
COVID-19 Breakthrough Infection after Inactivated Vaccine Induced Robust Antibody Responses and Cross-Neutralization of SARS-CoV-2 Variants, but Less Immunity against Omicron

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Binding—Antibody and Surrogate Virus Neutralization Test (sVNT)
2.3. Focus Reduction Neutralization Test (FRNT50)
2.4. Statistical Analysis
3. Results
3.1. Demographic Data
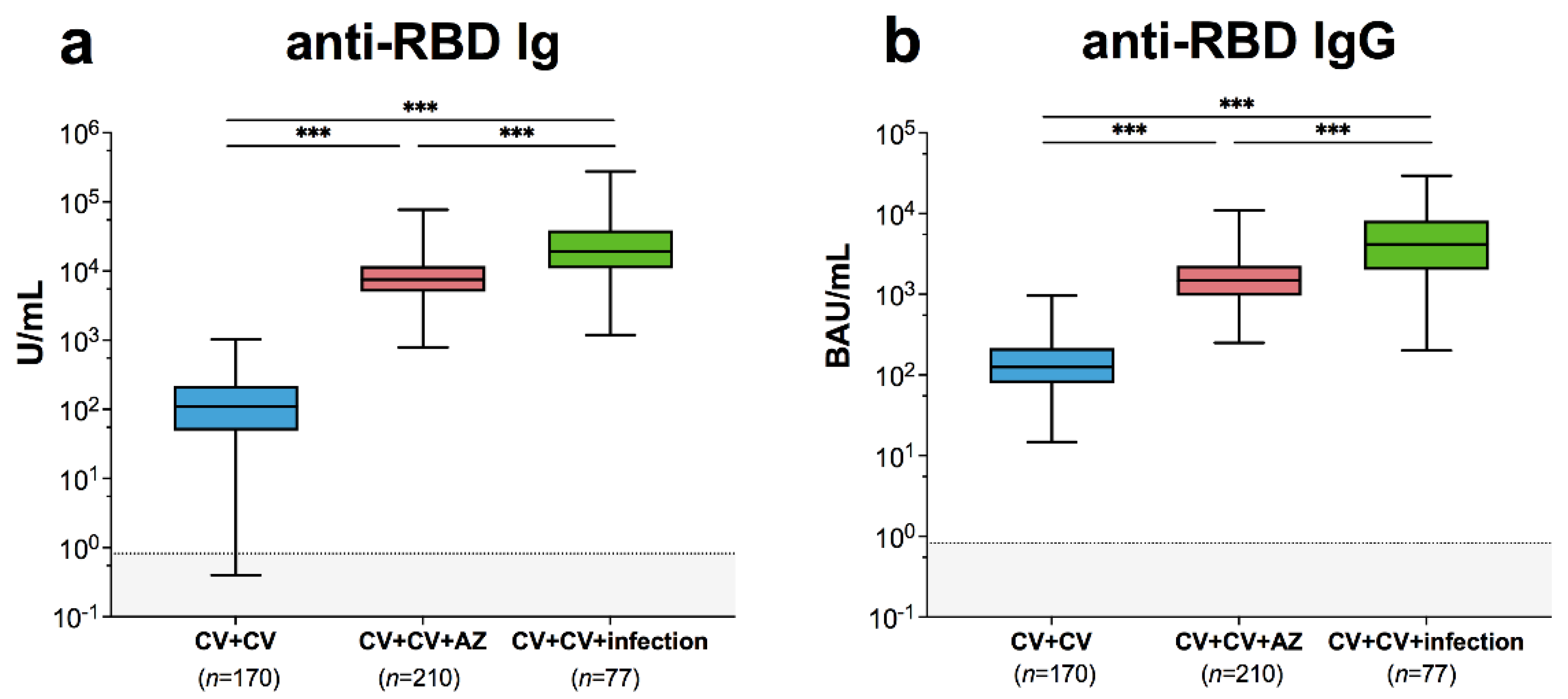
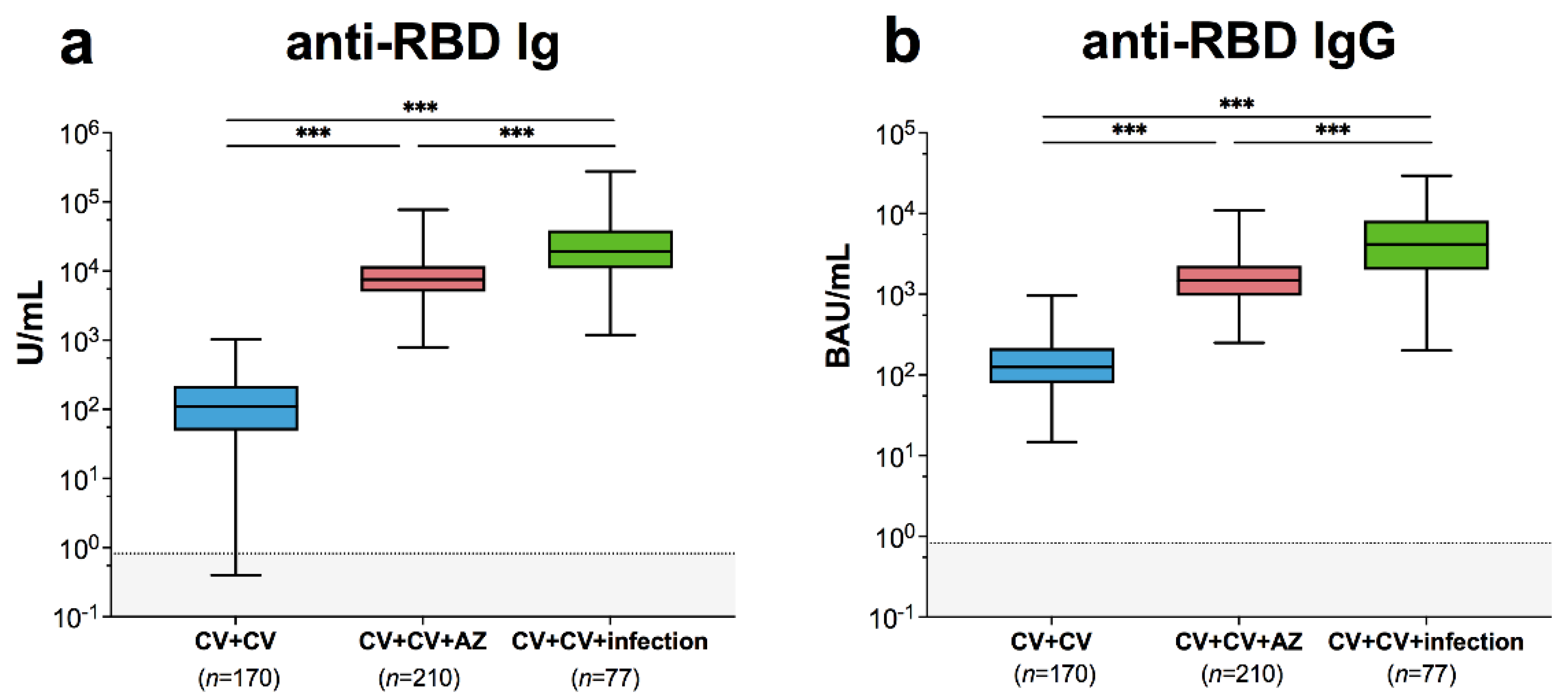
3.2. Binding Antibody Measurement
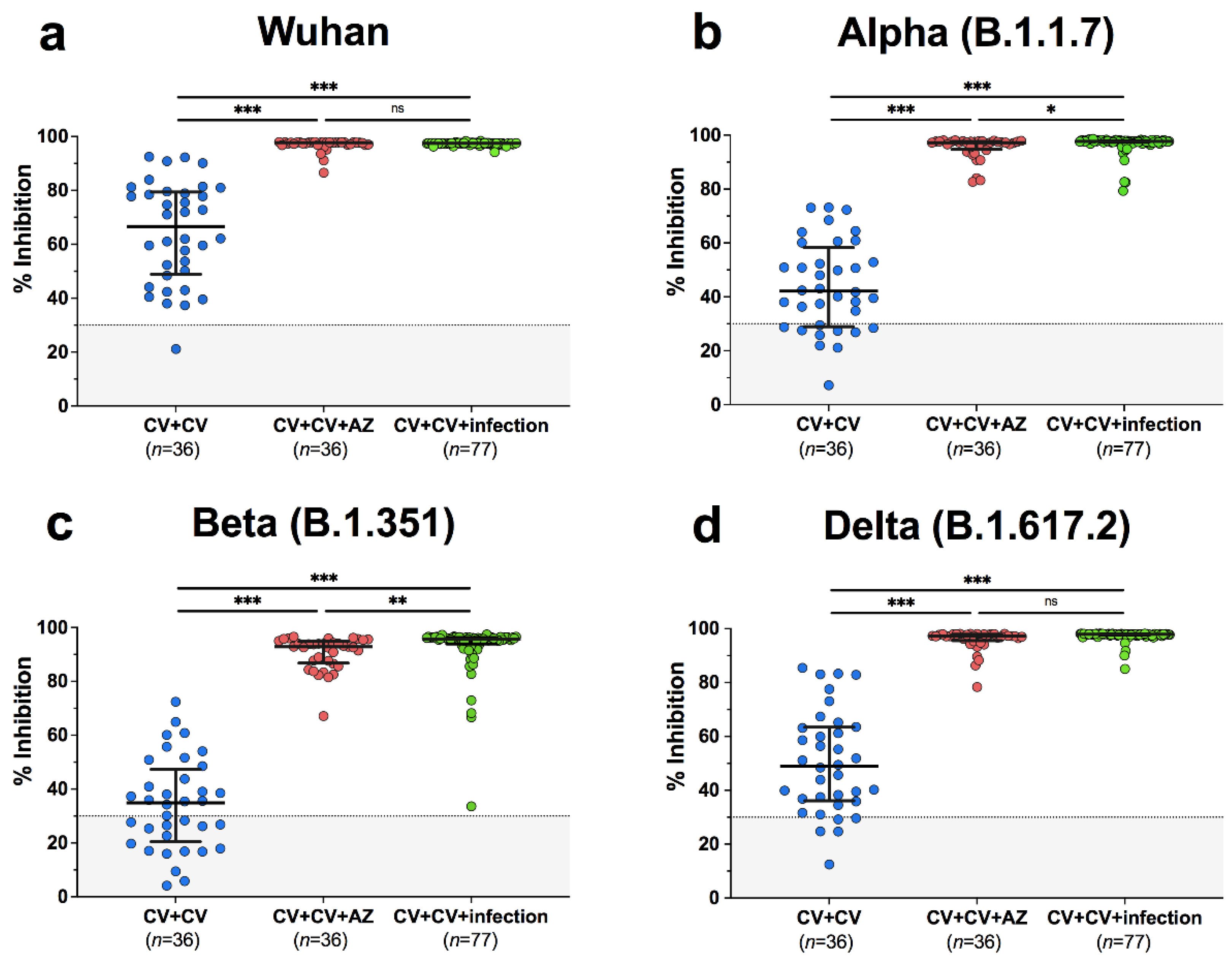
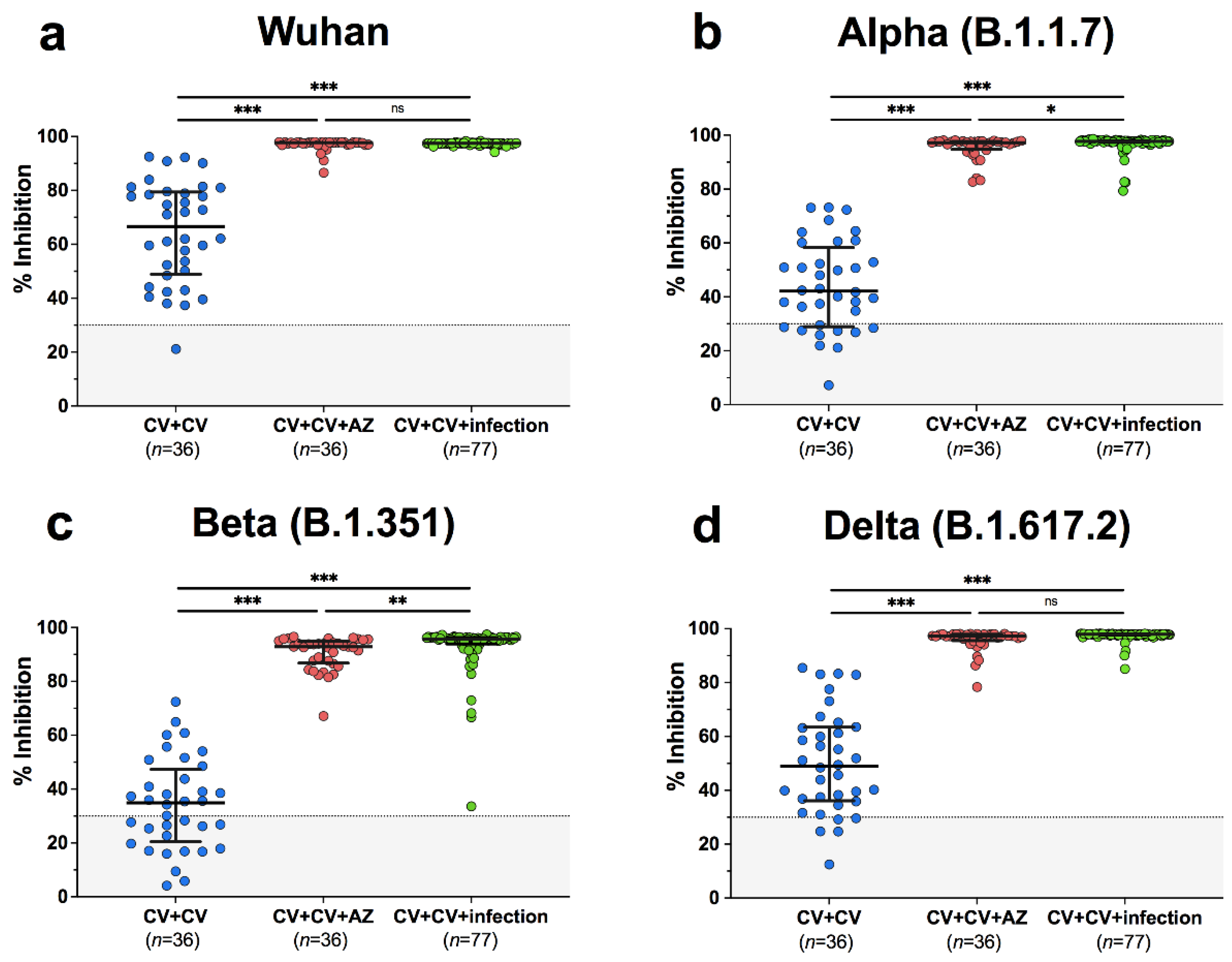
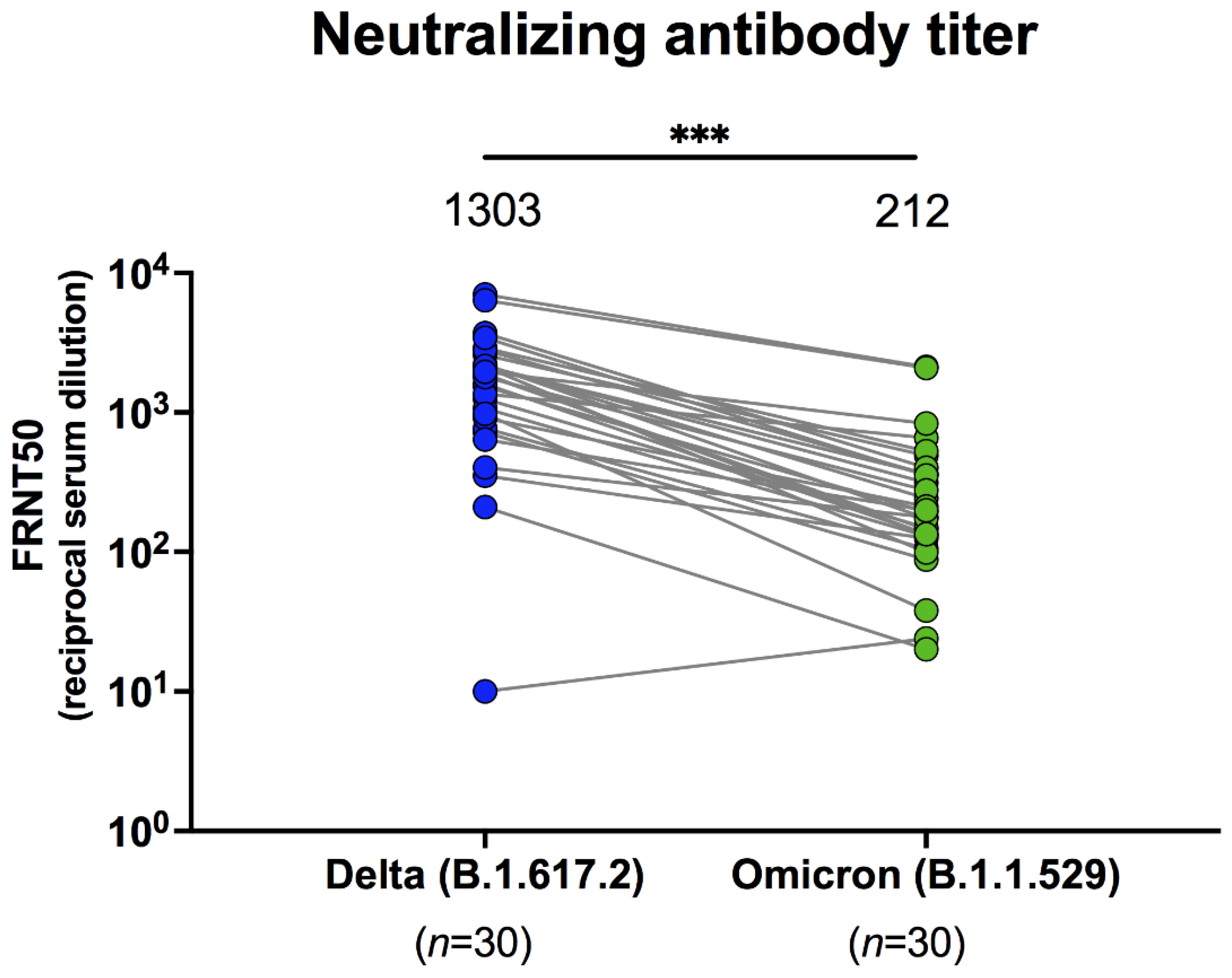
3.3. Neutralization Assay
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 14 January 2022).
- Thepgumpanat, P. Reuters: Thailand Allows Emergency Use of Sinovac’s COVID-19 Vaccine. Available online: https://www.reuters.com/article/us-health-coronavirus-thailand-idUSKBN2AM1BX (accessed on 26 February 2022).
- Thailand Food and Drug Administration. Summary of Product Characteristic CoronaVac. Available online: https://www.fda.moph.go.th/sites/drug/Shared%20Documents/Vaccine/U1DR1C1072640000311C-SPC-EN.pdf (accessed on 26 February 2022).
- European Medicine Agency. Vaxzevria (Previously COVID-19 Vaccne AstraZeneca). Available online: https://www.ema.europa.eu/en/medicines/human/EPAR/vaxzevria-previously-covid-19-vaccine-astrazeneca (accessed on 26 February 2022).
- Mizrahi, B.; Lotan, R.; Kalkstein, N.; Peretz, A.; Perez, G.; Ben-Tov, A.; Chodick, G.; Gazit, S.; Patalon, T. Correlation of SARS-CoV-2-breakthrough infections to time-from-vaccine. Nat. Commun. 2021, 12, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Bergwerk, M.; Gonen, T.; Lustig, Y.; Amit, S.; Lipsitch, M.; Cohen, C.; Mandelboim, M.; Levin, E.G.; Rubin, C.; Indenbaum, V.; et al. Covid-19 breakthrough infections in vaccinated health care workers. N. Engl. J. Med. 2021, 385, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Yorsaeng, R.; Suntronwong, N.; Phowatthanasathian, H.; Assawakosri, S.; Kanokudom, S.; Thongmee, T.; Vichaiwattana, P.; Auphimai, C.; Wongsrisang, L.; Srimuan, D.; et al. Immunogenicity of a third dose viral-vectored COVID-19 vaccine after receiving two-dose inactivated vaccines in healthy adults. Vaccine 2021, 40, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Ai, J.; Zhang, H.; Zhang, Y.; Lin, K.; Zhang, Y.; Wu, J.; Wan, Y.; Huang, Y.; Song, J.; Fu, Z.; et al. Omicron variant showed lower neutralizing sensitivity than other SARS-CoV-2 variants to immune sera elicited by vaccines after boost. Emerg. Microbes Infect. 2022, 11, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Nemet, I.; Kliker, L.; Lustig, Y.; Zuckerman, N.; Erster, O.; Cohen, C.; Kreiss, Y.; Alroy-Preis, S.; Regev-Yochay, G.; Mendelson, E.; et al. Third BNT162b2 Vaccination Neutralization of SARS-CoV-2 Omicron Infection. N. Engl. J. Med. 2022, 386, 492–494. [Google Scholar] [CrossRef] [PubMed]
- Zuo, F.; Abolhassani, H.; Du, L.; Piralla, A.; Bertoglio, F.; de Campos-Mata, L.; Wan, H.; Schubert, M.; Wang, Y.; Sun, R.; et al. Heterologous immunization with inactivated vaccine followed by mRNA booster elicits strong humoral and cellular immune responses against the SARS-CoV-2 Omicron variant. medRxiv 2022. [Google Scholar] [CrossRef]
- Assawakosri, S.; Kanokudom, S.; Suntronwong, N.; Auphimai, C.; Nilyanimit, P.; Vichaiwattana, P.; Thongmee, T.; Duangchinda, T.; Chantima, W.; Pakchotanon, P.; et al. Neutralizing Activities against the Omicron Variant after a Heterologous Booster in Healthy Adults Receiving Two Doses of CoronaVac Vaccination. medRxiv 2022. [Google Scholar] [CrossRef]
- Tan, C.W.; Chia, W.N.; Qin, X.; Liu, P.; Chen, M.I.; Tiu, C.; Hu, Z.; Chen, V.C.; Young, B.E.; Sia, W.R.; et al. A SARS-CoV-2 surrogate virus neutralization test based on antibody-mediated blockage of ACE2-spike protein-protein interaction. Nat. Biotechnol. 2020, 38, 1073–1078. [Google Scholar] [CrossRef] [PubMed]
- Supasa, P.; Zhou, D.; Dejnirattisai, W.; Liu, C.; Mentzer, A.J.; Ginn, H.M.; Zhao, Y.; Duyvesteyn, H.M.E.; Nutalai, R.; Tuekprakhon, A.; et al. Reduced neutralization of SARS-CoV-2 B.1.1.7 variant by convalescent and vaccine sera. Cell 2021, 184, 2201–2211. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Phillips, D.J.; White, T.; Sayal, H.; Aley, P.K.; Bibi, S.; Dold, C.; Fuskova, M.; Gilbert, S.C.; Hirsch, I.; et al. Correlates of protection against symptomatic and asymptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 2032–2040. [Google Scholar] [CrossRef] [PubMed]
- Bates, T.A.; McBride, S.K.; Winders, B.; Choen, D.; Trautmann, L.; Curlin, M.E.; Tafesse, F.G. Antibody response and variant cross-neutralization after SARS-CoV-2 breakthrough infection. JAMA 2022, 327, 179–181. [Google Scholar] [CrossRef]
- Stamatatos, L.; Czartoski, J.; Wan, Y.H.; Homad, L.J.; Rubin, V.; Glantz, H.; Neradilek, M.; Seydoux, E.; Jennewein, M.F.; MacCamy, A.J.; et al. mRNA vaccination boosts cross-variant neutralizing antibodies elicited by SARS-CoV-2 infection. Science 2021, 372, eabg9175. [Google Scholar] [CrossRef]
- Pulliam, J.R.; van Schalkwyk, C.; Govender, N.; von Gottberg, A.; Cohen, C.; Groome, M.J.; Dushoff, J.; Mlisana, K.; Moultrie, H. Increased risk of SARS-CoV-2 reinfection associated with emergence of the Omicron variant in South Africa. medRxiv 2021. [Google Scholar] [CrossRef]
- Roessler, A.; Riepler, L.; Bante, D.; von Laer, D.; Kimpel, J. SARS-CoV-2 B. 1.1. 529 variant (Omicron) evades neutralization by sera from vaccinated and convalescent individuals. medRxiv 2021. [Google Scholar] [CrossRef]
- Sarkar, R.; Lo, M.; Saha, R.; Dutta, S.; Chawla-Sarkar, M. S glycoprotein diversity of the Omicron variant. medRxiv 2021. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | CV + CV (n = 170) | CV + CV + AZ (n = 210) | CV + CV + INF (n = 77) | p-Value |
|---|---|---|---|---|
| Sex (n, %) | ||||
| female | 89 (52.4%) | 151 (71.9%) | 58 (75.3%) | p < 0.001 a, p < 0.001 b, p = 0.56 c |
| male | 81 (47.6%) | 59 (28.1%) | 19 (24.7%) | |
| Age in years (mean, SD) | 42.3 (9.6) | 40.0 (9.8) | 34.2 (9.9) | p = 0.02 d, p < 0.001 e, p < 0.001 f |
| Interval between 1st and 2nd dose (median, IQR) | 23 (21–26) | 21 (21–26) | 23 (21–28) | |
| Interval between 2nd and 3rd dose (median, IQR) | N/A | 70 (61–79) | N/A | |
| Interval between 2nd dose and symptom onset (median, IQR) | N/A | N/A | 88 (68–100) | |
| Interval between last vaccination and blood sampling (median, IQR) | 29 (27–31) | 28 (20–32) | N/A | |
| Interval between symptom onset and blood sampling (median, IQR) | N/A | N/A | 34 (29–43) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suntronwong, N.; Yorsaeng, R.; Puenpa, J.; Auphimai, C.; Thongmee, T.; Vichaiwattana, P.; Kanokudom, S.; Duangchinda, T.; Chantima, W.; Pakchotanon, P.; et al. COVID-19 Breakthrough Infection after Inactivated Vaccine Induced Robust Antibody Responses and Cross-Neutralization of SARS-CoV-2 Variants, but Less Immunity against Omicron. Vaccines 2022, 10, 391. https://doi.org/10.3390/vaccines10030391
Suntronwong N, Yorsaeng R, Puenpa J, Auphimai C, Thongmee T, Vichaiwattana P, Kanokudom S, Duangchinda T, Chantima W, Pakchotanon P, et al. COVID-19 Breakthrough Infection after Inactivated Vaccine Induced Robust Antibody Responses and Cross-Neutralization of SARS-CoV-2 Variants, but Less Immunity against Omicron. Vaccines. 2022; 10(3):391. https://doi.org/10.3390/vaccines10030391
Chicago/Turabian StyleSuntronwong, Nungruthai, Ritthideach Yorsaeng, Jiratchaya Puenpa, Chompoonut Auphimai, Thanunrat Thongmee, Preeyaporn Vichaiwattana, Sitthichai Kanokudom, Thaneeya Duangchinda, Warangkana Chantima, Pattarakul Pakchotanon, and et al. 2022. "COVID-19 Breakthrough Infection after Inactivated Vaccine Induced Robust Antibody Responses and Cross-Neutralization of SARS-CoV-2 Variants, but Less Immunity against Omicron" Vaccines 10, no. 3: 391. https://doi.org/10.3390/vaccines10030391
APA StyleSuntronwong, N., Yorsaeng, R., Puenpa, J., Auphimai, C., Thongmee, T., Vichaiwattana, P., Kanokudom, S., Duangchinda, T., Chantima, W., Pakchotanon, P., Assawakosri, S., Nilyanimit, P., Klinfueng, S., Wongsrisang, L., Srimuan, D., Thatsanatorn, T., Sudhinaraset, N., Wanlapakorn, N., & Poovorawan, Y. (2022). COVID-19 Breakthrough Infection after Inactivated Vaccine Induced Robust Antibody Responses and Cross-Neutralization of SARS-CoV-2 Variants, but Less Immunity against Omicron. Vaccines, 10(3), 391. https://doi.org/10.3390/vaccines10030391