Abstract
Obstructive sleep apnoea (OSA) is characterized by overproduction of reactive oxygen species and oxidative stress. The antioxidant enzyme paraoxonase-1 (PON-1) may be useful for monitoring the antioxidant defence systems and the effect of treatments in OSA patients. We investigated, by means of systematic review and meta-analysis, the serum concentrations of PON-1 in OSA patients and non-OSA controls. A literature search was conducted in PubMed, Web of Science, Scopus and Google Scholar databases, from the outset to November 2021, utilizing the terms: “paraoxonase” or “PON” or “paraoxonase-1” or “PON-1” and “obstructive sleep apnoea syndrome” or “OSAS” or “OSA”. Eleven studies in 429 OSA patients and 258 non-OSA controls were involved in the meta-analysis. The pooled serum PON-1 concentrations were significantly lower in OSA (standardized mean difference (SMD) = −0.70, 95% CI −1.13 to −0.28; p = 0.001). Despite the extreme between-study heterogeneity, the SMD values were not substantially affected by the sequential omission of individual studies. There was no publication bias. Our systematic review and meta-analysis supports the presence of an impaired antioxidant defence system in OSA, possibly the consequence of intermittent hypoxia. Further studies are required to determine the clinical use of PON-1 measurements for risk stratification and monitoring in OSA patients.
1. Introduction
Obstructive sleep apnoea (OSA) is a respiratory disorder that occurs with recurrent episodes of upper airway blockage during sleep [1]. These events are associated with oxyhemoglobin desaturations and are considered equivalent to hypoxia-reperfusion injury, a condition that enhances reactive oxygen species (ROS) production and inflammatory response [2]. OSA is known to be associated with obesity, hyperglycaemia and dyslipidaemia, and is an independent risk factor for atherosclerotic cardiovascular disease [3].
It has been proposed the over-production of ROS and the impairment in antioxidant defence systems might account for the development and the progression of atherosclerosis in OSA [4]. There are various known antioxidant molecules which play a defensive role against excess oxidative stress in different diseases [5,6]. Paraoxonases (PON) are a family of enzymes that protect against oxidative damage and lipid peroxidation, modulating the susceptibility of high-density cholesterol lipoprotein (HDL) to atherogenic modifications [7,8]. The (PON) family includes PON-1, PON-2 and PON-3. PON-1 and PON-3 bind to circulating HDL, while PON-2 is located intracellularly [9]. PON-1 and its isoforms, the most studied, are involved in the prevention of cardiovascular and neurodegenerative diseases [10,11,12]. Alterations of PON-1 activity have been reported in various inflammatory and oxidative stress-related diseases, e.g., type 2 diabetes, chronic obstructive pulmonary disease and sleep disorders [13,14,15]. However, conflicting results have been reported regarding the association between PON-1 and OSA [16,17]. We sought to address this issue by critically appraising, by means of systematic review and meta-analysis, studies investigating serum PON-1 concentrations in OSA patients and non-OSA controls.
2. Materials and Methods
2.1. Search Strategy, Eligibility Criteria and Study Selection
A systematic literature search of publications in the databases PubMed, Web of Science, Scopus and Google Scholar, from the outset to November 2021, was conducted using the terms “paraoxonase” or “PON” or “paraoxonase-1” or “PON-1” and “obstructive sleep apnoea syndrome” or “OSAS” or “OSA”, and their combination. The abstracts were independently examined by two investigators, who revised only the relevant complete articles. Eligibility criteria were: (i) Evaluation of PON-1 activity in plasma or serum; (ii) comparison between patients with OSA and non-OSA subjects (case–control design); (iii) sample size ≥10 OSA patients; (iv) English language; and (v) the presence of full text. To identify additional studies, the references of the recovered articles were also examined. The presence of any disagreement between reviewers was resolved involving a third investigator.
The Joanna Briggs Institute (JBI) Critical Appraisal Checklist for analytical studies was utilized to assess the risk of bias. A score of ≥5, 4 and <4 indicated low, moderate and high risk, respectively [18]. The Grades of Recommendation, Assessment, Development and Evaluation (GRADE) Working Group system was used to evaluate the certainty of evidence. GRADE considers the study design (randomized vs. observational), the existence of unexplained heterogeneity, the risk of bias (JBI checklist), the indirectness of evidence, the presence of imprecise results (sample size, 95% confidence interval width and threshold crossing), the effect size (standardized mean difference (SMD) < 0.5, small; SMD 0.5–0.8, moderate; and SMD > 0.8, large) [19] and the probability of publication bias [20,21]. The study fully conforms with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 assertion [22]. The protocol was approved by the International Prospective Register of Systematic Reviews (PROSPERO CRD42022298912).
2.2. Statistical Analysis
In order to build forest plots of continuous data and evaluate differences in PON-1 concentrations between OSA and non-OSA subjects, standardized mean differences (SMDs) and 95% confidence intervals (CIs) were used (significance level at p < 0.05). When necessary, means and standard deviations were extrapolated from medians and interquartile ranges [23] or from graphs using the Graph Data Extractor software.
The Q statistic (significance level at p < 0.10) and the I2 statistic (I2 < 25%, no heterogeneity; I2 between 25% and 50%, moderate heterogeneity; I2 between 50% and 75%, large heterogeneity; and I2 > 75%, extreme heterogeneity) were performed to measure heterogeneity of SMD values across studies [24,25]. In the case of presence of high heterogeneity, defined as I2 ≥ 50%, a random-effects model was used [25].
In order to investigate the influence of each study on the overall risk estimate, an analysis of sensitivity was performed [26].
The Begg’s adjusted rank correlation test and Egger’s regression asymmetry test (significance level at p < 0.05 for both) were used to evaluate the presence of publication bias, the associations between study size and magnitude of effect [27,28]. The Duval and Tweedie “trim and fill” method was also performed to test for, and eventually correct, publication bias [29]. Univariate meta-regression analyses were conducted to investigate relations between effect size and the following parameters: Age, percentage of males, body mass index (BMI), total cholesterol, LDL-cholesterol, HDL-cholesterol, triglycerides, apnoea hypopnea index (AHI), sample size and publication year. Statistical analyses were performed using Stata 14 (STATA Corp., College Station, TX, USA).
3. Results
3.1. Systematic Research and Study Characteristics
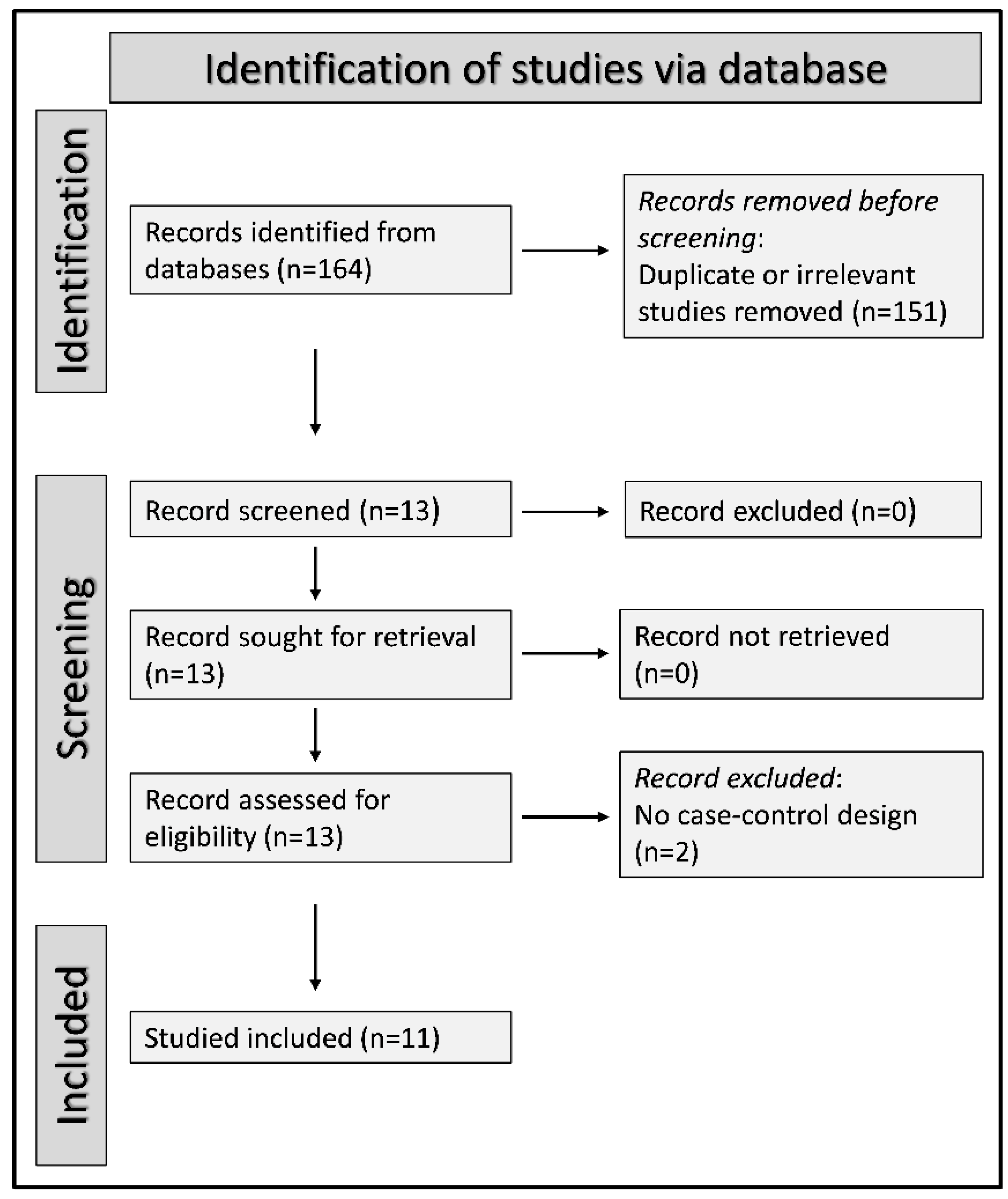
Initially, 164 potentially relevant studies were identified. After the first screening, 151 out of 164 were excluded because they were either duplicates or inappropriate. Among the remaining 13 articles, two were further excluded because they did not accomplish the inclusion criteria. Therefore, a total of 11 studies were enclosed in the meta-analysis [15,16,30,31,32,33,34,35,36,37,38]. A flow chart of the screening process is shown in Figure 1. A total of 429 OSA patients with a mean age of 49 years (84% males) and 258 non-OSA control subjects with a mean age of 47 years (74% males) were included. The characteristics of the studies, published between 2004 and 2018, are shown in Table 1.
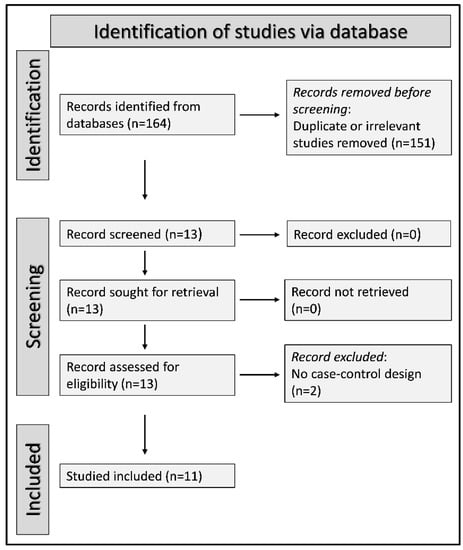
Figure 1.
PRISMA 2020 flow diagram.

Table 1.
Study characteristics.
3.2. Risk of Bias
In all studies included, a low risk of bias was estimated (Table 2).
Table 2.
The Joanna Briggs Institute critical appraisal checklist.
3.3. Results of Individual Studies and Syntheses
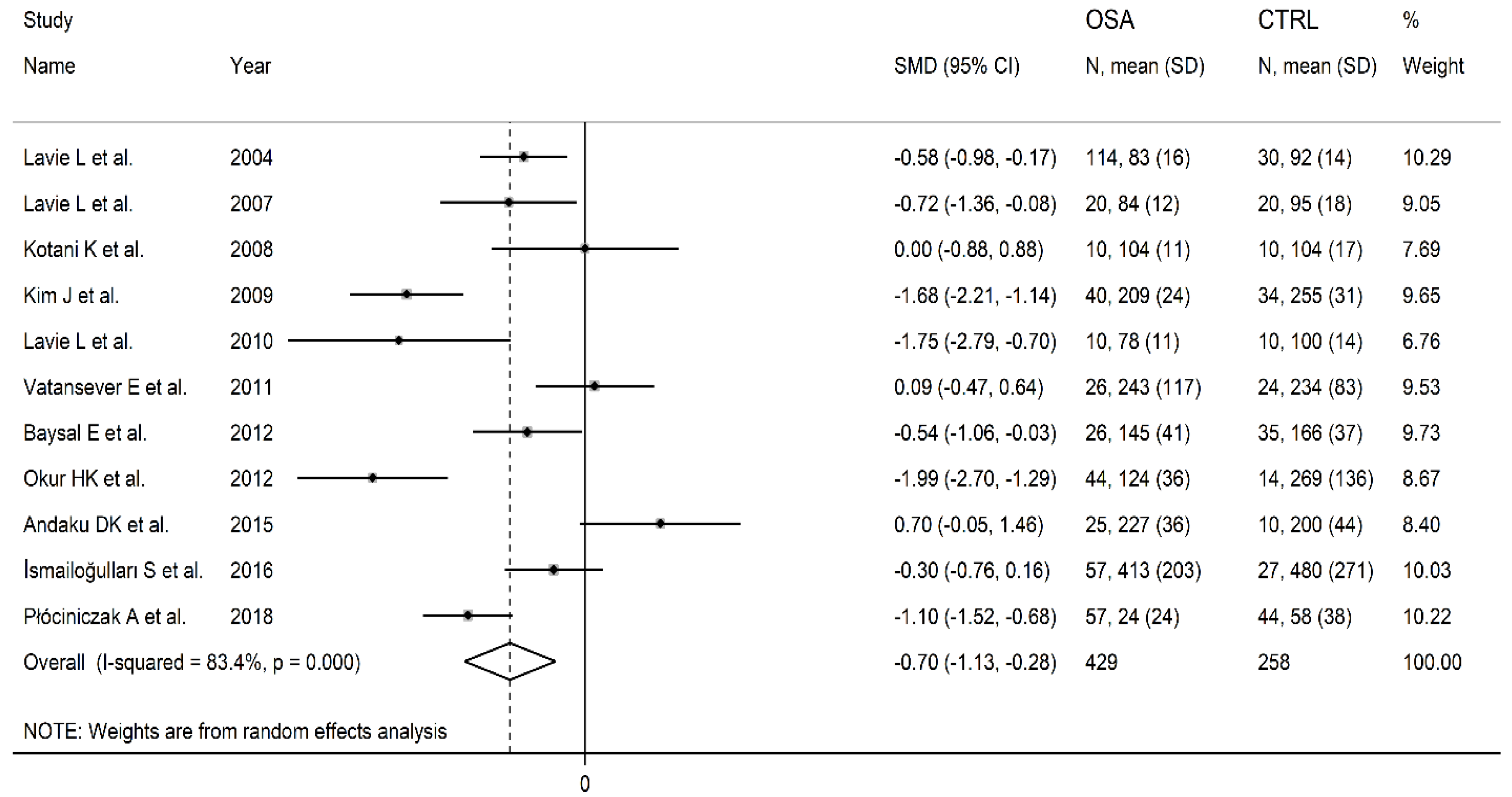
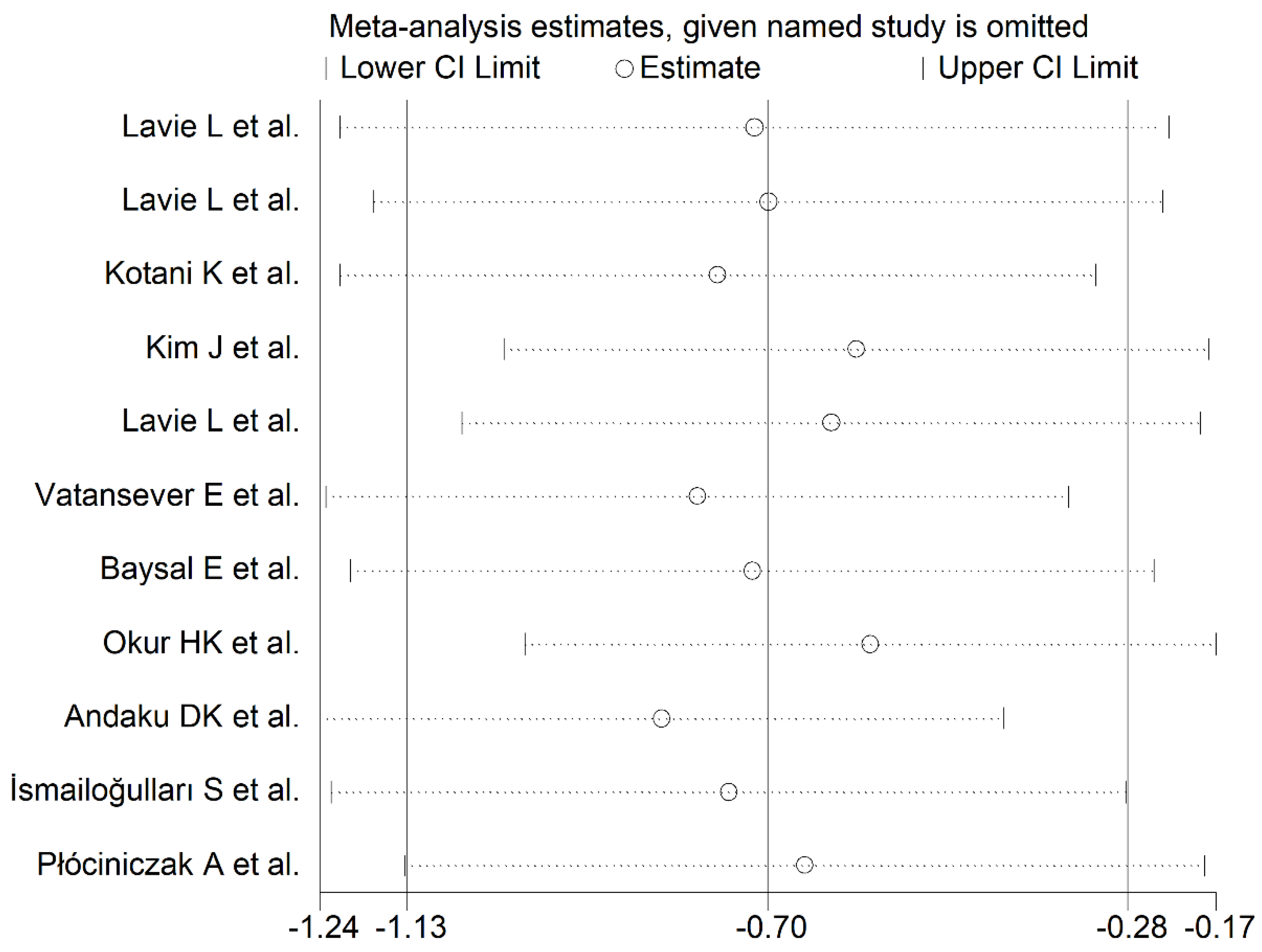
The forest plot reporting the PON-1 concentrations in OSA patients and control subjects is displayed in Figure 2. The results showed that in two studies [34,36], OSA patients had non-significantly higher PON-1 concentrations when compared with controls (mean difference range, 0.09 to 0.70). In one study, there were no between-group differences [31]. In the residual eight studies [15,16,30,32,33,35,37,38], OSA patients showed lower PON-1 concentrations than controls (mean difference range, −1.99 to −0.30) and the difference was statistically significant in all but one [37]. Random-effects models were used because of the extreme heterogeneity observed (I2 = 83.4%, p < 0.001). Pooled results indicated that PON-1 concentrations were significantly lower in OSA patients (SMD = −0.70, 95% CI −1.13 to −0.28; p = 0.001). Using the sensitivity analysis, the pooled SMD values were not substantially altered when individual studies were sequentially discarded (effect size range, between −0.83 and −0.58, Figure 3).
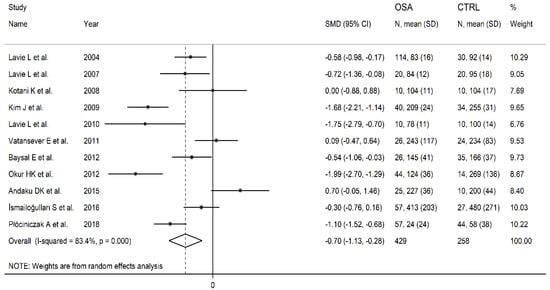
Figure 2.
Forest plot of studies evaluating serum paraoxonase-1(PON-1) concentrations in patients with obstructive sleep apnoea(OSA) and controls.
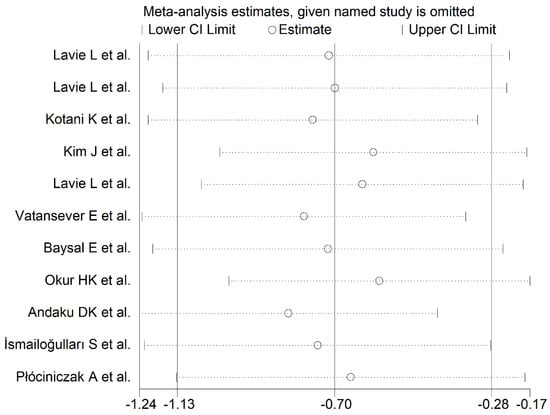
Figure 3.
Sensitivity analysis of the association between serum PON-1 concentrations and OSA. For each study, the shown effect size (hollow circles) corresponds to an overall effect size computed from a meta-analysis excluding that study.
3.4. Publication Bias
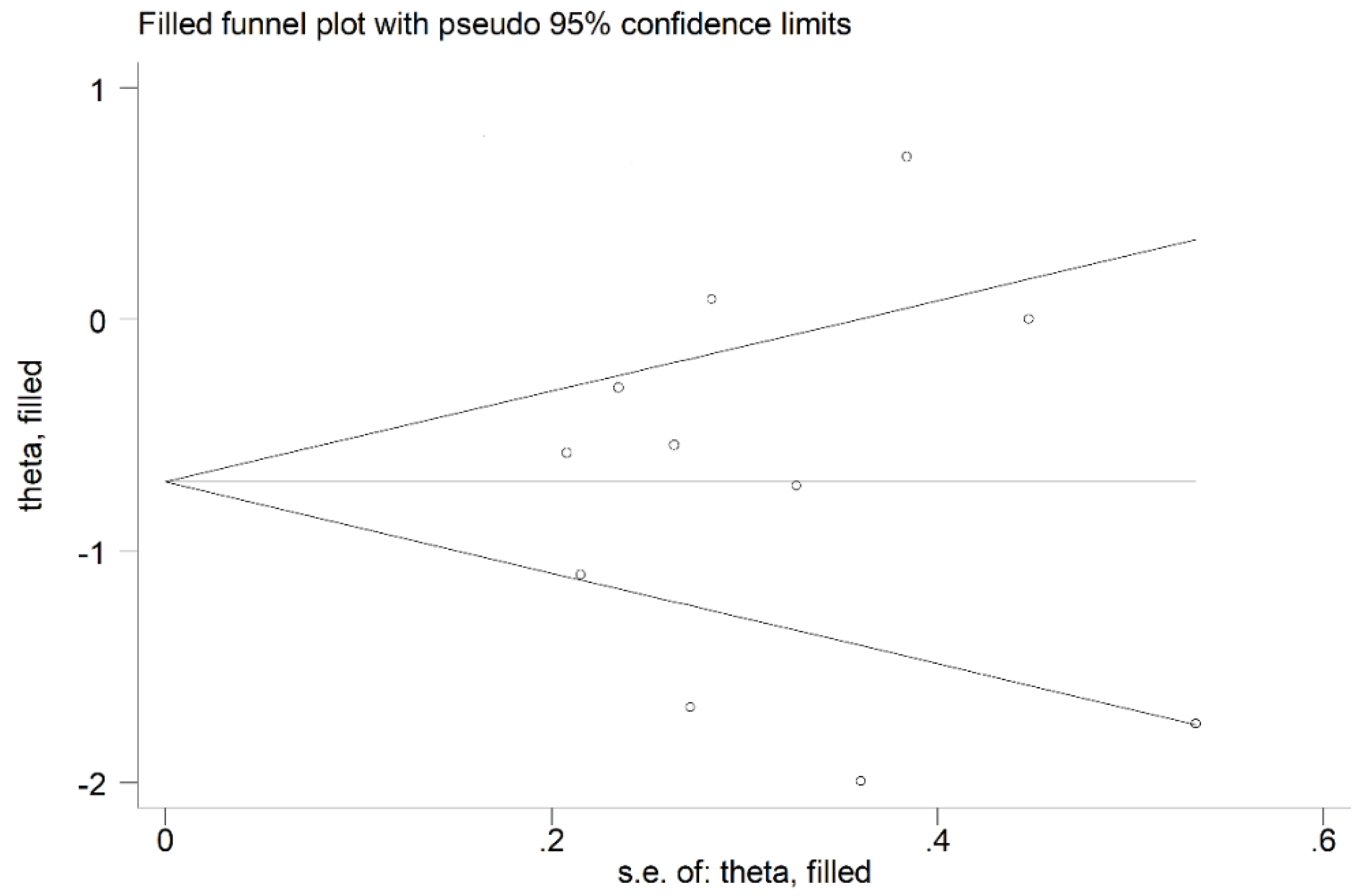
No publication bias was observed (Begg’s test, p = 1.00; Egger’s test, p = 0.99). Therefore, the trim-and-fill method did not detect missing studies to be included in the funnel plot (Figure 4).
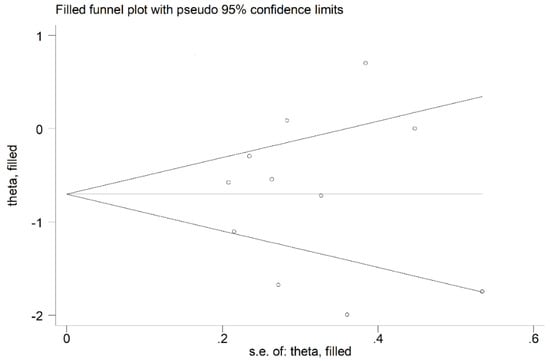
Figure 4.
Funnel plot of studies investigating the association between serum PON-1 concentrations and OSA after trimming and filling. The enclosed circles represent the dummy studies, while free circles symbolise the genuine studies.
3.5. Meta-Regression Analysis
No significant associations were detected between effect size and age (t = 0.62, p = 0.55), percentage of males (t = −0.124, p = 0.25), BMI (t = −0.55, p = 0.60), total cholesterol (t = 0.35, p = 0.74), LDL-cholesterol (t = 0.36, p = 0.73), HDL-cholesterol (t = 1.08, p = 0.32), triglycerides (t = −0.55, p = 0.60), AHI (t = −0.23, p = 0.83), sample size (t = −0.26, p = 0.80) and publication year (t = 0.30, p = 0.77).
3.6. Certainty of Evidence
The initial level of certainty for PON SMD values was evaluated low, due to the cross-sectional nature of the studies (rating 2, ⊕⊕⊖⊖). After considering the presence of low risk of bias in all articles (no rating change required), the high and unexplained heterogeneity (downgrade one level), the absence of indirectness (no rating change required), the relatively low imprecision (relatively narrow confidence intervals without threshold crossing, no rating change required), the moderate effect size (SMD = −0.70, no rating change required) and the absence of publication bias (no rating change required), the global level of certainty was degraded to very low (rating 1, ⊕⊖⊖⊖).
4. Discussion
The overproduction of ROS in OSA patients has been primarily attributed to the nocturnal intermittent hypoxia typical of the condition [4]. Several studies have reported excessive oxidative stress in untreated OSA and reduced oxidative stress burden during continuous positive airway pressure therapy [39,40]. It has been also proposed that the imbalance between pro-oxidant and antioxidant systems might contribute to the development of atherosclerotic cardiovascular disease in OSA [41]. In this context, an impaired capacity of PON-1 to preserve LDL from the oxidation of free radical has been reported in subjects with high cardiovascular risk [42]. Furthermore, PON-1 prevents endothelial dysfunction, commonly observed in OSA [43,44]. Therefore, PON-1 may be a useful marker for monitoring the oxidant–antioxidant balance in OSA patients.
The pooled SMD values observed in our study indicate a significant reduction in serum PON-1 concentrations in OSA patients when compared with non-OSA controls. Despite the extreme and unexplained between-study heterogeneity observed, the SMD values were not significantly modified in sensitivity analysis and there was no publication bias. No significant associations were observed between effect size and age, gender, BMI, total cholesterol, LDL cholesterol, HDL cholesterol, triglycerides, AHI, sample size and year of publication. Other unreported factors affecting the pro- vs. antioxidant balance, e.g., smoking history, comorbidities, use of specific medications, diet, lifestyle and genetic determinants of PON-1, may have contributed to the observed heterogeneity. In particular, the PON-1 R192Q and PON-1 L55M genetic polymorphisms have been associated with differences in PON-1 concentration and activity [45]. Despite these limitations, this meta-analysis supports the presence of a significant reduction of PON-1 concentrations in OSA.
Recently, a meta-analysis evaluating PON-1 concentrations in OSA patients was published by Fadaei et al. [46]. However, no significant differences in PON-1 concentrations were reported in a smaller number of studies, 5 vs. 11, which might explain their findings. Additionally, we conducted meta-regression analyses and assessed the certainty of evidence according to GRADE.
5. Conclusions
Our systematic review and meta-analysis showed significantly lower concentrations of the antioxidant PON-1 in OSA patients when compared to non-OSA controls. This supports the existence of a reduction in antioxidant protection mechanisms in OSA, likely secondary to nocturnal intermittent hypoxia. However, the significant heterogeneity observed warrants further research using rigorous standardized methods and diagnostic criteria to better establish the clinical utility of PON-1 measurements in OSA patients.
Author Contributions
All authors contributed to the study conception and design. Study Design: A.Z., M.C.P. and P.P.; Data Collection: E.Z., M.C.P., A.G.F. and C.C. Statistical Analysis: A.Z., A.A.M., G.P.; Data Interpretation: A.Z., M.C.P., A.G.F. and P.P.; Manuscript Preparation: M.C.P., E.Z., A.Z., A.A.M. and P.P.; Literature Search: E.Z., A.Z. and M.C.P.; Funding Acquisition: M.C.P., A.Z., C.C. and P.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by grants from: Ministry of Education, Universities and Research (MIUR) “Programma Operativo Nazionale (PON) Ricerca e Innovazione 2014–2020”, Asse I “Capitale Umano,” Azione I.2 A.I.M, “Attrazione e mobilita dei ricercatori,” Linea 1 (Mobilità dei Ricercatori); University of Sassari, Fondo di Ateneo per la Ricerca: annualità 2020.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- Patil, S.P.; Schneider, H.; Schwartz, A.R.; Smith, P.L. Adult obstructive sleep apnea: Pathophysiology and diagnosis. Chest 2007, 132, 325–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mochol, J.; Gawrys, J.; Gajecki, D.; Szahidewicz-Krupska, E.; Martynowicz, H.; Doroszko, A. Cardiovascular Disorders Triggered by Obstructive Sleep Apnea-A Focus on Endothelium and Blood Components. Int. J. Mol. Sci. 2021, 22, 5139. [Google Scholar] [CrossRef] [PubMed]
- Tietjens, J.R.; Claman, D.; Kezirian, E.J.; De Marco, T.; Mirzayan, A.; Sadroonri, B.; Goldberg, A.N.; Long, C.; Gerstenfeld, E.P.; Yeghiazarians, Y. Obstructive Sleep Apnea in Cardiovascular Disease: A Review of the Literature and Proposed Multidisciplinary Clinical Management Strategy. J. Am. Heart Assoc. 2019, 8, e010440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavie, L. Oxidative stress--a unifying paradigm in obstructive sleep apnea and comorbidities. Prog. Cardiovasc. Dis. 2009, 51, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, E.; Zinellu, A.; Fois, A.G.; Fois, S.S.; Piras, B.; Carru, C.; Pirina, P. Reliability and Usefulness of Different Biomarkers of Oxidative Stress in Chronic Obstructive Pulmonary Disease. Oxid. Med. Cell Longev. 2020, 2020, 4982324. [Google Scholar] [CrossRef] [PubMed]
- Jelic, M.; Mandic, A.; Maricic, S.; Srdjenovic, B. Oxidative stress and its role in cancer. J. Cancer Res. Ther. 2021, 17, 22–28. [Google Scholar] [CrossRef]
- Martinelli, N.; Consoli, L.; Girelli, D.; Grison, E.; Corrocher, R.; Olivieri, O. Paraoxonases: Ancient substrate hunters and their evolving role in ischemic heart disease. Adv. Clin. Chem. 2013, 59, 65–100. [Google Scholar]
- Goswami, B.; Tayal, D.; Gupta, N.; Mallika, V. Paraoxonase: A multifaceted biomolecule. Clin. Chim. Acta 2009, 410, 1–12. [Google Scholar] [CrossRef]
- Précourt, L.P.; Amre, D.; Denis, M.C.; Lavoie, J.C.; Delvin, E.; Seidman, E.; Levy, E. The three-gene paraoxonase family: Physiologic roles, actions and regulation. Atherosclerosis 2011, 214, 20–36. [Google Scholar] [CrossRef]
- Ceron, J.J.; Tecles, F.; Tvarijonaviciute, A. Serum paraoxonase 1 (PON-1) measurement: An update. BMC Vet. Res. 2014, 10, 74. [Google Scholar] [CrossRef]
- Taler-Verčič, A.; Goličnik, M.; Bavec, A. The Structure and Function of Paraoxonase-1 and Its Comparison to Paraoxonase-2 and -3. Molecules 2020, 25, 5980. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Bakker, S.J.L.; James, R.W.; Dullaart, R.P.F. Serum paraoxonase-1 activity and risk of incident cardiovascular disease: The PREVEND study and meta-analysis of prospective populationstudies. Atherosclerosis 2016, 245, 143–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokri, Y.; Variji, A.; Nosrati, M.; Khonakdar-Tarsi, A.; Kianmehr, A.; Kashi, Z.; Bahar, A.; Bagheri, A.; Mahrooz, A. Importance of paraoxonase 1 (PON-1) as an antioxidant and antiatherogenic enzyme in the cardiovascular complications of type 2 diabetes: Genotypic and phenotypic evaluation. Diabetes Res. Clin. Pract. 2020, 161, 108067. [Google Scholar] [CrossRef]
- Sarioglu, N.; Bilen, C.; Cevik, C.; Gencer, N. Paraoxonase Activity and Phenotype Distribution in Patients with Chronic Obstructive Pulmonary Disease. Eurasian J. Med. 2020, 52, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Okur, H.K.; Pelin, Z.; Yuksel, M.; Yosunkaya, S. Lipid peroxidation and paraoxonase activity in nocturnal cyclic and sustained intermittent hypoxia. Sleep Breath 2013, 17, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Lavie, L.; Vishnevsky, A.; Lavie, P. Evidence for lipid peroxidation in obstructive sleep apnea. Sleep 2004, 27, 123–128. [Google Scholar]
- Yadav, R.; France, M.; Aghamohammadzadeh, R.; Liu, Y.; Hama, S.; Kwok, S.; Schofield, J.; Turkington, P.; Syed, A.A.; Malik, R.; et al. Impairment of high-density lipoprotein resistance to lipid peroxidation and adipose tissue inflammation in obesity complicated by obstructive sleep apnea. J. Clin. Endocrinol. Metab. 2014, 99, 3390–3398. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In Joanna Briggs Institute Reviewer’s Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2020; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 3 March 2022).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hultcrantz, M.; Rind, D.; Akl, E.A.; Treweek, S.; Mustafa, R.A.; Iorio, A. The GRADE Working Group clarifies the construct of certainty of evidence. J. Clin. Epidemiol. 2017, 87, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Coello, P.A.; Guyatt, G.H.; Yepes-Nuñez, J.J.; Akl, E.A.; Hazlewood, G.; Pardo-Hernandez, H.; Etxeandia-Ikobaltzeta, I.; Qaseem, A.; Williams, J.W., Jr.; et al. GRADE guidelines: 20. Assessing the certainty of evidence in the importance of outcomes or values and preferences-inconsistency, imprecision, and other domains. J. Clin. Epidemiol. 2019, 111, 83–93. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A. Assessing the influence of a single study in the meta-analysis estimate. Stata Tech. Bull. 1999, 47, 15–17. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Lavie, L.; Vishnevsky, A.; Lavie, P. Oxidative stress and systemic inflammation in patients with sleep apnea: Role of obesity. Sleep Biol. Rhythm. 2007, 5, 100–110. [Google Scholar] [CrossRef]
- Kotani, K.; Kimura, S.; Tsuzaki, K.; Sakane, N.; Komada, I.; Schulze, J.; Gugliucci, A. Reduced paraoxonase 1/arylesterase activity and its post-therapeutic increase in obstructive sleep apnea syndrome: A preliminary study. Clin. Chim. Acta 2008, 395, 184–185. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.; In, K.; Kim, J.; You, S.; Kang, K.; Sim, J.; Lee, S.; Yoon, D.; Lee, J.; et al. Increase in serum haptoglobin and apolipoprotein M in patients with obstructive sleep apnoea. J. Sleep Res. 2009, 18, 313–320. [Google Scholar] [CrossRef]
- Lavie, L.; Dyugovskaya, L.; Golan-Shany, O.; Lavie, P. Heat-shock protein 70: Expression in monocytes of patients with sleep apnoea and association with oxidative stress and tumour necrosis factor-alpha. J. Sleep Res. 2010, 19 (1 Pt 2), 139–147. [Google Scholar] [CrossRef] [PubMed]
- Vatansever, E.; Surmen-Gur, E.; Ursavas, A.; Karadag, M. Obstructive sleep apnea causes oxidative damage to plasma lipids and proteins and decreases adiponectin levels. Sleep Breath 2011, 15, 275–282. [Google Scholar] [CrossRef]
- Baysal, E.; Taysi, S.; Aksoy, N.; Uyar, M.; Celenk, F.; Karatas, Z.A.; Tarakcioglu, M.; Bilinç, H.; Mumbuç, S.; Kanlikama, M. Serum paraoxonase, arylesterase activity and oxidative status in patients with obstructive sleep apnea syndrome (OSAS). Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 770–774. [Google Scholar] [PubMed]
- Andaku, D.K.; D’Almeida, V.; Carneiro, G.; Hix, S.; Tufik, S.; Togeiro, S.M. Sleepiness, inflammation and oxidative stress markers in middle-aged males with obstructive sleep apnea without metabolic syndrome: A cross-sectional study. Respir. Res. 2015, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismailogullari, S.; Gultekin, M.; Baskol, G.; Aksu, M. Increased oxidative stress and reduced antioxidant enzyme activity in obstructive sleep apnea syndrome. ISJMS 2016, 2, 56–59. [Google Scholar]
- Płóciniczak, A.; Baszczuk, A.; Ludziejewska, A.; Winiarska, H.; Michalak, S.; Kasprzak, G.; Formanowicz, D.; Cofta, S.; Wysocka, E. Paraoxonase 1 Gene L55M Polymorphism and Paraoxonase 1 Activity in Obstructive Sleep Apnea Patients. Adv. Exp. Med. Biol. 2019, 1150, 17–24. [Google Scholar]
- Eisele, H.J.; Markart, P.; Schulz, R. Obstructive Sleep Apnea, Oxidative Stress, and Cardiovascular Disease: Evidence from Human Studies. Oxid. Med. Cell Longev. 2015, 2015, 608438. [Google Scholar] [CrossRef] [Green Version]
- Maniaci, A.; Iannella, G.; Cocuzza, S.; Vicini, C.; Magliulo, G.; Ferlito, S.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Nicolai, A.; et al. Oxidative Stress and Inflammation Biomarker Expression in Obstructive Sleep Apnea Patients. J. Clin. Med. 2021, 10, 277. [Google Scholar] [CrossRef]
- Suzuki, Y.J.; Jain, V.; Park, A.M.; Day, R.M. Oxidative stress and oxidant signaling in obstructive sleep apnea and associated cardiovascular diseases. Free Radic. Biol. Med. 2006, 40, 1683–1692. [Google Scholar] [CrossRef] [Green Version]
- Granér, M.; James, R.W.; Kahri, J.; Nieminen, M.S.; Syvänne, M.; Taskinen, M.R. Association of paraoxonase-1 activity and concentration with angiographic severity and extent of coronary artery disease. J. Am. Coll Cardiol. 2006, 47, 2429–2435. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, Z.; Babaei, S.; Maguire, G.F.; Draganov, D.; Kuksis, A.; La Du, B.N.; Connelly, P.W. Paraoxonase-1 reduces monocyte chemotaxis and adhesion to endothelial cells due to oxidation of palmitoyl, linoleoyl glycerophosphorylcholine. Cardiovasc Res. 2003, 57, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Ramar, K.; Caples, S.M. Vascular changes, cardiovascular disease and obstructive sleep apnea. Future Cardiol 2011, 7, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Shunmoogam, N.; Naidoo, P.; Chilton, R. Paraoxonase (PON)-1: A brief overview on genetics, structure, polymorphisms and clinical relevance. Vasc. Health Risk Manag. 2018, 14, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadaei, R.; Safari-Faramani, R.; Rezaei, M.; Ahmadi, R.; Rostampour, M.; Moradi, N.; Khazaie, H. Paraoxonase Activity in Patients with Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. SN Comp. Clin. Med. 2020, 2, 25–31. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).