
The Use of 3D Printed Models for Surgical Simulation of Cranioplasty in Craniosynostosis as Training and Education

 , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. D Printing and Model Creation
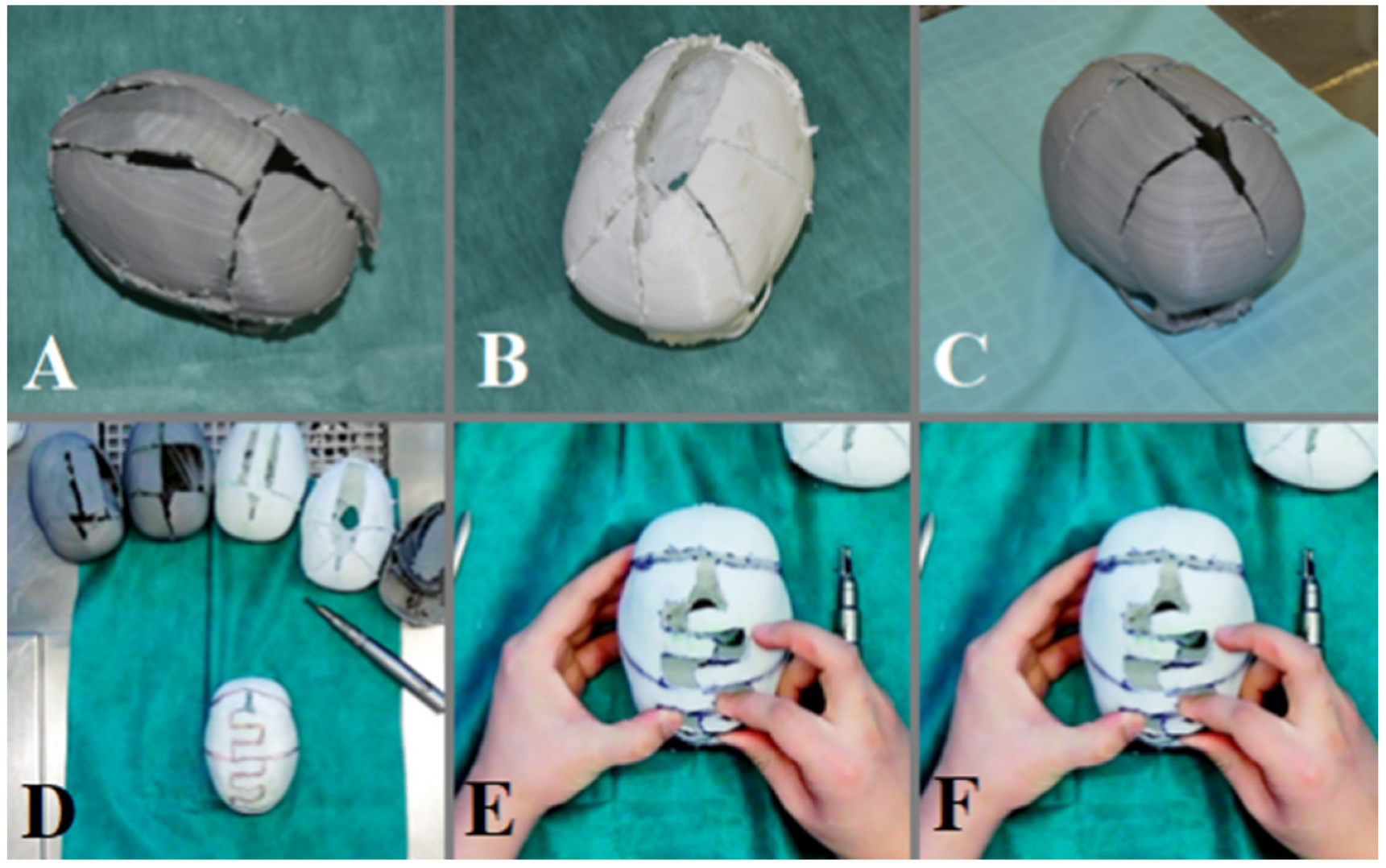
2.3. Surgical Simulation
2.4. Assessment of Learning Outcomes
2.5. Data Analysis
2.6. Ethical Considerations
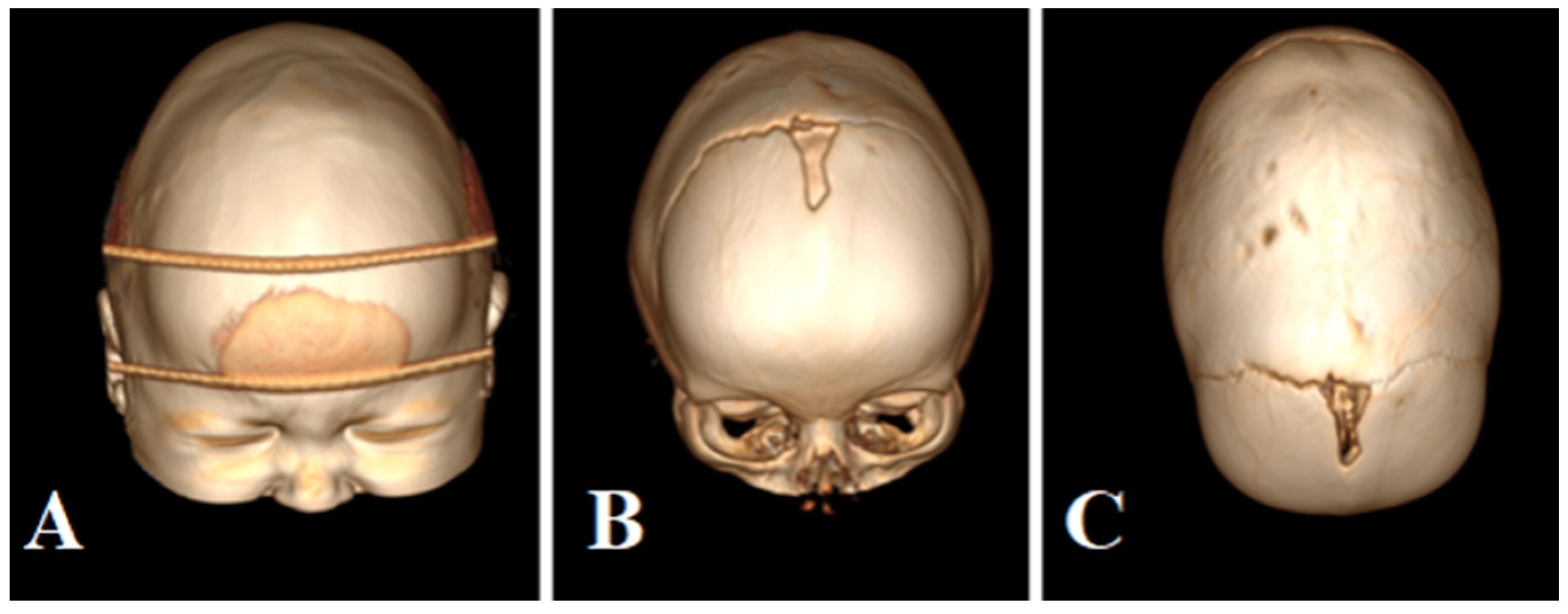
2.7. Description of the Case
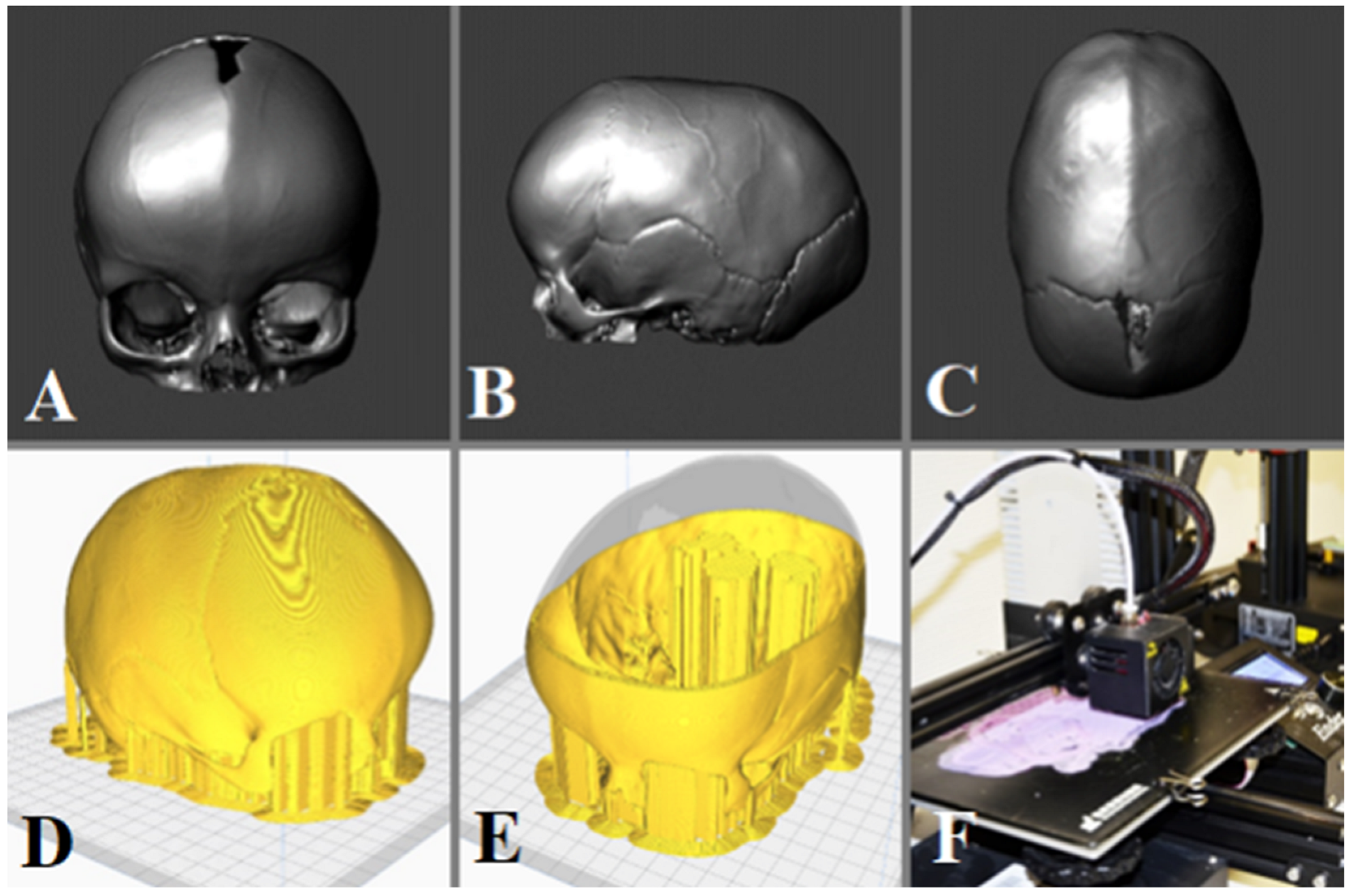
2.8. Procedure to Build and Print the 3D Model
3. Results
3.1. Demographic Characteristics
3.2. Learning Outcomes
3.3. Themes and Patterns
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Condino, S.; Montemurro, N.; Cattari, N.; D’amato, R.; Thomale, U.; Ferrari, V.; Cutolo, F. Evaluation of a Wearable AR Platform for Guiding Complex Craniotomies in Neurosurgery. Ann. Biomed. Eng. 2021, 49, 2590–2605. [Google Scholar] [CrossRef] [PubMed]
- Montemurro, N.; Condino, S.; Cattari, N.; D’amato, R.; Ferrari, V.; Cutolo, F. Augmented Reality-Assisted Craniotomy for Parasagittal and Convexity En Plaque Meningiomas and Custom-Made Cranio-Plasty: A Preliminary Laboratory Report. Int. J. Environ. Res. Public Health 2021, 18, 9955. [Google Scholar] [CrossRef] [PubMed]
- de Notaris, M.; Topczewski, T.; de Angelis, M.; Ensenat, J.; Alobid, I.; Gondolbleu, A.M. Anatomic skull base education using advanced neuroimaging 0g techniques. World Neurosurg. 2013, 79, S16.e9–S16.e13. [Google Scholar] [CrossRef] [PubMed]
- Baskaran, V.; Štrkalj, G.; Štrkalj, M.; Di Ieva, A. Current Applications and Future Perspectives of the Use of 3D Printing in Anatomical Training and Neurosurgery. Front. Neuroanat. 2016, 10, 69. [Google Scholar] [CrossRef]
- Tack, P.; Victor, J.; Gemmel, P.; Annemans, L. 3D-printing techniques in a medical setting: A systematic literature review. Biomed. Eng. Online 2016, 15, 115. [Google Scholar] [CrossRef]
- Rengier, F.; Mehndiratta, A.; von Tengg-Kobligk, H.; Zechmann, C.M.; Unterhinninghofen, R.; Kauczor, H.-U.; Giesel, F.L. 3D printing based on imaging data: Review of medical applications. Int. J. Comput. Assist. Radiol. Surg. 2010, 5, 335–341. [Google Scholar] [CrossRef]
- Ganguli, A.; Pagan-Diaz, G.J.; Grant, L.; Cvetkovic, C.; Bramlet, M.; Vozenilek, J.; Kesavadas, T.; Bashir, R. 3D printing for preoperative planning and surgical training: A review. Biomed. Microdevices 2018, 20, 65. [Google Scholar] [CrossRef]
- Ian, G.; David, W.; Rosen, D.W.; Stucker, B. Extrusion-Based Systems. In Additive Manufacturing Technologies; Springer: New York, NY, USA, 2014; Volume 17, p. 17. [Google Scholar]
- Mishra, R.; Narayanan, M.K.; Umana, G.E.; Montemurro, N.; Chaurasia, B.; Deora, H. Virtual Reality in Neurosurgery: Beyond Neurosurgical Planning. Int. J. Environ. Res. Public Health 2022, 19, 1719. [Google Scholar] [CrossRef]
- Montemurro, N.; Condino, S.; Carbone, M.; Cattari, N.; D’amato, R.; Cutolo, F.; Ferrari, V. Brain Tumor and Augmented Reality: New Technologies for the Future. Int. J. Environ. Res. Public Health 2022, 19, 6347. [Google Scholar] [CrossRef]
- Slater, B.J.; Lenton, K.A.; Kwan, M.D.; Gupta, D.M.; Wan, D.C.; Longaker, M.T. Cranial sutures: A brief review. Plast. Reconstr. Surg. 2008, 121, 170e–178e. [Google Scholar] [CrossRef]
- Panchal, J.; Uttchin, V. Management of craniosynostosis. Plast. Reconstr. Surg. 2003, 111, 2032–2048. [Google Scholar] [CrossRef]
- Sanan, A.; Haines, S.J. Repairing holes in the head: A history of cranioplasty. Neurosurgery 1997, 40, 588–603. [Google Scholar]
- Durand, J.L.; Renier, D.; Marchac, D. L’histoire des cranioplasties [The history of cranioplasty]. Ann. Chir. Plast. Esthet. 1997, 42, 75–83. [Google Scholar]
- Shah, A.M.; Jung, H.; Skirboll, S. Materials used in cranioplasty: A history and analysis. Neurosurg. Focus 2014, 36, E19. [Google Scholar] [CrossRef]
- Horos. Available online: https://fr.freedownloadmanager.org/Mac-OS/Horos-GRATUIT.html (accessed on 1 January 2023).
- Meshmixer 3.5.474. Available online: https://meshmixer.updatestar.com/fr (accessed on 1 January 2023).
- Cura 3.6.0. Available online: https://cura.updatestar.com/fr (accessed on 1 January 2023).
- Ramirez, M.E.; Pena, I.R.; Castillo, R.E.B.; Sufianov, A.; Goncharov, E.; Sanchez, J.A.S.; Colome-Hidalgo, M.; Nurmukhametov, R.; Céspedes, J.R.C.; Montemurro, N. Development of a 3D Printed Brain Model with Vasculature for Neurosurgical Procedure Visualisation and Training. Biomedicines 2023, 11, 330. [Google Scholar] [CrossRef]
- Ramirez, M.D.J.E.; Nurmukhametov, R.; Musa, G.; Castillo, R.E.B.; Encarnacion, V.L.A.; Sanchez, J.A.S.; Vazquez, C.A.; Efe, I.E. Three-Dimensional Plastic Modeling on Bone Frames for Cost-Effective Neuroanatomy Teaching. Cureus 2022, 14, e27472. [Google Scholar] [CrossRef]
- Wang, X.; Jiang, M.; Zhou, Z.W.; Gou, J.H.; Hui, D. 3D printing of polymer matrix composites: A review and prospective. Compos. Part B Eng. 2017, 110, 442–458. [Google Scholar] [CrossRef]
- Petzold, R.; Zeilhofer, H.F.; Kalender, W.A. Rapid protyping technology in medicine--basics and applications. Comput. Med. Imaging Graph. 1999, 23, 277–284. [Google Scholar] [CrossRef]
- Ramirez, M.D.J.E.; Nurmukhametov, R.; Bernard, E.; Peralta, I.; Efe, I.E. A Low-Cost Three-Dimensional Printed Retractor for Transforaminal Lumbar Interbody Fusion. Cureus 2022, 14, e24185. [Google Scholar] [CrossRef]
- Kuo, J.R.; Wang, C.C.; Chio, C.C.; Cheng, T.J. Neurological improvement after cranioplasty-analysis by transcranial doppler ultrasonography. J. Clin. Neurosci. 2004, 11, 486–489. [Google Scholar] [CrossRef]
- Manfiotto, M.; Mottolese, C.; Szathmari, A.; Beuriat, P.-A.; Klein, O.; Vinchon, M.; Gimbert, E.; Roujeau, T.; Scavarda, D.; Zerah, M.; et al. Decompressive craniectomy and CSF disorders in children. Childs Nerv. Syst. 2017, 33, 1751–1757. [Google Scholar] [CrossRef] [PubMed]
- Honeybul, S.; Janzen, C.; Kruger, K.; Ho, K.M. The Incidence of Neurologic Susceptibility to a Skull Defect. World Neurosurg. 2016, 86, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Golz, T.; Graham, C.R.; Busch, L.C.; Wulf, J.; Winder, R.J. Temperature elevation during simulated polymethylmethacrylate (PMMA) cranioplasty in a cadaver model. J. Clin. Neurosci. 2010, 17, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Blum, K.S.; Schneider, S.J.; Rosenthal, A.D. Methyl methacrylate cranioplasty in children: Long-term results. Pediatr. Neurosurg. 1997, 26, 33–35. [Google Scholar] [CrossRef]
- Marchac, D.; Greensmith, A. Long-term experience with methylmethacrylate cranioplasty in craniofacial surgery. J. Plast. Reconstr. Aesthet. Surg. 2008, 61, 744–752. [Google Scholar] [CrossRef]
- Montemurro, N. Telemedicine: Could it represent a new problem for spine surgeons to solve? Glob. Spine J. 2022, 12, 1306–1307. [Google Scholar] [CrossRef]
- Grant, G.A.; Jolley, M.; Ellenbogen, R.G.; Roberts, T.S.; Gruss, J.R.; Loeser, J.D. Failure of autologous bone-assisted cranioplasty following decompressive craniectomy in children and adolescents. J. Neurosurg. 2004, 100, 163–168. [Google Scholar] [CrossRef]
- van de Vijfeijken, S.E.; Münker, T.J.; Spijker, R.; Karssemakers, L.H.; Vandertop, W.P.; Becking, A.G.; Ubbink, D.T.; Dubois, L.; Milstein, D.; Depauw, P.; et al. Autologous Bone Is Inferior to Alloplastic Cranioplasties: Safety of Autograft and Allograft Materials for Cranioplasties, a Systematic Review. World Neurosurg. 2018, 117, 443–452.e8. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Stage of Training Program | Description |
|---|---|
| Introductory Session | An initial session introducing the participants to the use of 3D printed models for surgical simulation of cranioplasty in craniosynostosis. This session may cover topics such as the benefits of using 3D printed models, the anatomy and pathology of craniosynostosis, and the importance of surgical simulation in improving surgical skills. |
| Hands-on Practice Session | A hands-on practice session where the participants get to work with 3D printed models, simulating cranioplasty procedures. This may involve performing various surgical steps such as planning the incisions, drilling, and fixation of the bone segments using 3D printed models. Participants may receive guidance and feedback from experienced instructors to refine their skills. |
| Feedback and Debriefing Session | A session where participants can ask questions, clarify doubts, and receive feedback on their performance during the hands-on practice session. This session may also include debriefing on the surgical simulation exercise, discussing the challenges faced, and identifying areas for improvement. Participants may receive constructive feedback and suggestions for further improvement in their surgical skills using 3D printed models. |
| Aspect | Surgeons without 3D Model Training (Group A) | Surgeons with 3D Model Training (Group B) |
|---|---|---|
| Number of Surgeons | 5 | 5 |
| Training Program | N/A | Comprehensive training program |
| Introduction Session | N/A | Included |
| Hands-on Practice with 3D Models | N/A | Included |
| Feedback and Debriefing Session | N/A | Included |
| Experience with 3D Printed Models | No exposure | Exposure to realistic models |
| Surgical Simulation | N/A | Realistic surgical simulation |
| Surgical Education | Standard understanding | Enhanced understanding |
| Skill Development | Standard surgical skills | Improved surgical skills |
| Confidence in Cranioplasty | Standard confidence | Increased confidence |
| Complication Rates | Standard complication rates | Potentially reduced |
| Patient Outcomes | Standard patient outcomes | Potentially improved |
| Question | Answers |
|---|---|
| 1—Not engaged at all 2—Not engaged 3—Barely engaged 4—Moderate engaged 5—Highly engaged |
| 1—Very low 2—Low 3—Moderate 4—High 5—Very high |
| 1—Yes, significantly 2—Yes, to some extent 3—No, not really 4—No, not at all |
| 1—Poor 2—Fair 3—Good 4—Very good 5—Excellent |
| 1—Yes, significantly more engaging 2—Yes, somewhat more engaging 3—No, about the same level of engagement 4—No, less engaging |
| 1—Yes, significantly 2—Yes, to some extent 3—No, not really 4—No, not at all |
| 1—Very confident 2—Confident 3—Somewhat confident 4—Not confident at all |
| 1—Yes, significantly 2—Yes, to some extent 3—No, not really 4—No, not at all |
| 1—No improvement 2—Slight improvement 3—Improvement 4—Moderate improvement 5—Significant improvement |
| 1—Yes, significantly better 2—Yes, somewhat better 3—No, about the same learning experience 4—No, worse |
| Question | Participating Surgeons of the Group B | ||||
|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | |
| Highly engaged | Highly engaged | Moderate engagement | Highly engaged | Highly engaged |
| High | Very high | Moderate | High | Very high |
| Yes, significantly | Yes, to some extent | Yes, to some extent | Yes, to some extent | Yes, significantly |
| Good | Very good | Good | Good | Excellent |
| Yes, significantly more engaging | Yes, somewhat more engaging | Yes, somewhat more engaging | Yes, somewhat more engaging | Yes, somewhat more engaging |
| Yes, to some extent | Yes, significantly | Yes, significantly | Yes, significantly | Yes, significantly |
| Confident | Very confident | Very confident | Very confident | Very confident |
| Yes, significantly | Yes, to some extent | Yes, significantly | Yes, significantly | Yes, significantly |
| Significant improvement | Significant improvement | Significant improvement | Significant improvement | Significant improvement |
| Yes, somewhat better | Yes, significantly better | Yes, significantly better | Yes, significantly better | Yes, significantly better |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uhl, J.F.; Sufianov, A.; Ruiz, C.; Iakimov, Y.; Mogorron, H.J.; Encarnacion Ramirez, M.; Prat, G.; Lorea, B.; Baldoncini, M.; Goncharov, E.; et al. The Use of 3D Printed Models for Surgical Simulation of Cranioplasty in Craniosynostosis as Training and Education. Brain Sci. 2023, 13, 894. https://doi.org/10.3390/brainsci13060894
Uhl JF, Sufianov A, Ruiz C, Iakimov Y, Mogorron HJ, Encarnacion Ramirez M, Prat G, Lorea B, Baldoncini M, Goncharov E, et al. The Use of 3D Printed Models for Surgical Simulation of Cranioplasty in Craniosynostosis as Training and Education. Brain Sciences. 2023; 13(6):894. https://doi.org/10.3390/brainsci13060894
Chicago/Turabian StyleUhl, Jean Francois, Albert Sufianov, Camillo Ruiz, Yuri Iakimov, Huerta Jose Mogorron, Manuel Encarnacion Ramirez, Guillermo Prat, Barbara Lorea, Matias Baldoncini, Evgeniy Goncharov, and et al. 2023. "The Use of 3D Printed Models for Surgical Simulation of Cranioplasty in Craniosynostosis as Training and Education" Brain Sciences 13, no. 6: 894. https://doi.org/10.3390/brainsci13060894
APA StyleUhl, J. F., Sufianov, A., Ruiz, C., Iakimov, Y., Mogorron, H. J., Encarnacion Ramirez, M., Prat, G., Lorea, B., Baldoncini, M., Goncharov, E., Ramirez, I., Céspedes, J. R. C., Nurmukhametov, R., & Montemurro, N. (2023). The Use of 3D Printed Models for Surgical Simulation of Cranioplasty in Craniosynostosis as Training and Education. Brain Sciences, 13(6), 894. https://doi.org/10.3390/brainsci13060894