Abstract
The current study uses data surveyed between August and September 2021 in four ASEAN (Association of South East Asian Nations) countries to identify drivers of COVID-19 vaccine acceptance with different levels of the pandemic severity. It also examines the impact of the drivers on vaccine acceptance. The results show that the number of respondents who accept vaccines significantly dominates that of those who do not. In addition, the number of respondents who get the vaccine if the pandemic becomes more severe dominates that of those if it becomes less severe. Results generated from the logistic regressions show that the impact of the drivers on the COVID-19 vaccine acceptance with different levels of the pandemic severity varies in terms of magnitude and direction. Practical recommendations are made based on the findings.
1. Introduction
COVID-19 was declared a global pandemic in March 2020 [1]. However, the first case was detected on 30 December 2019 [2]. Eight months later (the date that the surveys to collect data for the current study started), the pandemic had spread to all continents, and negatively affected every aspect of people’s lives worldwide. For example, it was blamed for a global GDP loss of approximately 6.7 per cent (approximately four trillion USD) in 2020 [3]. More seriously, the virus infected 211,647,672 people and took 4429,460 lives during the period [4]. Several approaches have been applied to stop the pandemic and among them was vaccination. COVID-19 vaccines have been proven to help slow down the spread of the virus and ultimately to stop it by creating herd immunity. Therefore, COVID-19 vaccines are recommended by the World Health Organization (WHO) and many governments [5]. Although the COVID-19 vaccines are believed to help stop the pandemic, many people hesitate to have the vaccine due to several reasons, such as the level of the pandemic severity. In particular, if the pandemic becomes more severe people will rush to be vaccinated and vice versa. The hesitation and associated behaviors prevent us from reaching herd immunity. In addition, this behavior creates an opportunity for more variants such as Delta or Omicron [6] to develop, which may be more difficult to deal with. Vietnam, Indonesia, the Philippines, and Malaysia are among ASEAN countries where the cases and deaths caused by the pandemic were the highest and the vaccine coverage was lowest when the Delta variant of the Coronavirus emerged. The current study endeavors to identify the drivers of COVID-19 vaccine acceptance (“vaccine acceptance” and “willingness to be vaccinated” are interchangeably used in the current study) with different levels of the pandemic severity and to examine the impact of the drivers on the acceptance.
2. Research Design, Methodology and Models
2.1. Study Design
2.1.1. Selection of Study Locations
Four countries where the cases and deaths caused by the pandemic were highest and the vaccine coverage is lowest in the ASEAN countries were selected. These include Vietnam, Indonesia, the Philippines, and Malaysia.
Vietnam is a good country to be selected for the study for the following reasons: the country has successfully dealt with COVID-19 in the first three waves by applying the 5K (in Vietnamese) rules. The rules are mask-wearing (Khau trang), disinfection (Khu khuan), social distancing (Khoang cach), no gathering (Khong tu tap) and health declaration (Khai bao y te). It can be seen that vaccination was not among the recommended rules [7].
In the fourth wave, which occurred in April 2021 with the emergence of the new variant, Delta (more infectious, more lethal and faster spread speed), the old approaches (quick track of F0, quarantine or lockdown, etc.) were not sufficiently applicable and useful anymore. In the meantime, the vaccine campaign had not started. As a result, the outbreak appeared to be out of control. In particular, the number of cases and deaths caused by the pandemic in the nation from 27 April 2021 to 27 August 2021 dramatically increased by 114 and 287 times, respectively. Meanwhile, the total vaccinations per hundred, the number of people vaccinated per hundred and that of people fully vaccinated per hundred estimated on 27 April 2021 was modest, approximately 0.32 [8]. Therefore, vaccination was added to the strategy to cope with the pandemic in Vietnam, as shown in Figure 1.

Figure 1.
The 5K Message and Vaccination to Safely Co-exist with COVID-19 in Vietnam.
Source: Vietnamese Ministry of Health, 2020.
Indonesia had the highest number of COVID-19 cases in ASEAN during the study period. In particular, the number of cases in the country doubled and the number of deaths tripled between 27 April 2021 and 27 August 2021. Meanwhile, the total vaccinations per hundred, the number of people vaccinated per hundred, and that of people fully vaccinated per hundred estimated on 27 April 2021 were 6.96, 4.35 and 2.61, respectively [8]. In addition, the approaches that the government used to deal with the pandemic, including vaccination, are debatable [9,10].
The number of cases and deaths caused by the pandemic in the Philippines doubled between 27 April 2021 and 27 August 2021. Meanwhile, the total vaccinations per hundred, the number of people vaccinated per hundred and that of people fully vaccinated per hundred estimated on 27 April 2021 were 1.63, 1.41 and 0.22, respectively [8].
Between 27 April 2021 and 27 August 2021 the number of cases and deaths caused by the pandemic in Malaysia increased by four and eleven times, respectively. In contrast, the total vaccinations per hundred, the number of people vaccinated per hundred and that of people fully vaccinated per hundred estimated on 27 April 2021 were 4.21, 2.59, and 1.62, respectively [8]. In addition, Arifin and Musa [11] showed that the number of deaths caused by COVID-19 in Malaysian adults who were unvaccinated significantly dominated that of those who were partially or fully vaccinated. As a result, the lockdown lasted longer than that in the other countries and the negative impact was more severe, especially for children [12].
2.1.2. Sampling
Since the dependent variables are dichotomous, logistic regressions are used. The sample size is calculated based on the following formula, which is adopted from Bujang, Sa’at [13]:
x is an integer representing the event per variable and i is the number of independent variables. The recommended x is 50 and the number of independent variables used in the current study is 48. Therefore, the sample size is 2500. During the study period, vaccines were administered to people aged between 18 and 64, then the vaccine coverage was expanded to other age groups. Between the vaccine shots, there is a waiting period. The waiting time varies from vaccine to vaccine. To save time, other age groups (older and younger people) were vaccinated if vaccines were available.
n = 100 + x ∗ i
Google Forms was used to design the questionnaires. The questionnaires were translated into local languages, Filipino, Indonesian, Malaysian, and Vietnamese. Links to the questionnaires were then distributed using email, Facebook, Twitter, Zalo, Viber, and Whatsapp to survey participants. The data in Indonesia were collected between 28 August 2021 and 11 September 2021, those in the Philippines were collected between 27 August 2021 and 16 September 2021, those in Vietnam were collected between 16 August 2021 and 27 August 2021 and those in Malaysia were collected between 16 August 2021 and 14 September 2021.
2.2. Research Methodologies, Models and Variable Description
Since the dependent variables are in binary format (1 = willing to be vaccinated against COVID-19, 0 = unwilling to be vaccinated), a binary regression specification is applied [14]. The independent variables are selected based on previous studies, especially those reviewed in the current study.
Yi represents COVID-19 vaccine acceptance (with different levels of the pandemic severity) of the ith respondent. In particular, Yi1 represents the COVID-19 vaccine acceptance in which the number of cases in the community increases (1 = willing to be vaccinated), Yi2 represents the COVID-19 vaccine acceptance in which the number of cases in the community decreases (1 = willing to be vaccinated), Yi3 represents the COVID-19 vaccine acceptance in which the number of deaths (caused by the virus) in the community increases (1 = willing to be vaccinated), Yi4 represents the COVID-19 vaccine acceptance in which the number of deaths in the community decreases (1 = willing to be vaccinated) and Yi5 represents the COVID-19 vaccine acceptance in which a new variant of the virus emerges (1 = willing to be vaccinated). It is hypothesized that people will be more willing to be vaccinated if the pandemic becomes more severe, such as the number of cases or deaths in their community increases or a new variant emerges [15].
Independent variables are grouped as follows: The willingness to be vaccinated against COVID-19 in people with different socio-demographic characteristics may not be identical. The socio-demographic characteristics in the current study include age (denoted by X1 and measured in years), gender (X2, 1 = male), residence (X3, 1 = urban), marital status (X4, 1 = married or cohabiting), family main income source (X5, 1 = yes), savings (X6, 1 = yes), gold assets (X7, 1 = yes), the number of dependents (X8, persons), education (X9, 1 = tertiary or above) and employment (X10, 1 = employed) [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34]. In addition, the willingness to be vaccinated against the virus of people with national health insurance (X11, 1 = national health insurance member) and private health insurance (X12, 1 = private health insurance member) and that of people without insurance is anticipated not to be the same [15,20,23,29]. Access to information (to receive news on the pandemic and vaccines) is believed to help people to have a better and sufficient understanding of the pandemic and vaccines, hence is expected to have an impact on the willingness to be vaccinated. In the current study, the access is represented by the number of information channels to receive news on the pandemic (X13, measured in channels) and news on the vaccines (X14, measured in channels), the frequency to receive news on the pandemic (X15, 1 = daily, 0 = otherwise) and news on the vaccines (X16, 1 = daily, 0 = otherwise), the sufficiency of news on the pandemic (X17, 1 = sufficient) and on the vaccines (X18, 1 = sufficient). Vulnerable people tend to seek protection from medical interventions such as vaccines. In the current study, a person is considered to be vulnerable if he or she belongs to the vaccine priority groups (X19, 1 = yes) [35] or lives with someone who belongs to these groups (X20, 1 = yes) or has comorbidities (X21, 1 = yes) [36] or has been infected with the virus (X29, 1 = yes) or has a family member or friend or co-worker who is infected with the virus (X30, 1 = yes) [16,18,19,24,28,32]. Similarly, the willingness of people to be vaccinated who are fearful may not be identical to that of those who are fearless. In the current study, it includes the fear of being discriminated against (such as being banned from traveling, entering crowded places such as malls or supermarkets or stadiums, receiving government assistance) if not vaccinated (X31, 1 = fearful, 0 = fearless), the fear of catching the virus (X32, 1 = fearful, 0 = fearless) and the fear of needles (X33, 1 = fearful, 0 = fearless) [15,20,21,26,30,34]. In contrast, people who are concerned about the vaccines and relevant matters tend to hesitate to get vaccinated. In the current study, the respondents were asked if they were concerned about the side effects (X35, 1 = concerned), safety (X38, 1 = concerned), immunity (X37, 1 = concerned), and cost (X40, 1 = concerned) of the vaccines. In addition, they were asked if they were concerned about the sufficiency of the official information on the vaccines (X34, 1 = concerned), the response procedure if a person has a severe shock after being vaccinated (X36, 1 = concerned), the distance between their residence and vaccination site (X39, 1 = concerned), waiting time to be vaccinated (X41, 1 = concerned), time frame within which to be vaccinated (X42, 1 = concerned) and the safety and cleanness of the vaccination waiting room (X43, 1 = concerned) [15,21,22,23,30,31,34]. Knowledge can help people to have a better and sufficient understanding of the pandemic and virus. Therefore, the willingness to be vaccinated of people with better and sufficient knowledge in these aspects and that of other people may not be identical [15,19,20,23,28]. In the current study, respondents were asked and tested as to whether they have sufficient knowledge about common symptoms of people infected with the virus (X22, 1 = sufficient), on the virus transmission route (X23, 1 = sufficient), on the ways to prevent the virus (X24, 1 = sufficient), on the spread speed of the virus (X25, 1 = sufficient), on the virus fatality (X26, 1 = sufficient), on the herd immunity generated by at least 70 per cent of the population having been infected with the virus (X27, 1 = sufficient) and generated by there being at least 70 per cent of the population fully vaccinated (X28, 1 = sufficient) and on the common symptoms after being vaccinated (X44, 1 = sufficient). Four dummy variables are used to represent the nationality of the respondents in the four countries, which are Vietnamese (X45, 1 = Vietnamese), Indonesian (X46, 1 = Indonesian), Filipino (X47, 1 = Filipino) and Malaysian (X48, 1 = Malaysian). These factors can be briefly illustrated in Figure 2.
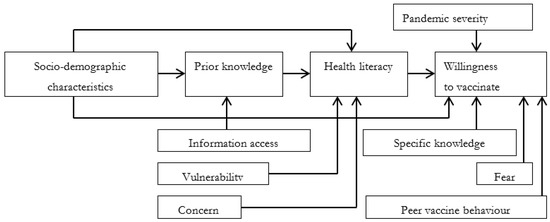
Figure 2.
Conceptual framework on COVID-19 vaccine acceptance. Source. Illustrated by the authors with ideas adapted from Sun, Shi [37].
3. Results and Discussion
3.1. COVID-19 Acceptance and the Pandemic Severity
The respondents were asked if they would be willing to be vaccinated if the number of cases or deaths (caused by the virus) in their community increases or if a new variant of Coronavirus emerges (more severe) and decreases (less severe) or no variants of the virus. Overall, the percentage of respondents who are willing to be vaccinated significantly dominates that of those who are not willing. In addition, if the pandemic becomes more severe the percentage of respondents who are willing to be vaccinated is approximately two per cent higher than that if it becomes less severe.
Details of the number of respondents who are willing to be vaccinated with different levels of the pandemic severity are presented in Table 1 and Figure 3. Figure 3 shows that the COVID-19 vaccine acceptance rate rages between 77 to 80 per cent, depending on the level of the pandemic severity. In particular, the number of respondents (of all ages) who are willing to be vaccinated if the pandemic becomes more severe slightly dominates that of those if it becomes less severe.

Table 1.
COVID-19 vaccine acceptance with different levels of pandemic severity.
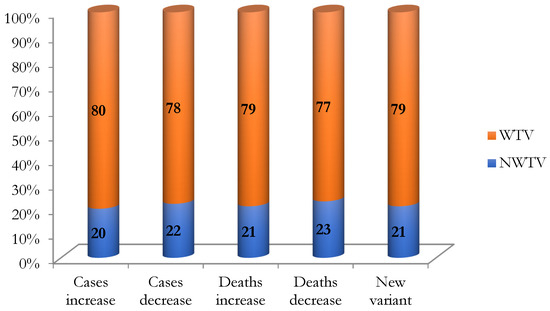
Figure 3.
COVID-19 vaccine acceptance with different levels of pandemic severity. Source. Drawn by the authors using surveyed data. Note. WTV: Willing to be vaccinated, NWTV: Not willing to be vaccinated.
People with more work or family responsibilities tend to seek protective medical intervention, such as vaccines, than other people. As expected, the number of respondents with more family responsibilities such as females (as Asian culture), married or cohabited, the family main income source, with dependents or employed who are willing to be vaccinated significantly dominates that of those with fewer family responsibilities. In addition, the number of respondents (in these groups) who are willing to be vaccinated when the pandemic becomes more severe slightly dominates that of those when it becomes less severe.
The number of rural respondents who are willing to be vaccinated significantly dominates that of urban respondents. In addition, the number of respondents in this group who are willing to be vaccinated when the pandemic becomes more severe slightly dominates that of those when it becomes less serious.
The number of respondents with protection such as having health insurance (national or private) or savings or gold assets who are willing to be vaccinated significantly dominates that of those without the insurance or savings or gold assets. Additionally, the number of respondents (in these groups) who are willing to be vaccinated if the pandemic becomes more severe slightly dominates that of those when it becomes less severe.
The access to information and information sufficiency on the pandemic and vaccines can help people better understand the danger or fatality from the virus and the advantages of the vaccines, hence it may have an impact on their willingness to be vaccinated. The access to information in the current study is represented by the number of channels (12). In addition, it is represented by the frequency (daily or not) that respondents receive the information. It is also represented by the information sufficiency (sufficient or insufficient) that they receive.
As expected, the number of respondents with better information access (such as having more channels—more than 6 out of 12 channels to receive news on the pandemic and vaccines—more frequently receiving the information and receiving sufficient information) who are willing to be vaccinated significantly dominates that of those with poorer information access or insufficient information. Additionally, the number of respondents (in these groups) who are willing to be vaccinated if the pandemic becomes more severe slightly dominates that of those if it becomes less severe.
Vulnerable people tend to seek protection more than those who are not at risk. Vulnerable people in the current study include those who belong to the vaccine priority groups, who live with someone belonging to these groups, or who have a family member or friend or co-worker infected with the virus. The results show that the number of these vulnerable respondents who are willing to be vaccinated significantly dominates that of those who are not. In addition, respondents who have comorbidities and those who have been infected with the virus are listed as vulnerable people. The results show that the number of respondents who do not have any comorbidities or have never been infected with the virus and are willing to be vaccinated slightly dominates that of those who have a medical history or have been infected with the virus. Additionally, when the pandemic becomes more severe the number of vulnerable respondents who are willing to be vaccinated slightly dominates that of those when it becomes less severe.
As previously addressed, possessing better or sufficient knowledge can help people better understand the consequences of being infected with the virus and the advantages of being protected by the vaccines. In the current study, knowledge is represented by general knowledge (education) and specific knowledge. As anticipated, the number of respondents with a higher education level and sufficient knowledge (such as the symptoms of people infected with the Coronavirus, the virus transmission route, the ways to prevent the virus, the virus spread speed, the virus fatality, herd immunity, and the common symptoms after being vaccinated) who are willing to be vaccinated significantly dominates that of those with lower education or insufficient knowledge. In addition, the number of respondents (in these groups) who are willing to be vaccinated if the pandemic becomes more severe slightly dominates that of those if it becomes less severe.
Fear forces people to seek protection. In the current study, it includes the fear of catching the virus, being discriminated against if not vaccinated, and needles. As anticipated, the number of respondents with the fear of the above things (including needles) who are willing to be vaccinated significantly dominates that of those who are fearless. Despite the fear, the number of respondents who are willing to be vaccinated modestly increases if the pandemic becomes more severe.
In contrast to fear, if people are concerned about something, they tend to be reluctant to proceed. The current study asks if the respondents are concerned about the information sufficiency of the vaccines, on the side effects of the vaccines, on the vaccine immunity, on the vaccine safety, on the distance between their residence and the vaccination site, on the vaccine cost, on the waiting time to be vaccinated, on the vaccination time frame and on the safety and cleanness of the vaccination waiting room. The results show that the number of respondents who are not concerned about the above causes and willing to be vaccinated significantly dominates that of those without the concern. Despite the concern, the number of respondents who are willing to be vaccinated slightly increases if the pandemic becomes more severe.
The number of Vietnamese, Indonesian and Filipino respondents who are willing to be vaccinated significantly dominates that of those who are not. In addition, the vaccine acceptance of respondents according to the pandemic severity is identical.
3.2. The Association between COVID-19 Vaccine Acceptance and the Influential Factors
The impact of influential factors on the COVID-19 vaccine acceptance of the respondents is examined using binary regression. Multicollinearity tests have been conducted and the mean VIF (variance inflation factor) is 2.19, which is significantly lower than ten. In addition, the matrix of correlation shows no correlation coefficients greater than 5.5. These test results indicate that no serious issues of multicollinearity exist [38,39,40,41,42,43,44]. The regression results are presented in Table 2.
Table 2.
Association between COVID-19 vaccine acceptance and the influential factors.
As expected, older respondents (X1), who usually possess sufficient knowledge, are more likely to be vaccinated. The impact is significant at the one and five per cent level, depending on the level of the pandemic severity. This finding is almost in accordance with that found by Edwards and Biddle [17], Freeman and Loe [18], and Kessels and Luyten [16], but different from that explored by Al-Mistarehi and Kheirallah [24], and Dodd and Cvejic [23]. The literature also shows that elderly people with a medical history tend to hesitate to be vaccinated. However, their hesitation has consequences. For example, during the fourth wave, approximately 50 per cent of deaths (caused by the virus) in Ho Chi Minh City were elderly people with comorbidities and unvaccinated. To deal with this challenge, medical teams are sent to vaccinate these people at home [45].
As anticipated, urban residents (X3) are more likely to be vaccinated than their counterparts residing in rural areas. The impact is significant at the one and five per cent level, depending on the pandemic severity. This finding is almost similar to that found by Abedin and Islam [22], and Yoda and Katsuyama [21]. In addition to the fixed vaccine delivery points, mobile vaccination should also be arranged to vaccinate people residing in rural areas, especially in remote areas [46].
Gold assets (X7) are considered and used as savings in Asian culture. The results show that respondents with gold assets are less likely to be vaccinated when the number of cases in the community decreases. The impact is significant at the five per cent level.
Respondents with responsibilities such as having a dependent (X8) tend to follow precautionary procedures. The results show this behavior. In particular, respondents with a dependent are more likely to be vaccinated if the number of deaths caused by the virus increases in their community. The impact is significant at the ten per cent level. This finding is almost in accordance with that found by Chew, Cheong [29], Freeman, Loe [18], Khubchandani, Sharma [26], Kourlaba, Kourkouni [28] and Liu and Li [25].
Respondents with the national health insurance membership (X11) are less likely to be vaccinated. The impact is significant at the one and five per cent level, depending on the pandemic severity. If only clients who are willing to be vaccinated can claim insurance, insured clients may change their vaccine acceptance. Dodd, Cvejic [23] found similar behavior in Australia. The vaccines are still new and being a member of the national health insurance may be the driver of their vaccine hesitancy.
Respondents with more information channels (X14, more than 6 out of 12) to receive news on the vaccines are more likely to be vaccinated if the pandemic becomes more severe. The impact is significant at the one, five and ten per cent level, depending on the pandemic severity. Vietnamese are daily updated with news on the pandemic and vaccines through Television and radio programs such as “To Safely Co-exist with COVID-19”, and these channels appear to be efficient [47]. Respondents who daily update with news on the pandemic (X15) are more likely to be vaccinated when the pandemic becomes more severe. The impact is significant at the ten per cent level if the number of cases or deaths increases and at the one per cent level if a new variant emerges. Respondents with sufficient information on the vaccines (X17) are more likely to be vaccinated when the number of cases or deaths increases. The impact is significant at the one and ten per cent level, depending on the pandemic severity.
As anticipated, vulnerable respondents (X19, belong to the vaccine priority groups) are more likely to be vaccinated if the number of cases increases. The impact is significant at the five per cent. This finding is almost in accordance with that found by Freeman, Loe [18], Kessels, Luyten [16] and Kourlaba, Kourkouni [28]. Respondents with comorbidities (X21) are less likely to be vaccinated than those who do not have any medical history. This behavior was observed in the South of Vietnam during the fourth wave [45]. The impact is at the one and five per cent level, depending on the pandemic severity. As previously addressed, the comorbidities and the new vaccines may make them hesitate to be vaccinated. This finding is almost similar to that discovered by Al-Mistarehi, Kheirallah [24], Dodd, Cvejic [23] and Yoda and Katsuyama [21], but different from that found by Abedin, Islam [22].
Respondents with sufficient knowledge about the virus fatality (X26) are more likely to be vaccinated when a new variant emerges. The impact is significant at the ten per cent level. There have been several variants of Coronavirus. It has been proven that they spread faster and are more lethal than the original, especially the Delta. Respondents who believe that herd immunity occurs if at least 70 per cent of the population is fully vaccinated (X28) are more likely to be vaccinated. The impact is significant at the one per cent level. Schwarzinger, Watson [19] examined this behavior, but the impact was not significant.
Respondents who have a family member or a friend or a co-worker infected with the virus (X30) are more likely to be vaccinated. The impact is significant at the one, five, and ten per cent level, depending on pandemic severity. Respondents who are afraid of being discriminated against if not vaccinated (X31) are more likely to be vaccinated than those who are not. The impact is significant at the one per cent level. Apart from volunteering to be vaccinated, laws and regulations (such as fines or imprisonment) applied to those who are not willing to be vaccinated have (in particular circumstances) gradually changed the vaccine behavior of the Vietnamese [48]. Respondents with the fear of catching the virus (X32) are less likely to be vaccinated if the pandemic becomes more severe. The impact is significant at the five per cent level. This is an unexpected result and future studies would be able to further examine this impact. Kelly and Southwell [20] showed that the impact of this factor was significant, but Khubchandani and Sharma [26] found it insignificant. Respondents with the fear of needles (X33) are more likely to be vaccinated. The impact is at the one per cent level if the pandemic becomes more severe and five per cent level if it becomes less severe. Perhaps the fear of catching the virus dominates that of needles. In addition, laser bubble guns with reasonable prices are expected to be available in the near future and should be able to combat this fear [49].
Despite being concerned about the information sufficiency (X34), side effects (X35) and safety of the vaccines (X38), respondents are still willing to be vaccinated against the virus. The impact is significant at the one and five per cent level, depending on the level of severity and type of concern. Al-Mistarehi and Kheirallah [24] found the impact of the concern about the information sufficiency of the vaccines was significant, but Kawata and Nakabayashi [31], Neumann-Böhme and Varghese [30] and Yoda and Katsuyama [21] found it to be insignificant. There are two possibilities to explain this behavior: the respondents had received sufficient information about the vaccines, or the fear of catching the virus dominates the concerns about insufficient information about the vaccines or the safety of the vaccines. Common reactions after being vaccinated are usually mild. However, severe reactions such as shocks have been observed and the consequences are worse [50,51]. Therefore, it is not surprising that there are several respondents who are concerned about the availability of the response procedure if there is a severe shock after being vaccinated. Sufficient information about the response procedure and the ways to minimize the risks should be available and accessible in multiple languages, including local languages. In addition, the procedure should be available in multiple formats such as video and audio. The regression results show that respondents who are concerned about the response procedure (X36) are less likely to be vaccinated. The impact is significant at the one and five per cent level, depending on the level of severity. Due to the fatality of the Delta variant, people rushed to be vaccinated while the vaccination sites were limited. In addition, due to the vaccine supply, the facilities’ readiness at the site and available nurses, the waiting time at the site may be long. As a result, vaccination sites are normally crowded and people have to wait. The longer the waiting time the higher the risk of catching the virus. Mobile vaccination should be able to cope with this challenge [46]. The results show that respondents who are concerned about the waiting time (X41) are less likely to be vaccinated. The impact is significant at the one per cent level. Al-Mistarehi and Kheirallah [24] also found similar behavior. An unsuitable time frame (X42) to vaccinate or an unsafe vaccination site or waiting room may discourage people from being willing to be vaccinated. The model of mobile vaccination should be sufficiently flexible to deal with this challenge [46]. Despite being concerned about the time frame inconvenience or safety of the vaccination waiting room to vaccinate, respondents are still more likely to be vaccinated if a new variant emerges. The impact is significant at the five per cent level. Knowing common symptoms after being vaccinated can help people prepare to deal with them, hence making them more confident in being vaccinated.
The results show that respondents with sufficient knowledge about common symptoms after getting vaccinated (X44) are more likely to be vaccinated if the number of deaths increases or a new virus variant emerges. The impact is significant at the ten and one per cent level, respectively.
The impact of nationality on the willingness to be vaccinated is significant at the one per cent level for all study countries. In addition, the odds ratio (OR) of respondents who are willing to be vaccinated if the pandemic becomes more severe slightly dominates that of those if it becomes less severe. Additionally, the OR of Indonesian (X46) and Malaysian (X48) respondents who are willing to be vaccinated significantly dominates that of the Vietnamese (X45) and Filipino (X47). The impact of the remaining variables on the willingness to be vaccinated is not statistically significant and can be further examined in future studies.
4. Conclusions
The current study uses data surveyed between August and September 2021 in four ASEAN countries to examine the willingness to be vaccinated against COVID-19 according to the pandemic severity. It also applies logistic regressions to examine the association between the willingness to be vaccinated with the influential factors.
The results show that the number of respondents who are willing to be vaccinated if the pandemic becomes more severe dominates that of those if it becomes less severe. In addition, the number of respondents with more work or family responsibilities who are willing to be vaccinated significantly dominates that of those without or with fewer work or family responsibilities. The number of respondents with protection such as health insurance or savings or assets who are willing to be vaccinated significantly dominates that of those without the protection. The number of respondents with better information access who are willing to be vaccinated significantly dominates that of those without or with poorer information access. The number of respondents who belong to the vaccine priority groups or are living with a person belonging to the vaccine priority groups significantly dominates that of those who do not belong to the groups or are not living with anyone belonging to the groups. In contrast, the number of respondents with comorbidities or the infection significantly dominates that of those without any comorbidity or infection. The number of respondents with the fear (of being infected with the virus, of being discriminated against if not vaccinated or of needles) who are willing to be vaccinated significantly dominates that of those without the fear. In contrast, the number of respondents who are not concerned about the vaccines and relevant matters and are willing to be vaccinated significantly dominates that of those who are.
Results generated from the logistic regressions show that the impact of selected influential factors on the willingness to be vaccinated with different levels of pandemic severity varies in terms of magnitude and direction. The impact of several factors on the willingness to be vaccinated is not significant and can be further examined. Due to resource limitations, the study cannot cover other countries or territories in ASEAN countries where the pandemic may also be severe.
Author Contributions
A.H.D.: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing—original draft and Writing—review & editing. E.A.: Conceptualization, Investigation, and Supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
The Research Ethics Committee of Faculty Medicine Universitas Sebelas Maret after reviewing the research protocol, here with to certify that the research protocol titled: “Willingness to Get Vaccinated against Coronavirus among ASEAN Countries during the COVID-19 Pandemic”. Protocol/ID: 01/03/09/99.
Informed Consent Statement
Ethical clearance for the current study is approved and issued by the Faculty of Medicine, Universitas Sebelas Maret. No: 95/UN27.06.6.1/KEP/EC2021, Protocol/ID: 01/03/09/99. The current study was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from all survey participants and/or their legal guardian(s). In particular, the following statement was placed in the Survey Description: “You do not need to leave personal information. The information you provide will be aggregated and used for research purposes only and will not be shared with any third parties”.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the sensitive nature of the questions asked (especially those on demographic characteristics and personal perceptions), but are available from the corresponding author on reasonable request.
Acknowledgments
The authors would like to thank the respondents who have spared their valuable time to participate in the surveys. The author would like to express their appreciation to Michelle Dela Rosa and Sherry Mariz Rafael for their valuable assistance with data collection in the Philippines. The authors would like to thank the researchers at Sebelas Maret University, Thai Nguyen University of Agriculture and Forestry and Griffith University for their valuable comments.
Conflicts of Interest
The authors declare that they have no known competing financial interest or personal relationships that could have appeared to influence the work reported in this paper.
Abbreviations
X1: age (measured in years), X2: gender (1 = male), X3: residence (1 = urban), X4: marital status (1 = married or cohabitant), X5: family main income source (1 = yes), X6: savings (1 = yes), X7: gold assets (1 = yes), X8: number of dependants (persons), X9: education (1 = tertiary or above, 0 = others), X10: employment (1 = employed), X11: national health insurance member (1 = yes), X12: private health insurance member (1 = yes), X13: information channels to received new on the pandemic (channels), X14: information channels to received new on the vaccines (channels), X15: frequency of receiving new on the pandemic (1 = daily, 0 = others), X16: frequency of receiving new on the vaccines (1 = daily, 0 = others), X17: sufficiency of information on the pandemic (1 = sufficient), X18: sufficiency of information on the vaccines (1 = sufficient), X19: belongs to the vaccine priority groups (1 = yes), X20: living with someone who belongs to the vaccine priority groups (1 = yes), X21: having commodities (1 = yes), X22: knowledge sufficiency of symptoms of COVID-19 infected people (1 = sufficient), X23: knowledge sufficiency of the virus transmission route (1 = sufficient), X24: knowledge sufficiency of ways to prevent the virus (1 = sufficient), X25: knowledge sufficiency on Coronavirus spread speed (1 = sufficient), X26: knowledge sufficiency of Coronavirus fatality (1 = sufficient), X27: knowledge sufficiency on herd immunity if at least 70% of the population is infected (1 = sufficient), X28: knowledge sufficiency of herd immunity if at least 70% of the population is vaccinated (1 = sufficient), X29: ever been infected (1 = yes), X30: having closed one infected (1 = yes), X31: if not vaccinated, afraid of being discriminated against (1 = yes), X32: afraid of catching the virus (1 = yes), X33: afraid of needles (1 = yes), X34: concerned about the official and sufficiency of information on the vaccines (1 = concerned), X35: concerned about the side effects of the vaccines (1 = concerned), X36: concerned about the response procedure if there is a severe shock after being vaccinated (1 = concerned), X37: concerned about the vaccine immunity (1 = concerned), X38: concerned about the vaccine safety (1 = concerned), X39: concerned about the distance between the residence and the vaccination site (1 = concerned), X40: concerned about the vaccine cost (1 = concerned), X41: concerned about the waiting time to vaccinate (1 = concerned), X42: concerned about the time frame to vaccinate (1 = concerned), X43: concerned about the safety of the vaccination waiting room (1 = concerned), X44: knowledge sufficiency of common symptoms after being vaccinated (1 = sufficient), X45: dummy variable representing Vietnamese respondents, X46: dummy variable representing Indonesian respondents, X47: dummy variable representing Filipino respondents, X48: dummy variable representing Malaysian respondents.
References
- WHO. WHO Director-General’s Opening Remarks at The Media Briefing on COVID-19. 2020. [Cited 2021 August]. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 1 July 2021).
- WHO. WHO Coronavirus (COVID-19) Dashboard. 2020. [Cited 2021 July]. Available online: https://covid19.who.int/ (accessed on 1 July 2021).
- Statista. GDP Loss Due to COVID-19, by Economy 2020. 2021. [Cited 2021 August]. Available online: https://www.statista.com/statistics/1240594/gdp-loss-covid-19-economy/ (accessed on 1 August 2021).
- Worldometer. COVID-19 Coronavirus Pandemic. 2021. [Cited 2021 August]. Available online: https://www.worldometers.info/coronavirus/ (accessed on 1 August 2021).
- WHO. COVID-19 Advice for The Public: Getting Vaccinated. 2021. [Cited 2021 July]. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines/advice (accessed on 1 July 2021).
- WHO. Tracking SARS-CoV-2 Variants. 2021. [Cited 2021 July]. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 1 July 2021).
- MoH. 5k Message and Vaccination. 2020; [Cited 2021 July]. Available online: https://vncdc.gov.vn/du-co-vaccine-van-phai-luon-thuc-hien-5k-nd16013.html (accessed on 1 July 2021).
- Our World in Data. Daily New Confirmed COVID-19 Cases per Million People. 2021. [Cited 2021 July]. Available online: https://ourworldindata.org/explorers/coronavirus-data-explorer?zoomToSelection=true&time=2020-04-27..2021-08-27&facet=none&pickerSort=asc&pickerMetric=location&Metric=Confirmed+cases&Interval=7-day+rolling+average&Relative+to+Population=true&Align+outbreaks=false&country=VNM~IDN~PHL~MYS (accessed on 1 July 2021).
- Radjab, S.; Fuady, M.I.N. The Indonesian Government’s inconsistency in handling the Covid-19 pandemic. Yuridika 2021, 36, 745–758. [Google Scholar] [CrossRef]
- Hartanto, D.; Siregar, S.M. Determinants of overall public trust in local government: Meditation of government response to COVID-19 in Indonesian context. Transform. Gov. People Process Policy 2021, 15, 261–274. [Google Scholar] [CrossRef]
- Arifin, W.N.; Musa, K.I.; Hanis, T.M.; Hasani, W.S.R.; Nawi, C.M.N.H.C.; Khan, E.E.A.; Suliman, M.A.; Termizi, S.A.; Aziz, W.A.A. A Brief Analysis of The COVID-19 Death Data in Malaysia. MedRxiv 2021, 10, 1–11. [Google Scholar] [CrossRef]
- Fong, H.X.; Cornish, K.; Kirk, H.; Ilias, K.; Shaikh, M.F.; Golden, K.J. Impact of the COVID-19 lockdown in Malaysia: An examination of the psychological well-being of parent-child dyads and child behaviour in families with children on the autism spectrum. Front. Psychiatry 2021, 12, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Bujang, M.A.; Sa’At, N.; Sidik, T.M.I.T.A.B.; Joo, L.C. Sample size guidelines for logistic regression from observational studies with large population: Emphasis on the accuracy between statistics and parameters based on real life clinical data. Malays. J. Med. Sci. 2018, 25, 122. [Google Scholar] [CrossRef] [PubMed]
- Wooldridge, J. Introductory Econometrics: A Modern Approach, 5th ed.; Cengage Learning: Mason, OH, USA, 2012. [Google Scholar]
- Cerda, A.A.; García, L.Y. Hesitation and Refusal Factors in Individuals’ Decision-Making Processes Regarding a Coronavirus Disease 2019 Vaccination. Front. Public Health 2021, 9, 626852. [Google Scholar] [CrossRef] [PubMed]
- Kessels, R.; Luyten, J.; Tubeuf, S. Willingness To Get Vaccinated Against Covid-19 And Attitudes towards Vaccination in General. Vaccine 2021, 39, 4716–4722. [Google Scholar] [CrossRef]
- Edwards, B.; Biddle, N.; Gray, M.; Sollis, K. COVID-19 vaccine hesitancy and resistance: Correlates in a nationally representative longitudinal survey of the Australian population. PLoS ONE 2021, 16, e0248892. [Google Scholar] [CrossRef]
- Freeman, D.; Loe, B.S.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Jenner, L.; Petit, A.; Lewandowsky, S.; Vanderslott, S.; et al. COVID-19 vaccine hesitancy in the UK: The Oxford coronavirus explanations, attitudes, and narratives survey (Oceans) II. Psychol. Med. 2020, 10, 1–15. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Kelly, B.J.; Southwell, B.G.; McCormack, L.A.; Bann, C.M.; MacDonald, P.D.M.; Frasier, A.M.; Bevc, C.A.; Brewer, N.T.; Squiers, L.B. Predictors of willingness to get a COVID-19 vaccine in the U.S. BMC Infect. Dis. 2021, 21, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Yoda, T.; Katsuyama, H. Willingness To Receive COVID-19 Vaccination in Japan. Vaccines 2021, 9, 48. [Google Scholar] [CrossRef] [PubMed]
- Abedin, M.; Islam, M.A.; Rahman, F.N.; Reza, H.M.; Hossain, M.Z.; Arefin, A.; Hossain, A. Willingness to vaccinate against COVID-19 among Bangladeshi adults: Understanding the strategies to optimize vaccination coverage. PLoS ONE 2021, 16, e0250495. [Google Scholar] [CrossRef] [PubMed]
- Dodd, R.H.; Cvejic, E.; Bonner, C.; Pickles, K.; McCaffery, K.J.; Ayre, J.; Batcup, C.; Copp, T.; Cornell, S.; Dakin, T.; et al. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect. Dis. 2020, 21, 318–319. [Google Scholar] [CrossRef]
- Al-Mistarehi, A.-H.; Kheirallah, K.A.; Yassin, A.; Alomari, S.; Aledrisi, M.K.; Ata, E.M.B.; Hammad, N.H.; Khanfar, A.N.; Ibnian, A.M.; Khassawneh, B.Y. Determinants of the willingness of the general population to get vaccinated against COVID-19 in a developing country. Clin. Exp. Vaccine Res. 2021, 10, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Li, G.M. Hesitancy in the time of coronavirus: Temporal, spatial, and sociodemographic variations in COVID-19 vaccine hesitancy. SSM-Popul. Health 2021, 15, 100896. [Google Scholar] [CrossRef] [PubMed]
- Khubchandani, J.; Sharma, S.; Price, J.H.; Wiblishauser, M.J.; Sharma, M.; Webb, F.J. COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment. J. Community Health 2021, 46, 270–277. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Willingness to Vaccinate Against COVID-19 in the U.S.: Representative Longitudinal Evidence from April to October 2020. Am. J. Prev. Med. 2021, 60, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Kourlaba, G.; Kourkouni, E.; Maistreli, S.; Tsopela, C.-G.; Molocha, N.-M.; Triantafyllou, C.; Koniordou, M.; Kopsidas, I.; Chorianopoulou, E.; Maroudi-Manta, S.; et al. Willingness of Greek general population to get a COVID-19 vaccine. Glob. Health Res. Policy 2021, 6, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.; Cheong, C.; Kong, G.; Phua, K.; Ngiam, J.N.; Tan, B.Y.; Wang, B.; Hao, F.; Tan, W.; Han, X.; et al. An Asia-Pacific study on healthcare workers’ perceptions of, and willingness to receive, the COVID-19 vaccination. Int. J. Infect. Dis. 2021, 106, 52–60. [Google Scholar] [CrossRef]
- Neumann-Böhme, S.; Varghese, N.E.; Sabat, I.; Barros, P.P.; Brouwer, W.; Van Exel, J.; Schreyögg, J.; Stargardt, T. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur. J. Health Econ. 2020, 21, 977–982. [Google Scholar] [CrossRef] [PubMed]
- Kawata, K.; Nakabayashi, M. Determinants of COVID-19 vaccine preference: A survey study in Japan. SSM-Popul. Health 2021, 15, 100902. [Google Scholar] [CrossRef] [PubMed]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Biasio, L.; Bonaccorsi, G.; Lorini, C.; Mazzini, D.; Pecorelli, S. Italian Adults’ Likelihood of Getting COVID-19 Vaccine: A Second Online Survey. Vaccines 2021, 9, 268. [Google Scholar] [CrossRef] [PubMed]
- Khuc, Q.; Nguyen, T.; Nguyen, T.; Pham, L.; Le, D.-T.; Ho, H.-H.; Truong, T.-B.; Tran, Q.-K. Young Adults’ Intentions and Rationales for COVID-19 Vaccination Participation: Evidence from a Student Survey in Ho Chi Minh City, Vietnam. Vaccines 2021, 9, 794. [Google Scholar] [CrossRef]
- VNVC. 11 Vulnerable Groups That Are Prioritized for COVID-19 Vaccination in Vietnam. 2021. [Cited 2021 August]. Available online: https://vnvc.vn/doi-tuong-nao-duoc-uu-tien-tiem-vac-xin-covid-19/ (accessed on 1 August 2021).
- CDC. People with Certain Medical Conditions. 2021; [Cited 2021 July]. Available online: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html (accessed on 1 July 2021).
- Sun, X.; Shi, Y.; Zeng, Q.; Wang, Y.; Du, W.; Wei, N.; Xie, R.; Chang, C. Determinants of health literacy and health behavior regarding infectious respiratory diseases: A pathway model. BMC Public Health 2013, 13, 261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alin, A. Multicollinearity. WIREs Comput. Stat. 2010, 2, 370–374. [Google Scholar] [CrossRef]
- Chong, I.-G.; Jun, C.-H. Performance of some variable selection methods when multicollinearity is present. Chemom. Intell. Lab. Syst. 2005, 78, 103–112. [Google Scholar] [CrossRef]
- Daoud, J.I. Multicollinearity and Regression Analysis. J. Phys. Conf. Ser. 2017, 949, 012009. [Google Scholar] [CrossRef]
- Farrar, D.E.; Glauber, R.R. Multicollinearity in Regression Analysis: The Problem Revisited. Rev. Econ. Stat. 1967, 49, 92. [Google Scholar] [CrossRef]
- Graham, M.H. Confronting multicollinearity in ecological multiple regression. Ecology 2003, 84, 2809–2815. [Google Scholar] [CrossRef] [Green Version]
- Mansfield, E.R.; Helms, B.P. Detecting multicollinearity. Am. Stat. 1982, 36, 158–160. [Google Scholar]
- Schroeder, M.A.; Lander, J.; Levine-Silverman, S. Diagnosing and dealing with multicollinearity. West. J. Nurs. Res. 1990, 12, 175–187. [Google Scholar] [CrossRef] [PubMed]
- Binh, T. Review And Organize Vaccination against COVID-19 for the Elderly And People with Comorbidities at Home; Monitor And Manage F0 Closely. 2021. [Cited 2021 December]. Available online: https://suckhoedoisong.vn/ra-soat-to-chuc-tiem-vaccine-phong-covid-19-cho-nguoi-cao-tuoi-benh-nen-tai-nha-theo-doi-quan-ly-f0-chat-che-169211215192324964.htm (accessed on 1 December 2021).
- CDC. Mobile Vaccination Resources. 2021; [Cited 2021 December]. Available online: https://www.cdc.gov/vaccines/covid-19/planning/mobile.html (accessed on 1 December 2021).
- Tran, T.P.T.; Le, T.H.; Nguyen, T.N.P.; Hoang, V.M. Rapid response to the COVID-19 pandemic: Vietnam government’s experience and preliminary success. J. Glob. Health 2020, 10, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Communist Party of Vietnam. Is There A Penalty for Not Getting The COVID-19 Vaccine? 2021. [Cited 2021 December]. Available online: https://dangcongsan.vn/phong-chong-dich-covid-19/khong-tiem-vaccine-covid-19-co-bi-phat-587083.html (accessed on 1 December 2021).
- World Economic Forum. Needle-Free Injections Could Become a Reality, Thanks to Lasers and the ‘Bubble Gun’. 2021. [Cited 2021 November]. Available online: https://www.weforum.org/agenda/2021/10/new-technology-could-allow-you-to-have-a-needle-free-injection/ (accessed on 1 November 2021).
- BBC. Thanh Hoa: 4 Deaths after Receiving Vero Cell Vaccine. 2001. [Cited 2021 December]. Available online: https://www.bbc.com/vietnamese/59398026 (accessed on 1 December 2021).
- BBC. Thanh Hoa: 86 Students Were Hospitalized after Receiving Pfizer Vaccine. 2021. [Cited December]. Available online: https://www.bbc.com/vietnamese/vietnam-59404925 (accessed on 1 December 2021).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).