
Discharge Against Medical Advice Among Schizophrenia Patients in Germany: A Multicenter Cross-Sectional Study



Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
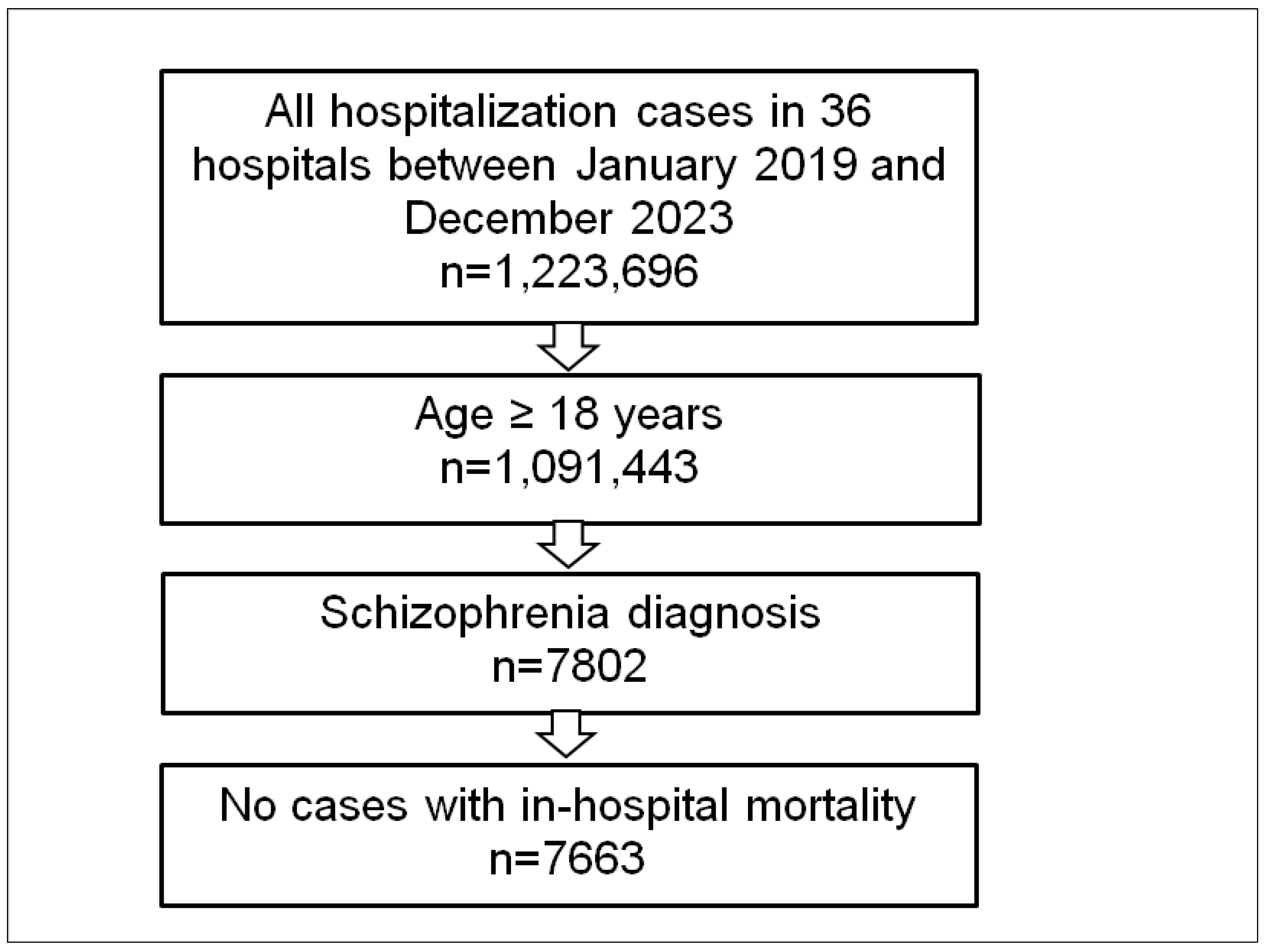
2.2. Study Population and Outcome
2.3. Statistical Analyses
3. Results
3.1. Baseline Characteristics
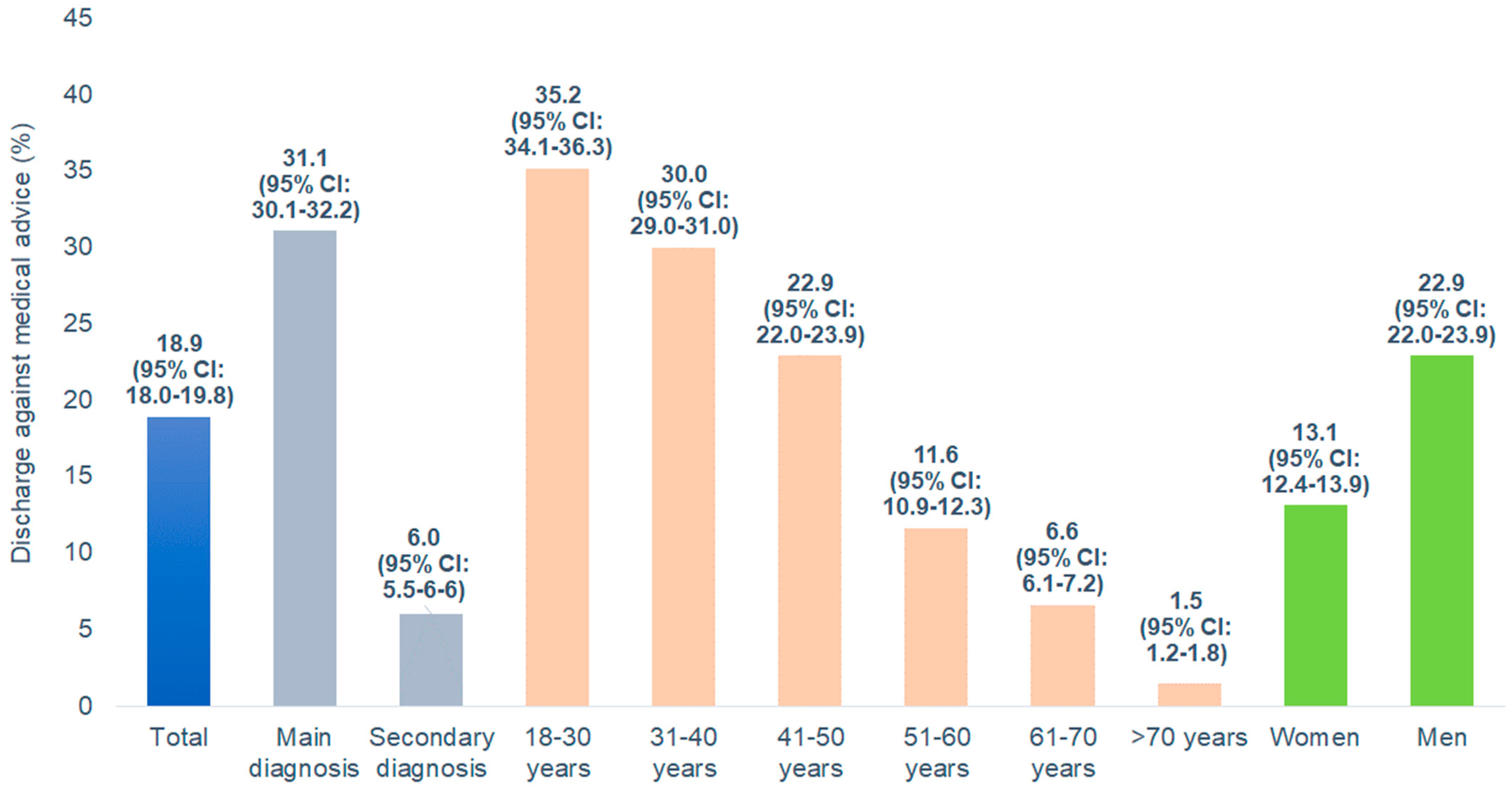
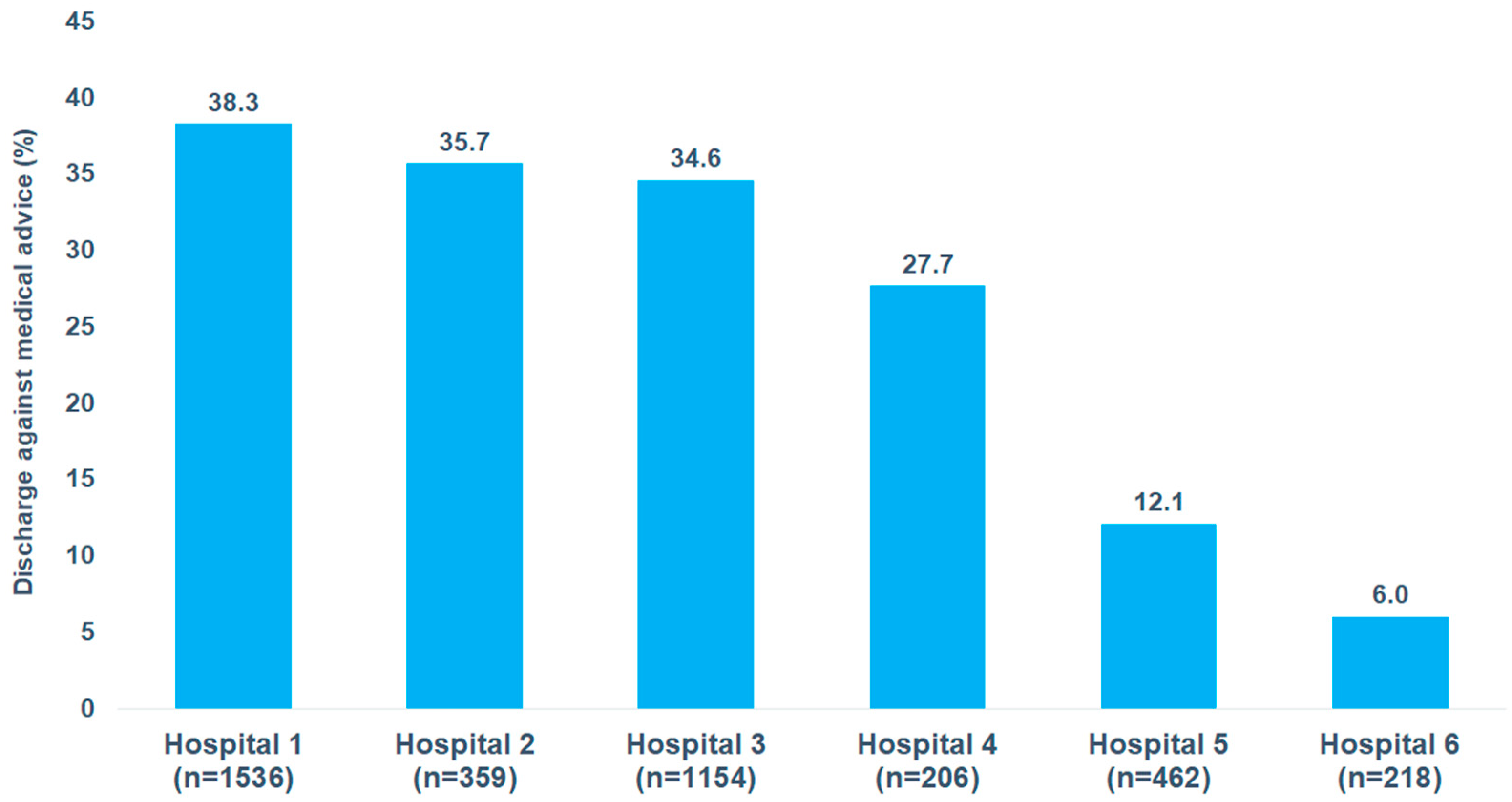
3.2. Prevalence of Discharge Against Medical Advice
3.3. Factors Associated with Discharge Against Medical Advice
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Albayati, A.; Douedi, S.; Alshami, A.; Hossain, M.A.; Sen, S.; Buccellato, V.; Cutroneo, A.; Beelitz, J.; Asif, A. Why Do Patients Leave against Medical Advice? Reasons, Consequences, Prevention, and Interventions. Healthcare 2021, 9, 111. [Google Scholar] [CrossRef]
- Spooner, K.K.; Salemi, J.L.; Salihu, H.M.; Zoorob, R.J. Discharge Against Medical Advice in the United States, 2002–2011. Mayo Clin. Proc. 2017, 92, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Howes, O.D.; Bukala, B.R.; Beck, K. Schizophrenia: From neurochemistry to circuits, symptoms, and treatments. Nat. Rev. Neurol. 2024, 20, 22–35. [Google Scholar] [CrossRef]
- Brook, M.; Hilty, D.M.; Liu, W.; Hu, R.; Frye, M.A. Discharge against medical advice from inpatient psychiatric treatment: A literature review. Psychiatr. Serv. 2006, 57, 1192–1198. [Google Scholar] [CrossRef] [PubMed]
- Valevski, A.; Zalsman, G.; Tsafrir, S.; Lipschitz-Elhawi, R.; Weizman, A.; Shohat, T. Rate of readmission and mortality risks of schizophrenia patients who were discharged against medical advice. Eur. Psychiatry 2012, 27, 496–499. [Google Scholar] [CrossRef] [PubMed]
- Sclar, D.A.; Robison, L.M. Hospital admission for schizophrenia and discharge against medical advice in the United States. Prim. Care Companion J. Clin. Psychiatry 2010, 12, 27329. [Google Scholar] [CrossRef]
- Wung, Y.T.; Chen, C.C.; Chen, F.C.; Lin, C.H. Schizophrenia patients discharged against medical advice at a mental hospital in Taiwan. Psychiatry Clin. Neurosci. 2010, 64, 415–420. [Google Scholar] [CrossRef] [PubMed]
- Choi, M.; Kim, H.; Qian, H.; Palepu, A. Readmission rates of patients discharged against medical advice: A matched cohort study. PLoS ONE 2011, 6, e24459. [Google Scholar] [CrossRef] [PubMed]
- Kostev, K.; Krieg, S.; Krieg, A.; Luedde, T.; Loosen, S.H.; Roderburg, C. In-Hospital Mortality and Associated Factors among Colorectal Cancer Patients in Germany. Cancers 2024, 16, 1219. [Google Scholar] [CrossRef] [PubMed]
- Kostev, K.; Michalowsky, B.; Bohlken, J. In-Hospital Mortality in Patients with and without Dementia across Age Groups, Clinical Departments, and Primary Admission Diagnoses. Brain Sci. 2024, 14, 455. [Google Scholar] [CrossRef] [PubMed]
- Jürgens, L.; Sarabhai, T.; Kostev, K. In-Hospital Mortality Among Elderly Patients Hospitalized for Femur Fracture with and Without Diabetes Mellitus: A Multicenter Case-Control Study. J. Clin. Med. 2024, 13, 6484. [Google Scholar] [CrossRef] [PubMed]
- Kao, Y.C.; Liu, Y.P. Effects of age of onset on clinical characteristics in schizophrenia spectrum disorders. BMC Psychiatry 2010, 10, 63. [Google Scholar] [CrossRef] [PubMed]
- Immonen, J.; Jääskeläinen, E.; Korpela, H.; Miettunen, J. Age at onset and the outcomes of schizophrenia: A systematic review and meta-analysis. Early Interv. Psychiatry 2017, 11, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Emsley, R.; Chiliza, B.; Asmal, L.; Harvey, B.H. The nature of relapse in schizophrenia. BMC Psychiatry 2013, 13, 50. [Google Scholar] [CrossRef] [PubMed]
- Rivelli, A.; Fitzpatrick, V.; Nelson, M.; Laubmeier, K.; Zeni, C.; Mylavarapu, S. Real-world predictors of relapse in patients with schizophrenia and schizoaffective disorder in a large health system. Schizophrenia 2024, 10, 28. [Google Scholar] [CrossRef] [PubMed]
- Khokhar, J.Y.; Dwiel, L.L.; Henricks, A.M.; Doucette, W.T.; Green, A.I. The link between schizophrenia and substance use disorder: A unifying hypothesis. Schizophr. Res. 2018, 194, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Masroor, A.; Khorochkov, A.; Prieto, J.; Singh, K.B.; Nnadozie, M.C.; Abdal, M.; Shrestha, N.; Abe, R.A.M.; Mohammed, L. Unraveling the Association Between Schizophrenia and Substance Use Disorder-Predictors, Mechanisms and Treatment Modifications: A Systematic Review. Cureus 2021, 13, e16722. [Google Scholar] [CrossRef]
- Ti, L.; Ti, L. Leaving the Hospital Against Medical Advice Among People Who Use Illicit Drugs: A Systematic Review. Am. J. Public Health 2015, 105, e53–e59. [Google Scholar] [CrossRef] [PubMed]
- Kraut, A.; Fransoo, R.; Olafson, K.; Ramsey, C.D.; Yogendran, M.; Garland, A. A population-based analysis of leaving the hospital against medical advice: Incidence and associated variables. BMC Health Serv. Res. 2013, 13, 415. [Google Scholar] [CrossRef]
- Katzenellenbogen, J.M.; Sanfilippo, F.M.; Hobbs, M.S.; Knuiman, M.W.; Bessarab, D.; Durey, A.; Thompson, S.C. Voting with their feet—Predictors of discharge against medical advice in Aboriginal and non-Aboriginal ischaemic heart disease inpatients in Western Australia: An analytic study using data linkage. BMC Health Serv. Res. 2013, 13, 330. [Google Scholar] [CrossRef] [PubMed]
- Sealy, L.; Zwi, K.; McDonald, G.; Saavedra, A.; Crawford, L.; Gunasekera, H. Predictors of Discharge Against Medical Advice in a Tertiary Paediatric Hospital. Int. J. Environ. Res. Public Health 2019, 16, 1326. [Google Scholar] [CrossRef] [PubMed]
- Little, J.D. In schizophrenia, are lack of capacity and lack of insight more usefully understood as anosognosia? Australas. Psychiatry 2021, 29, 346–348. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Hospitalizations (N = 7663) |
|---|---|
| Mean age (standard deviation) | 49.5 (17.7) |
| 18–30 | 1335 (17.4) |
| 31–40 | 1450 (18.9) |
| 41–50 | 1264 (16.5) |
| 51–60 | 1368 (17.9) |
| 61–70 | 1177 (15.4) |
| >70 | 1069 (14.0) |
| Female | 3110 (40.6) |
| Male | 4553 (59.4) |
| Schizophrenia as primary diagnosis | 3935 (51.4) |
| Schizophrenia as secondary diagnosis | 3728 (48.6) |
| Schizophrenia ICD-10 codes | |
| Paranoid schizophrenia (F20.0) | 5666 (73.9) |
| Schizophrenia, unspecified (F20.9) | 1021 (13.3) |
| Other schizophrenia diagnoses (F20.1–F20.6) | 976 (12.7) |
| Hospital department | |
| Psychiatry | 4272 (55.8) |
| Somatic departments | 3391 (44.2) |
| Length of hospital stay in days (median, IQR) | 10 (25) |
| Codiagnoses | |
| Thyroid gland disorders | 735 (9.6) |
| Diabetes mellitus | 1144 (14.9) |
| Lipid metabolism disorders | 505 (6.6) |
| Volume depletion | 460 (6.0) |
| Hypokalemia | 665 (8.7) |
| Hypertension | 1910 (24.9) |
| Urinary tract infection | 506 (6.6) |
| COPD | 523 (6.8) |
| Respiratory failure | 517 (6.8) |
| Alcohol-related disorders | 683 (8.9) |
| Cannabis-related disorders | 652 (8.5) |
| Univariable Regression | Multivariable Regression | |||
|---|---|---|---|---|
| Variable | cOR (95% CI) | p Value | aOR (95% CI) * | p Value |
| Age group | ||||
| Age 18–30 years | 35.75 (21.55–59.32) | <0.0001 | 7.44 (4.35–12.73) | <0.0001 |
| Age 31–40 years | 28.20 (17.00–46.79) | <0.0001 | 6.63 (3.89–11.29) | <0.0001 |
| Age 41–50 years | 19.50 (11.70–32.51) | <0.0001 | 5.59 (3.28–9.54) | <0.0001 |
| Age 51–60 years | 8.65 (5.14–14.56) | <0.0001 | 3.41 (1.99–5.85) | <0.0001 |
| Age 61–70 years | 4.67 (2.71–8.05) | <0.0001 | 2.73 (1.57–4.77) | <0.0005 |
| Age > 70 years | Reference | Reference | ||
| Sex | ||||
| Female | Reference | Reference | ||
| Male | 1.97 (1.74–2.24) | <0.0001 | 1.07 (0.93–1.24) | 0.3248 |
| Schizophrenia diagnosis type | ||||
| Schizophrenia as primary diagnosis | 7.01 (6.03–8.15) | <0.0001 | 3.61 (3.05–4.26) | <0.0001 |
| Schizophrenia as secondary diagnosis | Reference | Reference | ||
| Hospital department | ||||
| Psychiatric hospital department ** | 16.86 (13.56–20.97) | <0.0001 | - | |
| Somatic hospital department ** | Reference | - | ||
| Further diagnoses of schizophrenia patients | ||||
| Thyroid gland disorders | 0.38 (0.29–0.49) | <0.0001 | 0.75 (0.56–1.01) | 0.0518 |
| Diabetes mellitus | 0.31 (0.25–0.39) | <0.0001 | 0.98 (0.76–1.27) | 0.8855 |
| Lipid metabolism disorders | 0.25 (0.17–0.36) | <0.0001 | 0.53 (035–0.79) | 0.0020 |
| Volume depletion | 0.22 (0.15–0.34) | <0.0001 | 1.05 (0.67–1.66) | 0.823 |
| Hypokalemia | 0.48 (0.37–0.62) | <0.0001 | 1.26 (0.94–1.69) | 0.1185 |
| Hypertension | 0.24 (0.19–0.28) | <0.0001 | 0.61 (0.49–0.76) | <0.0001 |
| Urinary tract infection | 0.13 (0.08–0.22) | <0.0001 | 0.44 (0.26–0.74) | 0.0019 |
| COPD | 0.20 (0.14–0.30) | <0.0001 | 0.74 (0.47–1.14) | 0.1653 |
| Respiratory failure | 0.07 (0.04–0.14) | <0.0001 | 0.32 (0.16–0.65) | 0.0001 |
| Alcohol-related disorders | 2.25 (1.89–2.67) | <0.0001 | 1.68 (1.38–2.04) | <0.0001 |
| Cannabis-related disorders | 3.48 (2.94–4.11) | <0.0001 | 1.43 (1.18–1.72) | <0.0001 |
| Variable | OR (95% CI) * | p Value |
|---|---|---|
| Age group | ||
| Age 18–30 years | 4.83 (2.17–10.73) | 0.0001 |
| Age 31–40 years | 4.46 (2.01–9.89) | 0.0002 |
| Age 41–50 years | 3.79 (1.70–8.41) | 0.0011 |
| Age 51–60 years | 2.75 (1.23–6.15) | 0.0138 |
| Age 61–70 years | 2.53 (1.11–5.80) | 0.0279 |
| Age > 70 years | Reference | |
| Sex | ||
| Female | Reference | |
| Male | 1.06 (0.90–1.25) | 0.4739 |
| Codiagnoses | ||
| Thyroid gland disorders | 0.68 (0.48–0.95) | 0.0239 |
| Diabetes mellitus | 0.95 (0.68–1.31) | 0.7367 |
| Lipid metabolism disorders | 0.60 (0.39–0.94) | 0.0243 |
| Volume depletion | 1.06 (0.52–2.16) | 0.8828 |
| Hypokalemia | 1.42 (0.99–2.03) | 0.0537 |
| Hypertension | 0.58 (0.45–0.75) | <0.0001 |
| Urinary tract infection | 0.41 (0.21–0.81) | 0.0099 |
| COPD | 0.44 (0.21–0.90) | 0.0236 |
| Respiratory failure | 0.38 (0.05–3.00) | 0.3585 |
| Alcohol-related disorders | 1.25 (0.99–1.58) | 0.0640 |
| Cannabis-related disorders | 1.29 (1.05–1.58) | 0.0159 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kostev, K.; Rodemer, I.; Hajek, A.; Konrad, M.; Smith, L. Discharge Against Medical Advice Among Schizophrenia Patients in Germany: A Multicenter Cross-Sectional Study. Brain Sci. 2025, 15, 196. https://doi.org/10.3390/brainsci15020196
Kostev K, Rodemer I, Hajek A, Konrad M, Smith L. Discharge Against Medical Advice Among Schizophrenia Patients in Germany: A Multicenter Cross-Sectional Study. Brain Sciences. 2025; 15(2):196. https://doi.org/10.3390/brainsci15020196
Chicago/Turabian StyleKostev, Karel, Ira Rodemer, André Hajek, Marcel Konrad, and Lee Smith. 2025. "Discharge Against Medical Advice Among Schizophrenia Patients in Germany: A Multicenter Cross-Sectional Study" Brain Sciences 15, no. 2: 196. https://doi.org/10.3390/brainsci15020196
APA StyleKostev, K., Rodemer, I., Hajek, A., Konrad, M., & Smith, L. (2025). Discharge Against Medical Advice Among Schizophrenia Patients in Germany: A Multicenter Cross-Sectional Study. Brain Sciences, 15(2), 196. https://doi.org/10.3390/brainsci15020196