
Immune Checkpoint Inhibitor Associated Autoimmune Encephalitis, Rare and Novel Topic of Neuroimmunology: A Case Report and Review of the Literature

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
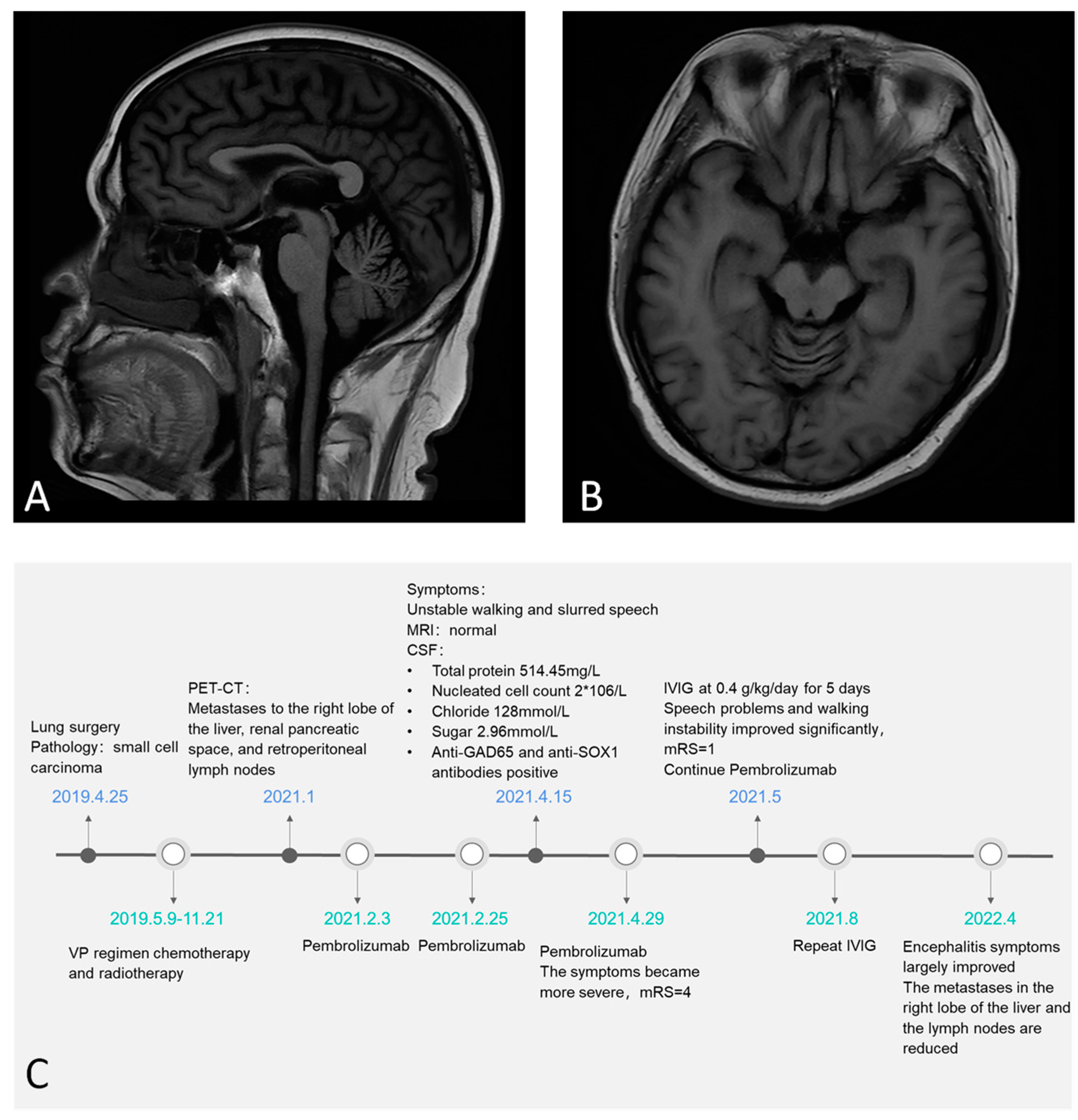
3. Case Report
4. Discussion
4.1. Pembrolizumab-Associated GAD65 Antibody AE, a Very Rare Complication of ICI
4.2. Literature Review of ICI-Associated AE
4.3. Current Dilemma: The Balance between ICI Therapy, Tumor Progression, and AE Treatment
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dolladille, C.; Ederhy, S.; Sassier, M.; Cautela, J.; Thuny, F.; Cohen, A.A.; Fedrizzi, S.; Chrétien, B.; DA Silva, A.; Plane, A.-F.; et al. Immune Checkpoint Inhibitor Rechallenge After Immune-Related Adverse Events in Patients with Cancer. JAMA Oncol. 2020, 6, 865–871. [Google Scholar] [CrossRef]
- Gubin, M.M.; Zhang, X.; Schuster, H.; Caron, E.; Ward, J.P.; Noguchi, T.; Ivanova, Y.; Hundal, J.; Arthur, C.D.; Krebber, W.J.; et al. Checkpoint blockade cancer immunotherapy targets tumour-specific mutant antigens. Nature 2014, 515, 577–581. [Google Scholar] [CrossRef] [PubMed]
- Wei, S.C.; Levine, J.H.; Cogdill, A.P.; Zhao, Y.; Anang, N.-A.A.S.; Andrews, M.C.; Sharma, P.; Wang, J.; Wargo, J.A.; Pe’Er, D.; et al. Distinct Cellular Mechanisms Underlie Anti-CTLA-4 and Anti-PD-1 Checkpoint Blockade. Cell 2017, 170, 1120–1133.e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, A.A.; Patel, V.G. The role of PD-L1 expression as a predictive biomarker: An analysis of all US Food and Drug Ad-ministration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 278. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.Y.; Salem, J.E.; Cohen, J.V.; Chandra, S.; Menzer, C.; Ye, F.; Zhao, S.; Das, S.; Beckermann, K.E.; Ha, L.; et al. Fatal Toxic Effects Associated with Immune Checkpoint Inhibitors: A Systematic Review and Meta-analysis. JAMA Oncol. 2018, 4, 1721–1728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flaig, T.W. NCCN Guidelines Updates: Management of Muscle-Invasive Bladder Cancer. J. Natl. Compr. Cancer Netw. 2019, 17, 591–593. [Google Scholar]
- Messersmith, W.A. NCCN Guidelines Updates: Management of Metastatic Colorectal Cancer. J. Natl. Compr. Cancer Netw. 2019, 17, 599–601. [Google Scholar]
- Gubens, M.A.; Davies, M. NCCN Guidelines Updates: New Immunotherapy Strategies for Improving Outcomes in Non-Small Cell Lung Cancer. J. Natl. Compr. Cancer Netw. 2019, 17, 574–578. [Google Scholar]
- Dammeijer, F.; van Gulijk, M.; Mulder, E.E.; Lukkes, M.; Klaase, L.; van den Bosch, T.; van Nimwegen, M.; Lau, S.P.; Latupeirissa, K.; Schetters, S.; et al. The PD-1/PD-L1-Checkpoint Restrains T cell Immunity in Tumor-Draining Lymph Nodes. Cancer Cell 2020, 38, 685–700.e8. [Google Scholar] [CrossRef]
- Bagchi, S.; Yuan, R.; Engleman, E.G. Immune Checkpoint Inhibitors for the Treatment of Cancer: Clinical Impact and Mechanisms of Response and Resistance. Annu. Rev. Pathol. Mech. Dis. 2021, 16, 223–249. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Lacchetti, C.; Schneider, B.J.; Atkins, M.B.; Brassil, K.J.; Caterino, J.M.; Chau, I.; Ernstoff, M.S.; Gardner, J.M.; Ginex, P.; et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2018, 36, 1714–1768. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Casals, M.; Brahmer, J.R.; Callahan, M.K.; Flores-Chavez, A.; Keegan, N.; Khamashta, M.A.; Lambotte, O.; Mariette, X.; Prat, A.; Suarez-Almazor, M.E. Immune-related adverse events of checkpoint inhibitors. Nat. Rev. Dis. Primers 2020, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Sidlow, R.; Hellmann, M.D. Immune-Related Adverse Events Associated with Immune Checkpoint Blockade. N. Engl. J. Med. 2018, 378, 158–168. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, L.B.; Salama, A. A review of cancer immunotherapy toxicity. CA A Cancer J. Clin. 2020, 70, 86–104. [Google Scholar] [CrossRef] [Green Version]
- Martins, F.; Sofiya, L.; Sykiotis, G.P.; Lamine, F.; Maillard, M.; Fraga, M.; Shabafrouz, K.; Ribi, C.; Cairoli, A.; Guex-Crosier, Y.; et al. Adverse effects of immune-checkpoint inhibitors: Epidemiology, management and surveillance. Nat. Rev. Clin. Oncol. 2019, 16, 563–580. [Google Scholar] [CrossRef]
- Abdel-Wahab, N.; Safa, H.; Abudayyeh, A.; Johnson, D.H.; Trinh, V.A.; Zobniw, C.M.; Lin, H.; Wong, M.K.; Ab-delrahim, M.; Gaber, A.O.; et al. Checkpoint inhibitor therapy for cancer in solid organ transplantation recipients: An institutional experience and a systematic review of the literature. J. Immunother. Cancer 2019, 7, 106. [Google Scholar] [CrossRef]
- Williams, T.J.; Benavides, D.R.; Patrice, K.A.; Dalmau, J.O.; de Avila, A.L.; Le, D.T.; Lipson, E.J.; Probasco, J.C.; Mowry, E.M. Association of Autoimmune Encephalitis with Combined Immune Checkpoint Inhibitor Treatment for Metastatic Cancer. JAMA Neurol. 2016, 73, 928–933. [Google Scholar] [CrossRef]
- Chung, M.; Jaffer, M.; Verma, N.; Mokhtari, S.; Ramsakal, A.; Peguero, E. Immune checkpoint inhibitor induced anti-glutamic acid decarboxylase 65 (Anti-GAD 65) limbic encephalitis responsive to intravenous immunoglobulin and plasma exchange. J. Neurol. 2020, 267, 1023–1025. [Google Scholar] [CrossRef]
- Graus, F.; Dalmau, J. Paraneoplastic neurological syndromes in the era of immune-checkpoint inhibitors. Nat. Rev. Clin. Oncol. 2019, 16, 535–548. [Google Scholar] [CrossRef]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE); Version 5.0; US Department of Health and Human Services: Washington, DC, USA, 2017.
- Bruna, J.; Argyriou, A.A.; Anastopoulou, G.G.; Alemany, M.; Nadal, E.; Kalofonou, F.; Piulats, J.M.; Simó, M.; Velasco, R.; Kalofonos, H.P. Incidence and characteristics of neurotoxicity in immune checkpoint inhibitors with focus on neuromuscular events: Experience beyond the clinical trials. J. Peripher. Nerv. Syst. 2020, 25, 171–177. [Google Scholar] [CrossRef]
- Xu, M.; Nie, Y.; Yang, Y.; Lu, Y.T.; Su, Q. Risk of Neurological Toxicities Following the Use of Different Immune Checkpoint Inhibitor Regimens in Solid Tumors: A Systematic Review and Meta-analysis. Neurologist 2019, 24, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Vogrig, A.; Fouret, M.; Joubert, B.; Picard, G.; Rogemond, V.; Pinto, A.-L.; Muñiz-Castrillo, S.; Roger, M.; Raimbourg, J.; Dayen, C.; et al. Increased frequency of anti-Ma2 encephalitis associated with immune checkpoint inhibitors. Neurol. Neuroimmunol. Neuroinflamm. 2019, 6, e604. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taliansky, A.; Furman, O.; Gadot, M.; Urban, D.; Bar, J.; Shapira-Frumer, R.; Kaufman, B.; Asher, N.; Leibowitz-Amit, R.; Itay, A. Immune checkpoint inhibitors–related encephalitis in melanoma and non-melanoma cancer patients: A single center experience. Support. Care Cancer 2021, 29, 7563–7568. [Google Scholar] [CrossRef] [PubMed]
- Yin, D.; Chen, S.; Liu, J. Sleep Disturbances in Autoimmune Neurologic Diseases: Manifestation and Pathophysiology. Front. Neurosci. 2021, 15, 687536. [Google Scholar] [CrossRef] [PubMed]
- Gill, A.; Perez, M.A.; Perrone, C.M.; Bae, C.J.; Pruitt, A.A.; Lancaster, E. A case series of PD-1 inhibitor-associated paraneoplastic neurologic syndromes. J. Neuroimmunol. 2019, 334, 576980. [Google Scholar] [CrossRef]
- Brown, M.P.; Hissaria, P.; Hsieh, A.H.; Kneebone, C.; Vallat, W. Autoimmune limbic encephalitis with anti-contactin-associated protein-like 2 antibody secondary to pembrolizumab therapy. J. Neuroimmunol. 2017, 305, 16–18. [Google Scholar] [CrossRef]
- Kopecky, J.; Kubecek, O.; Geryk, T.; Slovackova, B.; Hoffmann, P.; Ziaran, M.; Priester, P. Nivolumab induced en-cephalopathy in a man with metastatic renal cell cancer: A case report. J. Med. Case Rep. 2018, 12, 262. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Dunn-Pirio, A.; Luedke, M.; Morgenlander, J.; Skeen, M.; Eckstein, C. Nivolumab-Induced Autoimmune En-cephalitis in Two Patients with Lung Adenocarcinoma. Case Rep. Neurol. Med. 2018, 2018, 2548528. [Google Scholar]
- Shibaki, R.; Murakami, S.; Oki, K.; Ohe, Y. Nivolumab-induced autoimmune encephalitis in an anti-neuronal autoanti-body-positive patient. Jpn. J. Clin. Oncol. 2019, 49, 793–794. [Google Scholar] [CrossRef]
- Mongay-Ochoa, N.; Vogrig, A.; Muñiz-Castrillo, S.; Honnorat, J. Anti-Hu-associated paraneoplastic syndromes triggered by immune-checkpoint inhibitor treatment. J. Neurol. 2020, 267, 2154–2156. [Google Scholar] [CrossRef]
- Shah, N.; Jacob, J.; Househ, Z.; Shiner, E.; Baird, L.; Soudy, H. Unchecked immunity: A unique case of sequential immune-related adverse events with Pembrolizumab. J. Immunother. Cancer 2019, 7, 247. [Google Scholar] [CrossRef] [Green Version]
- Lyons, S.; Joyce, R.; Moynagh, P.; O’Donnell, L.; Blazkova, S.; Counihan, T.J. Autoimmune encephalitis associated with Ma2 antibodies and immune checkpoint inhibitor therapy. Pract. Neurol. 2020, 20, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.; Zheng, K.; Zhang, Y. Paraneoplastic Encephalitis and Enteric Neuropathy Associated with Anti-Hu Antibody in a Patient Following Immune-checkpoint Inhibitor Therapy. J. Immunother. 2020, 43, 165–168. [Google Scholar] [CrossRef]
- Hottinger, A.F.; de Micheli, R.; Guido, V.; Karampera, A.; Hagmann, P.; Du Pasquier, R. Natalizumab may control immune checkpoint inhibitor–induced limbic encephalitis. Neurol. Neuroimmunol. Neuroinflamm. 2018, 5, e439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piepgras, J.; Müller, A.; Steffen, F.; Lotz, J.; Loquai, C.; Zipp, F.; Dresel, C.; Bittner, S. Neurofilament light chain levels reflect outcome in a patient with glutamic acid decarboxylase 65 antibody–positive autoimmune encephalitis under immune checkpoint inhibitor therapy. Eur. J. Neurol. 2021, 28, 1086–1089. [Google Scholar] [CrossRef]
- Burke, M.; Hardesty, M.; Downs, W. A case of severe encephalitis while on PD-1 immunotherapy for recurrent clear cell ovarian cancer. Gynecol. Oncol. Rep. 2018, 24, 51–53. [Google Scholar] [CrossRef]
- Duong, S.L.; Barbiero, F.J.; Nowak, R.J.; Baehring, J.M. Neurotoxicities associated with immune checkpoint inhibitor therapy. J. Neuro-Oncol. 2021, 152, 265–277. [Google Scholar] [CrossRef]
- Ghous, G.; Shoukat, H.M.H.; Tarar, Z.I.; Zafar, M.U.; McGreevy, J.W. Encephalitis Associated with Hemophagocytic Lymphohistiocytosis Secondary to Immune Checkpoint Inhibitors: An Unfamiliar Spin-Off. Cureus 2021, 13, e16079. [Google Scholar] [CrossRef] [PubMed]
- Maniscalco, G.T.; Zekeridou, A.; Allegorico, L.; Ranieri, A.; Napolitano, M.; Pezzella, M.; Della Gatta, L.; Manzo, V.; Ferrari, S.; Mariotto, S. GAD65 autoimmunity after treatment with nivolumab: A multifocal presentation. Neurol. Sci. 2021, 42, 4289–4291. [Google Scholar] [CrossRef]
- Shechtman, Y.; Shalata, W.; Khoury, R.; Mahajna, A.; Weller, B.; Agbarya, A. Encephalitis Induced by Durvalumab During Treatment of Metastatic Small-Cell Lung Cancer: Illustrative Case and Review of the Literature. J. Immunother. 2021, 44, 243–247. [Google Scholar] [CrossRef]
- Yordduangjun, N.; Dishion, E.; McKnight, C.A.; Caplan, J.P. Immune Checkpoint Inhibitor–Associated Autoimmune Encephalitis. J. Acad. Consult. Psychiatry 2021, 62, 115–118. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, Y.; Nagasawa, H.; Katagiri, Y.; Wada, M. Atezolizumab-associated encephalitis in metastatic lung adenocarcinoma: A case report. J. Med. Case Rep. 2020, 14, 88. [Google Scholar] [CrossRef]
- Quach, H.T.; Robbins, C.J.; Balko, J.M.; Chiu, C.Y.; Miller, S.; Wilson, M.R.; Nelson, G.E.; Johnson, D.B. Severe Epididymo-Orchitis and Encephalitis Complicating Anti-PD-1 Therapy. Oncologist 2019, 24, 872–876. [Google Scholar] [CrossRef] [Green Version]
- Braden, J.; Lee, J.H. Immune Checkpoint Inhibitor Induced Pericarditis and Encephalitis in a Patient Treated with Ipilimumab and Nivolumab for Metastatic Melanoma: A Case Report and Review of the Literature. Front. Oncol. 2021, 11, 749834. [Google Scholar] [CrossRef] [PubMed]
- Nishijima, H.; Suzuki, C.; Kon, T.; Nakamura, T.; Tanaka, H.; Sakamoto, Y.; Tomiyama, M. Bilateral Thalamic Lesions Associated with Atezolizumab-Induced Autoimmune Encephalitis. Neurology 2021, 96, 126–127. [Google Scholar] [CrossRef] [PubMed]
- Shionoya, Y.; Hattori, A.; Hanada, T.; Fujino, M. Case Report: Durvalumab-Associated Encephalitis in Extensive-Stage Small Cell Lung Carcinoma. Front. Oncol. 2021, 11, 693279. [Google Scholar] [CrossRef]
- Niki, M.; Nakaya, A.; Kurata, T.; Nakahama, K.; Yoshioka, H.; Kaneda, T.; Kibata, K.; Ogata, M.; Nomura, S. Pem-brolizumab-induced autoimmune encephalitis in a patient with advanced non-small cell lung cancer: A case report. Mol. Clin. Oncol. 2019, 10, 267–269. [Google Scholar]
- Nalbantoglu, M.; Altunrende, B.; Tuncer, O.G.; Akman, G. Autoimmune Encephalitis After Treatment of Hodgkin’s Lymphoma with the Immune Checkpoint Inhibitor Nivolumab. Noro Psikiyatr. Ars. 2021, 58, 163–165. [Google Scholar]
- Thouvenin, L.; Olivier, T.; Banna, G.; Addeo, A.; Friedlaender, A. Immune checkpoint inhibitor-induced aseptic menin-gitis and encephalitis: A case-series and narrative review. Ther. Adv. Drug Saf. 2021, 12, 20420986211004745. [Google Scholar] [CrossRef]
- Chen, S.; Zhang, Y.; Shen, D.; Zhou, Q. The pathogenicity of culprit antibody in autoimmune encephalitis. Chin. J. Contemp. Neurol. Neurosurg. 2022, 22, 1–7. [Google Scholar]
- Zhou, Q.; Zhu, X.; Meng, H.; Zhang, M.; Chen, S. Anti-dipeptidyl-peptidase-like protein 6 encephalitis, a rare cause of reversible rapid progressive dementia and insomnia. J. Neuroimmunol. 2020, 339, 577114. [Google Scholar] [CrossRef] [PubMed]
- Yshii, L.M.; Hohlfeld, R.; Liblau, R.S. Inflammatory CNS disease caused by immune checkpoint inhibitors: Status and perspectives. Nat. Rev. Neurol. 2017, 13, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-T.; Chen, Y.-P.; Lin, W.-C.; Su, W.-C.; Sun, Y.-T. Immune Checkpoint Inhibitor-Induced Myasthenia Gravis. Front. Neurol. 2020, 11, 634. [Google Scholar] [CrossRef] [PubMed]
- Fan, Q.; Hu, Y.; Wang, X.; Zhao, B. Guillain–Barré syndrome in patients treated with immune checkpoint inhibitors. J. Neurol. 2021, 268, 2169–2174. [Google Scholar] [CrossRef]
- Okada, K.; Seki, M.; Yaguchi, H.; Sakuta, K.; Mukai, T.; Yamada, S.; Oki, K.; Nakahara, J.; Suzuki, S. Polyradiculo-neuropathy induced by immune checkpoint inhibitors: A case series and review of the literature. J. Neurol. 2021, 268, 680–688. [Google Scholar] [CrossRef]
- Baldauf, M.C.; Kapauer, M.; Joerger, M.; Flatz, L.; Rodriguez, R.; Frank, S.; Felbecker, A.; Hartmann-Fussenegger, S.; Hundsberger, T. Pembrolizumab-Associated CD8+ Vasculitic Mononeuritis Multiplex in a Patient with Mesothelioma. Neurol. Neuroimmunol. Neuroinflamm. 2021, 8, e993. [Google Scholar] [CrossRef]
- Yang, J.; Liu, X. Immunotherapy for Refractory Autoimmune Encephalitis. Front. Immunol. 2021, 12, 790962. [Google Scholar] [CrossRef]
- Reid, P.D.; Cifu, A.S.; Bass, A.R. Management of Immunotherapy-Related Toxicities in Patients Treated with Immune Checkpoint Inhibitor Therapy. JAMA 2021, 325, 482–483. [Google Scholar] [CrossRef]
- Ni, Y.; Shen, D.; Zhang, Y.; Song, Y.; Gao, Y.; Zhou, Q.; He, L.; Yin, D.; Wang, Y.; Song, F.; et al. Expanding the clinical spectrum of anti-IgLON5 disease: A multicenter retrospective study. Eur. J. Neurol. 2022, 29, 267–276. [Google Scholar] [CrossRef]

{kind=link}
| Author | ICI | Age | Sex | Onset Time | Cancer | Antibody (CSF/Serum) | Symptoms and irAEs Grade | CSF (White Cells/Protein/OCB) and MRI | Treatment | Prognosis |
|---|---|---|---|---|---|---|---|---|---|---|
| Brown [27] | Pembrolizumab | 67 | M | 7 M | Melanoma | CASPR2 Ab(+/+) | Short-term memory loss, anxiety episodes, G3 | ↑/N/NA T2 hyperintensity of the MTL bilaterally | steroid | partially improved |
| Kopecky [28] | Nivolumab | 64 | M | 3 M | Renal cancer | Ma2 Ab(+/−) | Uncontrollable movements, choreiform movements, G3 | N/N/NA increased signal within the basal ganglia | steroid, infliximab | deceased |
| Shah [29] | Nivolumab | 44 | F | 4 M | Lung adenocarcinoma | GAD Ab(+/+) | Dysarthria, dyskinesias, refractory seizures, G4 | ↑/N/NA T2 signal hyperintensities of the bilateral MTL compatible with limbic encephalitis | ICIs discontinued, steroid, PLEX, rituximab | partially improved |
| Nivolumab | 66 | F | 4 M | Lung cancer | Dysarthria, dysarthric, dyskinesias, bilateral arm and leg ballismus, G3 | N/↑/NA symmetric T2 hyperintense and T1 hypointense basal ganglia abnormalities | ICIs discontinued, steroid, IVIg, rituximab | deceased | ||
| Williams [17] | Ipilimumab/Nivolumab | 56 | F | 18 D | Melanoma | NMDAR Ab(+/−) | Disorientation, inattention, bradykinesia, hyperreflexia, G3 | ↑/N/NA stable encephalomalacia at sites of prior radiosurgery with no additional metastases | ICIs discontinued, steroid, IVIg | partially improved |
| Ipilimumab/Nivolumab | 65 | M | NA | Lung cancer | SOX1 Ab(−/+) | Short-term memory loss, progressive difficulty ambulating, G3 | ↑/↑/NA new nonspecific T2 hyperintensities in the right MTL | ICIs discontinued, steroid | improved | |
| Gill [26] | Pembrolizumab | 71 | F | 3 M | Lung adenocarcinoma | Ri Ab(+/−) | Diplopia, unsteady gait, urinary incontinence, G4 | ↑/↑/NA Normal | ICIs discontinued, steroid, rituximab | not improved |
| Nivolumab | 68 | F | NA | Merkel cell carcinoma | Hu Ab(+/+), NMDAR Ab(+/−) | Progressively altered mental status, truncal ataxia, vertical nystagmus, G3 | N/↑/+ T2/FLAIR hyperintensities bilaterally in the medial temporal lobes | ICIs discontinued, steroid, IVIg, rituximab | not improved | |
| Shibaki [30] | Nivolumab | 78 | M | 9 D | Pleural mesothelioma | Ma2 Ab(−/+) | Fever, anorexia, somnolence syndrome, nystagmus, G3 | ↑/↑/NA T2 high signal intensity in the mesencephalon and medial thalamus | ICIs discontinued, steroid | improved |
| Vogrig [23] | Pembrolizumab | 79 | M | 2 M | Lung cancer | Ma2 Ab(NA/NA) | Impulsivity and disinhibition, hyperphagia, confusion, decreased consciousness, G4 | N/↑/NA NA | ICIs discontinued, steroid | partially improved |
| Ipilimumab/Nivolumab | 71 | M | 5 M | Pleural mesothelioma | Ma2 Ab(+/+) | Narcolepsy-cataplexy, hyperphagia, psychiatric symptoms, G3 | ↑/↑/NA FLAIR hypersignal involving the uncus bilaterally, periventricular regions of the third ventricle and hypothalamus | ICIs discontinued, steroid, rituximab | not improved | |
| Nivolumab | 57 | F | 8 M | Pleural mesothelioma | Ma2 Ab(+/+) | Memory deficits, epilepsy, psychomotor retardation, G4 | NA/↑/NA FLAIR bilateral MTL hypersignal | ICIs discontinued, steroid, IVIg | not improved | |
| Pembrolizumab | 47 | M | 8 M | Lung cancer | Ma2 Ab(+/+) | Ophthalmoplegia, head drop, G3 | N/N/+ FLAIR bilateral MTL hypersignal | ICIs discontinued, Steroid | not improved | |
| Nivolumab | 55 | M | 3 M | Kidney cancer | Ma2 Ab(+/+) | Right ear hearing loss, ataxia, vertigo, memory deficits, G3 | N/↑/NA FLAIR bilateral MTL hypersignal | ICIs discontinued, steroid, PLEX | not improved | |
| Nivolumab | 69 | M | 3 M | Kidney cancer | Ma2 Ab(+/−) | Confusion, focal seizures, G3 | N/↑/NA FLAIR bilateral MTL hypersignal | ICIs discontinued, Steroid | not improved | |
| Fellner [31] | Nivolumab | 26 | F | NA | Hodgkin lymphoma | Ma2 Ab(−/+) | Seizures, G4 | N/N/NA FLAIR signal changes in MTL | ICIs discontinued, Steroid | improved |
| Ipilimumab/Nivolumab | 19 | F | NA | Melanoma | Fever, altered mental state, G4 | ↑/↑/NA NA | ICIs discontinued, Steroid | improved | ||
| N. Shah [32] | Pembrolizumab | 70 | M | 17 M | Melanoma | NMDAR Ab(+/+) | Hypoactive delirium, recurrent falls, brief witnessed tonic-clonic seizures, G4 | N/↑/NA Normal | ICIs discontinued, steroid, IVIg | not improved |
| Chung [18] | Ipilimumab/Nivolumab | 36 | F | 2 M | Thymoma | GAD Ab(+/N) | Progressive short-term memory loss, seizures, G4 | N/N/NA fluid-attenuated inversion recovery hyperintensities involving the MTL and hippocampi bilaterally | ICIs discontinued, steroid, IVIg | deceased |
| Lyons [33] | Nivolumab | 56 | F | 3.5 M | Renal cancer | Ma2 Ab(+/+) | Seizure, memory loss, behavioral and personality changes, left internuclear, ophthalmoplegia, G4 | N/↑/NA multiple areas of increased T2 fluid-attenuated inversion recovery signal intensity in the temporal lobes, frontal lobes, brainstem, including bilateral limbic structures and left temporal cortex | ICIs discontinued, steroid, IVIg, mycophenolate mofetil | not improved |
| Kang [34] | Sintilimab | 66 | F | 3 M | SCLC | Hu Ab(+/N) | Focal seizures, G3 | ↑/N/NA NA | ICIs discontinued, steroid | partially improved |
| Hottinger [35] | Ipilimumab/Nivolumab | 71 | F | 4 D | SCLC | Hu Ab(+/N) | Memory deficits, G2 | ↑/N/NA severe abnormalities in both hippocampi with contrast-enhancing lesions | ICIs discontinued, steroid, natalizumab | partially improved |
| Piepgras [36] | Ipilimumab/Nivolumab | 52 | F | 2 W | Melanoma | GAD Ab(+/+) | Short-term memory loss, cognitive dysfunction, limb ataxia, epileptic seizures, G4 | ↑/↑/NA small alterations | ICIs discontinued, steroid, infliximab, reuse nivolumab | deceased |
| Burke [37] | Nivolumab | 64 | F | 4 M | Ovarian clear cell cancer | GAD Ab(−/+) | fever, stiff arms and legs, occasional spasms, G3 | N/N/NA Normal | steroid, PLEX | partially improved |
| Duong [38] | Nivolumab | 57 | M | 5 W | SCLC | GAD Ab(−/+) | NA | ↑/N/NA FLAIR signal in MTL | steroid, IVIg | deceased |
| Nivolumab | 64 | M | 6 M | SCLC | SOX1 Ab(+/−) | NA | ↑/N/+ NA | steroid, IVIg | deceased | |
| Ipilimumab/Nivolumab | 71 | F | 18 M | NSCLC | NA | ↑/↑/NA FLAIR signal in temporal lobes and thalami | steroid | partially improved | ||
| Ghous [39] | Ipilimumab/Nivolumab | 33 | M | 1 M | Melanoma | GAD Ab(+/−) | Slurred speech, word-finding difficulty, ataxia, lower extremity hyperreflexia, G3 | N/↑/+ Normal | steroid | partially improved |
| Maniscalco [40] | Nivolumab | 63 | M | 3 M | Melanoma | GAD Ab(+/+) | seizures, memory loss, behavioral changes, walking difficulties, G4 | ↑/N/+ limbic involvement | ICIs discontinued, steroid, IVIg | not improved |
| Shechtman [41] | Durvalumab | 66 | F | 2 M | SCLC | GABAbR Ab(+/+) | Seizures, disorientation, memory disturbances, G4 | N/N/NA mild chronic microvascular ischemic changes | steroid | partially improved |
| Yordduangjun [42] | Dostarlimab | 52 | F | NA | Endometrial cancer | NMDAR Ab(NA/NA) | Confusion, tremors, loss of fine motor skills, G3 | ↑/↑/+ right temporal sclerosis | ICIs discontinued, steroid, IVIg, rituximab | partially improved |
| Taliansky [24] | Anti CTLA4 | 70 | M | 20 D | SCLC | Seizures, speech disturbances, G4 | NA/↑/NA Normal | ICIs discontinued, NA | partially improved | |
| Anti PD1 | 87 | M | 12 D | Urothelial carcinoma | Confusion, G3 | NA/↑/NA Normal | ICIs discontinued, NA | not improved | ||
| Anti CTLA4+anti PD1 | 49 | F | 9 D | Uterine carcinoma | Cerebellar ataxia, opsoclonus, tremor, G3 | NA/↑/NA Normal | ICIs discontinued, NA | partially improved | ||
| Anti PD1 | 71 | F | 24 D | Breast cancer | Psychotic state, G3 | NA/↑/NA Normal | ICIs discontinued, NA | partially improved | ||
| Anti PD1 | 84 | M | 21 D | Melanoma | Confusion, somnolence, G2 | NA/N/NA Normal | NA, ICIs continued | partially improved | ||
| Anti PD1 | 59 | M | 210 D | Melanoma | Confusion, somnolence, headache, G2 | NA/↑/NA Normal | NA, change the ICI type | partially improved | ||
| Anti PD1 | 71 | F | 110 D | NSCLC | speech and behavioral disturbance, generalized and complex partial epileptic event, G3 | NA/↑/NA Abnormal | ICIs discontinued, NA | not improved | ||
| Anti PD1 | 68 | M | 150 D | NSCLC, adenocarcinoma | Confusion, generalized epileptic event, G4 | NA/↑/NA Normal | ICIs discontinued, NA | partially improved | ||
| Anti PD1 | 67 | F | 15 D | NSCLC, adenocarcinoma | Confusion, sensory neuropathy, G3 | NA/↑/NA Normal | ICIs discontinued, NA | partially improved | ||
| Anti PD1+anti LAG3 | 67 | F | 11 D | Melanoma | Ataxia, speech disturbances, partial seizure, G3 | NA/↑/NA Normal | ICIs discontinued, NA | partially improved | ||
| Anti PD1 | 73 | F | 15 D | Renal cancer | Headache, confusion, G3 | NA/↑/NA Normal | ICIs discontinued, NA | partially improved | ||
| Yamaguchi [43] | Atezolizumab | 56 | M | 17 D | Lung cancer | Consciousness disturbance, motor aphasia, G3 | ↑/↑/NA Normal | ICIs discontinued, steroid | partially improved | |
| QUACH [44] | Pembrolizumab | 69 | M | 2 M | Melanoma | Headaches, fever, and altered mental status, G3 | N/↑/NA suspected left vertebral artery occlusion, known cavernous venous malformation, chronic right optic nerve atrophy | ICIs discontinued, steroid | improved | |
| Braden [45] | Ipilimumab/Nivolumab | 61 | M | 7 M | Melanoma | Sudden onset aphasia, left lower limb myoclonic jerks, confusion, G3 | N/↑/NA FLAIR hyperintensity in the right MTL with differentials including encephalitis or postictal changes | ICIs discontinued, steroid | partially improved | |
| Nishijima [46] | Atezolizumab | 72 | F | 7 M | NSCLC | Gait disturbance, mild disturbance of consciousness, G3 | N/N/+ symmetrical high signal in the thalamus bilaterally | steroid, IVIg | not improved | |
| Shionoya [47] | Durvalumab | 68 | F | 1 M | SCLC | disorientation, memory impairment, eating difficulty, G3 | ↑/↑/NA Normal | ICIs discontinued, Steroid | improved | |
| NIKI [48] | Pembrolizumab | 51 | M | 6 M | NSCLC | seizure, difficulty in walking and communicating, G4 | ↑/↑/NA a tumor in the right frontal lobe of the brain | ICIs discontinued, Steroid | partially improved | |
| Nalbantoğlu [49] | Nivolumab | 40 | M | 1 M | Hodgkin lymphoma | disorientation, inattention, postural tremor in the upper left extremity, and ataxia G3 | ↑/↑/+ right occipital, left frontal millimetric lesions with gadolinium enhancement | ICIs discontinued, Steroid | partially improved | |
| Thouvenin [50] | Ipilimumab/Nivolumab | 70 | M | 3 W | Renal cancer | Confusion, gait disturbance, aphasia, G3 | ↑/↑/NA MRI was limited because of the patient’s agitation | ICIs discontinued, Steroid | partially improved |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gao, Y.; Pan, J.; Shen, D.; Peng, L.; Mao, Z.; Wang, C.; Meng, H.; Zhou, Q.; Chen, S. Immune Checkpoint Inhibitor Associated Autoimmune Encephalitis, Rare and Novel Topic of Neuroimmunology: A Case Report and Review of the Literature. Brain Sci. 2022, 12, 773. https://doi.org/10.3390/brainsci12060773
Gao Y, Pan J, Shen D, Peng L, Mao Z, Wang C, Meng H, Zhou Q, Chen S. Immune Checkpoint Inhibitor Associated Autoimmune Encephalitis, Rare and Novel Topic of Neuroimmunology: A Case Report and Review of the Literature. Brain Sciences. 2022; 12(6):773. https://doi.org/10.3390/brainsci12060773
Chicago/Turabian StyleGao, Yining, Jie Pan, Dingding Shen, Lisheng Peng, Zhifeng Mao, Chunxia Wang, Huanyu Meng, Qinming Zhou, and Sheng Chen. 2022. "Immune Checkpoint Inhibitor Associated Autoimmune Encephalitis, Rare and Novel Topic of Neuroimmunology: A Case Report and Review of the Literature" Brain Sciences 12, no. 6: 773. https://doi.org/10.3390/brainsci12060773
APA StyleGao, Y., Pan, J., Shen, D., Peng, L., Mao, Z., Wang, C., Meng, H., Zhou, Q., & Chen, S. (2022). Immune Checkpoint Inhibitor Associated Autoimmune Encephalitis, Rare and Novel Topic of Neuroimmunology: A Case Report and Review of the Literature. Brain Sciences, 12(6), 773. https://doi.org/10.3390/brainsci12060773