
Methodological Approaches to Pain Memory Assessment in Chronic Pain: A Scoping Review


Abstract
1. Introduction
Objective and Research Question
2. Methods
2.1. Design
2.2. Search Strategy
2.3. Study Selection
2.4. Data Extraction
3. Results
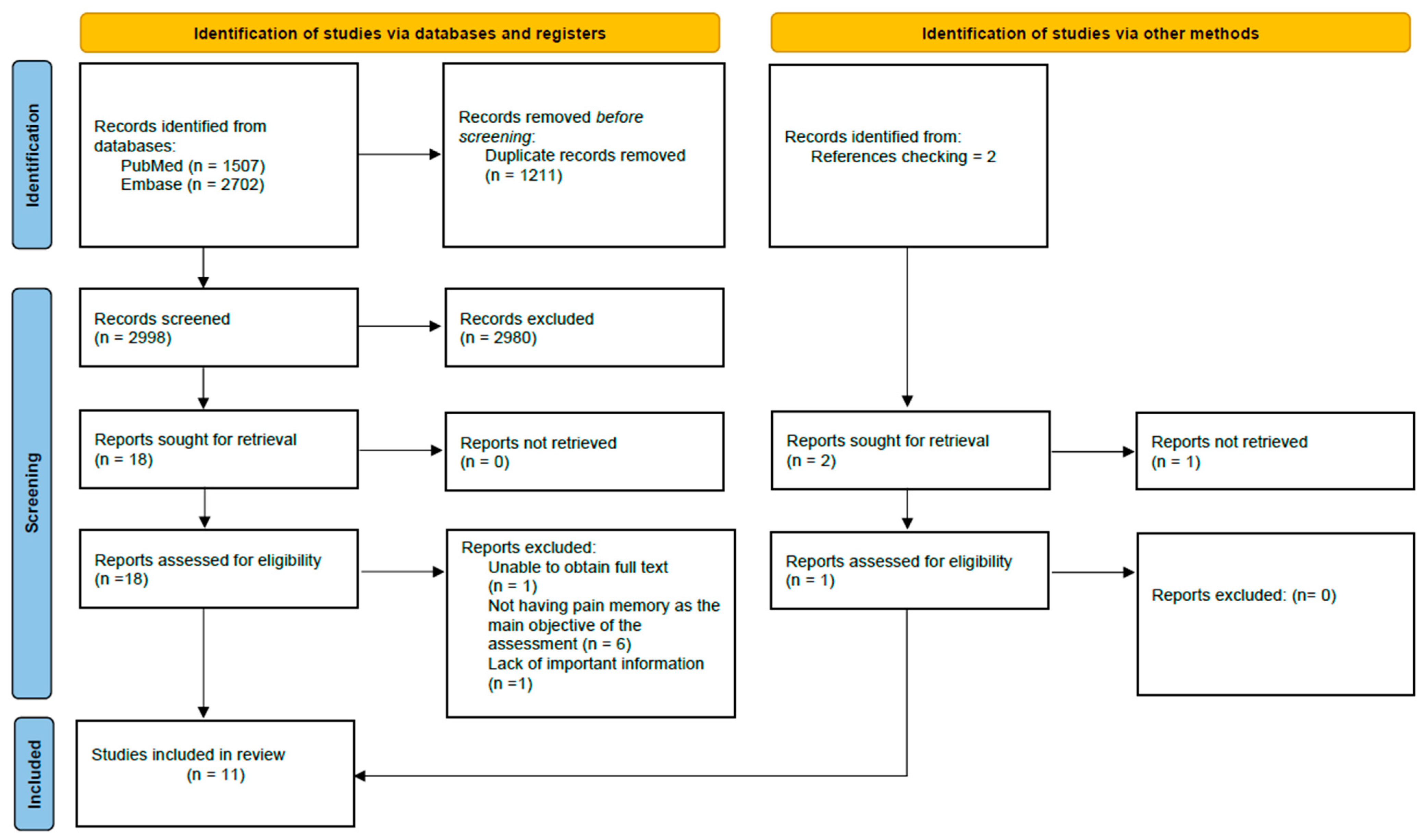
3.1. Search Results
3.2. Data Items Results
3.2.1. Sample
3.2.2. Association Between Studies
3.2.3. Outcomes
3.2.4. Characteristics of the Interventions
3.2.5. Characteristics of the Pain Recall
3.2.6. Summary of Findings
4. Discussion
- The sample consists exclusively of adults with chronic pain.
- Pain memory assessment is a primary objective of the study.
- The evaluation and recall of pain intensity and/or pain unpleasantness are pain memory outcomes.
- The studies follow one of two methodological approaches: assessing pain memory in the context of a specific treatment, or assessing pain memory using daily measures.
4.1. Recall Characteristics and Methodological Challenges
4.2. Research Implications
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Squire, L.R. Memory and brain systems: 1969–2009. J. Neurosci. 2009, 29, 12711–12716. [Google Scholar] [CrossRef] [PubMed]
- Merskey, H. Pain, learning and memory. J. Psychosom. Res. 1975, 19, 319–324. [Google Scholar] [CrossRef]
- Baddeley, A. Working memory. Science 1992, 255, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Albanese, M.C.; Duerden, E.G.; Rainville, P.; Duncan, G.H. Memory traces of pain in human cortex. J. Neurosci. 2007, 27, 4612–4620. [Google Scholar] [CrossRef] [PubMed]
- Jantsch, H.H.F.; Gawlitza, M.; Geber, C.; Baumgärtner, U.; Krämer, H.H.; Magerl, W.; Treede, R.D.; Birklein, F. Explicit episodic memory for sensory-discriminative components of capsaicin-induced pain: Immediate and delayed ratings. Pain 2009, 143, 97–105. [Google Scholar] [CrossRef]
- Tasmuth, T.; Von Smitten, K.; Hietanen, P.; Kataja, M.; Kalso, E. Pain and other symptoms after different treatment modalities of breast cancer. Ann. Oncol. 1995, 6, 453–459. [Google Scholar] [CrossRef]
- Mansour, A.R.; Farmer, M.A.; Baliki, M.N.; Apkarian, A.V. Chronic pain: The role of learning and brain plasticity. Restor. Neurol. Neurosci. 2014, 32, 129–139. [Google Scholar] [CrossRef]
- Apkarian, A.V. Pain perception in relation to emotional learning. Curr. Opin. Neurobiol. 2008, 18, 464–468. [Google Scholar] [CrossRef]
- Kahneman, D.; Fredrickson, B.L.; Schreiber, C.A.; Redelmeier, D.A. When More Pain Is Preferred to Less: Adding a Better End. Psychol. Sci. 1993, 4, 401–405. [Google Scholar] [CrossRef]
- Dick, B.D.; Rashiq, S. Disruption of attention and working memory traces in individuals with chronic pain. Anesth. Analg. 2007, 104, 1223–1229. [Google Scholar] [CrossRef]
- Söderfjell, S. Musculoskeletal Pain, Memory, and Aging: Cross-Sectional and Longitudinal Findings. Doctoral Dissertation, Department of Psychology, Umeå University, Umeå, Sweden, 2005. [Google Scholar]
- La Touche, R.; Paris-Alemany, A.; Suso-Martí, L.; Martín-Alcocer, N.; Mercado, F.; Cuenca-Martínez, F. Pain memory in patients with chronic pain versus asymptomatic individuals: A prospective cohort study. Eur. J. Pain 2020, 24, 1741–1751. [Google Scholar] [CrossRef] [PubMed]
- Mcgorry, R.W.; Webster, B.S.; Snook, S.H.; Hsiang1, S.M. Accuracy of Pain Recall in Chronic and Recurrent Low Back Pain. J. Occup. Rehabil. 1999, 9, 169–178. [Google Scholar] [CrossRef]
- Rode, S.; Salkovskis, P.M.; Jack, T. An experimental study of attention, labelling and memory in people suffering from chronic pain. Pain 2001, 94, 193–203. [Google Scholar] [CrossRef]
- Schoth, D.E.; Radhakrishnan, K.; Liossi, C. A systematic review with subset meta-analysis of studies exploring memory recall biases for pain-related information in adults with chronic pain. Pain Rep. 2020, 5, e816. [Google Scholar] [CrossRef]
- Bruck, M.; Ceci, S.J.; Francoeur, E.; Barr, R. “I Hardly Cried When I Got My Shot!” Influencing Children’s Reports about a Visit to. Child Dev. 1995, 66, 193–208. [Google Scholar]
- Van den Brink, M.; Bandell-Hoekstra, E.N.; Abu-Saad, H.H. The occurrence of recall bias in pediatric headache: A comparison of questionnaire and diary data. Headache 2001, 41, 11–20. [Google Scholar] [CrossRef]
- Koyama, Y.; Koyama, T.; Kroncke, A.P.; Coghill, R.C. Effects of stimulus duration on heat induced pain: The relationship between real-time and post-stimulus pain ratings. Pain 2004, 107, 256–266. [Google Scholar] [CrossRef]
- Feine, J.S.; Lavigne, G.J.; Dao, T.T.T.; Morin, C.; Lund, J.P. Memories of chronic pain and perceptions of relief. Pain 1998, 77, 137–141. [Google Scholar] [CrossRef]
- Gavaruzzi, T.; Carnaghi, A.; Lotto, L.; Rumiati, R.; Meggiato, T.; Polato, F.; De Lazzari, F. Recalling pain experienced during a colonoscopy: Pain expectation and variability. Br. J. Health Psychol. 2010, 15, 253–264. [Google Scholar] [CrossRef]
- Atlas, L.Y.; Wager, T.D. How expectations shape pain. Neurosci. Lett. 2012, 520, 140–148. [Google Scholar] [CrossRef]
- Anunciação, L.; Portugal, A.C.; Landeira-Fernandez, J.; Bajcar, E.A.; Bąbel, P. The Lighter Side of Pain: Do Positive Affective States Predict Memory of Pain Induced by Running a Marathon? J. Pain Res. 2022, 15, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Peerdeman, K.J.; van Laarhoven, A.I.M.; Peters, M.L.; Evers, A.W.M. An integrative review of the influence of expectancies on pain. Front. Psychol. 2016, 7, 1270. [Google Scholar] [CrossRef] [PubMed]
- Bryant, R.A. Memory for pain and affect in chronic pain patients. Pain 1993, 54, 347–351. [Google Scholar] [CrossRef]
- Jamison, R.N.; Sbrocco, T.; Parris, W.C.V. The influence of physical and psychosocial factors on accuracy of memory for pain in chronic pain patients. Pain 1989, 37, 289–294. [Google Scholar] [CrossRef]
- Lefebvre, J.C.; Keefe, F.J. Memory for pain: The relationship of pain catastrophizing to the recall of daily rheumatoid arthritis pain. Clin. J. Pain 2002, 18, 56–63. [Google Scholar] [CrossRef]
- Lefebvre, J.C.; Keefe, F.J. The effect of neuroticism on the recall of persistent low-back pain and perceived activity interference. J. Pain 2013, 14, 948–956. [Google Scholar] [CrossRef]
- Linton, S.J.; Melin, L. The accuracy of remembering chronic pain. Pain 1982, 13, 281–285. [Google Scholar] [CrossRef]
- Linton, S.J. Memory for chronic pain intensity: Correlates of accuracy. Percept. Mot. Ski. 1991, 72 Pt 2, 1091–1095. [Google Scholar] [CrossRef]
- Porzelius, J. Memory for pain after nerve-block injections. Clin. J. Pain 1995, 11, 112–120. [Google Scholar] [CrossRef]
- Raselli, C.; Broderick, J.E. The association of depression and neuroticism with pain reports: A comparison of momentary and recalled pain assessment. J. Psychosom. Res. 2007, 62, 313–320. [Google Scholar] [CrossRef]
- Stone, A.A.; Broderick, J.E.; Shiffman, S.S.; Schwartz, J.E. Understanding recall of weekly pain from a momentary assessment perspective: Absolute agreement, between- and within-person consistency, and judged change in weekly pain. Pain 2004, 107, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A.; Schwartz, J.E.; Broderick, J.E.; Shiffman, S.S. Variability of momentary pain predicts recall of weekly pain: A consequence of the peak (or salience) memory heuristic. Personal. Soc. Psychol. Bull. 2005, 31, 1340–1346. [Google Scholar] [CrossRef] [PubMed]
- Smith, W.B.; Safer, M.A. Effects of present pain level on recall of chronic pain and medication use. Pain 1993, 55, 355–361. [Google Scholar] [CrossRef] [PubMed]
- Stone, A.A.; Broderick, J.E.; Schwartz, J.E.; Shiffman, S.; Litcher-Kelly, L.; Calvanese, P. Intensive momentary reporting of pain with an electronic diary: Reactivity, compliance, and patient satisfaction. Pain 2003, 104, 343–351. [Google Scholar] [CrossRef]
- Bajcar, E.A.; Swędzioł, W.; Wrześniewski, K.; Blecharz, J.; Bąbel, P. The Effects of Pain Expectancy and Desire for Pain Relief on the Memory of Pain in Half Trail Marathon Runners. J. Pain Res. 2022, 15, 181–191. [Google Scholar] [CrossRef]
- Gedney, J.J.; Logan, H.; Baron, R.S. Predictors of short-term and long-term memory of sensory and affective dimensions of pain. J. Pain 2003, 4, 47–55. [Google Scholar] [CrossRef]
- Bąbel, P.; Bajcar, E.A.; Śmieja, M.; Adamczyk, W.; Świder, K.; Kicman, P.; Lisińska, N. Pain begets pain. When marathon runners are not in pain anymore, they underestimate their memory of marathon pain––A mediation analysis. Eur. J. Pain 2018, 22, 800–809. [Google Scholar] [CrossRef]
- Kent, G. Memory of dental pain. Pain 1985, 21, 187–194. [Google Scholar] [CrossRef]
- Wauters, A.; Noel, M.; Van Ryckeghem, D.M.L.; Soltani, S.; Vervoort, T. The Moderating Role of Attention Control in the Relationship Between Pain Catastrophizing and Negatively-Biased Pain Memories in Youth with Chronic Pain. J. Pain 2021, 22, 1303–1314. [Google Scholar] [CrossRef]
- Haas, M.; Nyiendo, J.; Aickin, M. One-year trend in pain and disability relief recall in acute and chronic ambulatory low back pain patients. Pain 2002, 95, 83–91. [Google Scholar] [CrossRef]
- Jensen, M.P.; Tomé-Pires, C.; Solé, E.; Racine, M.; Castarlenas, E.; de la Vega, R.; Miró, J. Assessment of pain intensity in clinical trials: Individual ratings vs composite scores. Pain Med. 2015, 16, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.E.; Schwartz, J.E.; Vikingstad, G.; Pribbernow, M.; Grossman, S.; Stone, A.A. The accuracy of pain and fatigue items across different reporting periods. Pain 2008, 139, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Scholz, O.B. Was leisten Schmerztagebücher? Vorzüge und Grenzen ihrer Anwendung unter besonderer Berücksichtigung einzelfallbezogener Auswertung. Schmerz 1995, 9, 107–116. [Google Scholar] [CrossRef] [PubMed]
- De Wit, R.; van Dam, F.; Hanneman, M.; Zandbelt, L.; van Buuren, A.; van der Heijden, K.; Leenhouts, G.; Loonstra, S.; Abu-Saad, H.H. Evaluation of the use of a pain diary in chronic cancer pain patients at home. Pain 1999, 79, 89–99. [Google Scholar] [CrossRef]
- Bąbel, P. Memory of pain and affect associated with migraine and non-migraine headaches. Memory 2015, 23, 864–875. [Google Scholar] [CrossRef]
- Bąbel, P.; Krzemień, M. Memory of dental pain induced by tooth restoration. Stud Psychol. 2015, 53, 5–17. [Google Scholar]
- Gedney, J.J.; Logan, H. Memory for stress-associated acute pain. J. Pain 2004, 5, 83–91. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMAScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]

{kind=link}
| Terms | Boolean Operators | Filters |
|---|---|---|
| Memory, delay, recall, chronic pain, rheumatoid, osteoarthritis. | AND, OR | Age: adults Language: English Species: humans Others: Title/Abstract |
| Study | Sample | Association with Other Studys | Outcomes | Inclusion of Specific Treatment | Intervention | Recall |
|---|---|---|---|---|---|---|
| Bryant 1993 [24] | Chronic pain patients (n = 40): -Females: 19 -Males: 21 -Average age: 43.9 -Diagnoses: CLBP. | No | Pain memory outcomes -Pain intensity: VAS -Pain unpleasantness: VAS Other outcomes -Anxiety: VAS -Depression: VAS | Yes -Pain management program which included mainly CBT techniques. | Initial assessment: Before starting the treatment, each participant was asked to assess pain intensity, pain unpleasantness, anxiety, and depression, using a VAS for each of the outcomes. Treatment program: It was carried out for 6 weeks, with a weekly session lasting 2 h. Final assessment: At the beginning of the last session of the treatment, each participant was asked to assess pain intensity, pain unpleasantness, anxiety, and depression, using a VAS for each of the outcomes. Recall assessment: At the end of the last session, they were asked to recall the intensity of pain, unpleasantness of pain, anxiety, and depression they had before starting treatment, using a VAS scale for each of the outcomes. | At the end of the last session (6 weeks after the first assessment), the participants were asked to recall the intensity of pain, unpleasantness of pain, anxiety, and depression they had before starting treatment, using a VAS for each of the outcomes. |
| Jamison et al., 1989 [25] | Chronic pain patients (n = 93): -Females: 54 -Males: 39 -Average age: 41.6 -Diagnoses: chronic musculoskeletal pain and headache. | No | Pain memory outcomes -Pain intensity: 11-point scale (similar to the classic NRS) Other outcomes -Pain characteristics: NR -Psychosocial outcomes: NR -Physical changes: NR -Perceived impact of pain on daily activities: NR -Emotional distress: SCL-90 | No | Baseline assessment: Participants filled in a baseline questionnaire (which includes an assessment of pain characteristics, psychosocial outcomes, physical changes, perceived impact of pain on daily activities and emotional distress). Evaluation week: Participants monitored their pain every hour for one week (while awake) using pain cards (contained within a paper diary) which included pain assessment on a scale a 11-point scale, where 0 was no pain and 10 was the worst possible pain. Recall session: One day after the evaluation week was completed, the patients were asked to give their current pain intensity and to recall their average pain for four specific times during the day (8.00 a.m., 12.00 p.m., 6.00 p.m., and 10.00 p.m.) for the previous week. | One day after the evaluation week was completed, the patients were asked to recall their average pain for 4 specific times during the day (8.00 a.m., 12.00 p.m., 6.00 p.m. and 10.00 p.m.) for the previous week, using the 11-point scale. |
| Lefebvre and Keefe 2002 [26] | Chronic pain patients (n = 45): -Females: 37 -Males: 8 -Average age: 54.5 -Diagnoses: rheumatoid arthritis. | No | Pain memory outcomes -Pain intensity: VAS Other outcomes -Pain coping strategies (catastrophism): CSQ | No | Diary phase: Participants used a paper pain diary for 30 days. Each day, the participant recorded in the diary his average pain for that day using a VAS. Laboratory recall phase: Participants recalled their pain intensity using an OPRA. In addition, patients’ current pain intensity (using a VAS) and pain coping strategies (using the CSQ) were also assessed. | The exact timing of the recall is not reported. Recall of the intensity of the patient’s pain during the diary phase was carried out using an OPRA form. |
| Lefebvre and Keefe 2013 [27] | Chronic pain patients (n = 70): -Females: 40 -Males: 30 -Average age: 43.9 -Diagnoses: CLBP. | No | Pain memory outcomes -Pain intensity: VAS -Pain unpleasantness: VAS Other outcomes -Perceived activity interference due to pain: VAS -Usual activity interference due to pain: 11-point scale. -Depression: BDI-I. -Neuroticism: Neuroticism subscale of the NEO-PI-R. | No | Orientation phase: Participants scored on baseline measures of usual activity pain interference, depression, and neuroticism. Diary phase: Participants used a paper pain diary for 15 days, in which at the end of each day they wrote down the data corresponding to the intensity of the pain, unpleasantness of the pain, and perceived activity interference due to pain during that day. Laboratory recall phase: Participants recalled pain intensity, pain unpleasantness, and perceived activity interference due to pain using one OPRA for each outcome mentioned. In addition, an assessment of current pain intensity and current pain unpleasantness was also carried out (using a VAS). | The exact timing of the recall is not reported. Recall of the pain unpleasantness and pain intensity that the patient had during the diary phase was carried out using an OPRA form for each of the outcomes mentioned. |
| Linton and Melin 1982 [28] | Chronic pain patients (n = 12): -Females: 6 -Males: 6 -Average age: 48.0 -Diagnoses: presence of chronic pain. | No | Pain memory outcomes -Pain intensity: 0–100-point scale (similar to the classic VAS) | Yes -Pain treatment program. | Initial assessment: Before starting the treatment, each participant was asked to assess pain intensity using a 0–100-point scale, in which 0 was no pain and 100 was terrible, excruciating pain. Treatment phase: Patients were given a series of pain rating sheets and instructed to fill them out over a two-week period. During treatment, patients were periodically asked to rate their pain. It is important to mention that these scores were not related to the pain memory assessment. Recall assessment: Once the participant was discharged, they were asked to recall their baseline pain using the same scale. | Once the participant was discharged they were asked to recall their baseline pain intensity using the same scale. Not all participants underwent the same treatment time before being discharged, so recall times were not always the same for all. Therefore, the recall time was between week 3 and week 11 after the baseline measures. |
| Linton 1991 [29] | Chronic pain patients (n = 61): -Females: 61 -Males: 0 -Average age: 43.0 -Diagnoses: CLBP | No | Pain memory outcomes -Pain intensity: VAS Other outcomes -Depression: BDI -Functional level: ADLS -Current pain: VAS -Sleep quality: VAS -Helplessness: AHI | No | Evaluation week: Participants rated their pain intensity using a VAS (included in a paper diary) three times per day for one week. Recall session: 18 months after the evaluation week, the participants were asked to remember how intense their pain was during the evaluation week. | The pain intensity was recalled 18 months after the evaluation week using a VAS. |
| Porzelius 1995 [30] | Chronic pain patients (n = 49): -Females: 32 -Males: 17 -Average age: 50.0 -Diagnoses: presence of chronic pain. | No | Pain memory outcomes -Pain intensity: 11-point NRS Other outcomes -Qualitative dimensions of pain: MPQ-SF -Hypochondriasis and hysteria: sub-scales 1 and 3 of the MMPI-2 -Pain coping strategies (catastrophism): CSQ -Psychological distress: MSPQ -Functional activity: FASQ | Yes -Nerve-block injections | Initial evaluation (before the nerve block): Participants filled in psychological self-report questionnaires (MPQ-SF, MMPI-2, CSQ, MSPQ, and FASQ) and rated their pain at that time using the 11-point NRS. First evaluation after the nerve block: It was performed 30–60 min after injection, as this is the time it takes for the nerve block to produce the analgesic effect. What was assessed at this point was the intensity of pain experienced at the time by the patient using the 11-point NRS. Second evaluation after the nerve block: It was carried out 2 days after the nerve block. Both current pain and pain recall after the nerve block were assessed using the 11-point NRS. Third evaluation after nerve block: It was carried out 2 weeks after the nerve block. Both current pain and pain recall after the nerve block were assessed using the 11-point NRS. | The recall of pain intensity experienced just after the nerve block was carried out 2 days and 2 weeks after the injection, using the 11-point NRS in both cases. |
| Raselli and Broderick 2007 [31] | Chronic pain patients (n = 66): -Females: 56 -Males: 10 -Average age: 51.0 -Diagnoses: fibromyalgia, osteoarthritis, rheumatoid arthritis, and ankylosing spondylitis. | Yes (Stone et al., 2004 [32], and Stone et al., 2005 [33]) | Pain memory outcomes -Pain intensity: VAS -Pain unpleasantness: VAS Other outcomes -Depression: BDI-II -Neuroticism: NEO-PI -Judged change in pain: 5-point scale [ranging from +2 (much worse) to −2 (much better)] | No | Visit 1: Participants filled in a baseline questionnaire (which includes depression and neuroticism assessments) and the weekly pain questionnaire (which includes pain intensity, pain unpleasantness, and judged change in pain assessments). Visit 2: Participants filled in the weekly pain questionnaire (includes pain intensity, pain unpleasantness, and judged change in pain assessments). During the 7 days between Visit 2 and Visit 3: Participants used an ED for 7 days. The ED was evaluated once a day, when the patient was in pain, the intensity of the pain, and the unpleasantness of the pain (using a VAS for each one of the outcomes). This evaluation is called EMA. Visit 3: Participants filled in the weekly pain questionnaire (which included pain intensity, pain unpleasantness, and judged change in pain assessments). During the 7 days between Visit 2 and Visit 4: Participants used an ED for 7 days. The ED was evaluated once a day, when the patient was in pain, the intensity of the pain, and the unpleasantness of the pain (using a VAS for each one of the outcomes). This evaluation is called EMA. Visit 4: Participants filled in the weekly pain questionnaire (which includes pain intensity, pain unpleasantness, and judged change in pain assessments). | 1st: At visit 3, recall of the pain intensity and pain unpleasantness of the last 7 days (using the VAS included in the weekly pain questionnaire) was performed. 2nd: At visit 4, recall of the pain intensity and pain unpleasantness of the last 7 days (using the VAS included in the weekly pain questionnaire) was performed. At visits 1 and 2, the intensity of pain and the unpleasantness of pain over the past 7 days were also assessed (using the VAS included in the weekly pain questionnaire), but since the pain scores during those 7 days were not evaluated (as they were between visits 2 and 3, and 3 and 4), it is not considered as a recall associated with the pain memory assessment. |
| Smith and Safer 1993 [34] | Chronic pain patients (n = 31): -Females: 23 -Males: 8 -Average age: NR -Diagnoses: presence of chronic pain. | No | Pain memory outcomes -Pain intensity: VAS Other outcomes -Use of medication -Meal registration -Sleep/awake record | Yes -Physical therapy | Use of an ED for one week: For one week, the participant used an ED where he recorded every change in the intensity of his pain (using a VAS), every time he took pain medication, every time he ate, every time he went to sleep, and every time he woke up. Control group: Participants assigned to this group were scheduled one week after starting to use the ED. In this session, the participants were asked to recall the amount of pain medication used the previous day and during the previous week, and the changes and pain levels of the previous day and the previous week. PT group: Participants assigned to this group were scheduled to be seen one week after starting to use the ED. At this appointment, they were first given a physical therapy session, and then asked to recall the amount of pain medication used the previous day and during the previous week and the changes and pain levels of the previous day and the previous week. | One week after starting to use the ED, changes in pain intensity and pain levels from both the previous day and the previous week were recalled (for both variables, the VAS scale was used). Depending on the group to which the participant belonged, this recall could be carried out after a physical therapy session. |
| Stone et al., 2004 [32] | Chronic pain patients (n = 68): -Females: NR -Males: NR -Average age: NR -Diagnoses: fibromyalgia, rheumatoid arthritis, osteoarthritis (of the hip or knee), and ankylosing spondylitis. | Yes (Raselli and Broderick, 2007 [31], and Stone et al., 2005 [33]) | Pain memory outcomes -Pain intensity: VAS Other outcomes -Anxiety: NR -Depression: NR -Health: NR -Quality of life: NR -Judged change in pain: 5-point scale [ranging from +2 (much worse) to −2 (much better)] | No | Visit 1: Participants filled in a baseline questionnaire (which included anxiety, depression, health, and quality of life assessments) and the weekly pain questionnaire (which includes pain intensity and judged change in pain assessments). Visit 2: Participants filled in the weekly pain questionnaire (which included pain intensity assessment). During the 7 days between Visit 2 and Visit 3: The ED was evaluated once a day, randomly, and indicated by a beep, the intensity of the pain was recorded (using a VAS). This evaluation is called EMA. If the participant had no pain at the time of the evaluation, the pain intensity was scored as 0. Visit 3: Participants filled in the weekly pain questionnaire (which includes pain intensity assessment). During the 7 days between Visit 3 and Visit 4: The ED was evaluated once a day, randomly, and indicated by a beep, the intensity of the pain (using a VAS) was recorded. This evaluation is called EMA. If the participant had no pain at the time of the evaluation, the pain intensity was scored as 0. Visit 4: Participants filled in the weekly pain questionnaire (which includes pain intensity assessment). | 1st: At visit 3, recall of the pain intensity of the last 7 days (using the VAS included in the weekly pain questionnaire) was performed. 2nd: At visit 4, recall of the pain intensity of the last 7 days (using the VAS included in the weekly pain questionnaire) was performed. At visits 1 and 2, the intensity of pain and the unpleasantness of pain over the past 7 days were also assessed (using the VAS included in the weekly pain questionnaire), but since the pain scores during those 7 days were not evaluated (as they were between visits 2 and 3, and 3 and 4), it is not considered as a recall associated with the pain memory assessment. |
| Stone et al., 2005 [33] | Chronic pain patients (n = 68): -Females: NR -Males: NR -Average age: NR -Diagnoses: fibromyalgia, rheumatoid arthritis, osteoarthritis (of the hip or knee), and ankylosing spondylitis. | Yes (Raselli and Broderick, 2007 [31] and Stone et al., 2004 [32]) | Pain memory outcomes -Pain intensity: VAS Other outcomes -Anxiety: NR -Depression: NR -Health: NR -Quality of life: NR | No | Visit 1: Participants filled in a baseline questionnaire (which included anxiety, depression, health, and quality of life assessments) and the weekly pain questionnaire (which included pain intensity assessment). Visit 2: Participants filled in the weekly pain questionnaire (which included pain intensity assessment). During the 7 days between Visit 2 and Visit 3: Participants used an ED for 7 days. The ED was evaluated once a day, randomly, and indicated by a beep, the intensity of the pain (using a VAS) was recorded. This evaluation is called EMA. If the participant had no pain at the time of the evaluation, the pain intensity was scored as 0. Visit 3: Participants filled in the weekly pain questionnaire (which included pain intensity assessment). During the 7 days between Visit 3 and Visit 4: Participants used an ED for 7 days. The ED was evaluated once a day, randomly, and indicated by a beep, the intensity of the pain (using a VAS) was recorded. This evaluation is called EMA. If the participant had no pain at the time of the evaluation, the pain intensity was scored as 0. Visit 4: Participants filled in the weekly pain questionnaire (which includes pain intensity assessment). | 1st: At visit 3, recall of the pain intensity of the last 7 days (using the VAS included in the weekly pain questionnaire) was performed. 2nd: At visit 4, recall of the pain intensity of the last 7 days (using the VAS included in the weekly pain questionnaire) was performed. At visits 1 and 2, the intensity of pain and the unpleasantness of pain over the past 7 days were also assessed (using the VAS included in the weekly pain questionnaire), but since the pain scores during those 7 days were not evaluated (as they are between visits 2, and 3 and 3 and 4), it is not considered as a recall associated with the pain memory assessment. |
| Sample Characteristics | Outcomes | Instruments | Intervention Approach | Recall Characteristics |
|---|---|---|---|---|
| -Adults: 11/11 -Chronic pain patients: 11/11 | Pain memory outcomes: -Pain intensity: 11/11 -Pain unpleasantness: 3/11 Non-pain memory outcomes: -Pain-related outcomes: 6/11 -Psychosocial outcomes: 9/11 -Other outcomes: 6/11 | Pain memory outcomes assessment tools: -VAS or similar: 9/11 -NRS or similar: 2/11 -OPRA: 2/11 Daily recollection tools: -ED: 4/11 -PD: 4/11 | -Pain memory assessment focusing on the application of a specific treatment: 4/11 -Pain memory assessment focusing on the collection of daily measures: 8/11 | Regarding intervention: -During the intervention: 3/11 -Post intervention: 11/11 Recall time: <24 h: 3/11 −24–48 h: 4/11 48 h–1 week: 1/11 2 weeks–1 month: 1/11 >1 month: 1/11 NR: 2/11 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forner-Álvarez, C.; Cuenca-Martínez, F. Methodological Approaches to Pain Memory Assessment in Chronic Pain: A Scoping Review. Brain Sci. 2025, 15, 308. https://doi.org/10.3390/brainsci15030308
Forner-Álvarez C, Cuenca-Martínez F. Methodological Approaches to Pain Memory Assessment in Chronic Pain: A Scoping Review. Brain Sciences. 2025; 15(3):308. https://doi.org/10.3390/brainsci15030308
Chicago/Turabian StyleForner-Álvarez, Carlos, and Ferran Cuenca-Martínez. 2025. "Methodological Approaches to Pain Memory Assessment in Chronic Pain: A Scoping Review" Brain Sciences 15, no. 3: 308. https://doi.org/10.3390/brainsci15030308
APA StyleForner-Álvarez, C., & Cuenca-Martínez, F. (2025). Methodological Approaches to Pain Memory Assessment in Chronic Pain: A Scoping Review. Brain Sciences, 15(3), 308. https://doi.org/10.3390/brainsci15030308