behavior, and willingness to recommend vaccines among Finnish healthcare workers. PLoS ONE 2019, 14, e0224330. [Google Scholar] [CrossRef]
- Petek, D.; Kamnik-Jug, K. Motivators and barriers to vaccination of health professionals against seasonal influenza in primary healthcare. BMC Health Serv. Res. 2018, 18, 853. [Google Scholar] [CrossRef]
- Hollmeyer, H.G.; Hayden, F.; Poland, G.; Buchholz, U. Influenza vaccination of health care workers in hospitals--a review of studies on attitudes and predictors. Vaccine 2009, 27, 3935–3944. [Google Scholar] [CrossRef]
- Rhudy, L.M.; Tucker, S.J.; Ofstead, C.L.; Poland, G.A. Personal Choice or Evidence-Based Nursing Intervention: Nurses’ Decision-Making about Influenza Vaccination. Worldviews Evid.-Based Nurs. 2010, 7, 111–120. [Google Scholar] [CrossRef]
- Carvalho, T.; Krammer, F.; Iwasaki, A. The first 12 months of COVID-19: A timeline of immunological insights. Nat. Rev. Immunol. 2021, 21, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Zhao, S.; Ou, J.; Zhang, J.; Lan, W.; Guan, W.; Wu, X.; Yan, Y.; Zhao, W.; Wu, J.; et al. COVID-19: Coronavirus Vaccine Development Updates. Front. Immunol. 2020, 11, 602256. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Vaccine R&D Investments. Available online: https://www.knowledgeportalia.org/covid19-r-d-funding (accessed on 28 March 2022).
- Ball, P. The lightning-fast quest for COVID vaccines—And what it means for other diseases. Nature 2021, 589, 16–18. [Google Scholar] [CrossRef] [PubMed]
- BBC News. COVID-19 Vaccine: First Person Receives Pfizer Jab in UK. Available online: https://www.bbc.com/news/uk-55227325 (accessed on 8 December 2020).
- Bok, K.; Sitar, S.; Graham, B.S.; Mascola, J.R. Accelerated COVID-19 vaccine development: Milestones, lessons, and prospects. Immunity 2021, 54, 1636–1651. [Google Scholar] [CrossRef]
- U.S. Food and Drug Administration. FDA Approves First COVID-19 Vaccine. Available online: https://www.fda.gov/news-events/press-announcements/fda-approves-first-covid-19-vaccine (accessed on 10 March 2022).
- FDA. Spikevax and Moderna COVID-19 Vaccine. Available online: https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/spikevax-and-moderna-covid-19-vaccine (accessed on 20 March 2022).
- Koontalay, A.; Suksatan, W.; Prabsangob, K.; Sadang, J.M. Healthcare Workers’ Burdens During the COVID-19 Pandemic: A Qualitative Systematic Review. J. Multidiscip. Healthc. 2021, 14, 3015–3025. [Google Scholar] [CrossRef] [PubMed]
- Kwok, K.O.; Li, K.-K.; Wei, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Verger, P.; Scronias, D.; Dauby, N.; Adedzi, K.A.; Gobert, C.; Bergeat, M.; Gagneur, A.; Dubé, E. Attitudes of healthcare workers towards COVID-19 vaccination: A survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance 2021, 26, 2002047. [Google Scholar] [CrossRef]
- Gagneux-Brunon, A.; Detoc, M.; Bruel, S.; Tardy, B.; Rozaire, O.; Frappe, P.; Botelho-Nevers, E. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: A cross-sectional survey. J. Hosp. Infect. 2021, 108, 168–173. [Google Scholar] [CrossRef]
- Ledda, C.; Costantino, C.; Cuccia, M.; Maltezou, H.C.; Rapisarda, V. Attitudes of Healthcare Personnel towards Vaccinations before and during the COVID-19 Pandemic. Int. J. Env. Res. Public Health 2021, 18, 168–173. [Google Scholar] [CrossRef]
- Fakonti, G.; Kyprianidou, M.; Toumbis, G.; Giannakou, K. Attitudes and Acceptance of COVID-19 Vaccination Among Nurses and Midwives in Cyprus: A Cross-Sectional Survey. Front. Public Health 2021, 9, 656138. [Google Scholar] [CrossRef]
- Gharpure, R.; Guo, A.; Bishnoi, C.K.; Patel, U.; Gifford, D.; Tippins, A.; Jaffe, A.; Shulman, E.; Stone, N.; Mungai, E.; et al. Early COVID-19 First-Dose Vaccination Coverage Among Residents and Staff Members of Skilled Nursing Facilities Participating in the Pharmacy Partnership for Long-Term Care Program—United States, December 2020-January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Reses, H.E.; Jones, E.S.; Richardson, D.B.; Cate, K.M.; Walker, D.W.; Shapiro, C.N. COVID-19 vaccination coverage among hospital-based healthcare personnel reported through the Department of Health and Human Services Unified Hospital Data Surveillance System, United States, January 20, 2021-September 15, 2021. Am. J. Infect. Control 2021, 49, 1554–1557. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.T.; Althomsons, S.P.; Wu, H.; Budnitz, D.S.; Kalayil, E.J.; Lindley, M.C.; Pingali, C.; Bridges, C.B.; Geller, A.I.; Fiebelkorn, A.P.; et al. Disparities in COVID-19 Vaccination Coverage Among Health Care Personnel Working in Long-Term Care Facilities, by Job Category, National Healthcare Safety Network—United States, March 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 1036–1039. [Google Scholar] [CrossRef] [PubMed]
- American Medical Association. AMA Survey Shows Over 96% of Doctors Fully Vaccinated against COVID-19. Available online: www.ama-assn.org/press-center/press-releases/ama-survey-shows-over-96-doctors-fully-vaccinated-against-covid-19 (accessed on 17 August 2021).
- Levy, R. How Many Health Care Workers Are Vaccinated? It’s Anyone’s Guess. Available online: https://www.politico.com/news/2022/01/19/health-care-workers-hospitals-vaccinated-527392 (accessed on 15 March 2022).
- Hagood, E.A.; Mintzer Herlihy, S. Addressing heterogeneous parental concerns about vaccination with a multiple-source model: A parent and educator perspective. Hum. Vaccines Immunother. 2013, 9, 1790–1794. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef]
- Sage Working Group. Report of the SAGE Working Group on Vaccine Hesitancy; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- Ritchie, H.; Mathieu, E.; Rodés-Guirao, L.; Appel, C.; Giattino, C.; Ortiz-Ospina, E.; Hasell, J.; Macdonald, B.; Beltekian, D.; Roser, M. Coronavirus Pandemic (COVID-19). Available online: https://ourworldindata.org/ (accessed on 27 April 2022).
- Gur-Arie, R.; Jamrozik, E.; Kingori, P. No Jab, No Job? Ethical Issues in Mandatory COVID-19 Vaccination of Healthcare Personnel. BMJ Glob. Health 2021, 6, e004877. [Google Scholar] [CrossRef]
- Federal Government of the United States. Medicare and Medicaid Programs; Omnibus COVID-19 Health Care Staff Vaccination. A Rule by the Centers for Medicare & Medicaid Services; 0938-AU75; Federal Government of the United States: Washington, DC, USA, 2021. [Google Scholar]
- Waldman, S.E.; Buehring, T.; Escobar, D.J.; Gohil, S.K.; Gonzales, R.; Huang, S.S.; Olenslager, K.; Prabaker, K.K.; Sandoval, T.; Yim, J.; et al. Secondary Cases of Delta-Variant COVID-19 Among Vaccinated Healthcare Workers with Breakthrough Infections is Rare. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, ciab916. [Google Scholar] [CrossRef]
- Cabezas, C.; Coma, E.; Mora-Fernandez, N.; Li, X.; Martinez-Marcos, M.; Fina, F.; Fabregas, M.; Hermosilla, E.; Jover, A.; Contel, J.C.; et al. Associations of BNT162b2 vaccination with SARS-CoV-2 infection and hospital admission and death with COVID-19 in nursing homes and healthcare workers in Catalonia: Prospective cohort study. BMJ 2021, 374, n1868. [Google Scholar] [CrossRef]
- Litigation Update for CMS Omnibus COVID-19 Health Care Staff Vaccination Interim Final Rule. Available online: https://www.cms.gov/About-CMS/Agency-Information/Emergency/EPRO/Current-Emergencies/Current-Emergencies-page (accessed on 15 March 2022).
- Gostin, L.O.; Parmet, W.E.; Rosenbaum, S. The US Supreme Court’s Rulings on Large Business and Health Care Worker Vaccine Mandates: Ramifications for the COVID-19 Response and the Future of Federal Public Health Protection. JAMA 2022, 327, 713–714. [Google Scholar] [CrossRef]
- Center for Clinical Standards and Quality/Quality, S.O.G. Guidance for the Interim Final Rule—Medicare and Medicaid Programs; Omnibus COVID-19 Health Care Staff Vaccination; QSO-22-11-ALL; Centers for Medicare & Medicaid Services: Baltimore, MD, USA, 20 January 2022. [Google Scholar]
- Dror, A.A.; Eisenbach, N.; Taiber, S.; Morozov, N.G.; Mizrachi, M.; Zigron, A.; Srouji, S.; Sela, E. Vaccine hesitancy: The next challenge in the fight against COVID-19. Eur. J. Epidemiol. 2020, 35, 775–779. [Google Scholar] [CrossRef] [PubMed]
- Pacella-LaBarbara, M.L.; Park, Y.L.; Patterson, P.D.; Doshi, A.; Guyette, M.K.; Wong, A.H.; Chang, B.P.; Suffoletto, B.P. COVID-19 Vaccine Uptake and Intent Among Emergency Healthcare Workers: A Cross-Sectional Survey. J. Occup. Environ. Med. 2021, 63, 852–856. [Google Scholar] [CrossRef] [PubMed]
- Qunaibi, E.; Basheti, I.; Soudy, M.; Sultan, I. Hesitancy of Arab Healthcare Workers towards COVID-19 Vaccination: A Large-Scale Multinational Study. Vaccines 2021, 9, 446. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.D.; Johnson, K.S.; Myles, L.; Herndon, L.; Montoya, A.; Fashaw, S.; Gifford, D. Lessons learned from frontline skilled nursing facility staff regarding COVID-19 vaccine hesitancy. J. Am. Geriatr. Soc. 2021, 69, 1140–1146. [Google Scholar] [CrossRef]
- Harrison, J.; Berry, S.; Mor, V.; Gifford, D. “Somebody Like Me”: Understanding COVID-19 Vaccine Hesitancy among Staff in Skilled Nursing Facilities. J. Am. Med. Dir. Assoc. 2021, 22, 1133–1137. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Toth-Manikowski, S.M.; Swirsky, E.S.; Gandhi, R.; Piscitello, G. COVID-19 vaccination hesitancy among health care workers, communication, and policy-making. Am. J. Infect. Control 2022, 50, 20–25. [Google Scholar] [CrossRef]
- Janssen, C.; Maillard, A.; Bodelet, C.; Claudel, A.-L.; Gaillat, J.; Delory, T.; on behalf of the ACV Alpin Study Group. Hesitancy towards COVID-19 Vaccination among Healthcare Workers: A Multi-Centric Survey in France. Vaccines 2021, 9, 547. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. COVID-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect. Control 2021, 49, 1152–1157. [Google Scholar] [CrossRef]
- Green-McKenzie, J.; Shofer, F.S.; Momplaisir, F.; Kuter, B.J.; Kruse, G.; Bilal, U.; Behta, M.; O’Donnell, J.; Al-Ramahi, N.; Kasbekar, N.; et al. Factors Associated With COVID-19 Vaccine Receipt by Health Care Personnel at a Major Academic Hospital During the First Months of Vaccine Availability. JAMA Netw. Open 2021, 4, e2136582. [Google Scholar] [CrossRef]
- Mohammed, R.; Nguse, T.M.; Habte, B.M.; Fentie, A.M.; Gebretekle, G.B. COVID-19 vaccine hesitancy among Ethiopian healthcare workers. PLoS ONE 2021, 16, e0261125. [Google Scholar] [CrossRef] [PubMed]
- Holzmann-Littig, C.; Braunisch, M.C.; Kranke, P.; Popp, M.; Seeber, C.; Fichtner, F.; Littig, B.; Carbajo-Lozoya, J.; Allwang, C.; Frank, T.; et al. COVID-19 Vaccination Acceptance and Hesitancy among Healthcare Workers in Germany. Vaccines 2021, 9, 777. [Google Scholar] [CrossRef] [PubMed]
- Yanez, N.D.; Weiss, N.S.; Romand, J.-A.; Treggiari, M.M. COVID-19 mortality risk for older men and women. BMC Public Health 2020, 20, 1742. [Google Scholar] [CrossRef] [PubMed]
- Gadoth, A.; Halbrook, M.; Martin-Blais, R.; Gray, A.; Tobin, N.H.; Ferbas, K.G.; Aldrovandi, G.M.; Rimoin, A.W. Cross-sectional Assessment of COVID-19 Vaccine Acceptance Among Health Care Workers in Los Angeles. Ann. Intern. Med. 2021, 174, 882–885. [Google Scholar] [CrossRef]
- Kara Esen, B.; Can, G.; Pirdal, B.Z.; Aydin, S.N.; Ozdil, A.; Balkan, I.I.; Budak, B.; Keskindemirci, Y.; Karaali, R.; Saltoglu, N. COVID-19 Vaccine Hesitancy in Healthcare Personnel: A University Hospital Experience. Vaccines 2021, 9, 1343. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Cheong, C.; Kong, G.; Phua, K.; Ngiam, J.N.; Tan, B.Y.Q.; Wang, B.; Hao, F.; Tan, W.; Han, X.; et al. An Asia-Pacific study on healthcare workers’ perceptions of, and willingness to receive, the COVID-19 vaccination. Int. J. Infect. Dis. 2021, 106, 52–60. [Google Scholar] [CrossRef]
- Ciardi, F.; Menon, V.; Jensen, J.L.; Shariff, M.A.; Pillai, A.; Venugopal, U.; Kasubhai, M.; Dimitrov, V.; Kanna, B.; Poole, B.D. Knowledge, Attitudes and Perceptions of COVID-19 Vaccination among Healthcare Workers of an Inner-City Hospital in New York. Vaccines 2021, 9, 516. [Google Scholar] [CrossRef]
- Khubchandani, J.; Macias, Y. COVID-19 vaccination hesitancy in Hispanics and African-Americans: A review and recommendations for practice. Brain Behav. Immun.-Health 2021, 15, 100277. [Google Scholar] [CrossRef]
- Momplaisir, F.M.; Kuter, B.J.; Ghadimi, F.; Browne, S.; Nkwihoreze, H.; Feemster, K.A.; Frank, I.; Faig, W.; Shen, A.K.; Offit, P.A.; et al. Racial/Ethnic Differences in COVID-19 Vaccine Hesitancy Among Health Care Workers in 2 Large Academic Hospitals. JAMA Netw. Open 2021, 4, e2121931. [Google Scholar] [CrossRef]
- Painter, E.M.; Ussery, E.N.; Patel, A.; Hughes, M.M.; Zell, E.R.; Moulia, D.L.; Scharf, L.G.; Lynch, M.; Ritchey, M.D.; Toblin, R.L.; et al. Demographic Characteristics of Persons Vaccinated During the First Month of the COVID-19 Vaccination Program—United States, December 14, 2020–January 14, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 174–177. [Google Scholar] [CrossRef]
- Schrading, W.A.; Trent, S.A.; Paxton, J.H.; Rodriguez, R.M.; Swanson, M.B.; Mohr, N.M.; Talan, D.A.; Project, C.E.D.N. Vaccination rates and acceptance of SARS-CoV-2 vaccination among U.S. emergency department health care personnel. Acad. Emerg. Med. Off. J. Soc. Acad. Emerg. Med. 2021, 28, 455–458. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.X.; Gilbert, K.L.; Lively, K.L.; Laurent, C.; Chawla, R.; Li, C.; Johnson, R.; Petcu, R.; Mehra, M.; Spooner, A.; et al. Correlates of COVID-19 Vaccine Hesitancy among a Community Sample of African Americans Living in the Southern United States. Vaccines 2021, 9, 879. [Google Scholar] [CrossRef] [PubMed]
- Fares, S.; Elmnyer, M.M.; Mohamed, S.S.; Elsayed, R. COVID-19 Vaccination Perception and Attitude among Healthcare Workers in Egypt. J. Prim. Care Community Health 2021, 12, 21501327211013303. [Google Scholar] [CrossRef] [PubMed]
- Manning, M.L.; Gerolamo, A.M.; Marino, M.A.; Hanson-Zalot, M.E.; Pogorzelska-Maziarz, M. COVID-19 vaccination readiness among nurse faculty and student nurses. Nurs. Outlook 2021, 69, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Parente, D.J.; Ojo, A.; Gurley, T.; LeMaster, J.W.; Meyer, M.; Wild, D.M.; Mustafa, R.A. Acceptance of COVID-19 Vaccination Among Health System Personnel. J. Am. Board Fam. Med. 2021, 34, 498–508. [Google Scholar] [CrossRef] [PubMed]
- Biswas, N.; Mustapha, T.; Khubchandani, J.; Price, J.H. The Nature and Extent of COVID-19 Vaccination Hesitancy in Healthcare Workers. J. Community Health 2021, 46, 1244–1251. [Google Scholar] [CrossRef]
- Browne, S.K.; Feemster, K.A.; Shen, A.K.; Green-McKenzie, J.; Momplaisir, F.M.; Faig, W.; Offit, P.A.; Kuter, B.J. Coronavirus disease 2019 (COVID-19) vaccine hesitancy among physicians, physician assistants, nurse practitioners, and nurses in two academic hospitals in Philadelphia. Infect. Control Hosp. Epidemiol. 2021, 1–9. [Google Scholar] [CrossRef]
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Intention of healthcare workers to accept COVID-19 vaccination and related factors: A systematic review and meta-analysis. Asian Pac. J. Trop. Med. 2021, 14, 543–554. [Google Scholar] [CrossRef]
- Qattan, A.M.N.; Alshareef, N.; Alsharqi, O.; Al Rahahleh, N.; Chirwa, G.C.; Al-Hanawi, M.K. Acceptability of a COVID-19 Vaccine Among Healthcare Workers in the Kingdom of Saudi Arabia. Front. Med. 2021, 8, 644300. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.M.; Ismail, S.A.; Ojo-Aromokudu, O.; Naqvi, H.; Coghill, Y.; Donovan, H.; Letley, L.; Paterson, P.; Mounier-Jack, S. COVID-19 vaccination beliefs, attitudes, and behaviours among health and social care workers in the UK: A mixed-methods study. PLoS ONE 2022, 17, e0260949. [Google Scholar] [CrossRef]
- Navin, M.C.; Oberleitner, L.M.-S.; Lucia, V.C.; Ozdych, M.; Afonso, N.; Kennedy, R.H.; Keil, H.; Wu, L.; Mathew, T.A. COVID-19 Vaccine Hesitancy Among Healthcare Personnel Who Generally Accept Vaccines. J. Community Health 2022, 47, 519–529. [Google Scholar] [CrossRef] [PubMed]
- Kirzinger, A.; Kearney, A.; Hamel, L.; Brodie, M. KFF/The Washington Post Frontline Health Care Workers Survey; Kaiser Family Foundation: Oakland, CA, USA, 2021; pp. 1–26. [Google Scholar]
- Geller, A.I.; Budnitz, D.S.; Dubendris, H.; Gharpure, R.; Soe, M.; Wu, H.; Kalayil, E.J.; Benin, A.L.; Patel, S.A.; Lindley, M.C.; et al. Surveillance of COVID-19 Vaccination in Nursing Homes, United States, December 2020–July 2021. Public Health Rep. 2022, 137, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Unroe, K.T.; Evans, R.; Weaver, L.; Rusyniak, D.; Blackburn, J. Willingness of Long-Term Care Staff to Receive a COVID-19 Vaccine: A Single State Survey. J. Am. Geriatr. Soc. 2021, 69, 593–599. [Google Scholar] [CrossRef] [PubMed]
- Lang, M.A.; Stahlman, S.; Wells, N.Y.; Fedgo, A.A.; Patel, D.M.; Chauhan, A.; Mancuso, J.D. Disparities in COVID-19 vaccine initiation and completion among active component service members and health care personnel, 11 December 2020–12 March 2021. MSMR 2021, 28, 2–9. [Google Scholar] [PubMed]
- The Chairtis Group. Vaccine Hesitancy Among Rural Hospitals: The Arrival of a Challenging “New Normal”. 2021. Available online: https://www.chartis.com/insights/vaccine-hesitancy-among-rural-hospitals-arrival-challenging-new-normal (accessed on 26 April 2022).
- Dubov, A.; Distelberg, B.J.; Abdul-Mutakabbir, J.C.; Beeson, W.L.; Loo, L.K.; Montgomery, S.B.; Oyoyo, U.E.; Patel, P.; Peteet, B.; Shoptaw, S.; et al. Predictors of COVID-19 Vaccine Acceptance and Hesitancy among Healthcare Workers in Southern California: Not Just “Anti” vs. “Pro” Vaccine. Vaccines 2021, 9, 1428. [Google Scholar] [CrossRef]
- El-Sokkary, R.H.; El Seifi, O.S.; Hassan, H.M.; Mortada, E.M.; Hashem, M.K.; Gadelrab, M.R.M.A.; Tash, R.M.E. Predictors of COVID-19 vaccine hesitancy among Egyptian healthcare workers: A cross-sectional study. BMC Infect. Dis. 2021, 21, 762. [Google Scholar] [CrossRef]
- Lazer, D.; Qu, H.; Ognyanova, K.; Baum, M.; Perlis, R.H.; Druckman, J.; Uslu, A.; Lin, J.; Santillana, M.; Green, J.; et al. The COVID States Project #40: COVID-19 Vaccine Attitudes among Healthcare Workers. 18 February 2021. Available online: https://osf.io/yhk5j (accessed on 26 April 2022).
- Shallal, A.; Abada, E.; Musallam, R.; Fehmi, O.; Kaljee, L.; Fehmi, Z.; Alzouhayli, S.; Ujayli, D.; Dankerlui, D.; Kim, S.; et al. Evaluation of COVID-19 Vaccine Attitudes among Arab American Healthcare Professionals Living in the United States. Vaccines 2021, 9, 942. [Google Scholar] [CrossRef]
- Paris, C.; Bénézit, F.; Geslin, M.; Polard, E.; Baldeyrou, M.; Turmel, V.; Tadié, É.; Garlantezec, R.; Tattevin, P. COVID-19 vaccine hesitancy among healthcare workers. Infect. Dis. Now 2021, 51, 484–487. [Google Scholar] [CrossRef]
- Kim, M.H.; Son, N.-H.; Park, Y.S.; Lee, J.H.; Kim, D.A.; Kim, Y.C. Effect of a hospital-wide campaign on COVID-19 vaccination uptake among healthcare workers in the context of raised concerns for life-threatening side effects. PLoS ONE 2021, 16, e0258236. [Google Scholar] [CrossRef]
- Cowan, S.K.; Mark, N.; Reich, J.A. COVID-19 Vaccine Hesitancy Is the New Terrain for Political Division among Americans. Socius 2021, 7, 23780231211023657. [Google Scholar] [CrossRef]
- Kerr, J.; Panagopoulos, C.; van der Linden, S. Political polarization on COVID-19 pandemic response in the United States. Personal. Individ. Differ. 2021, 179, 110892. [Google Scholar] [CrossRef]
- SOBO, E.J. THEORIZING (VACCINE) REFUSAL: Through the Looking Glass. Cult. Anthropol. 2016, 31, 342–350. [Google Scholar] [CrossRef]
- Gabarron, E.; Oyeyemi, S.O.; Wynn, R. COVID-19-related misinformation on social media: A systematic review. Bull. World Health Organ. 2021, 99, 455–463A. [Google Scholar] [CrossRef] [PubMed]
- Jennings, W.; Stoker, G.; Bunting, H.; Valgarðsson, V.O.; Gaskell, J.; Devine, D.; McKay, L.; Mills, M.C. Lack of Trust, Conspiracy Beliefs, and Social Media Use Predict COVID-19 Vaccine Hesitancy. Vaccines 2021, 9, 593. [Google Scholar] [CrossRef]
- Piltch-Loeb, R.; Savoia, E.; Goldberg, B.; Hughes, B.; Verhey, T.; Kayyem, J.; Miller-Idriss, C.; Testa, M. Examining the effect of information channel on COVID-19 vaccine acceptance. PLoS ONE 2021, 16, e0251095. [Google Scholar] [CrossRef]
- Wilson, S.L.; Wiysonge, C. Social media and vaccine hesitancy. BMJ Glob. Health 2020, 5, e004206. [Google Scholar] [CrossRef]
- González Cano-Caballero, M.; Gil García, E.; Garrido Peña, F.; Cano-Caballero Galvez, M.D. Opinions of Andalusian primary health care professionals. Sist. Sanit. Navar. 2018, 41, 27–34. [Google Scholar] [CrossRef]
- Pataka, A.; Kotoulas, S.; Stefanidou, E.; Grigoriou, I.; Tzinas, A.; Tsiouprou, I.; Zarogoulidis, P.; Courcoutsakis, N.; Argyropoulou, P. Acceptability of Healthcare Professionals to Get Vaccinated against COVID-19 Two Weeks before Initiation of National Vaccination. Medicina 2021, 57, 611. [Google Scholar] [CrossRef]
- Öncel, S.; Alvur, M.; Çakıcı, Ö. Turkish Healthcare Workers’ Personal and Parental Attitudes to COVID-19 Vaccination From a Role Modeling Perspective. Cureus 2022, 14, e22555. [Google Scholar] [CrossRef]
- Simonson, M.D.; Baum, M.; Lazer, D.; Ognyanova, K.; Gitomer, A.; Perlis, R.H.; Uslu, A.; Druckman, J.; Green, J.; Santillana, M. The COVID States Project# 45: Vaccine Hesitancy And Resistance Among Parents. 2021. Available online: https://osf.io/e95bc/ (accessed on 26 April 2022).
- Wileden, L. The Link Betwee Parents’ and Children’s Vaccination in Detroit; The University of Michigan: Ann Arbor, MI, USA, 2022. [Google Scholar]
- Ma, L.; Yang, J.; Zhang, T.; Han, X.; Huang, Q.; Yang, Y.; Feng, L.; Yang, W.; Wang, C. Willingness toward COVID-19 vaccination, coadministration with other vaccines and receive a COVID-19 vaccine booster: A cross-sectional study on the guardians of children in China. Hum. Vaccines Immunother. 2022, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Pan, F.; Zhao, H.; Nicholas, S.; Maitland, E.; Liu, R.; Hou, Q. Parents’ Decisions to Vaccinate Children against COVID-19: A Scoping Review. Vaccines 2021, 9, 1476. [Google Scholar] [CrossRef] [PubMed]
- Hudson, A.; Montelpare, W.J. Predictors of Vaccine Hesitancy: Implications for COVID-19 Public Health Messaging. Int. J. Environ. Res. Public Health 2021, 18, 8054. [Google Scholar] [CrossRef] [PubMed]
- Raude, J. L’hésitation vaccinale: Une perspective psychosociologique. Bull. L’académie Natl. Médecine 2016, 200, 199–209. [Google Scholar] [CrossRef]
- Khuller, D. Why Are So Many Health-Care Workers Resisting the COVID Vaccine? The New Yorker. Available online: https://www.newyorker.com/science/medical-dispatch/why-are-so-many-health-care-workers-resisting-the-covid-vaccine (accessed on 2 February 2021).
- Grochowska, M.; Ratajczak, A.; Zdunek, G.; Adamiec, A.; Waszkiewicz, P.; Feleszko, W. A Comparison of the Level of Acceptance and Hesitancy towards the Influenza Vaccine and the Forthcoming COVID-19 Vaccine in the Medical Community. Vaccines 2021, 9, 475. [Google Scholar] [CrossRef]
- Kashif, M.; Fatima, I.; Ahmed, A.M.; Arshad Ali, S.; Memon, R.S.; Afzal, M.; Saeed, U.; Gul, S.; Ahmad, J.; Malik, F.; et al. Perception, Willingness, Barriers, and Hesitancy Towards COVID-19 Vaccine in Pakistan: Comparison Between Healthcare Workers and General Population. Cureus 2021, 13, e19106. [Google Scholar] [CrossRef]
- Wang, M.-W.; Wen, W.; Wang, N.; Zhou, M.-Y.; Wang, C.-Y.; Ni, J.; Jiang, J.-J.; Zhang, X.-W.; Feng, Z.-H.; Cheng, Y.-R. COVID-19 Vaccination Acceptance Among Healthcare Workers and Non-healthcare Workers in China: A Survey. Front. Public Health 2021, 9, 709056. [Google Scholar] [CrossRef]
- Al-Metwali, B.Z.; Al-Jumaili, A.A.; Al-Alag, Z.A.; Sorofman, B. Exploring the acceptance of COVID-19 vaccine among healthcare workers and general population using health belief model. J. Eval. Clin. Pract. 2021, 27, 1112–1122. [Google Scholar] [CrossRef]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef]
- Pan American Health Organization. Policy Brief—Addressing COVID-19 Vaccine Hesitancy among Healthcare Workers in the Caribean; Pan American Health Organization: Washington, DC, USA, 2021. [Google Scholar]
- Meyer, M.N.; Gjorgjieva, T.; Rosica, D. Trends in Health Care Worker Intentions to Receive a COVID-19 Vaccine and Reasons for Hesitancy. JAMA Netw. Open 2021, 4, e215344. [Google Scholar] [CrossRef]
- Pal, S.; Shekhar, R.; Kottewar, S.; Upadhyay, S.; Singh, M.; Pathak, D.; Kapuria, D.; Barrett, E.; Sheikh, A.B. COVID-19 Vaccine Hesitancy and Attitude toward Booster Doses among US Healthcare Workers. Vaccines 2021, 9, 1358. [Google Scholar] [CrossRef] [PubMed]
- Woolf, K.; Gogoi, M.; Martin, C.A.; Papineni, P.; Lagrata, S.; Nellums, L.B.; McManus, I.C.; Guyatt, A.L.; Melbourne, C.; Bryant, L.; et al. Healthcare workers’ views on mandatory SARS-CoV-2 vaccination in the UK: A cross-sectional, mixed-methods analysis from the UK-REACH study. eClinicalMedicine. 2022, 46, 101346. [Google Scholar] [CrossRef] [PubMed]
- Choi, K.; Chang, J.; Luo, Y.X.; Lewin, B.; Munoz-Plaza, C.; Bronstein, D.; Rondinelli, J.; Bruxvoort, K. “Still on the Fence:” A Mixed Methods Investigation of COVID-19 Vaccine Confidence Among Health Care Providers. Workplace Health Saf. 2022, 70, 21650799211049811. [Google Scholar] [CrossRef] [PubMed]
- Tran, A.; Witek, T.J., Jr. The Emergency Use Authorization of Pharmaceuticals: History and Utility During the COVID-19 Pandemic. Pharm. Med. 2021, 35, 203–213. [Google Scholar] [CrossRef]
- FDA. Coronavirus (COVID-19) Update: FDA Takes Key Action by Approving Second COVID-19 Vaccine. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-takes-key-action-approving-second-covid-19-vaccine (accessed on 10 March 2022).
- CDC COVID-19 Response Team; FDA. Allergic Reactions Including Anaphylaxis After Receipt of the First Dose of Moderna COVID-19 Vaccine—United States, 21 December 2020–10 January 2021. MMWR. Morb. Mortal. Wkly. Rep. 2021, 70, 125–129. [Google Scholar] [CrossRef]
- Sharifian-Dorche, M.; Bahmanyar, M.; Sharifian-Dorche, A.; Mohammadi, P.; Nomovi, M.; Mowla, A. Vaccine-induced immune thrombotic thrombocytopenia and cerebral venous sinus thrombosis post COVID-19 vaccination; a systematic review. J. Neurol. Sci. 2021, 428, 117607. [Google Scholar] [CrossRef]
- Bozkurt, B.; Kamat, I.; Hotez, P.J. Myocarditis with COVID-19 mRNA Vaccines. Circulation 2021, 144, 471–484. [Google Scholar] [CrossRef]
- Islam, M.S.; Kamal, A.-H.M.; Kabir, A.; Southern, D.L.; Khan, S.H.; Hasan, S.M.M.; Sarkar, T.; Sharmin, S.; Das, S.; Roy, T.; et al. COVID-19 vaccine rumors and conspiracy theories: The need for cognitive inoculation against misinformation to improve vaccine adherence. PLoS ONE 2021, 16, e0251605. [Google Scholar] [CrossRef]
- Schuchat, A.; Marks, P. Joint CDC and FDA Statement on Johnson & Johnson COVID-19 Vaccine; FDA: Silver Spring, MD, USA, 2021. [Google Scholar]
- FDA. FDA and CDC Lift Recommended Pause on Johnson & Johnson (Janssen) COVID-19 Vaccine Use following thorough Safety Review; FDA: Silver Spring, MD, USA, 2021. [Google Scholar]
- Wise, J. COVID-19: European countries suspend use of Oxford-AstraZeneca vaccine after reports of blood clots. BMJ 2021, 372, n699. [Google Scholar] [CrossRef]
- European Medicines Agency. COVID-19 Vaccine AstraZeneca: Benefits Still Outweigh the Risks Despite Possible Link to Rare Blood Clot with Low Platelets. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazeneca-benefits-still-outweigh-risks-despite-possible-link-rare-blood-clots (accessed on 10 March 2022).
- Kupferschmidt, K.; Vogel, G. European Countries Resume Use of Astrazeneca’s COVID-19 Vaccine, Hoping Pause Has Not Dented Confidence. Available online: https://www.science.org/content/article/european-countries-resume-use-astrazenecas-covid-19-vaccine-hoping-pause-has-not-dented (accessed on 10 March 2022).
- Forman, R.; Jit, M.; Mossialos, E. Divergent vaccination policies could fuel mistrust and hesitancy. Lancet 2021, 397, 2333. [Google Scholar] [CrossRef]
- Hsieh, Y.L.; Rak, S.; SteelFisher, G.K.; Bauhoff, S. Effect of the suspension of the J&J COVID-19 vaccine on vaccine hesitancy in the United States. Vaccine 2022, 40, 424–427. [Google Scholar] [CrossRef] [PubMed]
- Townsel, C.; Moniz, M.H.; Wagner, A.L.; Zikmund-Fisher, B.J.; Hawley, S.; Jiang, L.; Stout, M.J. COVID-19 vaccine hesitancy among reproductive-aged female tier 1A healthcare workers in a United States Medical Center. J. Perinatol. 2021, 41, 2549–2551. [Google Scholar] [CrossRef] [PubMed]
- Swann, M.C.; Bendetson, J.; Johnson, A.; Jatta, M.; Schleupner, C.J.; Baffoe-Bonnie, A. Examining Drivers of COVID-19 Vaccine Hesitancy Among Healthcare Workers. Infect. Control Hosp. Epidemiol. 2022, 1–40. [Google Scholar] [CrossRef] [PubMed]
- Dolu, İ.; Turhan, Z.; Yalnız Dilcen, H. COVID-19 Vaccine Acceptance is associated with Vaccine Hesitancy, Perceived Risk and Previous Vaccination Experiences. Disaster Med. Public Health Prep. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Advisory Committee on Immunization Practices; Centers for Disease Control and Prevention. Immunization of health-care personnel: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. Recomm. Rep. Morb. Mortal. Wkly. Rep. Recomm. Rep. 2011, 60, 1–45. [Google Scholar]
- Rubin, R. Pregnant People’s Paradox—Excluded From Vaccine Trials Despite Having a Higher Risk of COVID-19 Complications. JAMA 2021, 325, 1027–1028. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States; CDC: Atlanta, GA, USA, 2021. [Google Scholar]
- Centers for Disease Control and Prevention. COVID-19 (Coronavirus Disease): People with Certain Medical Conditions; CDC: Atlanta, GA, USA, 2021. [Google Scholar]
- Holley, P. She’s Leading the Fight Against Mandatory Vaccines in Texas. She Also Happens to Be a Nurse. Available online: https://www.texasmonthly.com/news-politics/houston-methodist-nurse-vaccine-refusal/ (accessed on 10 March 2022).
- Rick Green-Granite State News Collaborative. Adverse Reaction: Why do some NH healthcare workers oppose the COVID-19 vaccine? NH Business Review, 21 October 2021. [Google Scholar]
- Del Rio, C.; Malani, P. COVID-19 in 2021—Continuing Uncertainty. JAMA 2021, 325, 1389–1390. [Google Scholar] [CrossRef]
- Montastruc, J.-L.; Biron, P.; Sommet, A. Efficacy of COVID-19 vaccines: Several modes of expression should be presented in scientific publications. Fundam. Clin. Pharmacol. 2022, 36, 218–220. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.-M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Lopez Bernal, J.; Andrews, N.; Gower, C.; Gallagher, E.; Simmons, R.; Thelwall, S.; Stowe, J.; Tessier, E.; Groves, N.; Dabrera, G.; et al. Effectiveness of COVID-19 Vaccines against the B.1.617.2 (Delta) Variant. N. Engl. J. Med. 2021, 385, 585–594. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Child & Adolescent Immunization Schedule. Available online: https://www.cdc.gov/vaccines/schedules/hcp/imz/child-adolescent.html (accessed on 29 March 2022).
- Centers for Disease Control and Prevention. Adult Immunization Schedule—Recommendations for Ages 19 or Older, United States, 2022; CDC: Atlanta, GA, USA, 2022. [Google Scholar]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. COVID-19 Breakthrough Infections in Vaccinated Health Care Workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Eyre, D.W.; Taylor, D.; Purver, M.; Chapman, D.; Fowler, T.; Pouwels, K.B.; Walker, A.S.; Peto, T.E.A. Effect of COVID-19 Vaccination on Transmission of Alpha and Delta Variants. N. Engl. J. Med. 2022, 386, 744–756. [Google Scholar] [CrossRef] [PubMed]
- Wilder-Smith, A. What is the vaccine effect on reducing transmission in the context of the SARS-CoV-2 delta variant? Lancet Infect. Dis. 2022, 22, 152–153. [Google Scholar] [CrossRef]
- Passaretti, C.L.; Priem, J.S.; Agner, T.G.; McCurdy, L. Reducing the rates of household transmission: The impact of COVID-19 vaccination in healthcare workers with a known household exposure. Vaccine 2022, 40, 1213–1214. [Google Scholar] [CrossRef]
- Hak, E.; Schönbeck, Y.; De Melker, H.; Van Essen, G.A.; Sanders, E.A. Negative attitude of highly educated parents and health care workers towards future vaccinations in the Dutch childhood vaccination program. Vaccine 2005, 23, 3103–3107. [Google Scholar] [CrossRef]
- Ten Kate, J.; Koster, W.D.; Van der Waal, J. “Following Your Gut” or “Questioning the Scientific Evidence”: Understanding Vaccine Skepticism among More-Educated Dutch Parents. J. Health Soc. Behav. 2021, 62, 85–99. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2020, 384, 403–416. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Weinberg, S.H.; Butchart, A.T.; Davis, M.M. Size of clinical trials and Introductory prices of prophylactic vaccine series. Hum. Vaccines Immunother. 2012, 8, 1066–1070. [Google Scholar] [CrossRef]
- Roy, B.; Kumar, V.; Venkatesh, A. Health care workers’ reluctance to take the COVID-19 vaccine: A consumer-marketing approach to identifying and overcoming hesitancy. NEJM Catal. Innov. Care Deliv. 2020, 1, 1–10. [Google Scholar]
- Ali, K.; Berman, G.; Zhou, H.; Deng, W.; Faughnan, V.; Coronado-Voges, M.; Ding, B.; Dooley, J.; Girard, B.; Hillebrand, W.; et al. Evaluation of mRNA-1273 SARS-CoV-2 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 2241–2251. [Google Scholar] [CrossRef] [PubMed]
- El Sahly, H.M.; Baden, L.R.; Essink, B.; Doblecki-Lewis, S.; Martin, J.M.; Anderson, E.J.; Campbell, T.B.; Clark, J.; Jackson, L.A.; Fichtenbaum, C.J.; et al. Efficacy of the mRNA-1273 SARS-CoV-2 Vaccine at Completion of Blinded Phase. N. Engl. J. Med. 2021, 385, 1774–1785. [Google Scholar] [CrossRef] [PubMed]
- Frenck, R.W., Jr.; Klein, N.P.; Kitchin, N.; Gurtman, A.; Absalon, J.; Lockhart, S.; Perez, J.L.; Walter, E.B.; Senders, S.; Bailey, R.; et al. Safety, Immunogenicity, and Efficacy of the BNT162b2 COVID-19 Vaccine in Adolescents. N. Engl. J. Med. 2021, 385, 239–250. [Google Scholar] [CrossRef]
- Thomas, S.J.; Moreira, E.D., Jr.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Polack, F.P.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA COVID-19 Vaccine through 6 Months. N. Engl. J. Med. 2021, 385, 1761–1773. [Google Scholar] [CrossRef]
- Emary, K.R.W.; Golubchik, T.; Aley, P.K.; Ariani, C.V.; Angus, B.; Bibi, S.; Blane, B.; Bonsall, D.; Cicconi, P.; Charlton, S.; et al. Efficacy of ChAdOx1 nCoV-19 (AZD1222) vaccine against SARS-CoV-2 variant of concern 202012/01 (B.1.1.7): An exploratory analysis of a randomised controlled trial. Lancet 2021, 397, 1351–1362. [Google Scholar] [CrossRef]
- Han, S. Clinical vaccine development. Clin. Exp. Vaccine Res. 2015, 4, 46–53. [Google Scholar] [CrossRef]
- Onakpoya, I.J.; Heneghan, C.J.; Aronson, J.K. Post-marketing withdrawal of 462 medicinal products because of adverse drug reactions: A systematic review of the world literature. BMC Med. 2016, 14, 10. [Google Scholar] [CrossRef]
- Frank, C.; Himmelstein, D.U.; Woolhandler, S.; Bor, D.H.; Wolfe, S.M.; Heymann, O.; Zallman, L.; Lasser, K.E. Era Of Faster FDA Drug Approval Has Also Seen Increased Black-Box Warnings And Market Withdrawals. Health Aff. 2014, 33, 1453–1459. [Google Scholar] [CrossRef]
- Dolgin, E. The tangled history of mRNA vaccines. Nature 2021, 597, 318–324. [Google Scholar] [CrossRef] [PubMed]
- Gladwell, M. The Tipping Point: How Little Things can Make a Big Difference; First Back Bay Paperback Edition; Back Bay Books: Boston, MA, USA, 2002. [Google Scholar]
- Ahmad, M.; Akande, A.; Majid, U. Health care provider trust in vaccination: A systematic review and qualitative meta-synthesis. Eur. J. Public Health 2022, 32, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Konrad, T.R.; Pathman, D.E. Pediatrician and family physician agreement with and adoption of universal hepatitis B immunization. J. Fam. Pract. 1996, 42, 587–592. [Google Scholar]
- American Nurses Foundation. December Pulse on the Nation’s Nurses COVID-19 Survey Series: COVID-19 Vaccine. Available online: https://www.nursingworld.org/practice-policy/work-environment/health-safety/disaster-preparedness/coronavirus/what-you-need-to-know/covid-19-vaccine-survey/ (accessed on 29 March 2022).
- Urback, R. We should try to understand the paradox of the vaccine-hesitant health care worker. The Globe and Mail, 11 November 2021. [Google Scholar]
- McCallum, J.M.; Arekere, D.M.; Green, B.L.; Katz, R.V.; Rivers, B.M. Awareness and knowledge of the U.S. Public Health Service syphilis study at Tuskegee: Implications for biomedical research. J. Health Care Poor Underserved 2006, 17, 716–733. [Google Scholar] [CrossRef] [PubMed]
- Dara, S.; Sharma, S.K.; Kumar, A.; Goel, A.D.; Jain, V.; Sharma, M.C.; Gupta, M.K.; Saurabh, S.; Bhardwaj, P.; Misra, S. Awareness, Attitude, and Acceptability of Healthcare Workers About COVID-19 Vaccination in Western India. Cureus 2021, 13, e18400. [Google Scholar] [CrossRef]
- Kumar, R.; Alabdulla, M.; Elhassan, N.M.; Reagu, S.M. Qatar Healthcare Workers’ COVID-19 Vaccine Hesitancy and Attitudes: A National Cross-Sectional Survey. Front. Public Health 2021, 9, 727748. [Google Scholar] [CrossRef]
- Karafillakis, E.; Dinca, I.; Apfel, F.; Cecconi, S.; Wűrz, A.; Takacs, J.; Suk, J.; Celentano, L.P.; Kramarz, P.; Larson, H.J. Vaccine hesitancy among healthcare workers in Europe: A qualitative study. Vaccine 2016, 34, 5013–5020. [Google Scholar] [CrossRef]
- Kimball, S. What’s Next for Pfizer, Moderna beyond Their Projected $51 Billion in Combined Covid Vaccine Sales This Year. Available online: https://www.cnbc.com/2022/03/03/covid-pfizer-moderna-project-51-billion-in-combined-vaccine-sales-this-year.html (accessed on 27 March 2022).
- Collange, F.; Fressard, L.; Verger, P.; Josancy, F.; Sebbah, R.; Gautier, A. Vaccinations: Attitudes et pratiques des médecins généralistes. Études Résultats 2015, 910, 1–8. [Google Scholar]
- Oliver, D. Trust in CDC, FDA Took a Beating During Pandemic. Available online: https://www.webmd.com/lung/news/20210609/trust-in-cdc-fda-took-a-beating-during-pandemic (accessed on 21 March 2022).
- NORC. Surveys of Trust in the U.S. Health Care System; NORC: Washington, DC, USA, 5 May 2021. [Google Scholar]
- Specialty Physicians Weigh in with Opinions about the US Food and Drug Administration. Available online: https://www.spherixglobalinsights.com/specialty-physicians-weigh-in-with-opinions-about-the-us-food-and-drug-administration/ (accessed on 15 March 2022).
- Walsh, S.; Merrick, R.; Milne, R.; Brayne, C. Aducanumab for Alzheimer’s disease? BMJ (Clin. Res. Ed.) 2021, 374, n1682. [Google Scholar] [CrossRef]
- Offit, P.A. The Cutter incident, 50 years later. N. Engl. J. Med. 2005, 352, 1411–1412. [Google Scholar] [CrossRef]
- Matson, D.O. RotaShield: The ill-fated rhesus-human reassortant rotavirus vaccine. Pediatr. Ann. 2006, 35, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Dorribo, V.; Lazor-Blanchet, C.; Hugli, O.; Zanetti, G. Health care workers’ influenza vaccination: Motivations and mandatory mask policy. Occup. Med. 2015, 65, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Billings, J.; Ching, B.C.F.; Gkofa, V.; Greene, T.; Bloomfield, M. Experiences of frontline healthcare workers and their views about support during COVID-19 and previous pandemics: A systematic review and qualitative meta-synthesis. BMC Health Serv. Res. 2021, 21, 923. [Google Scholar] [CrossRef] [PubMed]
- Iguacel, I.; Luna Maldonado, A.; Luna Ruiz-Cabello, A.; Samatán, E.; Alarcón, J.; Ángeles Orte, M.; Santodomingo Mateos, S.; Martínez-Jarreta, B. Attitudes of Healthcare Professionals and General Population Toward Vaccines and the Intention to Be Vaccinated Against COVID-19 in Spain. Front. Public Health 2021, 9, 739003. [Google Scholar] [CrossRef]
- Vignier, N.; Brureau, K.; Granier, S.; Breton, J.; Michaud, C.; Gaillet, M.; Agostini, C.; Ballet, M.; Nacher, M.; Valdes, A.; et al. Attitudes towards the COVID-19 Vaccine and Willingness to Get Vaccinated among Healthcare Workers in French Guiana: The Influence of Geographical Origin. Vaccines 2021, 9, 682. [Google Scholar] [CrossRef]
- Oliver, K.; Raut, A.; Pierre, S.; Silvera, L.; Boulos, A.; Gale, A.; Baum, A.; Chory, A.; Davis, N.J.; D’Souza, D.; et al. Factors associated with COVID-19 vaccine receipt at two integrated healthcare systems in New York City: A cross-sectional study of healthcare workers. BMJ Open 2022, 12, e053641. [Google Scholar] [CrossRef]
- Gaspar da Rocha, A.; Santa-Rosa, B.; Vieira, D.N.; Silvestre, M. Vaccination Hesitancy in Health Care Providers: The Example for the General Population in the Time of a Pandemic. Port. J. Public Health 2021, 39, 74–77. [Google Scholar] [CrossRef]
- Vahidy, F.; Boom, M.L.; Drews, A.L.; Hackett, C.; Miller, S.M.; Phillips, R.A.; Schwartz, R.L.; Sostman, H.D. Houston Methodist’s Mandate of COVID-19 Vaccine Boosters Among Health Care Workers: Setting Precedents During Unprecedented Times. NEJM Catal. Innov. Care Deliv. 2022, 3, 1–12. [Google Scholar]
- Kirzinger, A.; Muñana, C.; Brodie, M. Vaccine Hesitancy in Rural America. Available online: https://www.kff.org/coronavirus-covid-19/poll-finding/vaccine-hesitancy-in-rural-america/ (accessed on 27 March 2022).
- Anaya-Morga, L. UCAL anesthesiologist, vocal against COVID vaccine mandates, is escorted out of workplace. Los Angeles Times, 6 October 2021. [Google Scholar]
- Barnard, A.; Ashford, G.; Vigdor, N. These Health Care Workers Would Rather Get Fired Than Get Vaccinated. The New York Times, 26 September 2021. [Google Scholar]
- Gooch, K. Vaccination-Related Employee Departures at 55 Hospitals, Health Systems. Available online: https://www.beckershospitalreview.com/workforce/vaccination-requirements-spur-employee-terminations-resignations-numbers-from-6-health-systems.html (accessed on 25 March 2022).
- Holpuch, A. ‘I’m Not an Anti-Vaxxer, But…’US Health Workers’ Vaccine Hesitancy Raises Alarm. The Guardian, 10 January 2021. [Google Scholar]
- Zitser, J.; Ankel, S. Here’s Why a Surprising Number of Healthcare Workers Are Rejecting COVID-19 Vaccines Despite Having Witnessed the Immense Suffering of the Pandemic. Available online: https://www.businessinsider.com/covid-19-heres-why-healthcare-workers-are-turning-down-the-vaccines-2021-2 (accessed on 26 April 2022).
- Siegler, A.J.; Luisi, N.; Hall, E.W.; Bradley, H.; Sanchez, T.; Lopman, B.A.; Sullivan, P.S. Trajectory of COVID-19 Vaccine Hesitancy Over Time and Association of Initial Vaccine Hesitancy With Subsequent Vaccination. JAMA Netw. Open 2021, 4, e2126882. [Google Scholar] [CrossRef]
- Youssef, D.; Abou-Abbas, L.; Berry, A.; Youssef, J.; Hassan, H. Determinants of acceptance of Coronavirus disease-2019 (COVID-19) vaccine among Lebanese health care workers using health belief model. PLoS ONE 2022, 17, e0264128. [Google Scholar] [CrossRef]
- Shachar, C. Understanding Vaccine Hesitancy and Refusal Through a Rights-Based Framework. Am. J. Public Health 2022, 112, 229–231. [Google Scholar] [CrossRef] [PubMed]
- Association, A.M. AMA in Support of COVID-19 Vaccine Mandates for Health Care Workers. Available online: https://www.ama-assn.org/press-center/press-releases/ama-support-covid-19-vaccine-mandates-health-care-workers (accessed on 28 March 2022).
- Wang, K.; Wong, E.L.-Y.; Ho, K.-F.; Cheung, A.W.-L.; Yau, P.S.-Y.; Dong, D.; Wong, S.Y.-S.; Yeoh, E.-K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef] [PubMed]
- Farah, W.; Breeher, L.; Shah, V.; Hainy, C.; Tommaso, C.P.; Swift, M.D. Disparities in COVID-19 vaccine uptake among health care workers. Vaccine 2022, 40, 2749–2754. [Google Scholar] [CrossRef] [PubMed]
- Gesser-Edelsburg, A.; Walter, N.; Green, M.S. Health care workers—Part of the system or part of the public? Ambivalent risk perception in health care workers. Am. J. Infect. Control 2014, 42, 829–833. [Google Scholar] [CrossRef]
- Betsch, C. Overcoming healthcare workers vaccine refusal—Competition between egoism and altruism. Eurosurveill 2014, 19, 20979. [Google Scholar] [CrossRef]
- Štěpánek, L.; Janošíková, M.; Nakládalová, M.; Ivanová, K.; Macík, J.; Boriková, A.; Vildová, H. Motivation for COVID-19 Vaccination in Priority Occupational Groups: A Cross-Sectional Survey. Int. J. Environ. Res. Public Health 2021, 18, 11726. [Google Scholar] [CrossRef]
- Experimental? It Doesn’t Mean What You Think It Means. Available online: https://www.denverlawreview.org/dlr-online-article/experimental-it-doesnt-mean-what-you-think-it-means. (accessed on 26 April 2022).
- Aci, O.S.; Kackin, O.; Karaaslan, S.; Ciydem, E. Qualitative examination of the attitudes of healthcare workers in Turkey regarding COVID-19 vaccines. Int. J. Nurs. Knowl. 2022, 33, 136–146. [Google Scholar] [CrossRef]
- Abramson, Z.H.; Levi, O. Influenza vaccination among primary healthcare workers. Vaccine 2008, 26, 2482–2489. [Google Scholar] [CrossRef]
- Nilan, K.; McKeever, T.M.; McNeill, A.; Raw, M.; Murray, R.L. Prevalence of tobacco use in healthcare workers: A systematic review and meta-analysis. PLoS ONE 2019, 14, e0220168. [Google Scholar] [CrossRef]
- Chudasama, R.V.; Khunti, K.; Ekezie, W.C.; Pareek, M.; Zaccardi, F.; Gillies, C.L.; Seidu, S.; Davies, M.J.; Chudasama, Y.V. COVID-19 vaccine uptake and hesitancy opinions from frontline health care and social care workers: Survey data from 37 countries. Diabetes Metab. Syndr. Clin. Res. Rev. 2022, 16, 102361. [Google Scholar] [CrossRef]
- Tsirtsakis, A. What Makes Healthcare Workers Vaccine Hesitant? Available online: https://www1.racgp.org.au/newsgp/clinical/what-makes-healthcare-workers-vaccine-hesitant (accessed on 20 March 2022).
- Hollingsworth, H. Unvaccinated Medical Workers Turn to Religious Exemptions. Available online: https://www.usnews.com/news/us/articles/2022-02-14/unvaccinated-medical-workers-turn-to-religious-exemptions (accessed on 30 March 2022).
- Honora, A.; Wang, K.-Y.; Chih, W.-H. How does information overload about COVID-19 vaccines influence individuals’ vaccination intentions? The roles of cyberchondria, perceived risk, and vaccine skepticism. Comput. Hum. Behav. 2022, 130, 107176. [Google Scholar] [CrossRef] [PubMed]
- Noushad, M.; Rastam, S.; Nassani, M.Z.; Al-Saqqaf, I.S.; Hussain, M.; Yaroko, A.A.; Arshad, M.; Kirfi, A.M.; Koppolu, P.; Niazi, F.H.; et al. A Global Survey of COVID-19 Vaccine Acceptance Among Healthcare Workers. Front. Public Health 2022, 9, 794673. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, C.; Wilson, R.; O’Leary, M.; Eckersberger, E.; Larson, H.J. Strategies for addressing vaccine hesitancy—A systematic review. Vaccine 2015, 33, 4180–4190. [Google Scholar] [CrossRef] [PubMed]
- Nyhan, B.; Reifler, J.; Richey, S.; Freed, G.L. Effective Messages in Vaccine Promotion: A Randomized Trial. Pediatrics 2014, 133, e835–e842. [Google Scholar] [CrossRef] [PubMed]
- Takamatsu, A.; Honda, H.; Kojima, T.; Murata, K.; Babcock, H.M. Promoting coronavirus disease 2019 (COVID-19) vaccination among healthcare personnel: A multifaceted intervention at a tertiary-care center in Japan. Infect. Control Hosp. Epidemiol. 2021, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Berry, S.D.; Baier, R.R.; Syme, M.; Gouskova, N.; Bishnoi, C.; Patel, U.; Leitson, M.; Gharpure, R.; Stone, N.D.; Link-Gelles, R.; et al. Strategies associated with COVID-19 vaccine coverage among nursing home staff. J. Am. Geriatr. Soc. 2022, 70, 19–28. [Google Scholar] [CrossRef]
- Berry, S.D.; Goldfeld, K.S.; McConeghy, K.; Gifford, D.; Davidson, H.E.; Han, L.; Syme, M.; Gandhi, A.; Mitchell, S.L.; Harrison, J.; et al. Evaluating the Findings of the IMPACT-C Randomized Clinical Trial to Improve COVID-19 Vaccine Coverage in Skilled Nursing Facilities. JAMA Intern. Med. 2022, 182, 324–331. [Google Scholar] [CrossRef]
- Campos-Mercade, P.; Meier, A.N.; Schneider, F.H.; Meier, S.; Pope, D.; Wengström, E. Monetary incentives increase COVID-19 vaccinations. Science 2021, 374, 879–882. [Google Scholar] [CrossRef]
- Chang, T.; Jacobson, M.; Shah, M.; Pramanik, R.; Shah, S.B. Financial Incentives and Other Nudges Do Not Increase COVID-19 Vaccinations among The Vaccine Hesitant; National Bureau of Economic Research: Cambridge, MA, USA, 2021. [Google Scholar]
- Brewer, N.T.; Buttenheim, A.M.; Clinton, C.V.; Mello, M.M.; Benjamin, R.M.; Callaghan, T.; Caplan, A.; Carpiano, R.M.; DiResta, R.; Elharake, J.A.; et al. Incentives for COVID-19 vaccination. Lancet Reg. Health-Am. 2022, 8, 100205. [Google Scholar] [CrossRef]
- Jecker, N.S. Cash incentives, ethics, and COVID-19 vaccination. Science 2021, 374, 819–820. [Google Scholar] [CrossRef]
- World Health Organization. Behavioural Considerations for Acceptance and Uptake of COVID-19 Vaccines: WHO Technical Advisory Group on Behavioural Insights and Sciences for Health; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Santos, H.C.; Goren, A.; Chabris, C.F.; Meyer, M.N. Effect of Targeted Behavioral Science Messages on COVID-19 Vaccination Registration Among Employees of a Large Health System: A Randomized Trial. JAMA Netw. Open 2021, 4, e2118702. [Google Scholar] [CrossRef] [PubMed]
- Presseau, J.; Desveaux, L.; Allen, U.; Arnason, T.; Buchan, J.; Corace, K.; Dubey, V.; Evans, G.; Fabrigar, L.; Grimshaw, J. Behavioural science principles for supporting COVID-19 vaccine confidence and uptake among Ontario health care workers. Sci. Briefs Ont. COVID-19 Sci. Advis. Table 2021, 2, 12. [Google Scholar]
- Centers for Disease Control and Prevention. How to Build Healthcare Personnel’s Confidence in COVID-19 Vaccines; CDC: Atlanta, GA, USA, 2021. [Google Scholar]
- Hood, J.; Smith, A.; Childre, F. Developing a “Best Practice” Influenza Vaccination Program for Health Care Workers—An Evidence-Based, Leadership-Modeled Program. AAOHN J. 2009, 57, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Heyerdahl, L.W.; Dielen, S.; Nguyen, T.; Van Riet, C.; Kattumana, T.; Simas, C.; Vandaele, N.; Vandamme, A.-M.; Vandermeulen, C.; Giles-Vernick, T.; et al. Doubt at the core: Unspoken vaccine hesitancy among healthcare workers. Lancet Reg. Health-Eur. 2022, 12, 100289. [Google Scholar] [CrossRef]
- Evans, C.T.; DeYoung, B.J.; Gray, E.L.; Wallia, A.; Ho, J.; Carnethon, M.; Zembower, T.R.; Hirschhorn, L.R.; Wilkins, J.T. Coronavirus disease 2019 (COVID-19) vaccine intentions and uptake in a tertiary-care healthcare system: A longitudinal study. Infect. Control Hosp. Epidemiol. 2021, 1–7. [Google Scholar] [CrossRef]
- Kasozi, K.I.; Laudisoit, A.; Osuwat, L.O.; Batiha, G.E.; Al Omairi, N.E.; Aigbogun, E.; Ninsiima, H.I.; Usman, I.M.; DeTora, L.M.; MacLeod, E.T.; et al. A Descriptive-Multivariate Analysis of Community Knowledge, Confidence, and Trust in COVID-19 Clinical Trials among Healthcare Workers in Uganda. Vaccines 2021, 9, 253. [Google Scholar] [CrossRef]
- Adane, M.; Ademas, A.; Kloos, H. Knowledge, attitudes, and perceptions of COVID-19 vaccine and refusal to receive COVID-19 vaccine among healthcare workers in northeastern Ethiopia. BMC Public Health 2022, 22, 128. [Google Scholar] [CrossRef]
- Charles, S.; Gussone, F. Nurses Who Vaccinate: Anti-Vaccine Myth Dispeller Talks with Lester Holt. Available online: https://www.nbcnews.com/storyline/measles-outbreak/nurses-who-vaccinate-anti-vaccine-myth-dispeller-talks-lester-holt-n994736 (accessed on 5 March 2022).
- Mills, M.C.; Rüttenauer, T. The effect of mandatory COVID-19 certificates on vaccine uptake: Synthetic-control modelling of six countries. Lancet Public Health 2022, 7, e15–e22. [Google Scholar] [CrossRef]
- Juarez, R.; Siegal, N.; Maunakea, A. The Effects of COVID-19 Vaccine Mandates in Hawaii. Vaccines 2022, 10, 773. [Google Scholar] [CrossRef]
- Lytras, T.; Kopsachilis, F.; Mouratidou, E.; Papamichail, D.; Bonovas, S. Interventions to increase seasonal influenza vaccine coverage in healthcare workers: A systematic review and meta-regression analysis. Hum. Vaccines Immunother. 2016, 12, 671–681. [Google Scholar] [CrossRef]
- Poyiadji, N.; Tassopoulos, A.; Myers, D.T.; Wolf, L.; Griffith, B. COVID-19 Vaccine Mandates: Impact on Radiology Department Operations and Mitigation Strategies. J. Am. Coll. Radiol. 2022, 19, 437–445. [Google Scholar] [CrossRef] [PubMed]
- Winston, L.; Wagner, S.; Chan, S. Healthcare workers under a mandated H1N1 vaccination policy with employment termination penalty: A survey to assess employee perception. Vaccine 2014, 32, 4786–4790. [Google Scholar] [CrossRef] [PubMed]
- Rashid, H.; Yin, J.K.; Ward, K.; King, C.; Seale, H.; Booy, R. Assessing Interventions To Improve Influenza Vaccine Uptake Among Health Care Workers. Health Aff. 2016, 35, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Perlin, J.B.; Septimus, E.J.; Cormier, S.B.; Moody, J.A.; Hickok, J.D.; Bracken, R.M. Developing a program to increase seasonal influenza vaccination of healthcare workers: Lessons from a system of community hospitals. J. Healthc Qual. 2013, 35, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Influenza Vaccination Coverage among Health Care Personnel—United States, 2018–2019 Influenza Season; CDC: Atlanta, GA, USA, 2020. [Google Scholar]
- Madani, D. New York Hospital to ‘Pause’ Delivering Babies after Staffers Quit Rather Than Get Vaccinated. Available online: https://www.nbcnews.com/news/us-news/new-york-hospital-pause-delivering-babies-after-staffers-quit-rather-n1279001 (accessed on 20 March 2022).
- Monsalud, C.F.L.; Lind, M.F.G.; Hines, C.M.; Schora, D.; Grant, J.; McElvania, E.; Singh, K. Mitigating staff shortages: Risk of permitting healthcare workers to return to work after coronavirus disease 2019 (COVID-19) exposure. Infect. Control Hosp. Epidemiol. 2021, 1–2. [Google Scholar] [CrossRef]
- Sprengholz, P.; Betsch, C.; Böhm, R. Reactance revisited: Consequences of mandatory and scarce vaccination in the case of COVID-19. Appl. Psychol. Health Well-Being 2021, 13, 986–995. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Author | Survey Date | Country | Participants Number | Response | Author’s Conclusion |
|---|---|---|---|---|---|
| Verger [53] | October–November 2020 | France, Belgium, Canada | 2678 (Physicians and Nurses) | 48.6%—high acceptance 23.0%—moderate acceptance 28.4%—hesitancy or reluctance Main concern- safety | Must build trust about efficacy and safety |
| Biswas [99] | February 2020–January 2021 35 different studies | Worldwide | HCW 76,741 | 22.51% hesitant Range 4.3–72.0% Main concerns: side effects, safety, efficacy | Education and policy-based interventions are needed to ensure vaccination |
| Meyer [139] | December 2020 | United States | HCW 16,292 | 55.3% will receive 16.3% will not 28.4 % unsure Intentions to receive increased after EUA recommendation | Highly visible information from experts may increase intent |
| Pal [140] | February–March 2021 | United States | HCW 1374 | 7.9% hesitant Mistrust important factor 83.6% would accept an annual booster | Concerns about safety and efficacy and lack of trust underlie hesitancy |
| Bell [103] | January 2021 | United Kingdom | HCW SCW 1917 | 6.6% declined vaccine offer Complex analysis of characteristics of participants | Authors offer detailed policy recommendations |
| Woolf [141] | April–June 2021 | United Kingdom | HCW 5633 total 3235 answered free text question | 18% favored mandatory vaccination | Building trust with education and support may be effective with hesitant HCW |
| Janssen [81] | December 2020–March 2021 | France | 4349 HCWs | Online survey presenting hypothetical scenarios for efficacy, longevity, and adverse events. Quantified the effect of each on willingness. | Fear of adverse events was main concern, hesitancy decreased with time. Reassurance about adverse events is important. |
| Choi [142] | March–May 2021 | United States | 2948 HCWs surveyed, with semi-structured interviews | Nurses less likely than physicians to see vaccine as safe or effective. Many claiming vaccines unnecessary or unsafe. | Stressed education and mandates |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peterson, C.J.; Lee, B.; Nugent, K. COVID-19 Vaccination Hesitancy among Healthcare Workers—A Review. Vaccines 2022, 10, 948. https://doi.org/10.3390/vaccines10060948
Peterson CJ, Lee B, Nugent K. COVID-19 Vaccination Hesitancy among Healthcare Workers—A Review. Vaccines. 2022; 10(6):948. https://doi.org/10.3390/vaccines10060948
Chicago/Turabian StylePeterson, Christopher J., Benjamin Lee, and Kenneth Nugent. 2022. "COVID-19 Vaccination Hesitancy among Healthcare Workers—A Review" Vaccines 10, no. 6: 948. https://doi.org/10.3390/vaccines10060948
APA StylePeterson, C. J., Lee, B., & Nugent, K. (2022). COVID-19 Vaccination Hesitancy among Healthcare Workers—A Review. Vaccines, 10(6), 948. https://doi.org/10.3390/vaccines10060948