


Superficial Neuromodulation in Dysautonomia in Women with Post-COVID-19 Condition: A Pilot Study

 , , ,
, , ,  and
and
Abstract
1. Introduction
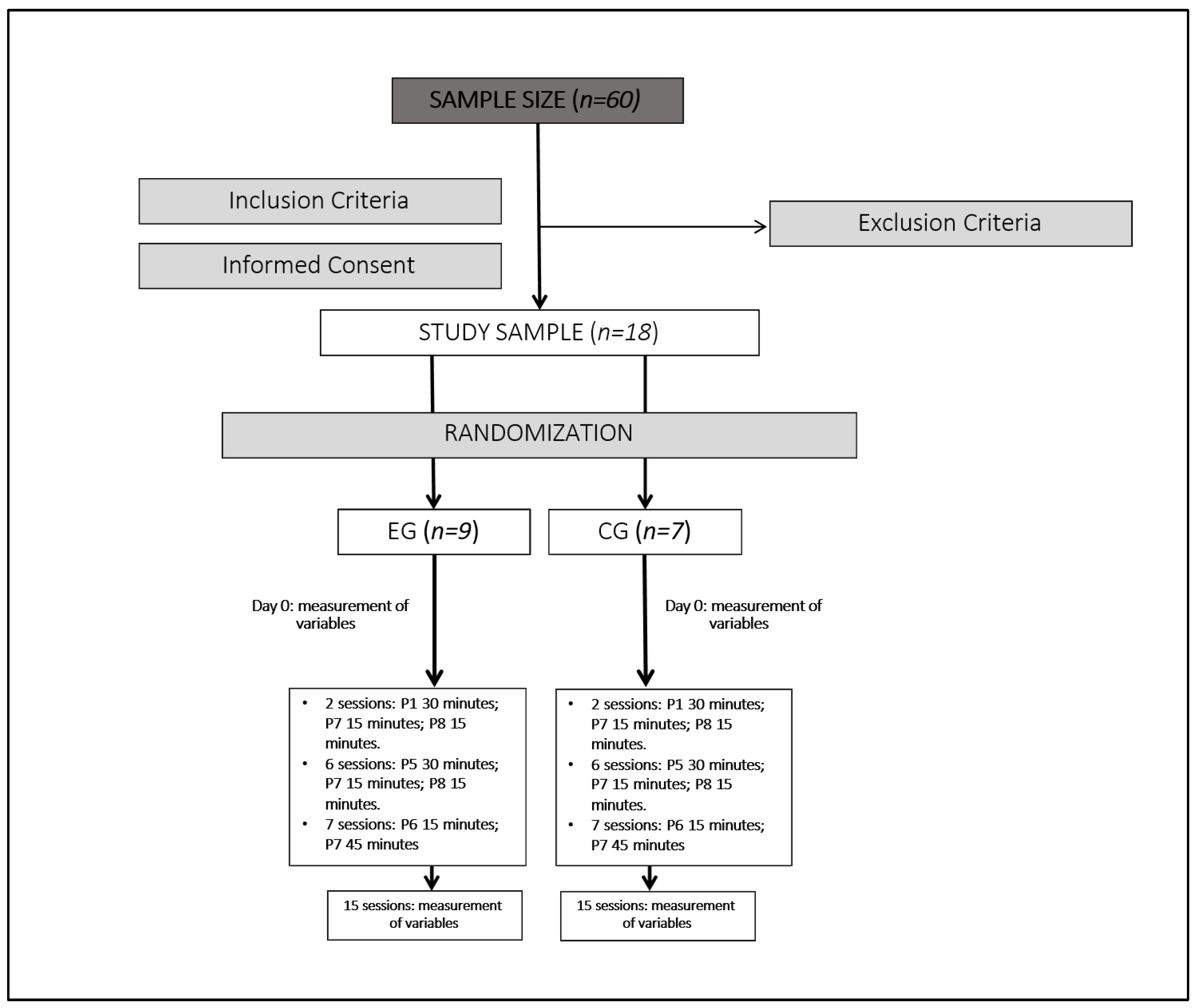
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bouza, E.; Cantón-Moreno, R.; De Lucas-Ramos, P.; García-Botella, A.; García-Lledó, A.; Gómez-Pavón, J.; González-Del Castillo, J.; Hernández-Sampelayo, T.; Martín-Delgado, M.C.; Martín-Sánchez, F.J.; et al. Síndrome post-COVID: Un documento de reflexión y opinión. Rev. Esp. Quimioter. 2021, 34, 269–279. [Google Scholar] [CrossRef] [PubMed]
- Emergency Use ICD Codes for COVID-19 Disease Outbreak. Available online: https://www.who.int/standards/classifications/classification-of-diseases/emergency-use-icd-codes-for-covid-19-disease-outbreak (accessed on 29 March 2021).
- SEMG. Guía Clínica para la Atención al Paciente Long COVID/COVID Persistente. Available online: https://www.semg.es/index.php/consensos-guias-y-protocolos/363-guia-clinica-para-la-atencion-al-paciente-long-covid-covid-persistente (accessed on 14 June 2021).
- Ministerio de Sanidad. Gobierno de España. Available online: https://www.sanidad.gob.es/ (accessed on 21 April 2021).
- Carod-Artal, F.J. Complicaciones neurológicas por coronavirus y COVID-19. Rev. Neurol. 2020, 70, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Llorente, B.C.; López, A.M.C.; Sánchez, R.H.; Gutiérrez, C.H. Protocolo diagnóstico de las manifestaciones crónicas de la COVID-19 [Diagnostic protocol for chronic manifestations of COVID-19]. Medicine 2022, 13, 3256–3260. [Google Scholar] [CrossRef] [PubMed]
- Shah, D.P.; Thaweethai, T.; Karlson, E.W.; Bonilla, H.; Horne, B.D.; Mullington, J.M.; Wisnivesky, J.P.; Hornig, M.; Shinnick, D.J.; Klein, J.D.; et al. Sex Differences in Long COVID. JAMA Netw. Open 2025, 8, e2455430. [Google Scholar] [CrossRef]
- Honigsbaum, M.; Krishnan, L. Taking pandemic sequelae seriously: From the Russian influenza to COVID-19 long-haulers. Lancet 2020, 396, 1389–1391. [Google Scholar] [CrossRef]
- Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Qusti, S.; Alshammari, E.M.; Gyebi, G.A.; Batiha, G.E. COVID-19-Induced Dysautonomia: A Menace of Sympathetic Storm. ASN Neuro 2021, 13, 17590914211057635. [Google Scholar] [CrossRef]
- Kaliyaperumal, D.; Rk, K.; Alagesan, M.; Ramalingam, S. Characterization of cardiac autonomic function in COVID-19 using heart rate variability: A hospital based preliminary observational study. J. Basic Clin. Physiol. Pharmacol. 2021, 32, 247–253. [Google Scholar] [CrossRef]
- Barizien, N.; Guen, M.; Russel, S.; Touche, P.; Huang, F.; Vallée, A. Clinical characterization of dysautonomia in long COVID-19 patients. Sci. Rep. 2021, 11, 14042. [Google Scholar] [CrossRef]
- Quinn, K.L.; Lam, G.Y.; Walsh, J.F.; Bhéreur, A.; Brown, A.D.; Chow, C.W.; Chung, K.Y.C.; Cowan, J.; Crampton, N.; Décary, S.; et al. Cardiovascular Considerations in the Management of People with Suspected Long COVID. Can. J. Cardiol. 2023, 39, 741–753. [Google Scholar] [CrossRef]
- Haischer, M.H.; Opielinski, L.E.; Mirkes, L.M.; Uhrich, T.D.; Bollaert, R.E.; Danduran, M.; Bement, M.H.; Piacentine, L.B.; Papanek, P.E.; Hunter, S.K. Heart rate variability is reduced in COVID-19 survivors and associated with physical activity and fatigue. Physiol. Rep. 2024, 12, e15912. [Google Scholar] [CrossRef]
- Cano-de-la-Cuerda, R.; Jiménez-Antona, C.; Melián-Ortiz, A.; Molero-Sánchez, A.; Gil-de Miguel, Á.; Lizcano-Álvarez, Á.; Hernández-Barrera, V.; Varillas-Delgado, D.; Laguarta-Val, S. Construct Validity and Test-Retest Reliability of a Free Mobile Application to Evaluate Aerobic Capacity and Endurance in Post-COVID-19 Syndrome Patients-A Pilot Study. J. Clin. Med. 2022, 24, 131. [Google Scholar] [CrossRef] [PubMed]
- Lizcano-Álvarez, Á.; Varillas-Delgado, D.; Cano-de-la-Cuerda, R.; Jiménez-Antona, C.; Melián-Ortiz, A.; Molero-Sánchez, A.; Laguarta-Val, S. The Association of Genetic Markers Involved in Muscle Performance Responding to Lactate Levels during Physical Exercise Therapy by Nordic Walking in Patients with Long COVID Syndrome: A Nonrandomized Controlled Pilot Study. Int. J. Mol. Sci. 2024, 25, 8305. [Google Scholar] [CrossRef]
- Laguarta-Val, S.; Varillas-Delgado, D.; Lizcano-Álvarez, Á.; Molero-Sánchez, A.; Melian-Ortiz, A.; Cano-de-la-Cuerda, R.; Jiménez-Antona, C. Effects of Aerobic Exercise Therapy through Nordic Walking Program in Lactate Concentrations, Fatigue and Quality-of-Life in Patients with Long-COVID Syndrome: A Non-Randomized Parallel Controlled Trial. J. Clin. Med. 2024, 13, 1035. [Google Scholar] [CrossRef] [PubMed]
- Kinser, A.M.; Sands, W.A.; Stone, M.H. Reliability and validity of a pressure algometer. J. Strength Cond. Res. 2009, 23, 312–314. [Google Scholar] [CrossRef] [PubMed]
- Torres-González, N.; Álvarez-Acosta, L.; Iriarte-Plasencia, A.; Barreto-Cáceres, V.; Valdivia-Miranda, D.; Hernández-Afonso, J.S. Control electrocardiográfico del intervalo QT mediante dispositivo portátil en pacientes ingresados por COVID-19. Propuesta de protocolo [Electrocardiographic/QT interval monitoring with a portable device in hospitalized patients with COVID-19: A protocol proposal]. Rev. Esp. Cardiol. 2020, 73, 771–773. [Google Scholar] [CrossRef]
- Kos, D.; Kerckhofs, E.; Carrea, I.; Verza, R.; Ramos, M.; Jansa, J. Evaluation of the Modified Fatigue Impact Scale in four different European countries. Mult. Scler. 2005, 11, 76–80. [Google Scholar] [CrossRef]
- Beck, S.L.; Schwartz, A.L.; Towsley, G.; Dudley, W.; Barsevick, A. Psychometric evaluation of the Pittsburgh Sleep Quality Index in cancer patients. J. Pain Symptom Manag. 2004, 27, 140–148. [Google Scholar] [CrossRef]
- Vilagut, G.; Ferrer, M.; Rajmil, L.; Rebollo, P.; Permanyer-Miralda, G.; Quintana, J.M.; Santed, R.; Valderas, J.M.; Ribera, A.; Domingo-Salvany, A.; et al. El Cuestionario de Salud SF-36 español: Una década de experiencia y nuevos desarrollos [The Spanish version of the Short Form 36 Health Survey: A decade of experience and new developments]. Gac. Sanit. 2005, 19, 135–150. [Google Scholar] [CrossRef]
- Arnanz, I.; Martínez-del-Valle, M.; Recio, S.; Blasco, R.; Benedito, T.; Sanz, M. Las escalas en la COVID-19 persistente. Med. Gen. Fam. 2021, 10, 79–84. [Google Scholar] [CrossRef]
- Chen, Y.M.; Cintrón, N.M.; Whitson, P.A. Long-term storage of salivary cortisol samples at room temperature. Clin. Chem. 1992, 38, 304. [Google Scholar] [CrossRef]
- Recuperación Exitosa de un Síndrome Regional Complejo a Través de la Electroterapia de Neuromodulación del Sistema Nervioso Autónomo. Available online: http://hdl.handle.net/10553/114084 (accessed on 19 October 2023).
- Tratamiento de la Neuralgia del Trigémino con Neuromodulación no Invasiva NESA: A Propósito de un Caso. Available online: http://hdl.handle.net/10553/115498 (accessed on 19 October 2023).
- Álamo, D.; Lledot-Amat, M.; Medina-Ramírez, R.I. Effects of non-invasive neuromodulation nesa® for the treatment of cerebral stroke sequelae. A case report. In Proceedings of the 17th ISPRM World Congress—ISPRM 2023, Cartagena, Colombia, 4–8 June 2023. [Google Scholar] [CrossRef]
- Caso Clínico de Neuromodulación Superficial Aplicada (NESA) en Pacientes con Esclerosis Múltiple. Available online: http://hdl.handle.net/10553/133551 (accessed on 19 October 2023).
- Teruel-Hernández, E.; López-Pina, J.A.; Souto-Camba, S.; Báez-Suárez, A.; Medina-Ramírez, R.; Gómez-Conesa, A. Improving Sleep Quality, Daytime Sleepiness, and Cognitive Function in Patients with Dementia by Therapeutic Exercise and NESA Neuromodulation: A Multicenter Clinical Trial. Int. J. Environ. Res. Public Health 2023, 20, 7027. [Google Scholar] [CrossRef] [PubMed]
- Soares, F.H.C.; Kubota, G.T.; Fernandes, A.M.; Hojo, B.; Couras, C.; Costa, B.V.; Lapa, J.D.D.S.; Braga, L.M.; Almeida, M.M.; Cunha, P.H.M.D.; et al. Prevalence and characteristics of new-onset pain in COVID-19 survivours, a controlled study. Eur. J. Pain 2021, 25, 1342–1354. [Google Scholar] [CrossRef] [PubMed]
- Fernández-de-Las-Peñas, C.; de-la-Llave-Rincón, A.I.; Ortega-Santiago, R.; Ambite-Quesada, S.; Gómez-Mayordomo, V.; Cuadrado, M.L.; Arias-Navalón, J.A.; Hernández-Barrera, V.; Martín-Guerrero, J.D.; Pellicer-Valero, O.J.; et al. Prevalence and risk factors of musculoskeletal pain symptoms as long-term post-COVID sequelae in hospitalized COVID-19 survivors: A multicenter study. Pain 2022, 163, e989–e996. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Del-Gaudio, A.; Vittori, A.; Bimonte, S.; Del-Prete, P.; Forte, C.A.; Cuomo, A.; De-Blasio, E. COVID-Pain: Acute and Late-Onset Painful Clinical Manifestations in COVID-19—Molecular Mechanisms and Research Perspectives. J. Pain Res. 2021, 14, 2403–2412. [Google Scholar] [CrossRef]
- Shanthanna, H.; Nelson, A.M.; Kissoon, N.; Narouze, S. The COVID-19 pandemic and its consequences for chronic pain: A narrative review. Anaesthesia 2022, 77, 1039–1050. [Google Scholar] [CrossRef]
- Plaut, S. “Long COVID-19” and viral “fibromyalgia-ness”: Suggesting a mechanistic role for fascial myofibroblasts (Nineveh, the shadow is in the fascia). Front. Med. 2023, 10, 952278. [Google Scholar] [CrossRef]
- Ursini, F.; Ciaffi, J.; Mancarella, L.; Lisi, L.; Brusi, V.; Cavallari, C.; D’Onghia, M.; Mari, A.; Borlandelli, E.; Faranda Cordella, J.; et al. Fibromyalgia: A new facet of the post-COVID-19 syndrome spectrum? Results from a web-based survey. RMD Open 2021, 7, e001735. [Google Scholar] [CrossRef]
- da-Silva, A.L.G.; Vieira, L.d.P.; Dias, L.S.; Prestes, C.V.; Back, G.D.; da Luz Goulart, C.; Arena, R.; Borghi-Silva, A.; Trimer, R. Impact of long COVID on the heart rate variability at rest and during deep breathing maneuver. Sci. Rep. 2023, 13, 22695. [Google Scholar] [CrossRef]
- Hernández, S.; Uribe, E.; Alfaro, J.M.; Campuzano, G.; Salazar, L.M. Cortisol. Mediciones de laboratorio y aplicación clínica. Med. Lab. 2016, 22, 147–163. [Google Scholar] [CrossRef]
- Raff, H. Utility of salivary cortisol measurements in Cushing’s syndrome and adrenal insufficiency. J. Clin. Endocrinol. Metab. 2009, 94, 3647–3655. [Google Scholar] [CrossRef]
- Bozovic, D.; Racic, M.; Ivkovic, N. Salivary cortisol levels as a biological marker of stress reaction. Med. Arch. 2013, 67, 374–377. [Google Scholar] [CrossRef] [PubMed]
- Weitzman, E.D.; Fukushima, D.; Nogeire, C.; Roffwarg, H.; Gallagher, T.F.; Hellman, L. Twenty-four hour pattern of the episodic secretion of cortisol in normal subjects. J. Clin. Endocrinol. Metab. 1971, 33, 14–22. [Google Scholar] [CrossRef]
- Carroll, T.; Raff, H.; Findling, J.W. Late-night salivary cortisol measurement in the diagnosis of Cushing’s syndrome. Nat. Clin. Pract. Endocrinol. Metab. 2008, 4, 344–350. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F.; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Iqbal, F.M.; Lam, K.; Sounderajah, V.; Clarke, J.M.; Ashrafian, H.; Darzi, A. Characteristics and predictors of acute and chronic post-COVID syndrome: A systematic review and meta-analysis. eClinicalMedicine 2021, 36, 100899. [Google Scholar] [CrossRef]
- Ostrowska, M.; Rzepka-Cholasińska, A.; Pietrzykowski, Ł.; Michalski, P.; Kosobucka-Ozdoba, A.; Jasiewicz, M.; Kasprzak, M.; Kryś, J.; Kubica, A. Effects of Multidisciplinary Rehabilitation Program in Patients with Long COVID-19: Post-COVID-19 Rehabilitation (PCR SIRIO 8) Study. J. Clin. Med. 2023, 12, 420. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, N.; Yamatoku, M.; Tsuchida, T.; Sato, H.; Yamaguchi, K. Effect of Repetitive Transcranial Magnetic Stimulation on Long Coronavirus Disease 2019 with Fatigue and Cognitive Dysfunction. Prog. Rehabil. Med. 2023, 8, 20230004. [Google Scholar] [CrossRef]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]

{kind=link}
| EG | CG | p-Value | |
|---|---|---|---|
| Age | 46.67 (10) | 45.43 (8.10) | 0.503 |
| Body weight (kg) | 61.71 (4.71) | 61.94 (3.39) | 0.612 |
| EG | CG | Time Effects | Time Effects per Group | Inter Groups | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| T0 | T1 | T2 | T0 | T1 | T2 | F; p-Value | η2 | F; p-Value | η2 | F; p-Value | |
| Cortisol (nmol/L) | 6.73 (3.98) 0.24 µg/dL | 12.07 (6.89) 0.43 µg/dL | 10.10 (5.31) 0.36 µg/dL | 7.27 (3.63) 0.26 µg/dL | 3.84 (3.29) 0.13 µg/dL | 15.14 (11.76) 0.54 µg/dL | 4.561; p = 0.019 | 0.246 | 5.751; p = 0.008 | 0.291 | 0.155; p = 0.699 |
| PPT C5–C6 (kg) | 1.43 (0.54) | 1.56 (0.68) | 1.87 (0.78) | 1.52 (0.88) | 1.74 (1.74) | 1.92 (1.76) | 3.902; p = 0.032 | 0.218 | 0.88; p = 0.916 | 0.006 | 0.040; p = 0.844 |
| PPT D5–D6 (kg) | 1.84 (0.84) | 2.04 (0.97) | 2.27 (0.91) | 2.18 (1.71) | 2.02 (1.66) | 2.37 (2.59) | 1.980; p = 0.157 | 0.124 | 0.555; p = 0.580 | 0.038 | 0.037; p = 0.851 |
| PPT tibial (kg) | 2.05 (1.04) | 2.33 (1.25) | 3.34 (1.26) | 2.30 (0.98) | 1.67 (1.02) | 2.13 (1.56) | 6.692; p = 0.04 | 0.323 | 6.186; p = 0.006 | 0.306 | 0.344; p = 0.064 |
| SDNN (ms) | 49.06 (29.31) | 149.52 (139.25) | 69.68 (58.33) | 84.65 (65.81) | 185.78 (161.57) | 42.26 (23.43) | 5.561; p = 0.005 | 0.319 | 0.579; p = 0.567 | 0.049 | 0.302; p = 0.021 |
| rMSSD (ms) | 48.91 (40.64) | 188.32 (196.00) | 75.15 (80.69) | 113.01 (106.69) | 243.62 (226.61) | 71.00 (68.45) | 6.334; p = 0.005 | 0.213 | 0.389; p = 0.682 | 0.027 | 0.719; p = 0.411 |
| HR (bpm) | 80.56 (9.20) | 89.56 (20.70) | 82.22 (10.69) | 71.57 (11.25) | 78.86 (37.98) | 77.29 (10.93) | 0.796; p = 0.461 | 0.054 | 0.105; p = 0.901 | 0.007 | 1.871; p = 0.193 |
| PSQI | 12.44 (5.92) | 12.00 (4.69) | 9.22 (6.04) | 11.14 (2.67) | 8.14 (2.48) | 8.14 (3.29) | 9.044; p ≤ 0.001 | 0.392 | 2.218; p = 0.128 | 0.137 | 0.926; p = 0.352 |
| MFIS | 60.67 (18.36) | 55.11 (21.06) | 51.78 (22.94) | 62.71 (9.41) | 54.57 (13.74) | 51.99 (16.39) | 7.526; p = 0.002 | 0.350 | 0.168; p = 0.846 | 0.012 | 0.001; p = 0.978 |
| EG | CG | Time Effects | Time Effects per Group | Inter Groups | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SF-36 | T0 | T1 | T2 | T0 | T1 | T2 | F; p-Value | η2 | F; p-Value | η22 | F; p-Value |
| Physical function | 41.22 (24.05) | 45.00 (25.62) | 50.49 (28.89) | 62.86 (24.64) | 65.71 (21.10) | 63.75 (20.06) | 0.840; p = 0.442 | 0.057 | 0.0664; p = 0.523 | 0.045 | 2.608; p = 0.129 |
| Physical role | 0.00 (0.00) | 25.00 (37.50) | 25.00 (35.36) | 17.85 (37.40) | 17.86 (37.40) | 9.76 (19.01) | 1.445; p = 0.253 | 0.094 | 2.642; p = 0.089 | 0.159 | 0.014; 0.909 |
| Body pain | 22.44 (11.76) | 38.44 (23.56) | 36.00 (21.82) | 28.57 (20.59) | 43.14 (23.92) | 50.48 (20.67) | 6.630; p = 0.004 | 0.321 | 0.501; p = 0.611 | 0.035 | 1.001; p = 0.334 |
| General health | 26.11 (12.18) | 23.89 (11.67) | 28.78 (12.23) | 34.29 (12.67) | 33.57 (12.20) | 33.19 (14.23) | 0.753; p = 0.480 | 0.051 | 1.053; p = 0.362 | 0.070 | 1.335; p = 0.267 |
| Vitality | 25.00 (19.84) | 29.44 (24.55) | 31.67 (10.16) | 15.00 (14.43) | 32.85 (14.10) | 24.81 (14.65) | 4.156; p = 0.026 | 0.229 | 1.528; p = 0.234 | 0.098 | 0.291; p = 0.598 |
| Social function | 34.72 (32.24) | 44.44 (33.14) | 47.22 (39.41) | 42.86 (26.86) | 42.86 (35.25) | 51.67 (39.81) | 1.039; p = 0.367 | 0.069 | 0.220; p = 0.804 | 0.015 | 0.057; p = 0.814 |
| Emotional role | 63.00 (48.43) | 51.86 (44.49) | 48.15 (47.46) | 62.00 (44.85) | 57.16 (41.78) | 60.00 (40.55) | 0.386; p = 0.684 | 0.027 | 0.177; p = 0.839 | 0.012 | 0.081; p = 0.780 |
| Mental health | 51.11 (19.98) | 50.67 (29.25) | 52.88 (24.25) | 59.43 (10.18) | 64.57 (17.26) | 63.35 (19.44) | 0.300; p = 0.743 | 0.021 | 0.257; p = 0.775 | 0.018 | 1.222; p = 0.288 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melián-Ortíz, A.; Zurdo-Sayalero, E.; Perpiñá-Martínez, S.; Delgado-Lacosta, A.; Jiménez-Antona, C.; Fernández-Carnero, J.; Laguarta-Val, S. Superficial Neuromodulation in Dysautonomia in Women with Post-COVID-19 Condition: A Pilot Study. Brain Sci. 2025, 15, 510. https://doi.org/10.3390/brainsci15050510
Melián-Ortíz A, Zurdo-Sayalero E, Perpiñá-Martínez S, Delgado-Lacosta A, Jiménez-Antona C, Fernández-Carnero J, Laguarta-Val S. Superficial Neuromodulation in Dysautonomia in Women with Post-COVID-19 Condition: A Pilot Study. Brain Sciences. 2025; 15(5):510. https://doi.org/10.3390/brainsci15050510
Chicago/Turabian StyleMelián-Ortíz, Alberto, Eduardo Zurdo-Sayalero, Sara Perpiñá-Martínez, Antonio Delgado-Lacosta, Carmen Jiménez-Antona, Josué Fernández-Carnero, and Sofía Laguarta-Val. 2025. "Superficial Neuromodulation in Dysautonomia in Women with Post-COVID-19 Condition: A Pilot Study" Brain Sciences 15, no. 5: 510. https://doi.org/10.3390/brainsci15050510
APA StyleMelián-Ortíz, A., Zurdo-Sayalero, E., Perpiñá-Martínez, S., Delgado-Lacosta, A., Jiménez-Antona, C., Fernández-Carnero, J., & Laguarta-Val, S. (2025). Superficial Neuromodulation in Dysautonomia in Women with Post-COVID-19 Condition: A Pilot Study. Brain Sciences, 15(5), 510. https://doi.org/10.3390/brainsci15050510