Abstract
Background: In rugby, the shoulder contributes to attack/defence during collisions, tackling, falling, scrummaging, and mauling. We investigated the frequency, tissue, and pathology type of shoulder injuries per player position among professional South African rugby players, and compared injury severity in the context of momentum, intensity, and collision variables. Methods: A prospective study collecting shoulder injury data of 80 male Super Rugby players (>18 years) over 4 seasons (2018–2021). Players wore a Catapult Evo GPS unit during training and match-play, recording performance variables and collision forces during injury. We collected tissue and pathology types of injury from players’ medical files, clinical examinations, and special investigations. Results: Shoulder injuries contributed to 17% of all injuries, ranging from 2 to 34% per year. Forwards (63%) sustained most shoulder injuries, specifically locks (30%). Acromioclavicular (AC) joint (47%) was mostly involved, and ligament/joint capsule (65%) was the most common tissue type injured. Injuries with the highest average momentum resulted in players suffering minimal to mild severity injuries (1–7 days time-loss). Backs (631.15 kg·m/s) required less momentum than forwards (816.00 kg·m/s) to suffer injuries resulting in >28 days time-loss (p = 0.008). Backs encountered higher match intensity (67.76 m/min, p = 0.031) and highest average collisions (0.28/min) without suffering more severe (>28 days time-loss) injuries. Match intensity of >60 m/min resulted in more than 55% of shoulder injuries. Conclusion: One in six injuries in this cohort was shoulder-related. Forwards, specifically locks, sustained most shoulder injuries. The AC joint was the tissue type that mainly contributed. Backline players were involved in higher velocity contact, game intensity, and collision frequency but suffered fewer injuries. However, they required less momentum to sustain more severe injuries.
1. Introduction
Professional rugby union (henceforth called rugby) is a multi-faceted collision sport played worldwide. The on-field rugby team comprises 15 players, sub-divided into eight forward and seven backline player positions [1,2,3]. The different player positions have different roles and a range of physical game demands [1,4,5,6], which involve high-velocity efforts (high-speed running, accelerations, decelerations), jumping, change of directions, static exertions, and low-velocity high-force efforts (tackle, ruck, maul, scrum) [1,7,8,9,10]. The combination of speed, strategy, and strength skills is also associated with a high proportion of traumatic injuries that may occur during training or match-play [11,12].
In rugby, the player’s shoulder is typically the first point of contact in physical collisions and technical contests such as tackling, cleaning out a ruck, scrummaging, and mauling [4,7,13,14]. The tackle is the match event responsible for almost all shoulder injuries (46–90%) [12,15,16,17,18,19,20]. In rugby, tackling is a core skill of defence for all players and is associated with a high risk of injury [21,22,23,24,25]. The high risk of shoulder injuries during tackle events may result from its unparalleled range of motion [16,26].
These physical demands on the shoulder are also position specific. A previous study found significant differences in player injury profiles, as well as between different positions. The study hypothesised that there are likely position-specific differences determined by the technical and physical requirements of each position [27]. The different positional requirements of rugby players, with specific reference to locomotor and contact skills, demand specific technical actions during attack or defence plays [5,7,14]. For example, only forwards are involved in static exertion periods (scrums). In the backline, collision events commonly occur when performing high-intensity running [1,5,7,12,13].
As a consequence of these demands, the shoulder is the second most commonly injured body site (28% of all injuries) after the knee [15,27] and causes the second-highest time-loss injuries after the knee joint [28]. A study on Premier League rugby players reported shoulder injuries as the most severe [28], and a Super Rugby tournament study found 25.6% of all injuries were in the upper limb [15]. This highlights the importance of an in-depth investigation involving collision events and resultant injury severities specific to the shoulder joint.
Global positioning systems tracking and microsensor technology are used in sports settings and analysed to better help understand sports performance [7]. The excessive forces applied to the shoulder joint of rugby players during collisions or tackles often result in shoulder injuries [17,22,23,24,27]. Factors such as high momentum, intense physical demands, and specific collision metrics can contribute to the likelihood and severity of shoulder injuries [7]. Quantifying these factors can assist in better preparing rugby players for collision demands of matches and strategies to reduce the risk of shoulder injuries.
The primary aim of this study is to describe the frequency of shoulder injuries per player position among professional South African rugby players, and to describe the severity of each reported shoulder injury (tissue type, pathology type) in the context of momentum, intensity, and collision variables. The hypothesis is that shoulder injuries differ among player positions, and the number of shoulder injuries is higher following high-impact matches.
2. Materials and Methods
2.1. Study Design and Ethical Considerations
This prospective study was implemented to record data at single time-points across four seasons. Before the onset of this study, the Ethics Committee at the University of Pretoria approved the study (REC 531/2020) with the permission of the Director of Rugby. The team physicians reviewed the medical files and the recorded GPS data of all players that sustained a shoulder injury during the period 2018–2021. The team’s sports scientist assisted in analysing the data.
2.2. Participants
All professional male rugby union players (>18 years) from one South African (SA) rugby franchise that competed in rugby tournaments (including the Super Rugby, Super Rugby Unlocked, Currie Cup, and Rainbow Cup) were eligible for inclusion in this study. Eighty (n = 80) professional rugby players from this franchise participated in rugby union tournament training and matches from 2018 to 2021. Each season started in November and ran until October the following year. Players from other SA franchises were excluded. Figure 1 explains the inclusion and exclusion criteria.
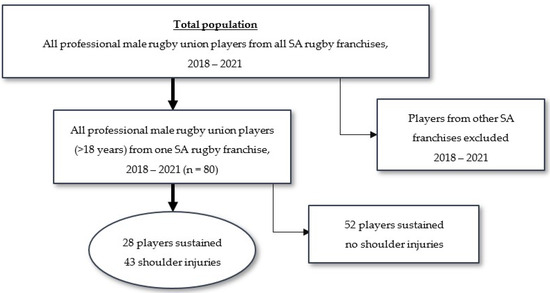
Figure 1.
Flow chart of total sampling population explaining the inclusion and exclusion criteria.
2.3. Data Collection
2.3.1. Definitions
Injury definitions for this study aligned with the consensus for injury data collection in rugby union and the International Olympic Committee consensus statement on methods for recording and reporting of epidemiological data [29,30]. As such, the following definitions were used:
- Injury: “tissue damage or other derangement of normal physical function due to participation in sports, resulting from rapid or repetitive transfer of kinetic energy” [29,30].
- Recurrent injury: “a player sustaining the same pathology to the same anatomical structure within 4 weeks. More than one injury in the same player was recorded as a separate injury” [29,30].
- Collision: “the gravitational force (G) experienced during contact, i.e., when tackled (either being tackled or executing the tackle) [29,30] was set to register an incident at ≥3 G”.
- Injury severity: “the estimated number of days a player is unable to participate in training or match-play” [29,30].
2.3.2. GPS Data Collection
Each player wore a Catapult Evo GPS unit (https://www.catapult.com, accessed on 15 April 2021) during training and match-play. The GPS unit is only a few millimeters in size and encased in a special pouch within the playing jersey on the player’s back, between their shoulder blades. The position of the GPS unit on the athlete’s thoracic spine did not hinder their upper limb or torso range of motion during training or match-play [4].
Each player’s device was switched on, and a satellite lock established before training or matches started. Players wore the same allocated device for training and matches, to keep inter-unit error to a minimum [31,32]. After each training session and match, the GPS units were collected and the data downloaded using OpenField proprietary software (Catapult, OpenField Version 14.1). The data were synced to Catapult’s cloud platform, exported to a Microsoft Excel spreadsheet, and downloaded to a local computer for further analysis.
Catapult is validated for various contact and non-contact sports settings [7,19,32,33,34]. The device uses tri-axial accelerometers (up/down, forwards/backwards, and sideways) that measure acceleration at 10,000 Hz and record at 100 Hz (100 times per second). The tri-axial gyroscopes, used along with the accelerometers, enable the device to measure acceleration, force, rotation, and body orientation with detailed movement assessment at the time of impact. It has a microprocessor that records over a thousand data points per second in real-time, ample storage on the device for post-session analysis, a powerful battery, and a GPS tracking engine. The frequency (collisions per minute) indicates the short, high-intensity bursts experienced over an entire match of 80 min. Collision per minute indicates how often a player position experience contact during their time on the field. The higher the frequency, the higher the volume of contact exposure is for a specific match [6,7,19,34,35,36].
2.3.3. Injury Data Collection
Injury data collection occurred continuously throughout all four seasons, from November to October the following year. The medical team recorded the demographic profile (Mean ± SD) of players with shoulder injuries, which included height (meter, m), body mass (kilogram, kg), and BMI (Body mass index, kg/m2). The specific rugby activity (match-play, training, conditioning, attacking, or defensive drills) during which injury occurred, was noted. Injuries were classified using the modified Orchard Sports Injury Classification System (OSICS) [37].
All the players’ medical history, collision data, injury data, and time to return-to-play data were collected. If available, information on the type of shoulder injury was gathered from the player’s medical files including clinical examinations and special investigations (i.e., ultrasound, computerised tomography, and magnetic resonance imaging). The time-loss (in days), specifically due to shoulder injuries, was documented. Various performance variables and collision forces experienced during the injury (from GPS data) were used in evaluating the spectrum of shoulder injuries, including the pathology of the injury.
2.3.4. Physical Outcome Variables and Specific Parameters Measured
Physical variables and specific locomotor parameters collected for each player included demographics (age, height, body mass, BMI), position of play, diagnosis (OSICS classification), GPS collision data [intensity of match (meters/minute), acceleration per minute (intensity), concentric load, collisions (amount per minute; break down to tackles and rucks, 1× plane), top speed/max velocity (meters/second), total distance (meters), impact (different plane like stepping off the ground or hand off; amount per game)], and time-loss [number of days lost to training and match-play, sub-divided into three categories; 1–7 days (minimal to mild); 8–28 days (moderate); >28 days (severe)]. Momentum was calculated using the following equation:
Momentum (kg·m/s) = mass (kg) × velocity (m/s)
The main outcome was to observe the frequency (n, %) of shoulder injuries per player position. The secondary outcome was to identify the severity (days lost) of each reported shoulder injury in the context of momentum, intensity, and collision variables, and to compare the impact of shoulder injuries between player positions (p < 0.05).
2.3.5. Calculation of Player Exposure
Exposure time over the 4 years was calculated based on the consensus statement on injury data collection in rugby [29]. NM × PM × DM (where NM is the number of matches, PM is the number of players per match, and DM is the match duration in hours). The total duration of a rugby union match is 80 min (1.33 h of play). Injury surveillance was conducted only on one team in the tournament; thus, PM was calculated as 15 players per team for each match. It was also assumed that there were 15 players for the entire match, ignoring the effects of yellow and red cards on match exposure.
2.4. Data Analysis
The analysis was conducted using the statistical program R (https://www.r-project.org/, accessed on 24 January 2023). Descriptive statistics include the mean and standard deviation (SD) and counts and proportions for the categorical variables. Exposure time was used to determine injury incidence and corresponding 95% CIs for the number of shoulder injuries per 1000 h of match-play, regardless of whether a player was injured more than once. Additional investigations included comparing results between the forwards and the backs. The Shapiro–Wilk’s test was used for the continued variables to determine if the data was normally distributed. The independent t-test was used to compare the results for the normally distributed data. The non-parametric alternative, the Mann–Whitney U test, was used when the normality assumption was rejected. The career ender data were excluded where time-loss is reported. All tests were performed at a 5% level of significance.
3. Results
The total match exposure time was computed to 1840 player-hours (981 player-hours for forwards; 859 player-hours for backs).
3.1. Demographic Data
During the 4 years, 80 players rotated through the squad. Players had a mean height of 1.88 ± 0.08 m and mean body mass of 102.96 ± 13.97 kg. The forwards had a BMI of 30.64 ± 2.64 kg/m2 and the backs 26.64 ± 1.70 kg/m2.
3.2. Frequency, Period Prevalence, and Incidence of Shoulder Injuries
A total of 92 matches were played over 4 years of which 34 in 2018, 30 in 2019, and 14 each in 2020 and 2021. The frequency of shoulder injuries was higher during 2018 (n = 16; 34%), followed by 2019 (n = 10; 26%) and 2021 (n = 15; 17%). A total of 28 players sustained 43 shoulder injuries with a period prevalence of 35%. Of the 43 shoulder injuries, 33 (77%) injuries were sustained on the player’s right side and 10 (23%) on the player’s left side. Recurrent injuries occurred in 15 cases. The overall incidence (per 1000 player-hours; 95% CI) of shoulder injuries was 23.37 (16.38–30.35). The total number of shoulder injuries during the 2018–2021 seasons (A) and for each year (B) is depicted in Figure 2.
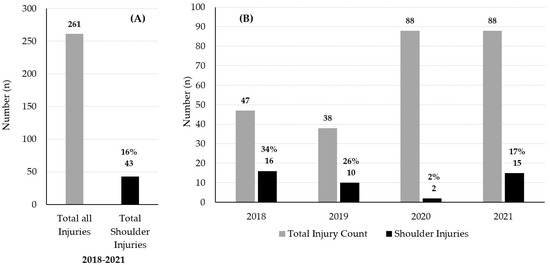
Figure 2.
(A) The total number of all injuries and the number and percentage of all shoulder injuries during the 2018–2021 seasons. (B) The total number of all injuries and the number and percentage of shoulder injuries each year. The SARS-CoV-2 (COVID-19 virus) global pandemic in 2020 negatively influenced participation in all sports.
Shoulder Injuries by Player Position
Forwards (n = 27; 63%) sustained more shoulder injuries compared to backs (n = 16; 37%). The incidence of shoulder injuries in forwards was 27.52 (17.14–37.90) and in backs was 18.63 (9.50–27.75). The total injury count for all shoulder injuries sustained by forwards and backs for each season is depicted in Figure 3.
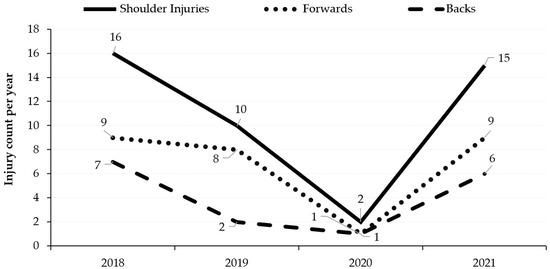
Figure 3.
Number of shoulder injuries sustained by forwards and backs for each year from 2018 to 2021. The SARS-CoV-2 (COVID-19 virus) global pandemic in 2020 negatively influenced participation in all sports.
The locks (n = 13; 30%) sustained the highest number of shoulder injuries, followed by the centres (n = 8; 19%), the loose-forwards (n = 7; 16%), and the props (n = 6; 14%). The locks (n = 8; 62%) also had the most recurrent injuries, followed by the wings (n = 3; 75%), and loosehead props (n = 2; 33%). The wing position sustained the only career-ending injury.
3.3. Severity of Shoulder Injuries (Tissue and Pathology Type) in the Context of Momentum
Table 1 displays the injury severity (days lost to play) and momentum (kg·m/s) by player position, tissue type, and pathology type of the shoulder injuries. Moderate (8–28 days; n = 19; 44%) and severe injuries (>28 days; n = 14; 33%) contributed to 33 (77%) shoulder injuries. The average momentum calculated for each severity group was 750.87 ± 95.20 kg·m/s (1–7 days), 724.20 ± 114.16 kg·m/s (8–28 days), and 736.77 ± 127.71 kg·m/s (>28 days). Forwards (n = 19, 70%) suffered more time-loss injuries (1–28 days) compared to backs (n = 9, 57%). Injuries with the highest average momentum resulted in players suffering mostly minimal to mild time-loss injuries (1–7 days). The locks (n = 4; 791.45 kg·m/s) and loose-forwards (n = 4; 776.49 kg·m/s) had more exposure to higher average momentum scenarios. The average momentum experienced by the other positions were wings (737.90 kg·m/s), centres (713.05 kg·m/s), props (708.57 kg·m/s), fullbacks (682.33 kg·m/s), scrumhalf (628.67 kg·m/s), hookers (623.70 kg·m/s), and flyhalf (448.40 kg·m/s). There was no significant difference (p = 0.0588) in the average momentum experienced by the forward players (762.96 ± 106.29 kg·m/s) compared to the back players (693.61 ± 114.97 kg·m/s). However, backs (631.15 ± 113.20 kg·m/s) required significantly less (p = 0.008) momentum than forwards (816.00 ± 66.36 kg·m/s) to suffer >28 day injury severity. The tissue type most frequently injured in the >28 days time-loss category was ligament/joint capsule injuries (including 1 career-ender; n = 11; 79%), muscle/tendon injuries (n = 3; 21%), and bone injuries (n = 1; 7%). AC joint injuries (n = 20; 61%) contributed most to the total count of the shoulder injuries and to more serious time-loss injuries (8–28 days; n = 12; 36% and >28 days; n = 7; 21%). The average momentum experienced for injury of each tissue type was bone (743.47 kg·m/s, n = 1), ligament/joint capsule (738.29 kg·m/s, n = 28), muscle/tendon (735.35 kg·m/s, n = 11), and nerve (726.16 kg·m/s, n = 3).

Table 1.
Severity and momentum by player position, tissue type, and pathology type.
3.4. Severity of Shoulder Injuries (Tissue and Pathology Type) in the Context of Match Intensity and Collision
Table 2 displays the severity (days lost to play), match intensity (m/min), and collisions (amount/min) of injuries by player position, tissue type, and pathology type of the shoulder injuries. The average match intensity calculated for each severity group was 64.49 ± 15.76 m/min (1–7 days), 60.36 ± 18.24 m/min (8–28 days), and 65.04 ± 12.23 m/min (>28 days). The average collisions calculated for each severity group were 0.29 ± 0.23/min (1–7 days), 0.24 ± 0.14/min (8–28 days), and 0.24 ± 0.14/min (>28 days).
Table 2.
Severity, match intensity, and collision by player position, tissue type, and pathology type.
Backs encountered a significantly higher (p = 0.031) match intensity (67.76 ± 14.60 m/min) than forwards (59.44 ± 15.65 m/min). The player positions experiencing the highest average amount of collisions per minute in the back positions were the centres (0.34 ± 0.23/min) and the fullbacks (0.33 ± 0.11/min), and in the forward positions, the locks (0.27 ± 0.14/min) and the loose-forwards (0.24 ± 0.08/min). Backs (0.28 ± 0.20/min) experienced a higher amount of collisions than forwards (0.23 ± 0.13/min; p = 0.669). The tissue types exposed to the highest average collisions were ligament/joint capsule (0.25 ± 0.15/min) and muscle/tendon (0.25 ± 0.19/min), followed by the nerve (0.22 ± NA/min) and bone (0.14 ± NA/min). The pathology type exposed to the highest average collisions were joint injury (0.31 ± 0.17/min), muscle injury (0.25 ± 0.19/min), traction injury (0.22 ± NA/min), joint sprain (0.21 ± 0.12/min), and fracture (0.14 ± NA/min).
Match Intensity of Each Reported Shoulder Injury
The average match intensity is plotted against the match intensity of each injury in Figure 4. Over the 4 seasons of play, the average match intensity for the 43 shoulder injuries was 62.54 ± 15.63 m/min (Range 14.30–101.20). A total of 25 (58%) injuries occurred at a match intensity above 60 m/min.
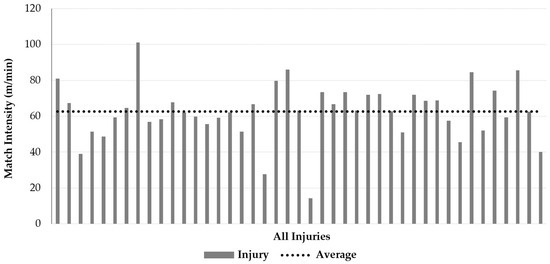
Figure 4.
The average match intensity plotted against the actual match intensity of each injury (n = 43).
The intensity (accelerations/min) and collisions (amount/min) are plotted against the average intensity of each injury in Figure 5. The average intensity (acceleration) was 0.63/min for the 43 injuries. The highest acceleration recorded was 2/min. Typically, when the accelerations increased above 0.50/min, the collisions remained below 0.50/min, except in one instance.
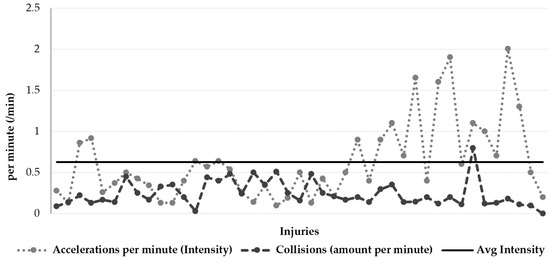
Figure 5.
The intensity (accelerations per minute) and collisions (amount per minute) plotted against the average intensity of each injury (n = 43).
4. Discussion
The main aim of this study was to describe the frequency of shoulder injuries per player position among professional South African rugby players, and this is the first study to describe the severity of each reported shoulder injury (tissue type, pathology type) in the context of momentum, intensity, and collision variables with real-time collision data over 4 years. Across the 4 years, 1 in 6 injuries was shoulder-related. Forwards sustained two-thirds of the shoulder injuries, specifically the locks (30%), and loose-forwards (16%). The ligament/joint capsule contributed two-thirds and muscle/tendon one-third. Almost half of the injuries affected the AC joint (sprains and dislocations). Player positions exposed to the highest average momentum were locks (791.45 kg·m/s), loose-forwards (776.49 kg·m/s), and wings (737.90 kg·m/s). Injuries with the highest average momentum resulted in players suffering mostly minimal to mild severity injuries (1–7 days time-loss). Backs required significantly less (p = 0.008) momentum than forwards to suffer >28-day injury severity. The highest average collisions were recorded among centres (0.34/min), fullbacks (0.33/min), and locks (0.27/min). Backs experienced a higher number of collisions than forwards. Backs also encountered a significantly higher (p = 0.031) match intensity than forwards. The player positions that recorded the highest average match intensity were flyhalf (86.10 m/min), scrumhalf (73.50 m/min), and centre (68.79 m/min), with more than 55% of shoulder injuries sustained when the match intensity was above 60.00 m/min for the respective positions.
In this study, forwards sustained two-thirds of the shoulder injuries. In rugby, forwards, particularly the back row (open-side flanker, blind-side flanker, and the eighth man), are reported to have higher incidences of all injuries than backs [38,39]. In a study involving 140,249 tackles in 434 professional matches, flankers were significantly involved in more tackles per match [40]. Loose-forwards also spend more time in high-intensity (tackling, sprinting, and high-speed running) situations [25,41]. In contrast, an English professional rugby union study reported a higher rate of tackle-derived shoulder injuries in backs [42].
We reported the highest number of shoulder injuries in locks. Other studies also found locks were the most injured players [43,44]. In rugby, each player position has different roles and responsibilities as well as diverse physical game demands that may be possible reasons for players to be exposed to different forces [7,13]. Locks are involved in many contact situations, which are not always at high speed but include tackles, scrum, line-outs, mauls, rucks, and being ball carriers [5,13,14].
In more than 90% of cases, the main tissue type involved ligament/joint capsule (65%) followed by muscle/tendon (26%). A Super Rugby tournament study found muscle/tendon (50%) and ligament/joint (33%) injuries accounted for more than 80% of injuries [15]. In rugby, approximately 5–6% of all reported tackle injuries are shoulder ligament injuries to the tackler [42]. The main mechanism of injury during a tackle is a direct shoulder collision with the opponent or when falling onto the abducted arm, resulting in stretching and straining ligaments [45].
AC joint injuries (47%) were the most frequently occurring diagnosis, followed by shoulder dislocation and muscle contusion. The most common match injury reported in English professional rugby union was an AC joint injury (32%) [42].
In this study, the player positions exposed to the highest average momentum were forwards (locks 791.45 kg·m/s, loose-forwards 776.49 kg·m/s). However, backs (631.15 kg·m/s) required significantly less (p = 0.0081) momentum than forwards (816.00 kg·m/s) to suffer more severe (>28 days) injuries. The momentum involved in this specific team’s contact events is on par with international standards, where a study found the range of momentum to be between 800 and 1000 kg·m/s [46]. The current momentum experienced by professional rugby players is higher than 20 years ago, as found in a study where the range was between 800 and 900 kg·m/s [46]. Even so, injuries with the highest average momentum resulted in players suffering mostly minimal to mild severity injuries (1–7 days time-loss). The use of momentum in quantifying collision events helps to objectively analyse contact scenarios by excluding the difference in player body mass and velocities between forwards and backs, with backs being faster and lighter than forwards [5,7,13,47].
We compared the collisions and accelerations per minute (intensity) to assess rugby as a high-intensity sport. Backs experienced more collisions than forwards, although it did not result in players suffering severe (>28 days time-loss) injuries. In a study over two seasons on the risks associated with tackles in rugby, collisions at high impact force were identified as significant (p < 0.01) risk factors for ball carriers and tacklers. Ball carriers were significantly (p < 0.001) more likely to be a back than a forward, and backs were significantly (p = 0.006) more likely to be injured [48]. Although backs encountered a significantly higher (p = 0.031) match intensity than forwards in our study, it did not advance to more severe (>28 days time-loss) injuries. These findings demonstrate that while high physiological demand is placed on rugby players due to match and training intensity and collisions, it is associated with minimal injury severity.
Strengths and Limitations
Although the use of GPS data in rugby and other sports codes is becoming standard practice when analysing sport performance, our novel study used GPS real-time collision data to compare the severity of each reported shoulder injury (tissue type, pathology type) in the context of momentum, intensity, and collision variables. It is also the first study to quantify the contact scenario with the resultant shoulder injury severity compared to player position. This study is the largest study of its kind, comparing the severity and time-loss of shoulder injuries in professional rugby players with real-time collision data for 4 years. Further scientific research is needed to quantify different pathologies in different rugby populations. These findings can be used in the future strategic design of shoulder injury prevention programs. This study has certain limitations. The SARS-CoV-2 (COVID-19 virus) global pandemic in 2020 negatively influenced the participation of all sports. International travel restrictions were implemented, and the South African teams were excluded from the Super Rugby competition. Therefore, the number of shoulder injuries in 2020 was lower. Momentum was calculated from variables, and intensities were based on GPS data, however it should be acknowledged that match events such as the tackle and scrum are technical. Therefore, applying these physical demands on the shoulder are dynamic and complex and future studies should consider incorporating auxiliary camera records. The actual training/match time a player was exposed to a certain contact load and the number of contact interventions by each player were not explored and future research will be of interest. The findings on male players from one sport cannot be generalised. Further scientific research is needed in different rugby populations to compare findings.
5. Conclusions
Shoulder injuries accounted for 1 in 6 injuries. Various anatomical structures in and around the shoulder were injured during contact scenarios, with the AC joint being the most common and severely involved (>28 days time-loss). The main tissue type implicated in shoulder injuries was the ligament/joint capsule. The rugby positions mostly exposed to contact scenarios are locks (highest severity in injury count), followed by back-three (wing specifically) and loose-forwards (exposed to high severity and momentum). Backline players are mostly involved in higher velocity contact situations compared to forwards being more involved in static contact situations but with a higher collision frequency. Backline players required significantly less momentum than forwards to suffer >28-day injury severity. However, high training, match intensity, and collisions are not associated with more severe injuries. Future use of this technology may assist in understanding the demands of the game and the mechanism of injury, as well the design and implementation of individual position-specific training programs with appropriate player management.
Future Recommendation
- Area(s) of importance in the shoulder that need special conditioning attention are the AC joint, muscle/tendon and ligaments.
- Future research should investigate the potential risk factor analysis and the association between momentum and injuries.
- Future strength and conditioning research should evaluate various techniques, including tackle, breakdown, scrum, and maul skills, to decrease shoulder injury frequency and severity.
- Future research should note that the contact load/demand placed on specific positions during a training week is additional to match-play and uncontrollable, i.e., collisions per minute (frequency), intensity (meters per minute), and momentum (velocity variable) in contact scenarios.
- Future research should evaluate the function and protective factors that different protective wear offers in decreasing shoulder injury severity.
- In the current level of sport and participation, we recommend that healthcare workers focus specifically on shoulder injury prevention strategies in future research.
Author Contributions
J.G.L.: study concept, study planning, data cleaning, data interpretation, manuscript writing (first draft), manuscript review and editing. A.J.v.R.: study planning, data cleaning, data interpretation, writing of the manuscript (first draft), manuscript review and editing. C.T.V.: data interpretation, writing of the manuscript (first draft), manuscript review and editing. S.H.: data interpretation, manuscript review and editing. T.B.: study planning, data cleaning, statistical analysis, data interpretation, manuscript writing, manuscript review and editing. D.C.J.v.R.: study planning, data cleaning, data interpretation, writing of the manuscript (first draft), manuscript review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of the Faculty of Health Sciences, University of Pretoria (REC531/2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study. The director of rugby at the Blue Bulls Company gave consent that the medical data from injuries and the GPS data from matches played over the research period, may be used. Written informed consent has been obtained from the director of rugby of the Blue Bulls Company to publish player data anonymously.
Data Availability Statement
Data sharing not applicable. No new data were created or analyzed in this study.
Acknowledgments
We thank the South African Rugby Franchise Company and the high performance and medical staff for their support, advice, and expertise during this study, specifically Herman Rossouw and Yusuf Vahed.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Donkin, C.; Venter, R.; Coetzee, D.; Kraak, W. Positional in-Match running demands of university rugby players in South Africa. Front. Psychol. 2020, 11, 1591. [Google Scholar] [CrossRef] [PubMed]
- Suarez-Arrones, L.; Portillo, J.; Pareja-Blanco, F.; de Villareal, E.S.; Sánchez-Medina, L.; Munguía-Izquierdo, D. Match-play activity profile in elite women’s rugby union players. J. Strength Cond. Res. 2014, 28, 452–458. [Google Scholar] [CrossRef]
- Roe, G.; Halkier, M.; Beggs, C.; Till, K.; Jones, B. The use of accelerometers to quantify collisions and running demands of rugby union match-play. Int. J. Perform. Anal. Sport 2016, 16, 590–601. [Google Scholar] [CrossRef]
- Sheehan, A.; Malone, S.; Walters, A.; Gabbett, T.; Collins, K. Match-play profile of elite rugby union, with special reference to repeated high-intensity effort activity (RHIE). Sport Sci. Health 2022, 18, 947–956. [Google Scholar] [CrossRef]
- Couderc, A.; Gabbett, T.J.; Piscione, J.; Robineau, J.; Peeters, A.; Igarza, G.; Thomas, C.; Hanon, C.; Lacome, M. Repeated high-intensity effort activity in international male rugby sevens. J. Strength Cond. Res. 2022, 24, 338–344. [Google Scholar] [CrossRef]
- Austin, D.J.; Gabbett, T.J.; Jenkins, D.G. Reliability and sensitivity of a repeated high-intensity exercise performance test for rugby league and rugby union. J. Strength Cond. Res. 2013, 27, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Cunniffe, B.; Proctor, W.; Baker, J.S.; Davies, B. An evaluation of the physiological demands of elite rugby union using global positioning system tracking software. J. Strength Cond. Res. 2009, 23, 1195–1203. [Google Scholar] [CrossRef]
- Read, D.B.; Jones, B.; Phibbs, P.J.; Roe, G.A.; Darrall-Jones, J.D.; Weakley, J.J.; Till, K. Physical demands of representative match-play in adolescent rugby union. J. Strength Cond. Res. 2017, 31, 1290–1296. [Google Scholar] [CrossRef]
- Gabbett, T.J. Physiological and anthropometric characteristics of amateur rugby league players. Br. J. Sports Med. 2000, 34, 303–307. [Google Scholar] [CrossRef]
- Read, D.B.; Till, K.; Beasley, G.; Clarkson, M.; Heyworth, R.; Lee, J.; Weakley, J.J.; Phibbs, P.J.; Roe, G.A.; Darrall-Jones, J.; et al. Maximum running intensities during English academy rugby union match-play. Sci. Med. Footb. 2019, 3, 43–49. [Google Scholar] [CrossRef]
- Papalia, R.; Tecame, A.; Torre, G.; Narbona, P.; Maffulli, N.; Denaro, V. Rugby and shoulder trauma: A systematic review. Transl. Med. UniSa 2015, 12, 5–13. [Google Scholar]
- Reardon, C.; Tobin, D.P.; Tierney, P.; Delahunt, E. The worst case scenario: Locomotor and collision demands of the longest periods of gameplay in professional rugby union. PLoS ONE 2017, 12, e0177072. [Google Scholar] [CrossRef]
- Pollard, B.T.; Turner, A.N.; Eager, R.; Cunningham, D.J.; Cook, C.J.; Hogben, P.; Kilduff, L.P. The ball in play demands of international rugby union. J. Sci. Med. Sport 2018, 21, 1090–1094. [Google Scholar] [CrossRef]
- Tierney, P.; Tobin, D.; Blake, C.; Delahunt, E. Attacking 22 entries in rugby union: Running demands and differences between successful and unsuccessful entries. Scand. J. Med. Sci. Sports 2017, 27, 1934–1941. [Google Scholar] [CrossRef] [PubMed]
- Schwellnus, M.P.; Thomson, A.; Derman, W.; Jordaan, E.; Readhead, C.; Collins, R.; Morris, I.; Strauss, O.; Van der Linde, E.; Williams, A. More than 50% of players sustained a time-loss injury (>1 day of lost training or playing time) during the 2012 Super Rugby Union Tournament: A prospective cohort study of 17,340 player-hours. Br. J. Sports Med. 2014, 48, 1306–1315. [Google Scholar] [CrossRef]
- King, D.; Hume, P.; Gianotti, S.; Clark, T. A retrospective review over 1999 to 2007 of head, shoulder and knee soft tissue and fracture dislocation injuries and associated costs for rugby league in New Zealand. Int. J. Sports Exerc. Med. 2011, 32, 287–291. [Google Scholar] [CrossRef]
- Crichton, J.; Jones, D.R.; Funk, L. Mechanisms of traumatic shoulder injury in elite rugby players. Br. J. Sports Med. 2012, 46, 538–542. [Google Scholar] [CrossRef] [PubMed]
- Quarrie, K.L.; Hopkins, W.G.; Anthony, M.J.; Gill, N.D. Positional demands of international rugby union: Evaluation of player actions and movements. J. Sci. Med. Sport 2013, 16, 353–359. [Google Scholar] [CrossRef]
- Deutsch, M.; Kearney, G.; Rehrer, N. Time–motion analysis of professional rugby union players during match-play. J. Sports Sci. 2007, 25, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Roberts, S.P.; Trewartha, G.; Higgitt, R.J.; El-Abd, J.; Stokes, K.A. The physical demands of elite English rugby union. J. Sports Sci. 2008, 26, 825–833. [Google Scholar] [CrossRef]
- Horsley, I.G.; Fowler, E.M.; Rolf, C.G. Shoulder injuries in professional rugby: A retrospective analysis. J. Orthop. Surg. Res. 2013, 8, 9. [Google Scholar] [CrossRef]
- Usman, J.; McIntosh, A.S. Upper limb injury in rugby union football: Results of a cohort study. Br. J. Sports Med. 2013, 47, 374–379. [Google Scholar] [CrossRef] [PubMed]
- Palmer-Green, D.S.; Stokes, K.A.; Fuller, C.W.; England, M.; Kemp, S.P.; Trewartha, G. Match injuries in English youth academy and schools rugby union: An epidemiological study. Am. J. Sports Med. 2013, 41, 749–755. [Google Scholar] [CrossRef]
- Roberts, S.P.; Trewartha, G.; England, M.; Shaddick, G.; Stokes, K.A. Epidemiology of time-loss injuries in English community-level rugby union. BMJ Open Sport Exerc. Med. 2013, 3, e003998. [Google Scholar] [CrossRef]
- Sundaram, A.; Bokor, D.J.; Davidson, A.S. Rugby Union on-field position and its relationship to shoulder injury leading to anterior reconstruction for instability. J. Sci. Med. Sport. 2011, 14, 111–114. [Google Scholar] [CrossRef]
- Brooks, J.H.; Fuller, C.; Kemp, S.; Reddin, D.B. Epidemiology of injuries in English professional rugby union: Part 1 match injuries. Br. J. Sports Med. 2005, 39, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Williams, S.; Trewartha, G.; Kemp, S.; Stokes, K. A meta-analysis of injuries in senior men’s professional Rugby Union. Sports Med. 2013, 43, 1043–1055. [Google Scholar] [CrossRef] [PubMed]
- Lynch, E.; Lombard, A.J.; Coopoo, Y.; Shaw, I.; Shaw, B.S. Shoulder injury incidence and severity through identification of risk factors in rugby union players. Pak. J. Med. Sci. 2013, 29, 1400. [Google Scholar] [CrossRef] [PubMed]
- Fuller, C.W.; Molloy, M.G.; Bagate, C.; Bahr, R.; Brooks, J.H.; Donson, H.; Kemp, S.P.T.; McCrory, P.; McIntosh, A.S.; Meeuwisse, W.H.; et al. Consensus statement on injury definitions and data collection procedures for studies of injuries in rugby union. Br. J. Sports Med. 2007, 41, 328–331. [Google Scholar] [CrossRef] [PubMed]
- Bahr, R.; Clarsen, B.; Derman, W.; Dvorak, J.; Emery, C.; Finch, C.; Hägglund, M.; Junge, A. International Olympic Committee consensus statement: Methods for recording and reporting of epidemiological data on injury and illness in sports. Br. J. Sports Med. 2020, 54, 372–389. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, S.; Till, K.; Weaving, D.; Jones, B. The use of microtechnology to quantify the peak match demands of the football codes: A systematic review. Sports Med. 2018, 48, 2549–2575. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.J.; Watsford, M.L.; Pine, M.J.; Spurrs, R.W.; Sporri, D. Assessment of 5 Hz and 10 Hz GPS units for measuring athlete movement demands. Int. J. Perform. Anal. Sport 2013, 13, 262–274. [Google Scholar] [CrossRef]
- Johnston, R.D.; Gabbett, T.J.; Jenkins, D.G.; Hulin, B.T. Influence of physical qualities on post-match fatigue in rugby league players. J. Sci. Med. Sport 2015, 18, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Orr, R.; Cheng, H.L. Incidence and characteristics of injuries in elite Australian junior rugby league players. J. Sci. Med. Sport 2016, 19, 212–217. [Google Scholar] [CrossRef]
- Hausler, J.; Halaki, M.; Orr, R. Application of global positioning system and microsensor technology in competitive rugby league match-play: A systematic review and meta-analysis. Sports Med. 2016, 46, 559–588. [Google Scholar] [CrossRef]
- Yeomans, C.; Kenny, I.C.; Cahalan, R.; Warrington, G.D.; Harrison, A.J.; Purtill, H.; Lyons, M.; Campbell, M.J.; Glynn, L.G.; Comyns, T.M. Injury trends in Irish amateur rugby: An epidemiological comparison of men and women. Sports Health 2021, 13, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Rae, K.; Orchard, J. The orchard sports injury classification system (OSICS) version 10. Clin. J. Sport Med. 2007, 17, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Best, J.P.; McIntosh, A.S.; Savage, T.N. Rugby World Cup 2003 injury surveillance project. Br. J. Sports Med. 2005, 39, 812–817. [Google Scholar] [CrossRef]
- Fuller, C.; Laborde, F.; Leather, R.; Molloy, M.G. International rugby board rugby world cup 2007 injury surveillance study. Br. J. Sports Med. 2008, 42, 452–459. [Google Scholar] [CrossRef]
- Quarrie, K.L.; Hopkins, W.G. Tackle injuries in professional rugby union. Am. J. Sports Med. 2008, 36, 1705–1716. [Google Scholar] [CrossRef]
- Eaton, C.; George, K. Position specific rehabilitation for rugby union players. Part I: Empirical movement analysis data. Phys. Ther. Sport 2006, 7, 22–29. [Google Scholar] [CrossRef]
- Headey, J.; Brooks, J.H.; Kemp, S.P. The epidemiology of shoulder injuries in English professional rugby union. Am. J. Sports Med. 2007, 35, 1537–1543. [Google Scholar] [CrossRef] [PubMed]
- Bird, Y.; Waller, A.E.; Marshall, S.W.; Alsop, J.; Chalmers, D.; Gerrard, D. The New Zealand Rugby Injury and Performance Project: V. Epidemiology of a season of rugby injury. Br. J. Sports Med. 1998, 32, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Silva, P. A study on prevalence and risk factors associated with injuries of inter-university rugby players in Sri Lanka based on playing position. BMJ 2021, 55, A97–A98. [Google Scholar]
- Funk, L.; Snow, M. SLAP tears of the glenoid labrum in contact athletes. Clin. J. Sport Med. 2007, 17, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Bevan, T.; Chew, S.; Godsland, I.; Oliver, N.S.; Hill, N.E. A game for all shapes and sizes? Changes in anthropometric and performance measures of elite professional rugby union players 1999–2018. BMJ Open Sport Exerc. Med. 2022, 8, e001235. [Google Scholar] [CrossRef]
- Hendricks, S.; Karpul, D.; Lambert, M. Momentum and kinetic energy before the tackle in rugby union. J. Sports Sci. Med. 2014, 13, 557–563. [Google Scholar] [PubMed]
- Fuller, C.W.; Ashton, T.; Brooks, J.H.; Cancea, R.J.; Hall, J.; Kemp, S.P. Injury risks associated with tackling in rugby union. Br. J. Sports Med. 2010, 44, 159–167. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).