
Paraoxonase-1 Concentrations in Obstructive Sleep Apnoea: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
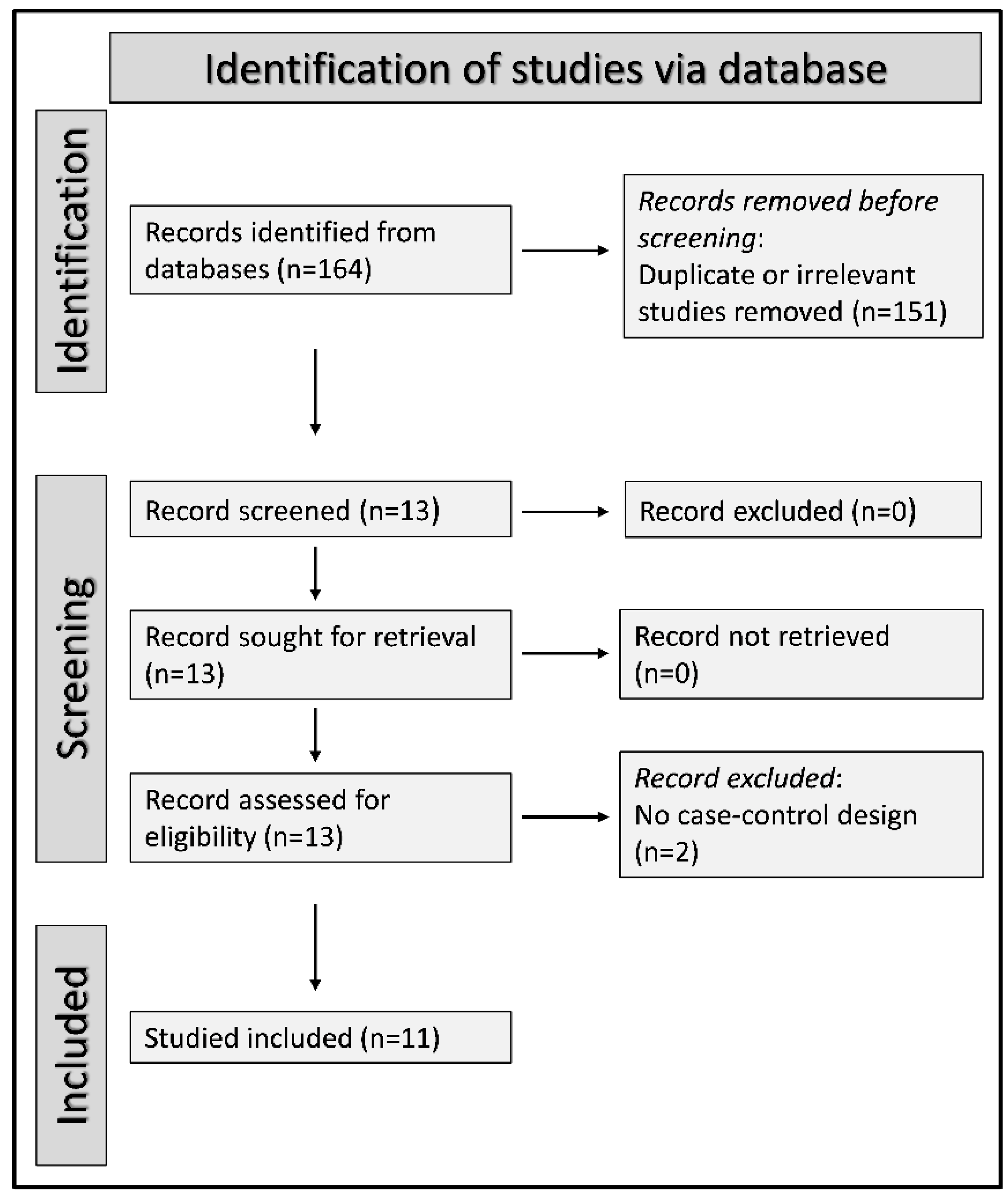
2.1. Search Strategy, Eligibility Criteria and Study Selection
2.2. Statistical Analysis
3. Results
3.1. Systematic Research and Study Characteristics
3.2. Risk of Bias
3.3. Results of Individual Studies and Syntheses
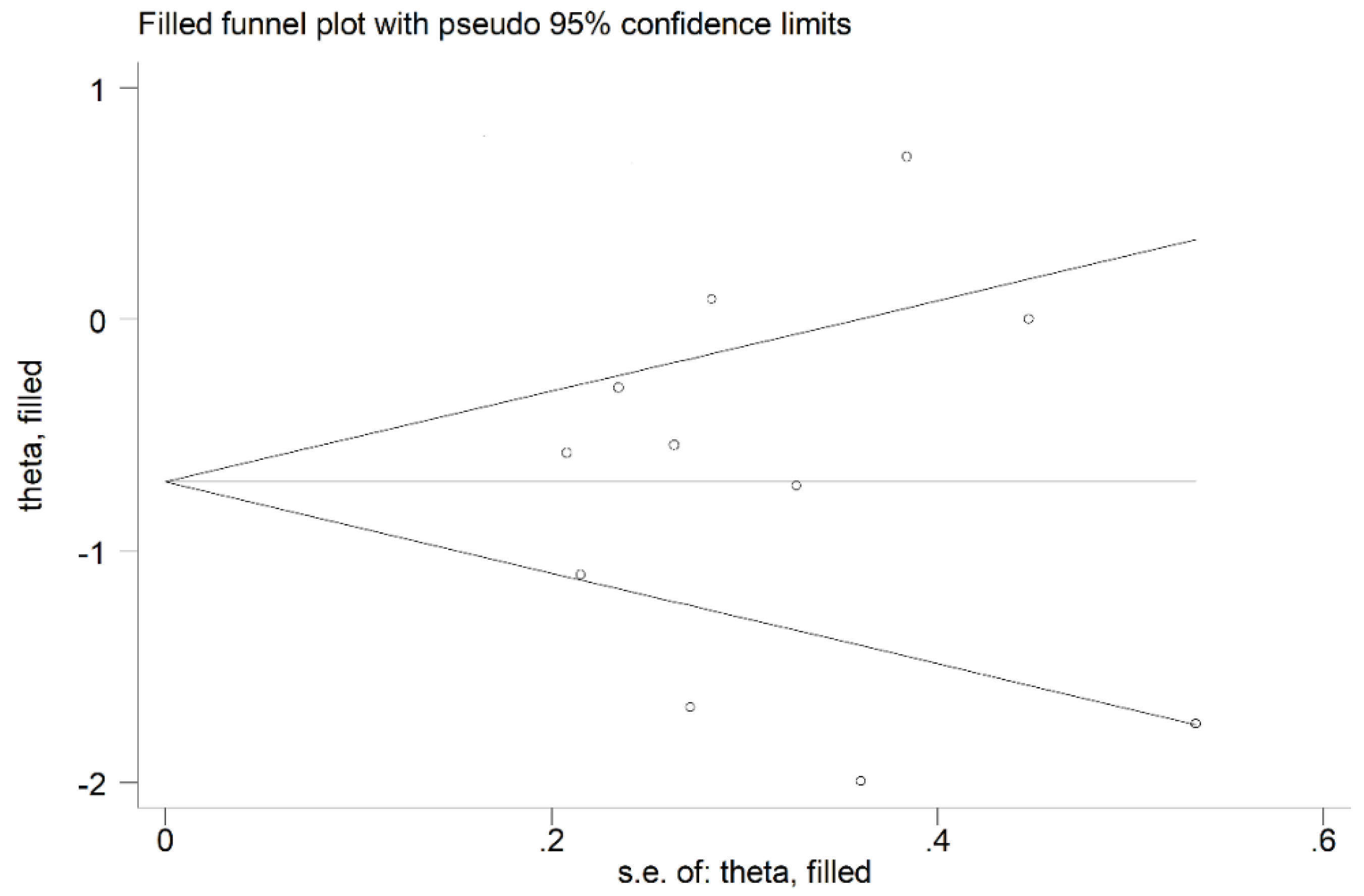
3.4. Publication Bias
3.5. Meta-Regression Analysis
3.6. Certainty of Evidence
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patil, S.P.; Schneider, H.; Schwartz, A.R.; Smith, P.L. Adult obstructive sleep apnea: Pathophysiology and diagnosis. Chest 2007, 132, 325–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mochol, J.; Gawrys, J.; Gajecki, D.; Szahidewicz-Krupska, E.; Martynowicz, H.; Doroszko, A. Cardiovascular Disorders Triggered by Obstructive Sleep Apnea-A Focus on Endothelium and Blood Components. Int. J. Mol. Sci. 2021, 22, 5139. [Google Scholar] [CrossRef] [PubMed]
- Tietjens, J.R.; Claman, D.; Kezirian, E.J.; De Marco, T.; Mirzayan, A.; Sadroonri, B.; Goldberg, A.N.; Long, C.; Gerstenfeld, E.P.; Yeghiazarians, Y. Obstructive Sleep Apnea in Cardiovascular Disease: A Review of the Literature and Proposed Multidisciplinary Clinical Management Strategy. J. Am. Heart Assoc. 2019, 8, e010440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lavie, L. Oxidative stress--a unifying paradigm in obstructive sleep apnea and comorbidities. Prog. Cardiovasc. Dis. 2009, 51, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Zinellu, E.; Zinellu, A.; Fois, A.G.; Fois, S.S.; Piras, B.; Carru, C.; Pirina, P. Reliability and Usefulness of Different Biomarkers of Oxidative Stress in Chronic Obstructive Pulmonary Disease. Oxid. Med. Cell Longev. 2020, 2020, 4982324. [Google Scholar] [CrossRef] [PubMed]
- Jelic, M.; Mandic, A.; Maricic, S.; Srdjenovic, B. Oxidative stress and its role in cancer. J. Cancer Res. Ther. 2021, 17, 22–28. [Google Scholar] [CrossRef]
- Martinelli, N.; Consoli, L.; Girelli, D.; Grison, E.; Corrocher, R.; Olivieri, O. Paraoxonases: Ancient substrate hunters and their evolving role in ischemic heart disease. Adv. Clin. Chem. 2013, 59, 65–100. [Google Scholar]
- Goswami, B.; Tayal, D.; Gupta, N.; Mallika, V. Paraoxonase: A multifaceted biomolecule. Clin. Chim. Acta 2009, 410, 1–12. [Google Scholar] [CrossRef]
- Précourt, L.P.; Amre, D.; Denis, M.C.; Lavoie, J.C.; Delvin, E.; Seidman, E.; Levy, E. The three-gene paraoxonase family: Physiologic roles, actions and regulation. Atherosclerosis 2011, 214, 20–36. [Google Scholar] [CrossRef]
- Ceron, J.J.; Tecles, F.; Tvarijonaviciute, A. Serum paraoxonase 1 (PON-1) measurement: An update. BMC Vet. Res. 2014, 10, 74. [Google Scholar] [CrossRef]
- Taler-Verčič, A.; Goličnik, M.; Bavec, A. The Structure and Function of Paraoxonase-1 and Its Comparison to Paraoxonase-2 and -3. Molecules 2020, 25, 5980. [Google Scholar] [CrossRef] [PubMed]
- Kunutsor, S.K.; Bakker, S.J.L.; James, R.W.; Dullaart, R.P.F. Serum paraoxonase-1 activity and risk of incident cardiovascular disease: The PREVEND study and meta-analysis of prospective populationstudies. Atherosclerosis 2016, 245, 143–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shokri, Y.; Variji, A.; Nosrati, M.; Khonakdar-Tarsi, A.; Kianmehr, A.; Kashi, Z.; Bahar, A.; Bagheri, A.; Mahrooz, A. Importance of paraoxonase 1 (PON-1) as an antioxidant and antiatherogenic enzyme in the cardiovascular complications of type 2 diabetes: Genotypic and phenotypic evaluation. Diabetes Res. Clin. Pract. 2020, 161, 108067. [Google Scholar] [CrossRef]
- Sarioglu, N.; Bilen, C.; Cevik, C.; Gencer, N. Paraoxonase Activity and Phenotype Distribution in Patients with Chronic Obstructive Pulmonary Disease. Eurasian J. Med. 2020, 52, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Okur, H.K.; Pelin, Z.; Yuksel, M.; Yosunkaya, S. Lipid peroxidation and paraoxonase activity in nocturnal cyclic and sustained intermittent hypoxia. Sleep Breath 2013, 17, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Lavie, L.; Vishnevsky, A.; Lavie, P. Evidence for lipid peroxidation in obstructive sleep apnea. Sleep 2004, 27, 123–128. [Google Scholar]
- Yadav, R.; France, M.; Aghamohammadzadeh, R.; Liu, Y.; Hama, S.; Kwok, S.; Schofield, J.; Turkington, P.; Syed, A.A.; Malik, R.; et al. Impairment of high-density lipoprotein resistance to lipid peroxidation and adipose tissue inflammation in obesity complicated by obstructive sleep apnea. J. Clin. Endocrinol. Metab. 2014, 99, 3390–3398. [Google Scholar] [CrossRef] [Green Version]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetcu, R.; Currie, M.; Qureshi, R.; Mattis, P.; Lisy, K.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In Joanna Briggs Institute Reviewer’s Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; The Joanna Briggs Institute: Adelaide, Australia, 2020; Available online: https://reviewersmanual.joannabriggs.org/ (accessed on 3 March 2022).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Erlbaum: Hillsdale, NJ, USA, 1988. [Google Scholar]
- Hultcrantz, M.; Rind, D.; Akl, E.A.; Treweek, S.; Mustafa, R.A.; Iorio, A. The GRADE Working Group clarifies the construct of certainty of evidence. J. Clin. Epidemiol. 2017, 87, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Coello, P.A.; Guyatt, G.H.; Yepes-Nuñez, J.J.; Akl, E.A.; Hazlewood, G.; Pardo-Hernandez, H.; Etxeandia-Ikobaltzeta, I.; Qaseem, A.; Williams, J.W., Jr.; et al. GRADE guidelines: 20. Assessing the certainty of evidence in the importance of outcomes or values and preferences-inconsistency, imprecision, and other domains. J. Clin. Epidemiol. 2019, 111, 83–93. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bowden, J.; Tierney, J.F.; Copas, A.J.; Burdett, S. Quantifying, displaying and accounting for heterogeneity in the meta-analysis of RCTs using standard and generalised Q statistics. BMC Med. Res. Methodol. 2011, 11, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Tobias, A. Assessing the influence of a single study in the meta-analysis estimate. Stata Tech. Bull. 1999, 47, 15–17. [Google Scholar]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M. Funnel plots for detecting bias in meta-analysis: Guidelines on choice of axis. J. Clin. Epidemiol. 2001, 54, 1046–1055. [Google Scholar] [CrossRef]
- Duval, S.; Tweedie, R. Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics 2000, 56, 455–463. [Google Scholar] [CrossRef]
- Lavie, L.; Vishnevsky, A.; Lavie, P. Oxidative stress and systemic inflammation in patients with sleep apnea: Role of obesity. Sleep Biol. Rhythm. 2007, 5, 100–110. [Google Scholar] [CrossRef]
- Kotani, K.; Kimura, S.; Tsuzaki, K.; Sakane, N.; Komada, I.; Schulze, J.; Gugliucci, A. Reduced paraoxonase 1/arylesterase activity and its post-therapeutic increase in obstructive sleep apnea syndrome: A preliminary study. Clin. Chim. Acta 2008, 395, 184–185. [Google Scholar] [CrossRef]
- Kim, J.; Lee, S.; In, K.; Kim, J.; You, S.; Kang, K.; Sim, J.; Lee, S.; Yoon, D.; Lee, J.; et al. Increase in serum haptoglobin and apolipoprotein M in patients with obstructive sleep apnoea. J. Sleep Res. 2009, 18, 313–320. [Google Scholar] [CrossRef]
- Lavie, L.; Dyugovskaya, L.; Golan-Shany, O.; Lavie, P. Heat-shock protein 70: Expression in monocytes of patients with sleep apnoea and association with oxidative stress and tumour necrosis factor-alpha. J. Sleep Res. 2010, 19 (1 Pt 2), 139–147. [Google Scholar] [CrossRef] [PubMed]
- Vatansever, E.; Surmen-Gur, E.; Ursavas, A.; Karadag, M. Obstructive sleep apnea causes oxidative damage to plasma lipids and proteins and decreases adiponectin levels. Sleep Breath 2011, 15, 275–282. [Google Scholar] [CrossRef]
- Baysal, E.; Taysi, S.; Aksoy, N.; Uyar, M.; Celenk, F.; Karatas, Z.A.; Tarakcioglu, M.; Bilinç, H.; Mumbuç, S.; Kanlikama, M. Serum paraoxonase, arylesterase activity and oxidative status in patients with obstructive sleep apnea syndrome (OSAS). Eur. Rev. Med. Pharmacol. Sci. 2012, 16, 770–774. [Google Scholar] [PubMed]
- Andaku, D.K.; D’Almeida, V.; Carneiro, G.; Hix, S.; Tufik, S.; Togeiro, S.M. Sleepiness, inflammation and oxidative stress markers in middle-aged males with obstructive sleep apnea without metabolic syndrome: A cross-sectional study. Respir. Res. 2015, 16, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ismailogullari, S.; Gultekin, M.; Baskol, G.; Aksu, M. Increased oxidative stress and reduced antioxidant enzyme activity in obstructive sleep apnea syndrome. ISJMS 2016, 2, 56–59. [Google Scholar]
- Płóciniczak, A.; Baszczuk, A.; Ludziejewska, A.; Winiarska, H.; Michalak, S.; Kasprzak, G.; Formanowicz, D.; Cofta, S.; Wysocka, E. Paraoxonase 1 Gene L55M Polymorphism and Paraoxonase 1 Activity in Obstructive Sleep Apnea Patients. Adv. Exp. Med. Biol. 2019, 1150, 17–24. [Google Scholar]
- Eisele, H.J.; Markart, P.; Schulz, R. Obstructive Sleep Apnea, Oxidative Stress, and Cardiovascular Disease: Evidence from Human Studies. Oxid. Med. Cell Longev. 2015, 2015, 608438. [Google Scholar] [CrossRef] [Green Version]
- Maniaci, A.; Iannella, G.; Cocuzza, S.; Vicini, C.; Magliulo, G.; Ferlito, S.; Cammaroto, G.; Meccariello, G.; De Vito, A.; Nicolai, A.; et al. Oxidative Stress and Inflammation Biomarker Expression in Obstructive Sleep Apnea Patients. J. Clin. Med. 2021, 10, 277. [Google Scholar] [CrossRef]
- Suzuki, Y.J.; Jain, V.; Park, A.M.; Day, R.M. Oxidative stress and oxidant signaling in obstructive sleep apnea and associated cardiovascular diseases. Free Radic. Biol. Med. 2006, 40, 1683–1692. [Google Scholar] [CrossRef] [Green Version]
- Granér, M.; James, R.W.; Kahri, J.; Nieminen, M.S.; Syvänne, M.; Taskinen, M.R. Association of paraoxonase-1 activity and concentration with angiographic severity and extent of coronary artery disease. J. Am. Coll Cardiol. 2006, 47, 2429–2435. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, Z.; Babaei, S.; Maguire, G.F.; Draganov, D.; Kuksis, A.; La Du, B.N.; Connelly, P.W. Paraoxonase-1 reduces monocyte chemotaxis and adhesion to endothelial cells due to oxidation of palmitoyl, linoleoyl glycerophosphorylcholine. Cardiovasc Res. 2003, 57, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Ramar, K.; Caples, S.M. Vascular changes, cardiovascular disease and obstructive sleep apnea. Future Cardiol 2011, 7, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Shunmoogam, N.; Naidoo, P.; Chilton, R. Paraoxonase (PON)-1: A brief overview on genetics, structure, polymorphisms and clinical relevance. Vasc. Health Risk Manag. 2018, 14, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadaei, R.; Safari-Faramani, R.; Rezaei, M.; Ahmadi, R.; Rostampour, M.; Moradi, N.; Khazaie, H. Paraoxonase Activity in Patients with Obstructive Sleep Apnea: A Systematic Review and Meta-analysis. SN Comp. Clin. Med. 2020, 2, 25–31. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control | OSA | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| First Author and Year, Country | N | Age Mean or Median | M/F | PON Mean ± SD (U/L) | N | Age Mean or Median | M/F | PON Mean ± SD (U/L) | AHI Events/h |
| Lavie L et al., 2004, Israel | 30 | 43 | 27/3 | 92 ± 14 * | 114 | 53 | 91/23 | 83 ± 16 * | NR |
| Lavie L et al., 2007, Israel | 20 | 42 | 16/4 | 95 ± 18 * | 20 | 42 | 16/4 | 84 ± 12 * | 29 |
| Kotani K et al., 2008, Japan | 10 | 52 | 5/5 | 104 ± 17 | 10 | 52 | 5/5 | 104 ± 11 | ≥20 |
| Kim J et al., 2009, South Korea | 34 | 45 | 34/0 | 255 ± 31 | 40 | 45 | 40/0 | 209 ± 24 | 54 |
| Lavie L et al., 2010, Israel | 10 | 43 | 8/2 | 100 ± 14 * | 10 | 45 | 8/2 | 78 ± 11 * | 29 |
| Vatansever E et al., 2011, Turkey | 24 | 47 | 24/0 | 234 ± 83 | 26 | 49 | 26/0 | 243 ± 117 | 38 |
| Baysal E et al., 2012, Turkey | 35 | 47 | 15/20 | 166 ± 37 | 26 | 49 | NR | 145 ± 41 | 31 |
| Okur HK et al., 2012, Turkey | 14 | 49 | 11/3 | 269 ± 136 | 44 | 44 | 40/4 | 124 ± 36 | 37 |
| Andaku DK et al., 2015, Brazil | 10 | 43 | 10/0 | 200 ± 44 * | 25 | 44 | 25/0 | 227 ± 36 * | 35 |
| İsmailoğulları S et al., 2016, Turkey | 27 | 48 | 18/9 | 480 ± 271 | 57 | 47 | 45/12 | 413 ± 203 | 42 |
| Płóciniczak A et al., 2018, Poland | 44 | 52 | 23/21 | 58 ± 38 | 57 | 58 | 44/13 | 24 ± 24 | 22 |
| Study | Were the Criteria for Inclusion in the Sample Clearly Defined? | Were the Study Subjects and the Setting Described in Detail? | Was the Exposure Measured in a Valid and Reliable Way? | Were Objective, Standard Criteria Used for Measurement of the Condition? | Were Confounding Factors Identified? | Were Strategies to Deal with Confounding Factors Stated? | Were the OUTCOMES Measured in a Valid and Reliable Way? | Was Appropriate Statistical Analysis Used? | Risk of Bias |
|---|---|---|---|---|---|---|---|---|---|
| Lavie L et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Lavie L et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Kotani K et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Kim J et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Lavie et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Vatansever E et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Baysal E et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Okur HK et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
| Andaku DK et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| İsmailoğulları S et al. | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Low |
| Płóciniczak A et al. | Yes | Yes | Yes | Yes | No | No | Yes | No | Low |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pau, M.C.; Zinellu, A.; Zinellu, E.; Pintus, G.; Carru, C.; Fois, A.G.; Mangoni, A.A.; Pirina, P. Paraoxonase-1 Concentrations in Obstructive Sleep Apnoea: A Systematic Review and Meta-Analysis. Antioxidants 2022, 11, 766. https://doi.org/10.3390/antiox11040766
Pau MC, Zinellu A, Zinellu E, Pintus G, Carru C, Fois AG, Mangoni AA, Pirina P. Paraoxonase-1 Concentrations in Obstructive Sleep Apnoea: A Systematic Review and Meta-Analysis. Antioxidants. 2022; 11(4):766. https://doi.org/10.3390/antiox11040766
Chicago/Turabian StylePau, Maria Carmina, Angelo Zinellu, Elisabetta Zinellu, Gianfranco Pintus, Ciriaco Carru, Alessandro G. Fois, Arduino A. Mangoni, and Pietro Pirina. 2022. "Paraoxonase-1 Concentrations in Obstructive Sleep Apnoea: A Systematic Review and Meta-Analysis" Antioxidants 11, no. 4: 766. https://doi.org/10.3390/antiox11040766
APA StylePau, M. C., Zinellu, A., Zinellu, E., Pintus, G., Carru, C., Fois, A. G., Mangoni, A. A., & Pirina, P. (2022). Paraoxonase-1 Concentrations in Obstructive Sleep Apnoea: A Systematic Review and Meta-Analysis. Antioxidants, 11(4), 766. https://doi.org/10.3390/antiox11040766