

Parental Perceptions and Barriers towards Childhood COVID-19 Vaccination in Saudi Arabia: A Cross-Sectional Analysis

 ,
,  ,
, 
 ,
,  , and
, and
Abstract
1. Introduction
2. Methodology
2.1. Ethical Approval
2.2. Study Design, Setting and Population
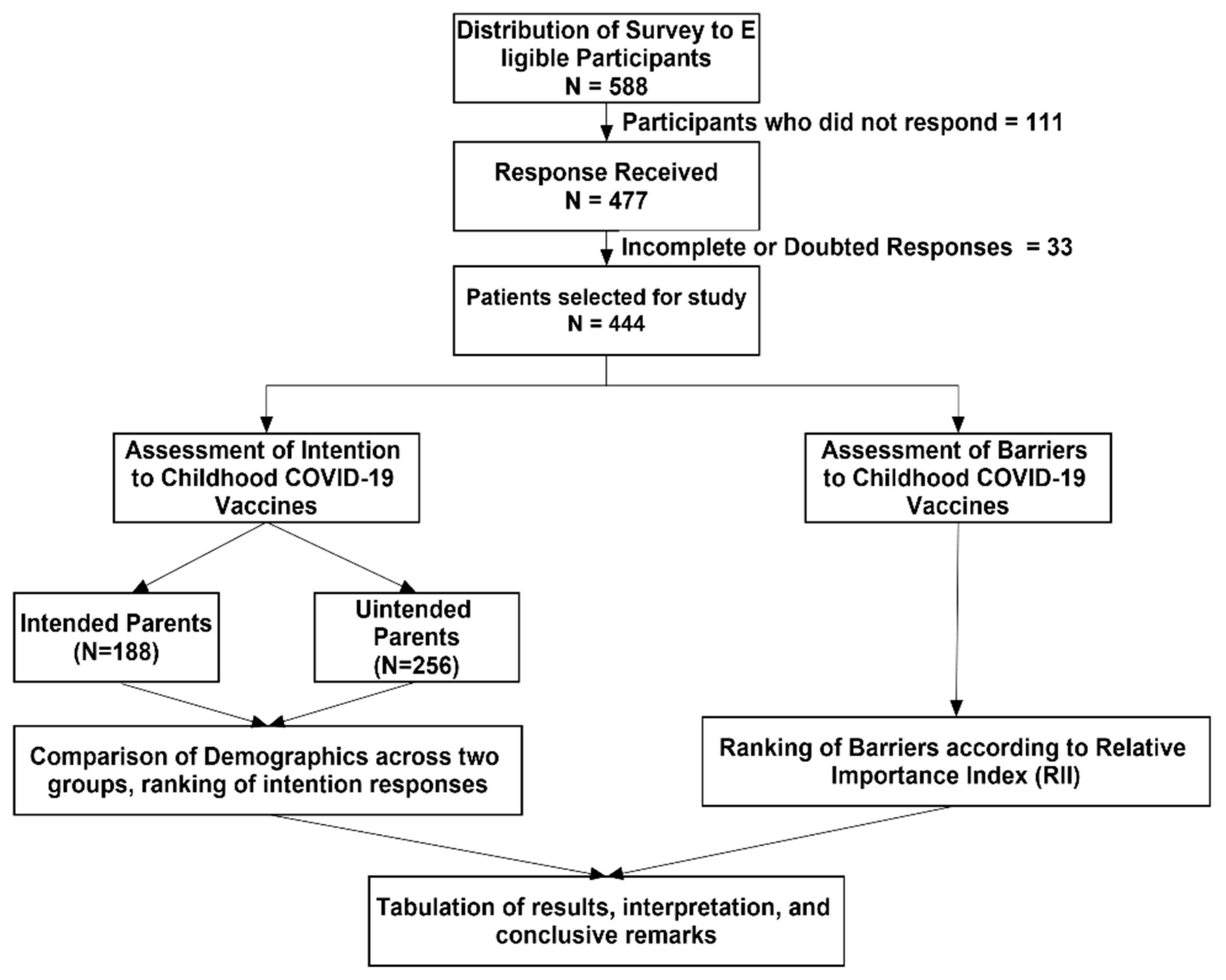
2.3. Sampling Technique and Sample Size Calcuation
2.4. Development and Validation of the Study Instrument
- Section I consisted of 9 items related to demographics. Apart from basic demographic questions, the participants were asked about their COVID-19 vaccination status and whether their child had received any seasonal influenza vaccine in the past 2 years. The participants were told to answer these questions by keeping the youngest child in mind.
- Section II consisted of 6 items assessing the participants’ intentions to vaccinate their child with the COVID-19 vaccine. The responses were recorded on a 5-point Likert Scale (very likely, somewhat likely, unsure, somewhat unlikely, very unlikely). For further analysis, these responses were collapsed and recoded with the values for very likely and likely coded as “1”, and the values for very unlikely, unlikely and unsure coded as “0”. However, reverse coding was used for Item 6. The maximum intention score was 6. The mean intention score was estimated. The percentage of agreement was calculated for the participants who agreed to the statements. These statements were ranked accordingly.
- Section III assessed the barriers to childhood COVID-19 vaccination. This section contained 7 items measuring the barriers on a 5-point Likert (strongly agree to strongly disagree).
2.5. Data Collection
2.6. Statistical Analysis
3. Results
3.1. Analysis of Items on Parents’ Intention towards the Childhood COVID-19 Vaccination
3.2. Potential Barriers Associated with the Uptake of the Childhood COVID-19 Vaccination
3.3. Factors Associated with Intention to Childhood COVID-19 Vaccination
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. WHO Corona Virus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 17 November 2022).
- Center for Disease Control and Prevention. Stay Up to Date with COVID-19 Vaccines Including Boosters: COVID-19 Vaccines for Children and Teens. 2022. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/adolescents.html (accessed on 27 September 2022).
- Tang, Y.; Li, W.; Baskota, M.; Zhou, Q.; Fu, Z.; Luo, Z.; Shi, Y.; Chen, Y.; Liu, E. Multisystem inflammatory syndrome in children during the coronavirus disease 2019 (COVID-19) pandemic: A systematic review of published case studies. Transl. Pediatr. 2021, 10, 121–135. [Google Scholar] [CrossRef]
- Velavan, T.P.; Pollard, A.J.; Kremsner, P.G. Herd immunity and vaccination of children for COVID-19. Int. J. Infect. Dis. 2020, 98, 14–15. [Google Scholar] [CrossRef]
- World Health Organization. Interim Statement on COVID-19 Vaccination for Children. 11 August 2022. Available online: https://www.who.int/news/item/11-08-2022-interim-statement-on-COVID-19-vaccination-for-children (accessed on 4 August 2022).
- Lv, M.; Luo, X.; Shen, Q.; Lei, R.; Liu, X.; Liu, E.; Li, Q.; Chen, Y. Safety, immunogenicity, and efficacy of COVID-19 vaccines in children and adolescents: A systematic review. Vaccines 2021, 9, 1102. [Google Scholar] [CrossRef]
- Al-Hanawi, M.K.; Keetile, M.; Kadasah, N.A.; Alshareef, N.; Qattan, A.M.N.; Alsharqi, O. Side Effects and Perceptions of COVID-19 Vaccination in Saudi Arabia: A Cross-Sectional Study. Front. Med. 2022, 9, 899517. [Google Scholar] [CrossRef]
- Ganesan, S.; Al Ketbi, L.M.B.; Al Kaabi, N.; Al Mansoori, M.; Al Maskari, N.N.; Al Shamsi, M.S.; Alderei, A.S.; El Eissaee, H.N.; Al Ketbi, A.F.; Al Shamsi, N.S.; et al. Vaccine Side Effects Following COVID-19 Vaccination Among the Residents of the UAE—An Observational Study. Front. Public Health 2022, 10, 876336. [Google Scholar] [CrossRef]
- Zahid, M.N. Unfolding the mild to moderate short-term side effects of four COVID-19 vaccines used in Bahrain: A cross-sectional study. Vaccines 2021, 9, 1369. [Google Scholar] [CrossRef]
- Chin, S.E.; Bhavsar, S.M.; Corson, A.; Ghersin, Z.J.; Kim, H.S. Cardiac Complications Associated with COVID-19, MIS-C, and mRNA COVID-19 Vaccination. Pediatr. Cardiol. 2022, 43, 483–488. [Google Scholar] [CrossRef]
- Oster, M.E.; Shay, D.K.; Su, J.R.; Gee, J.; Creech, C.B.; Broder, K.R.; Edwards, K.; Soslow, J.H.; Dendy, J.M.; Schlaudecker, E.; et al. Myocarditis cases reported after mRNA-based COVID-19 vaccination in the US from December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Alyami, M.H.; Naser, A.Y.; Orabi, M.A.A.; Alwafi, H.; Alyami, H.S. Epidemiology of COVID-19 in the Kingdom of Saudi Arabia: An ecological study. Front. Public Health 2020, 8, 506. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Coronavirus disease 2019 in children—United States, 12 February–2 April 2020. MMWR Morb. Mortal Wkly. Rep. 2020, 69, 422–426. [Google Scholar] [CrossRef]
- Zimmermann, P.; Curtis, N. Coronavirus infections in children including COVID-19: An overview of the epidemiology, clinical features, diagnosis, treatment and prevention options in children. Pediatr. Infect. Dis. J. 2020, 39, 355–368. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 7 July 2022).
- Al-Shehri, S.N.; Al-Shammari, S.A.; Khoja, T.A. Missed opportunities for immunization: A Saudi Arabia survey. Can. Fam. Physician 1992, 38, 1087. [Google Scholar] [PubMed]
- Aldakhil, H.; Albedah, N.; Alturaiki, N.; Alajlan, R.; Abusalih, H. Vaccine hesitancy towards childhood immunizations as a predictor of mothers’ intention to vaccinate their children against COVID-19 in Saudi Arabia. J. Infect. Public Health 2021, 14, 1497–1504. [Google Scholar] [CrossRef]
- Alsubaie, S.S.; Gosadi, I.M.; Alsaadi, B.M.; Albacker, N.B.; Bawazir, M.A.; Bin-Daud, N.; Almanie, W.B.; Alsaadi, M.A.; Alzamil, F.A. Vaccine hesitancy among Saudi parents and its determinants: Result from the WHO SAGE working group on vaccine hesitancy survey tool. Saudi Med. J. 2019, 40, 1242. [Google Scholar] [CrossRef] [PubMed]
- Yousif, M.; Albarraq, A.A.; Abdallah, M.A.A.; Elbur, A.I. Parents’ knowledge and attitudes on childhood immunization, Taif, Saudi Arabia. J. Vaccines Vaccin. 2013, 5, 2. [Google Scholar]
- Alrowaili, G.Z.R.; Dar, U.F.; Bandy, A.H. May we improve vaccine timeliness among children? A cross sectional survey in northern Saudi Arabia. J. Fam. Commun. Med. 2019, 26, 113. [Google Scholar]
- Ministry of Health Saudi Arabia. COVID-19 Statistics. 2022. Available online: https://covid19.moh.gov.sa/ (accessed on 18 November 2022).
- World Health Organization. WHO Corona Virus (COVID-19) Dashboard—Saudi Arabia. Available online: https://covid19.who.int/region/emro/country/sa (accessed on 15 November 2022).
- Ministry of Health Saudi Arabia. COVID-19 Vaccines. Available online: https://covid19awareness.sa/en/archives/10691 (accessed on 3 November 2022).
- Assiri, A.; Al-Tawfiq, J.A.; Alkhalifa, M.; Al Duhailan, H.; Al Qahtani, S.; Dawas, R.A.; El Seoudi, A.A.; Alomran, N.; Omar, O.A.; Alotaibi, N.; et al. Launching COVID-19 vaccination in Saudi Arabia: Lessons learned, and the way forward. Travel Med. Infect. Dis. 2021, 43, 102119. [Google Scholar] [CrossRef]
- Ministry of Health Saudi Arabia. MOH Starts Registering Citizens and Residents for COVID-19 Vaccination. 2020. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2020-12-15-006.aspx (accessed on 19 November 2022).
- Ministry of Health Saudi Arabia. MOH: Downward Trend Observed in COVID-19 Curve, Adherence to Precautionary Measures Remains Essential. 2021. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-05-16-001.aspx (accessed on 7 November 2022).
- Ministry of Health Saudi Arabia. MOH Launches «Maintain Your Level with Booster Shot» Campaign. 2021. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-12-19-004.aspx (accessed on 8 November 2022).
- Saudi Arabia Gazzette Report. 4th COVID-19 Dose Available to Those under 50 Suffering from Immunodeficiency. In Saudi Gazzette; Saudi Gazzette: Jeddah, Saudi Arabia, 2022; Available online: https://saudigazette.com.sa/article/620305/SAUDI-ARABIA/4th-COVID-19-dose-available-to-those-under-50-suffering-from-immunodeficiency (accessed on 18 November 2022).
- Ministry of Health Saudi Arabia. MOH Begins Vaccinating 12–18 Age Group with Pfizer Vaccine. 2021. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-06-27-008.aspx (accessed on 18 November 2022).
- Ministry of Health Saudi Arabia. MOH Urges Students to Take 2 COVID-19 Vaccine Doses Before Returning to Next School Year. 2021. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2021-08-02-007.aspx (accessed on 19 November 2022).
- Saudi Arabia Gazzette Report. Saudi Arabia Starts Giving COVID-19 Vaccines to Children Aged 5–11. 2021. Available online: https://saudigazette.com.sa/article/614992 (accessed on 8 November 2022).
- Ministry of Health Saudi Arabia. MOH: First Dose of COVID-19 Vaccine is Available for Children Aged 5–11 Years. 2022. Available online: https://www.moh.gov.sa/en/Ministry/MediaCenter/News/Pages/News-2022-01-16-002.aspx (accessed on 19 November 2022).
- Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Hatmal, M.; Alhaj-Qasem, D.M.; Olaimat, T.M.; Mohamud, R. Side effects and perceptions following COVID-19 vaccination in Jordan: A randomized, cross-sectional study implementing machine learning for predicting severity of side effects. Vaccines 2021, 9, 556. [Google Scholar] [CrossRef]
- Almalki, O.S.; Alfayez, O.M.; Al Yami, M.S.; Asiri, Y.A.; Almohammad, O.A. Parents’ Hesitancy to Vaccinate Their 5-11-Year-Old Children Against COVID-19 in Saudi Arabia: Predictors From the Health Belief Model. Front. Public Health 2022, 10, 842862. [Google Scholar] [CrossRef]
- General Authority of Statistics Saudi Arabia. Saudi Youth in Numbers. 2020. Available online: https://www.stats.gov.sa/sites/default/files/saudi_youth_in_numbers_report_2020en.pdf (accessed on 17 November 2022).
- Galanis, P.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Katsiroumpa, A.; Kaitelidou, D. Willingness, refusal and influential factors of parents to vaccinate their children against the COVID-19: A systematic review and meta-analysis. Prev. Med. 2022, 157, 106994. [Google Scholar] [CrossRef]
- Altulaihi, B.A.; Alaboodi, T.; Alharbi, K.G.; Alajmi, M.S.; Alkanhal, H.; Alshehri, A. Perception of parents towards COVID-19 vaccine for children in Saudi population. Cureus 2021, 13, e18342. [Google Scholar] [CrossRef] [PubMed]
- Almusbah, Z.; Alhajji, Z.; Alshayeb, Z.; Alhabdan, R.; Alghafli, S.; Almusabah, M.; Almuqarrab, F.; Aljazeeri, I.; Almuhawas, F. Caregivers’ willingness to vaccinate their children against COVID-19 in Saudi Arabia: A cross-sectional survey. Cureus 2021, 13, e17243. [Google Scholar] [CrossRef]
- Temsah, M.-H.; Alhuzaimi, A.N.; Aljamaan, F.; Bahkali, F.; Al-Eyadhy, A.; Alrabiaah, A.; Alhaboob, A.; Bashiri, F.A.; Alshaer, A.; Temsah, O.; et al. Parental attitudes and hesitancy about COVID-19 vs. routine childhood vaccinations: A national survey. Front. Public Health 2021, 9, 752323. [Google Scholar] [CrossRef] [PubMed]
- Al Naam, Y.A.; Elsafi, S.H.; Alkharraz, Z.S.; Almaqati, T.N.; Alomar, A.M.; Al Balawi, I.A.; Jebakumar, A.Z.; Ghazwani, A.A.; Almusabi, S.S.; Albusaili, S.; et al. Factors Related to COVID-19 Vaccine Hesitancy in Saudi Arabia. Public Health Pract. 2022, 3, 100258. [Google Scholar] [CrossRef]
- Al-Mohaithef, M.; Padhi, B.K.; Ennaceur, S. Socio-demographics correlate of COVID-19 vaccine hesitancy during the second wave of COVID-19 pandemic: A cross-sectional web-based survey in Saudi Arabia. Front. Public Health 2021, 794, 698106. [Google Scholar] [CrossRef] [PubMed]
- Ennaceur, S.; Al-Mohaithef, M. Parents’ Willingness to Vaccinate Children against COVID-19 in Saudi Arabia: A Cross-Sectional Study. Vaccines 2022, 10, 156. [Google Scholar] [CrossRef]
- Choi, U.; Pang, Y.; Zheng, Y.; Tang, P.K.; Hu, H.; Ung, C.O.L. Parents’ intention for their children to receive COVID-19 vaccine: Implications for vaccination program in Macao. Front. Pediatr. 2022, 10, 978661. [Google Scholar] [CrossRef]
- Mangat, C.; Rich, J.; Sanghavi, D.; Schmidt, R.; Milosavljrvic, N.; Linh, T.; Bansal, P. Parents’ perspective on COVID-19 vaccine in children 6 months through 4 years: A cross-sectional study from Northwest Wisconsin. BMJ Open 2022, 12, e065453. [Google Scholar] [CrossRef]
- Almansour, A.; Hussein, S.M.; Felemban, S.G.; Mahamid, A.W. Acceptance and hesitancy of parents to vaccinate children against coronavirus disease 2019 in Saudi Arabia. PLoS ONE 2022, 17, e0276183. [Google Scholar] [CrossRef]
- Sallam, M.; Al-Sanafi, M.; Sallam, M. A global map of COVID-19 vaccine acceptance rates per country: An updated concise narrative review. J. Multidiscip. Healthc. 2022, 15, 21. [Google Scholar] [CrossRef]
- Siegler, A.J.; Luisi, N.; Wall, E.H. Trajectory of COVID-19 vaccine hesitancy over time and association of initial vaccine hesitancy with subsequent vaccination. JAMA Netw. Open 2021, 4, e2126882. [Google Scholar] [CrossRef] [PubMed]
- Aedh, A.I. Parents’ Attitudes, Their Acceptance of the COVID-19 Vaccines for Children and the Contributing Factors in Najran, Saudi Arabia: A Cross-Sectional Survey. Vaccines 2022, 10, 1264. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. 2007, 26, 136. [Google Scholar] [CrossRef] [PubMed]
- Hasanain, F.H.; Jan, M.M. Delays in primary vaccination of infants living in Western Saudi Arabia. Saudi Med. J. 2002, 23, 1087–1089. [Google Scholar]
- Zeballos Rivas, D.R.; Jaldin, M.L.L.; Canaviri, B.N.; Escalante, L.F.P.; Fernández, A.M.C.A.; Ticona, J.P.A. Social media exposure, risk perception, preventive behaviors and attitudes during the COVID-19 epidemic in La Paz, Bolivia: A cross sectional study. PLoS ONE 2021, 16, e0245859. [Google Scholar] [CrossRef] [PubMed]
- Moran, K.R.; del Valle, S.Y. A meta-analysis of the association between gender and protective behaviors in response to respiratory epidemics and pandemics. PLoS ONE 2016, 11, e0164541. [Google Scholar] [CrossRef]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef]
- Kaufman, J.; Tuckerman, J.; Bonner, C.; Durrheim, D.N.; Costa, D.; Trevena, L.; Thomas, S.; Danchin, M. Parent-level barriers to uptake of childhood vaccination: A global overview of systematic reviews. BMJ Glob. Health 2021, 6, e006860. [Google Scholar] [CrossRef]
- Eysenbach, G. Improving the quality of Web surveys: The Checklist for Reporting Results of Internet E-Surveys (CHERRIES). J. Med. Internet Res. 2004, 6, e132. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographic Variable | Total Participants (n = 444) | Intending * (n = 188) | Non-Intending ** (n = 256) | p-Value |
|---|---|---|---|---|
| Age (Mean ± SD); Years | 28.41 ± 7.4 | 28.55 ± 7.6 | 28.30 ± 7.2 | 0.734 |
| Gender | ||||
| Male | 155 (34.9%) | 56 (29.8%) | 99 (38.7%) | 0.052 |
| Female | 289 (65.1%) | 132 (70.2%) | 157 (61.3%) | |
| Marital status | ||||
| Married | 292 (65.8%) | 128 (68.1%) | 164 (64.1%) | 0.524 |
| Divorced | 79 (17.8%) | 29 (15.4%) | 50 (19.5%) | |
| Separated | 73 (16.4%) | 31 (16.5%) | 42 (16.4%) | |
| Educational level | ||||
| Preparatory | 38 (8.6%) | 6 (3.2%) | 32 (12.5%) | 0.001 |
| Secondary | 197 (44.3%) | 80 (42.6%) | 117 (45.7%) | |
| University | 209 (47.1%) | 102 (54.2%) | 107 (41.8%) | |
| Profession | ||||
| Healthcare | 93 (20.9%) | 27 (14.4%) | 66 (25.8) | 0.003 |
| Non-healthcare | 351 (79.1%) | 161 (85.6%) | 190 (74.2%) | |
| Received the COVID-19 vaccination | ||||
| Yes | 402 (90.5%) | 185 (98.4%) | 217 (84.8) | <0.001 |
| No | 42 (9.5%) | 3 (1.6%) | 39 (15.2%) | |
| Child received an influenza vaccination in the past year | ||||
| Yes | 182 (41.0%) | 86 (45.7%) | 96 (37.5%) | 0.081 |
| No | 262 (59.0%) | 102 (54.3%) | 160 (62.5%) | |
| Who makes the healthcare decisions for the children | ||||
| Father | 84 (18.9%) | 20 (10.6%) | 64 (25.0%) | <0.001 |
| Mother | 110 (24.8%) | 55 (29.3%) | 55 (21.5%) | |
| Both | 250 (56.3%) | 113 (60.1%) | 137 (53.5%) |
| Statement | Very Likely n (%) | Somewhat Likely n (%) | Unsure n (%) | Somewhat Unlikely n (%) | Very Unlikely n (%) | RII * | Rank £ | % Agreement € |
|---|---|---|---|---|---|---|---|---|
| I plan to have my child vaccinated against COVID-19. | 68 (15.3) | 95 (21.4) | 42 (9.5) | 108 (24.3) | 131 (29.5) | 0.485 | 6 | 163 (36.7%) |
| I plan to have my child vaccinated as soon as a vaccine is available for children. | 7 (1.6) | 87 (19.6) | 130 (29.3) | 189 (42.6) | 31 (7) | 0.532 | 5 | 94 (21.2%) |
| I plan to have my child vaccinated but I will wait for some time and see how other children respond to the COVID-19 vaccine. | 147 (33.1) | 169 (38.1) | 45 (10.1) | 24 (5.4) | 59 (13.3) | 0.745 | 2 | 316 (71.2%) |
| I will vaccinate my children if it is made compulsory for schools, daycare, restaurants and malls by the government. | 183 (41.2) | 144 (32.4) | 22 (5) | 36 (8.1) | 59 (13.3) | 0.760 | 1 | 327 (73.6%) |
| I will vaccinate my children if their doctor/healthcare provider recommends it. | 173 (38.9) | 120 (27) | 39 (8.8) | 46 (10.4) | 66 (14.9) | 0.730 | 3 | 293 (66%) |
| I do not plan to vaccinate my children. | 95 (21.4) | 97 (21.8) | 114 (25.7) | 56 (12.6) | 82 (18.5) | 0.630 | 4 | 192 (432%) |
| Statement | Strongly Agree | Agree | Neutral | Strongly Disagree | Disagree | RII * | Rank £ | % Agreement € |
|---|---|---|---|---|---|---|---|---|
| Lack of scientific data regarding the vaccine’s efficacy for children. | 132 (29.7) | 143 (32.2) | 77 (17.3) | 78 (17.6) | 14 (3.2) | 0.736 | 2 | 275 (61.9%) |
| Concerns about the vaccine’s safety/side effects. | 154 (34.7) | 136 (30.6) | 70 (15.8) | 67 (15.1) | 17 (3.8) | 0.754 | 1 | 290 (65.3%) |
| The availability of too many vaccines makes it difficult to choose the best vaccine for children. | 82 (18.5) | 133 (30) | 82 (18.5) | 99 (22.3) | 48 (10.8) | 0.646 | 3 | 215 (48.4%) |
| Religious beliefs about avoiding the vaccine. | 38 (8.6) | 68 (15.3) | 135 (30.4) | 134 (30.2) | 69 (15.5) | 0.542 | 7 | 106 (23.9%) |
| Family/peer pressure to avoid the vaccine. | 60 (13.5) | 100 (22.5) | 89 (20.1) | 134 (30.2) | 61 (13.7) | 0.584 | 6 | 160 (36%) |
| Children are not at risk of COVID-19 complications. | 99 (22.3) | 84 (18.9) | 81 (18.2) | 127 (28.7) | 53 (11.9) | 0.622 | 5 | 183 (41.2%) |
| Wearing masks, using sanitizers and practicing social distancing are enough to protect children. | 60 (13.5) | 147 (33.1) | 78 (17.6) | 102 (23) | 57 (12.8) | 0.623 | 4 | 207 (46.6%) |
| Covariates | Univariate Analysis | p-Value | Multivariate Analysis | p-Value |
|---|---|---|---|---|
| COR (95% CI) | AOR (95% CI) | |||
| Age | 1.004 (0.979–1.030) | 0.733 | ||
| Gender | ||||
| Male | 1.00 (Ref.) | |||
| Female | 1.486 (0.995–2.220) | 0.053 | ||
| Marital status | ||||
| Married | 1.00 (Ref.) | |||
| Divorced/separated | 0.836 (0.561–1.245) | 0.378 | ||
| Educational level | ||||
| Preparatory | 1.00 (Ref.) | 1.00 (Ref.) | -- | |
| Secondary | 5.084 (2.040–12.670) | <0.001 | 3.617 (1.353–9.672) | 0.010 |
| University | 3.647 (1.457–9.125) | 0.006 | 2.775 (1.037–7.429) | 0.042 |
| Profession | ||||
| Healthcare | 1.00 (Ref.) | 1.00 (Ref.) | ||
| Non-healthcare | 2.071 (1.263–3.396) | 0.004 | 1.390 (0.783–2.468) | 0.261 |
| Received the COVID-19 vaccination | ||||
| No | 1.00 (Ref.) | 1.00 (Ref.) | -- | |
| Yes | 11.083 (3.370–36.451) | <0.001 | 7.062 (1.919–25.991) | 0.003 |
| Child received the influenza vaccination in the past year | ||||
| No | 1.00 (Ref.) | |||
| Yes | 1.405 (0.959–2.060) | 0.081 | ||
| Who makes the healthcare decision for the children? | ||||
| Father | 1.00 (Ref.) | 1.00 (Ref.) | -- | |
| Mother | 3.200 (1.711–5.984) | <0.001 | 4.353 (2.164–8.756) | <0.001 |
| Both mother and father (mutual) | 2.639 (1.507–4.623) | 0.001 | 3.195 (1.696–6.028) | <0.001 |
| Lack of scientific data regarding the vaccine’s efficacy for children | ||||
| Yes | 1.00 (Ref.) | 1.00 (Ref.) | ||
| No | 2.593 (1.619–4.152) | <0.001 | 1.608 (0.793–3.260) | 0.188 |
| Concerns about the vaccine’s safety in children | ||||
| Yes | 1.00 (Ref.) | 1.00 (Ref.) | ||
| No | 3.036 (1.851–4.979) | <0.001 | 2.483 (1.143–5.392) | 0.022 |
| The availability of too many vaccines makes it difficult to decide which one is better for children | ||||
| Yes | 1.00 (Ref.) | |||
| No | 0.837 (0.560–1.252) | 0.387 | ||
| Religious beliefs against vaccination | ||||
| Yes | 1.00 (Ref.) | |||
| No | 1.453 (0.995–2.122) | 0.053 | ||
| Family/peer pressure to avoid childhood COVID-19 vaccination | ||||
| Yes | 1.00 (Ref.) | 1.00 (Ref.) | ||
| No | 1.719 (1.174–2.516) | 0.005 | 0.983 (0.559–1.726) | 0.952 |
| Belief that children are not at risk of COVID-19 | ||||
| Yes | 1.00 (Ref.) | 1.00 (Ref.) | ||
| No | 1.510 (1.029–2.215) | 0.035 | 0.690 (0.375–1.271) | 0.234 |
| Wearing masks, using sanitizers and practicing social distancing are enough to protect children | ||||
| Yes | 1.00 (Ref.) | 1.00 (Ref.) | ||
| No | 1.660 (1.121–2.457) | 0.011 | 1.012 (0.551–1.860) | 0.969 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khan, Y.H.; Mallhi, T.H.; Salman, M.; Tanveer, N.; Butt, M.H.; Mustafa, Z.U.; Aftab, R.A.; Alanazi, A.S. Parental Perceptions and Barriers towards Childhood COVID-19 Vaccination in Saudi Arabia: A Cross-Sectional Analysis. Vaccines 2022, 10, 2093. https://doi.org/10.3390/vaccines10122093
Khan YH, Mallhi TH, Salman M, Tanveer N, Butt MH, Mustafa ZU, Aftab RA, Alanazi AS. Parental Perceptions and Barriers towards Childhood COVID-19 Vaccination in Saudi Arabia: A Cross-Sectional Analysis. Vaccines. 2022; 10(12):2093. https://doi.org/10.3390/vaccines10122093
Chicago/Turabian StyleKhan, Yusra Habib, Tauqeer Hussain Mallhi, Muhammad Salman, Nida Tanveer, Muhammad Hammad Butt, Zia Ul Mustafa, Raja Ahsan Aftab, and Abdullah Salah Alanazi. 2022. "Parental Perceptions and Barriers towards Childhood COVID-19 Vaccination in Saudi Arabia: A Cross-Sectional Analysis" Vaccines 10, no. 12: 2093. https://doi.org/10.3390/vaccines10122093
APA StyleKhan, Y. H., Mallhi, T. H., Salman, M., Tanveer, N., Butt, M. H., Mustafa, Z. U., Aftab, R. A., & Alanazi, A. S. (2022). Parental Perceptions and Barriers towards Childhood COVID-19 Vaccination in Saudi Arabia: A Cross-Sectional Analysis. Vaccines, 10(12), 2093. https://doi.org/10.3390/vaccines10122093