Abstract
Atrial fibrillation (AF) is a common cardiac arrhythmia characterized by irregular and rapid electrical activity in the atria, leading to ineffective contraction and poor blood flow. More than 90% of the left atrial (LA) thrombi that cause thromboembolic events during atrial fibrillation (AF) develop in the left atrial appendage (LAA). AF modifies the hemodynamics of the left atrium, which can result in thrombosis of the LAA, systemic embolism, and stroke. The current options to reduce thromboembolic events are oral anticoagulation, surgical LAA exclusion, or percutaneous LAA occlusion. However, the mechanism underlying thrombus development in the LAA remains poorly understood. Computational fluid dynamics (CFD) analysis can be used to better understand the risk of thrombus formation and subsequent embolic events. CFD enables the simulation and visualization of blood flow patterns within the heart, including complex structures such as the LAA. Using CFD, researchers can analyze the hemodynamics of blood flow, identify areas of stagnation or turbulence, and predict the risk of thrombus formation. The correlation between blood flow dynamics, atrial fibrillation, and the risk of stroke has been highlighted by CFD studies investigating the underlying mechanism of thrombus formation in the LAA. This review study intends to provide a comprehensive overview of the factors involved in thrombus formation and their implications for clinical practice by synthesizing the insights acquired from these CFD studies.
1. Introduction
The left atrial appendage (LAA), originating from the left atrium during fetal development, is described as a long, tubular, hooked structure with variations in size, shape, and volume [1]. The morphology of the LAA is highly diverse from patient to patient and is typically divided into four distinct types based on the structure it evokes: “Chicken wing” is the most frequent morphology (48%), followed by “Cactus” (30%), “Windsock” (19%), and “Cauliflower” (3%) [2]. Nevertheless, the classification is frequently open to misinterpretation and is reliant on the imaging plane. The volume size of LAA also varies significantly with the morphology [3]. Due to the LAA’s characteristics mentioned above, its effect on left atrial (LA) flow is difficult to evaluate.
Literature reveals that LAA is the most prevalent region for thrombus formation, increasing the risk of stroke in patients with atrial fibrillation (AF) [4,5,6]. AF is an electrophysiological pathology with irregular atrial beats, affecting between 1% and 2% of the general population, approximately 8% of people over 80 years old [7,8]. It has been identified as the principal cause of thromboembolic events, such as stroke and vascular dementia [9]. Consequently, there is an urgent need for more effective strategies for identifying and preventing thromboembolic events in AF patients [10]. AF can result in electrical, structural, and contractile remodeling [11,12,13]. Atrial expansion, LA dysfunction, and inadequate atrial contraction result in thrombus development, especially in the LAA [11,12,13]. Furthermore, blood stagnation frequently occurs in the LAA since the blood flow velocity drops dramatically [1,6,13]. Consequently, LAA has received interest as a therapeutic target for preventing thrombosis, particularly in AF patients.
Several therapies are currently available to prevent thrombus formation: (i) oral anticoagulation (i.e., warfarin and direct oral anticoagulants) [14,15,16]; (ii) LAA surgical exclusion [17]; and (iii) LAA percutaneous occlusion [18,19]. However, all of these options have drawbacks that restrict their practice and effectiveness, such as the possibility of hemorrhagic consequences in the case of anticoagulation therapy [14,15,16] and the risks associated with invasive and transcatheter procedures (for example, vascular injury, air-embolic events, and peri-device leaks) [17] for surgical and percutaneous treatments, respectively [18,19]. Although numerous treatments have been proven to reduce the risk of thrombotic events, research has shown a significant residual risk [1,13,20,21]. Due to the diverse morphological factors, such as shape, size, and LAA volume, the reported approaches may fail. In addition, researchers have recognized hemodynamic parameters such as velocity, vorticity, and shear stress as thrombosis predictors [22,23].
Blood flow within the left atrium has currently been evaluated using several methodologies. Transesophageal echocardiography (TEE) can measure the speed at which the LAA empties. However, in clinical practice, TEE cannot accurately measure other hemodynamic parameters, especially in the thrombus regions, since it can either incorrectly label muscles as thrombi or misidentify thrombi hidden in one of the lobes [24,25]. Consequently, an improved strategy must be developed. In clinical research, 4D magnetic resonance imaging (MRI) is a cutting-edge technology that provides more information about 3D blood flow during the cardiac cycle. However, resolution limitations make it difficult to obtain blood flow parameters precisely. In addition, scan times are relatively long [26,27].
Nowadays, computational modeling can provide a detailed knowledge of the mechanisms and effects of AF [28,29]. Personalized computer models can enable the modeling of fibrosis, atrial fiber orientation, and wall thickness heterogeneity’s influences on AF within realistic geometry and tissue properties [30,31]. The computational modeling process is carried out with the assistance of numerical analytic techniques and computational fluid dynamics (CFD). It can provide more quantitative data regarding blood flow and evaluate thrombosis risk [32]. Additionally, it can assess blood flow in specific regions containing LAA lobes. CFD has proved to be a valuable complementary tool for recommending ideal device sizing and placement for LAA occlusion device implantation [32]. In addition, CFD can be applied to better comprehend blood flow patterns following the LAA occlusion procedure and to estimate the risk of device-related thrombosis (DRT) for a given patient and device configuration.
This study aims to review the CFD simulation studies that analyzed hemodynamic parameters and thrombus formation risk. To the authors’ knowledge, there has been no published literature review on this subject to date.
2. CFD Simulation for Thrombus Formation Risk
2.1. Process Description: From Obtaining a CT Scan to CFD Simulation of Left Atrial Appendage
It is essential for diagnosis, treatment planning, and risk assessment to comprehend the hemodynamics of the left atrial appendage. Obtaining a CT scan and conducting a CFD simulation of the left atrial appendage is necessary to shed light on the methodology and considerations required for an accurate and meaningful analysis. The patient is placed on the examination table and positioned within the CT scanner. Multiple perspectives of the heart and left atrial appendage are captured. The resulting image data is saved for future examination. The CT images acquired are transferred to a computer and processed by specialized software. LA and LAA contours have been defined and segmented to produce a three-dimensional model of the structure. This model is the basis for subsequent CFD simulations. Mesh generation is the process of discretizing a 3D model into a computational mesh. In this phase, the model is subdivided into smaller elements that depict the geometry of the left atrial appendage and its surrounding structures. The resolution of the geometry is crucial for accurate CFD simulations. The CFD simulation’s conditions are specified. This includes identifying fluid properties such as viscosity and density, as well as the system’s initial and boundary conditions, such as inlet and outlet velocities, pressures, and flow characteristics. After defining the boundary conditions and generating the geometry, specialized software performs the CFD simulation. Mathematical equations are solved numerically, allowing for the prediction of flow behavior. After the CFD simulation has been completed, the results are analyzed and interpreted. Figure 1 presents a scheme of the process.
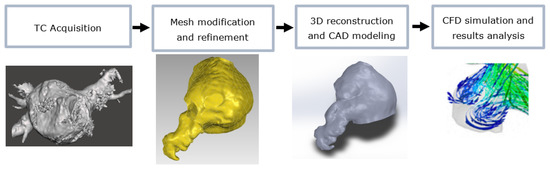
Figure 1.
Scheme of the process: from CT to CFD results.
2.2. Works Selection
In order to be included in this analysis, the studies must be written in English, perform a CFD simulation, and evaluate the thrombus risk assessment in the LAA. Every LAA shape was considered. In terms of CFD software, there was no restriction. Abstracts from meetings and conference papers were excluded. The expected outcomes are the influence of hemodynamic parameters, LAA shape, and CFD characteristics in thrombus formation risk.
During the process of the literature search, eligibility criteria were formulated in order to facilitate the independent selection of titles, descriptors/abstracts found. The literature search identified 65 relevant abstracts of full-text articles. After eliminating duplicate results (n =14), a total of 51 potentially eligible articles were selected. Conference papers (n = 9) and brief communications (n = 2) were excluded. In total, 16 papers were excluded for various reasons, including CFD blood simulations concerning the LAA or LA not being the main focus of the study (n = 15) and the production of personalized LAA occluders (n = 1). A flow diagram depicting this disposition of the studies was constructed (Figure 2). Characteristics of the included studies are shown in Table 1.
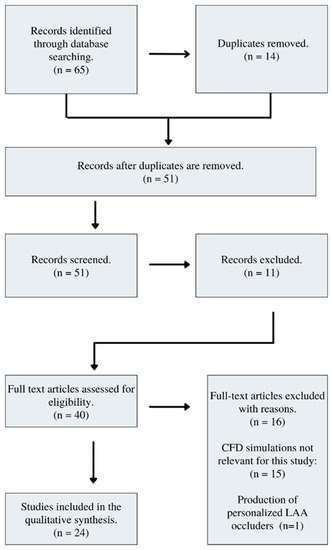
Figure 2.
Flow diagram of study selection.

Table 1.
Characteristics of the included studies.
3. Discussion
Abnormal electrical impulses in the roots of the pulmonary vein primarily cause AF. These impulses induce an uneven and inefficient contraction of the LA. This atypical contraction pattern promotes thrombus development in the LAA and is five times more prevalent in people with AF than in healthy patients [46,54]. Although several clinical investigations have analyzed the correlation between LAA morphology and stroke risk in individuals with AF, the underlying mechanisms are still unclear. Current risk categorization approaches for patients are obtained from major clinical trials based on demographic and clinical characteristics such as age, sex, hypertension, and a history of thromboembolic disease [14]. Since they are all non-patient-specific, their predictive value for a particular patient could be enhanced by incorporating mechanical or local patient-specific indicators, such as cardiac morphology or blood flow.
Developments in medical imaging, including TEE, MRI, and 3D computed tomography (CT), have opened up the possibility of applying computational fluid dynamic (CFD) tools for the analysis of intracardiac flow. Early research on LA CFD was performed using complete left-heart simulations; hence, CFD analyses focusing on LAA are comparatively recent [55]. Few publications provide numerical analyses of flow patterns in the LA, with some including the LAA model.
According to the literature, the chicken wing morphology is the least critical when compared to the other geometries, which reveals a link between the LAA morphology and the risk of clot formation [33,35,36,46]. However, varied quantifications of the risks can be found in the literature depending on the population that was analyzed; thus, it is difficult to generalize the significance of this association [5,49]. Notably, the Cauliflower shape appears to be related to an increased risk of thrombus formation [4,35,36].
Several clinical investigations suggested that the risk of stroke could be reduced by utilizing hemodynamic data on the LA and mainly on the LAA [22,26,36,38,46,53,56]. Using a CFD approach, it is possible to access various biophysical indicators in a complex fluid dynamics system, such as velocity and pressure fields, cardiac blood flow rates, vorticity and turbulent kinetic energy, as well as specific metrics such as Wall Shear Stress (WSS), Time-Averaged Wall Shear Stress (TAWS), Oscillatory Shear Index (OSI), Residence Time (RT), and Endothelial Cell Activation Potential (ECAP) [3,33,34,35,36,39,40,42,43,44,45,47,50,53].
The evaluation of velocity and pressure fields revealed insightful information regarding regions of disturbed flow, recirculation, and stagnation, which are known to contribute to thrombotic events [57,58]. These results confirm previous research that linked abnormal blood flow patterns to an increased risk of thrombus formation. The estimation of cardiac blood flow rates enabled a comprehensive evaluation of blood volume passing through various vasculature regions. Both low and high abnormal flow rates have been linked to an increased risk of thrombosis. The computation of vorticity and turbulent kinetic energy distributions yielded important information regarding the presence and magnitude of turbulent flow patterns. Vorticity denotes the local rotation of blood flow, whereas turbulent kinetic energy denotes the presence of turbulent flow patterns [53]. There is evidence that turbulent flow promotes endothelial dysfunction and thrombus formation. Both variables can affect the likelihood of thrombus formation. CFD permits the computation of vorticity and turbulent kinetic energy distributions, which aids in the identification of thrombosis-prone regions. WSS emerged as an important indicator of thrombus formation among the specific metrics investigated [59]. High WSS values were associated with endothelial cell damage, whereas low WSS values were associated with stagnant blood flow. It quantifies the frictional force imparted by the blood against the vessel wall as it flows. Measuring WSS helps identify regions of blood vessels where thrombosis risk may be elevated. In addition, the TAWSS evaluation presented a more comprehensive understanding of the shear stress experienced by endothelial cells throughout a cardiac cycle [60]. It is the average WSS value over a complete cardiac cycle. TAWSS assists in the identification of regions of the vasculature in which sustained low or oscillatory shear stress may contribute to endothelial dysfunction and consequent thrombus formation. OSI analysis permitted quantification of the magnitude and directionality of shear stress changes throughout a cardiac cycle [60]. High OSI values are associated with an increased risk of endothelial dysfunction and thrombus formation in regions with disturbed blood flow and a change in flow directionality. Analysis of Residence Time (RT) revealed the average time blood particles spend in specific regions of the vasculature [61]. Extended residence time caused by flow recirculation or stagnation can contribute to the formation of a thrombus. The identification of regions with extended residence time facilitates the identification of regions with an increased risk of thrombotic events. ECAP is a metric used to estimate the risk of endothelial cell activation, which contributes to thrombus formation [62]. It evaluates the potential for endothelial cell activation by combining multiple hemodynamic parameters, including WSS, pressure, and strain. ECAP assists in identifying regions where endothelial dysfunction increases the risk of thrombosis. These statistical metrics provide valuable insights into the risk of thrombus formation.
Among the reported studies, one of the main discussed topics is the interaction between LAA hemodynamic parameters, morphological type, and further obtained results’ comparison with the data collected by Di Biase et al. [4]. It is important to highlight that blood flow is critical in determining the possibility of thrombosis formation, particularly under AF conditions [44]. The flow patterns in the LA have been numerically analyzed in CFD studies [3,34,37], with some explicitly focusing on the LAA stasis in AF situations [33,35,50]. Some LAA morphological descriptors, such as ostium characteristics and pulmonary configuration, influenced LAA blood flow patterns [42]. As a result, these investigations were able to provide further knowledge on the AF phenomena and calculate inaccessible blood stasis-related parameters, such as residence time, vorticity, and shear stress. High volume, low blood flow velocity, and two-lobe-appendage are more likely to have blood stasis [42]. Furthermore, the distal part of LAA is reported as the most common region for blood stasis because of the lowest velocity magnitude [44]. Slow flow in the LAA increases blood viscosity, altering secondary swirling flows and intensifying blood stasis [47]. Non-Newtonian effects of blood rheology, neglected in several previous CFD studies, aggravate blood stasis and increase the likelihood of LAA thrombosis, a recognized risk factor in ischemic stroke. Non-Newtonian effects can be subtle when examined using instantaneous metrics but are manifested in the blood residence time [48]. Patient-specific CFD analyses of LA hemodynamics suggest that the thixotropic, shear-thinning rheology of blood can significantly affect flow patterns inside the atrial appendage in a hematocrit-dependent manner [47,48].
CFD simulations have some issues in assessing and quantifying the stasis risk for a particular patient since blood flow washing the LAA is a complex, multi-factorial process. There are primarily two ways to simulate CFD: fixed-wall simulations [3,34,35,36] and moving-wall simulations [34,37]. The first one does not account for the movement of the atrial wall; therefore, it may not accurately represent the atrial flow in all circumstances, especially in sinus rhythm. The other is based on reproducing the patient-specific heart action using medical imaging data. Thus, with this last approach, CFD simulations can properly replicate the hemodynamic state of the patient’s atrium when medical imaging is performed. This presents a challenge for forecasting medium- and long-term stasis in patients with paroxysmal atrial fibrillation. The comparison of the outcomes of fixed-wall and moving-wall simulations has revealed that flow patterns and residence time are remarkably comparable in the case of a compromised function, particularly when both the reservoir and booster functions of the appendage are diminished [33,37]. By employing the rigid-wall concept, it becomes feasible to faithfully reproduce the important conditions corresponding to a specific atrial morphology, irrespective of the atrial function during the period of data acquisition. Consequently, this approach mitigates the potential for inaccurately prognosticating the long-term stability in paroxysmal atrial fibrillation (AF) patients, thereby addressing a significant apprehension associated with the moving-wall simulation method.
The presence of closure devices is also analyzed in the literature [3,41,43,51]. A comparison between the results indicated that LAA closure significantly impacted blood flow velocity and paths. LAA closure successfully reduced LA vortices in strength and duration, indicating that percutaneous LAA occlusion can effectively reduce flow patterns associated with thrombus formation.
4. Conclusions
CFD has made incredible progress in recent years, emerging as an effective tool for analyzing the patterns of blood flow and their impact on various cardiovascular diseases. Among these medical conditions, the formation of LAA thrombus poses a substantial risk to atrial fibrillation patients. In the context of atrial fibrillation, these developments in CFD are increasingly acknowledged as a valuable resource for understanding the flow patterns within the LA and LAA and assessing the likelihood of blood stagnation in individual patients. This could enable the development of tools for identifying patient segments, selecting the optimal therapy, and supporting them during percutaneous intervention.
Recent CFD research has enabled a better understanding of AF principles and the calculation of otherwise inaccessible parameters relating to blood stasis and atrial flow patterns. However, these studies have some limitations. The considerable sensitivity of CFD to numerical assumptions, such as boundary conditions and material properties, which are used to decrease computational costs and simplify the modeling process, represents the significant limitations of the technique.
The accuracy of CFD model results is dependent on a number of variables, including the resolution of medical images, the quality of the discrete grid, the choice of boundary conditions and turbulent model, and the computational parameter settings. These factors collectively affect the simulation’s accuracy and its correspondence with real-world conditions. Regarding patient-specific boundary conditions, such as the flow profile in the mitral valve, obtaining precise and individualized data is a difficult undertaking. This aspect is essential for the future development and clinical deployment of patient-specific models. To improve the accuracy of CFD simulations, it is necessary to emphasize the need for additional research and technological advancements in the acquisition of precision patient-specific boundary conditions. This review also emphasizes the significant impact of simulation conditions on the flow field, specifically the selection between moving-wall and fixed-wall simulations, as well as the nature of velocity/pressure profiles. The analysis demonstrates distinct flow patterns that emerge from these variations, highlighting the importance of precisely defining boundary conditions and taking temporal changes in velocity and pressure profiles into account. This emphasizes the significance of selecting appropriate simulation parameters to enhance flow prediction capabilities in cardiology. By meticulously considering the effect of simulation conditions, it is possible to ensure more accurate representations of real-world scenarios and enhance the design and optimization of pertinent systems.
Insufficient appropriate reference solutions or experimental data for model validation and verification may potentially affect the CFD model development process.
5. Future Directions
CFD has played a pivotal role in elucidating the hemodynamic factors underlying LAA thrombus formation, thereby providing valuable insights into its mechanisms. In terms of expanding the understanding of LAA thrombus formation and its clinical significance, the future holds promising prospects for harnessing CFD’s potential.
CFD’s ability to generate patient-specific simulations is a significant technological advancement. By incorporating advanced imaging modalities, such as magnetic resonance imaging (MRI) and computed tomography (CT), it has become possible to generate patient-specific models of the LAA. These customized simulations take into account unique anatomical variations, including shape, size, and spatial orientation. In the future, it will be crucial for researchers to focus on refining and validating these patient-specific models. These efforts will increase the precision of CFD simulations, allowing for a more thorough understanding of LAA thrombus formation in individual patients.
Blood is a dynamic fluid composed of red blood cells, platelets, and plasma, all of which play a significant role in the process of blood clot formation. Future directions for CFD research include incorporating more complex models of blood constituents into simulations. By considering the behavior of these constituents and their interactions with the wall of the LAA and other blood components, it is possible to obtain a more comprehensive understanding of how blood clots form. These models have the potential to identify new hemodynamic markers that indicate blood clot formation and provide clinicians with valuable guidance for making informed decisions regarding anticoagulation therapy.
The formation of LAA thrombus involves intricate interactions between macroscopic and microscopic fluid dynamics. Although current CFD simulations provide useful insights into macroscopic flow patterns, they frequently struggle to accurately represent micro-scale phenomena. Future developments in CFD research look to develop multi-scale modeling techniques that bridge the gap between macroscopic and microscopic scales in order to overcome this limitation. These multi-scale models will allow for the investigation of phenomena of coagulation within the context of LAA thrombus formation, leading to a more comprehensive understanding of the underlying processes involved.
Combining artificial intelligence (AI) and machine learning (ML) techniques with CFD offers a fascinating chance to improve the understanding of LAA thrombus formation. AI/ML algorithms are capable of analyzing vast quantities of CFD simulation data and detecting intricate patterns that may not be immediately discernible to human observers. These algorithms have the potential to aid in the prediction of patient-specific thrombosis formation risks, the optimization of treatment strategies, and the improvement of patient outcomes. Utilizing the assets of CFD simulations and AI/ML capabilities, researchers can uncover new insights and create more accurate predictive models.
By analyzing future directions in CFD research, such as enhanced patient-specific simulations, incorporation of blood constituent models, multi-scale modeling, and integration with AI/ML techniques, it is possible to further improve our understanding of this complex phenomenon. These developments have the potential to influence the future of cardiovascular research and clinical decision-making, resulting in enhanced patient care and outcomes in the management of LAA thrombus formation.
Author Contributions
Conceptualization: A.M.A., A.P.P., M.O.-S. and L.G.; Formal analysis: S.V. and M.O.-S.; Methodology: S.V. and M.O.-S.; Supervision: A.M.A., A.P.P. and L.G.; Writing—original draft: S.V. and M.O.-S.; Writing—reviewing and editing: S.V., M.O.-S., A.M.A., A.P.P. and L.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
This work was sponsored by national funds through FCT—Fundação para a Ciência e Tecnologia, under the projects UIDB/00285/2020 and LA/P/0112/2020.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Al-Saady, N.M.; Obel, O.A.; Camm, A.J. Left Atrial Appendage: Structure, Function, and Role in Thromboembolism. Heart 1999, 82, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Beigel, R.; Wunderlich, N.C.; Ho, S.Y.; Arsanjani, R.; Siegel, R.J. The Left Atrial Appendage: Anatomy, Function, and Noninvasive Evaluation. JACC Cardiovasc. Imaging 2014, 7, 1251–1265. [Google Scholar] [CrossRef] [PubMed]
- Jia, D.; Jeon, B.; Park, H.B.; Chang, H.J.; Zhang, L.T. Image-Based Flow Simulations of Pre- and Post-Left Atrial Appendage Closure in the Left Atrium. Cardiovasc. Eng. Technol. 2019, 10, 225–241. [Google Scholar] [CrossRef]
- Di Biase, L.; Santangeli, P.; Anselmino, M.; Mohanty, P.; Salvetti, I.; Gili, S.; Horton, R.; Sanchez, J.E.; Bai, R.; Mohanty, S.; et al. Does the Left Atrial Appendage Morphology Correlate with the Risk of Stroke in Patients with Atrial Fibrillation? J. Am. Coll. Cardiol. 2012, 60, 531–538. [Google Scholar] [CrossRef]
- Lupercio, F.; Carlos Ruiz, J.; Briceno, D.F.; Romero, J.; Villablanca, P.A.; Berardi, C.; Faillace, R.; Krumerman, A.; Fisher, J.D.; Ferrick, K.; et al. Left Atrial Appendage Morphology Assessment for Risk Stratification of Embolic Stroke in Patients with Atrial Fibrillation: A Meta-Analysis. Heart Rhythm. 2016, 13, 1402–1409. [Google Scholar] [CrossRef] [PubMed]
- Özer, N.; Tokgözoğlu, L.; Övünç, K.; Kabakçı, G.; Aksöyek, S.; Aytemir, K.; Kes, S. Left Atrial Appendage Function in Patients with Cardioembolic Stroke in Sinus Rhythm and Atrial Fibrillation. J. Am. Soc. Echocardiogr. 2000, 13, 661–665. [Google Scholar] [CrossRef]
- Pellman, J.; Sheikh, F. Atrial Fibrillation: Mechanisms, Therapeutics, and Future Directions. Compr. Physiol. 2015, 5, 649–665. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Wolf, P.A.; D’Agostino, R.B.; Silbershatz, H.; Kannel, W.B.; Levy, D. Impact of Atrial Fibrillation on the Risk of Death. Circulation 1998, 98, 946–952. [Google Scholar] [CrossRef]
- Prince, M.; Bryce, R.; Albanese, E.; Wimo, A.; Ribeiro, W.; Ferri, C.P. The Global Prevalence of Dementia: A Systematic Review and Metaanalysis. Alzheimer’s Dement. 2013, 9, 63. [Google Scholar] [CrossRef]
- Singh, S.M.; Micieli, A.; Wijeysundera, H.C. Economic Evaluation of Percutaneous Left Atrial Appendage Occlusion, Dabigatran, and Warfarin for Stroke Prevention in Patients with Nonvalvular Atrial Fibrillation. Circulation 2013, 127, 2414–2423. [Google Scholar] [CrossRef]
- Marrouche, N.F.; Wilber, D.; Hindricks, G.; Jais, P.; Akoum, N.; Marchlinski, F.; Kholmovski, E.; Burgon, N.; Hu, N.; Mont, L.; et al. Association of Atrial Tissue Fibrosis Identified by Delayed Enhancement MRI and Atrial Fibrillation Catheter Ablation. JAMA 2014, 311, 498. [Google Scholar] [CrossRef] [PubMed]
- Dzeshka, M.S.; Lip, G.Y.H.; Snezhitskiy, V.; Shantsila, E. Cardiac Fibrosis in Patients with Atrial Fibrillation. J. Am. Coll. Cardiol. 2015, 66, 943–959. [Google Scholar] [CrossRef]
- Naksuk, N.; Padmanabhan, D.; Yogeswaran, V.; Asirvatham, S.J. Left Atrial Appendage. JACC Clin. Electrophysiol. 2016, 2, 403–412. [Google Scholar] [CrossRef]
- Holmes, D.R.; Lakkireddy, D.R.; Whitlock, R.P.; Waksman, R.; Mack, M.J. Left Atrial Appendage Occlusion. J. Am. Coll. Cardiol. 2014, 63, 291–298. [Google Scholar] [CrossRef] [PubMed]
- Hylek, E.M.; Evans-Molina, C.; Shea, C.; Henault, L.E.; Regan, S. Major Hemorrhage and Tolerability of Warfarin in the First Year of Therapy among Elderly Patients with Atrial Fibrillation. Circulation 2007, 115, 2689–2696. [Google Scholar] [CrossRef] [PubMed]
- Onalan, O.; Lashevsky, I.; Hamad, A.; Crystal, E. Nonpharmacologic Stroke Prevention in Atrial Fibrillation. Expert. Rev. Cardiovasc. Ther. 2005, 3, 619–633. [Google Scholar] [CrossRef]
- Ailawadi, G.; Gerdisch, M.W.; Harvey, R.L.; Hooker, R.L.; Damiano, R.J.; Salamon, T.; Mack, M.J. Exclusion of the Left Atrial Appendage with a Novel Device: Early Results of a Multicenter Trial. J. Thorac. Cardiovasc. Surg. 2011, 142, 1002–1009.e1. [Google Scholar] [CrossRef]
- Gan, C.H.; Bhat, A.; Davis, L.; Denniss, A.R. Percutaneous Transcatheter Left Atrial Appendage Closure Devices: Role in the Long-Term Management of Atrial Fibrillation. Heart Lung Circ. 2014, 23, 407–413. [Google Scholar] [CrossRef]
- Lam, Y.Y.; Yan, B.P.; Doshi, S.K.; Li, A.; Zhang, D.; Kaya, M.G.; Park, J.W. Preclinical Evaluation of a New Left Atrial Appendage Occluder (Lifetech LAmbreTM Device) in a Canine Model. Int. J. Cardiol. 2013, 168, 3996–4001. [Google Scholar] [CrossRef]
- Kanderian, A.S.; Gillinov, A.M.; Pettersson, G.B.; Blackstone, E.; Klein, A.L. Success of Surgical Left Atrial Appendage Closure. J. Am. Coll. Cardiol. 2008, 52, 924–929. [Google Scholar] [CrossRef]
- Aryana, A.; Singh, S.K.; Singh, S.M.; Gearoid O’Neill, P.; Bowers, M.R.; Allen, S.L.; Lewandowski, S.L.; Vierra, E.C.; d’Avila, A. Association between Incomplete Surgical Ligation of Left Atrial Appendage and Stroke and Systemic Embolization. Heart Rhythm. 2015, 12, 1431–1437. [Google Scholar] [CrossRef] [PubMed]
- Koizumi, R.; Funamoto, K.; Hayase, T.; Kanke, Y.; Shibata, M.; Shiraishi, Y.; Yambe, T. Numerical Analysis of Hemodynamic Changes in the Left Atrium Due to Atrial Fibrillation. J. Biomech. 2015, 48, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Fyrenius, A.; Wigström, L.; Ebbers, T.; Karlsson, M.; Engvall, J.; Bolger, A.F. Three Dimensional Flow in the Human Left Atrium. Heart 2001, 86, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Bansal, M.; Kasliwal, R.R. Echocardiography for Left Atrial Appendage Structure and Function. Indian Heart J. 2012, 64, 469–475. [Google Scholar] [CrossRef]
- García-Fernández, M.A.; Torrecilla, E.G.; Román, D.S.; Azevedo, J.; Bueno, H.; Moreno, M.M.; Delcán, J.L. Left Atrial Appendage Doppler Flow Patterns: Implications on Thrombus Formation. Am. Heart J. 1992, 124, 955–961. [Google Scholar] [CrossRef]
- Markl, M.; Lee, D.C.; Furiasse, N.; Carr, M.; Foucar, C.; Ng, J.; Carr, J.; Goldberger, J.J. Left Atrial and Left Atrial Appendage 4D Blood Flow Dynamics in Atrial Fibrillation. Circ. Cardiovasc. Imaging 2016, 9, e004984. [Google Scholar] [CrossRef]
- Doost, S.N.; Ghista, D.; Su, B.; Zhong, L.; Morsi, Y.S. Heart Blood Flow Simulation: A Perspective Review. Biomed. Eng. Online 2016, 15, 101. [Google Scholar] [CrossRef]
- Heijman, J.; Guichard, J.-B.; Dobrev, D.; Nattel, S. Translational Challenges in Atrial Fibrillation. Circ. Res. 2018, 122, 752–773. [Google Scholar] [CrossRef]
- Grandi, E.; Dobrev, D.; Heijman, J. Computational Modeling: What Does It Tell Us about Atrial Fibrillation Therapy? Int. J. Cardiol. 2019, 287, 155–161. [Google Scholar] [CrossRef]
- Aronis, K.N.; Ali, R.; Trayanova, N.A. The Role of Personalized Atrial Modeling in Understanding Atrial Fibrillation Mechanisms and Improving Treatment. Int. J. Cardiol. 2019, 287, 139–147. [Google Scholar] [CrossRef]
- Augustin, C.M.; Fastl, T.E.; Neic, A.; Bellini, C.; Whitaker, J.; Rajani, R.; O’Neill, M.D.; Bishop, M.J.; Plank, G.; Niederer, S.A. The Impact of Wall Thickness and Curvature on Wall Stress in Patient-Specific Electromechanical Models of the Left Atrium. Biomech. Model. Mechanobiol. 2020, 19, 1015–1034. [Google Scholar] [CrossRef] [PubMed]
- Mittal, R.; Seo, J.H.; Vedula, V.; Choi, Y.J.; Liu, H.; Huang, H.H.; Jain, S.; Younes, L.; Abraham, T.; George, R.T. Computational Modeling of Cardiac Hemodynamics: Current Status and Future Outlook. J. Comput. Phys. 2016, 305, 1065–1082. [Google Scholar] [CrossRef]
- Dueñas-Pamplona, J.; García, J.G.; Sierra-Pallares, J.; Ferrera, C.; Agujetas, R.; López-Mínguez, J.R. A Comprehensive Comparison of Various Patient-Specific CFD Models of the Left Atrium for Atrial Fibrillation Patients. Comput. Biol. Med. 2021, 133, 104423. [Google Scholar] [CrossRef]
- Otani, T.; Al-Issa, A.; Pourmorteza, A.; McVeigh, E.R.; Wada, S.; Ashikaga, H. A Computational Framework for Personalized Blood Flow Analysis in the Human Left Atrium. Ann. Biomed. Eng. 2016, 44, 3284–3294. [Google Scholar] [CrossRef] [PubMed]
- Bosi, G.M.; Cook, A.; Rai, R.; Menezes, L.J.; Schievano, S.; Torii, R.; Burriesci, G. Computational Fluid Dynamic Analysis of the Left Atrial Appendage to Predict Thrombosis Risk. Front. Cardiovasc. Med. 2018, 5, 34. [Google Scholar] [CrossRef] [PubMed]
- Fanni, B.M.; Capellini, K.; di Leonardo, M.; Clemente, A.; Cerone, E.; Berti, S.; Celi, S. Correlation between LAA Morphological Features and Computational Fluid Dynamics Analysis for Non-Valvular Atrial Fibrillation Patients. Appl. Sci. 2020, 10, 1448. [Google Scholar] [CrossRef]
- García-Villalba, M.; Rossini, L.; Gonzalo, A.; Vigneault, D.; Martinez-Legazpi, P.; Durán, E.; Flores, O.; Bermejo, J.; McVeigh, E.; Kahn, A.M.; et al. Demonstration of Patient-Specific Simulations to Assess Left Atrial Appendage Thrombogenesis Risk. Front. Physiol. 2021, 12, 596596. [Google Scholar] [CrossRef]
- Vella, D.; Monteleone, A.; Musotto, G.; Bosi, G.M.; Burriesci, G. Effect of the Alterations in Contractility and Morphology Produced by Atrial Fibrillation on the Thrombosis Potential of the Left Atrial Appendage. Front. Bioeng. Biotechnol. 2021, 9, 586041. [Google Scholar] [CrossRef]
- Wang, L.; Wang, Z.; Fang, R.; Li, Z.Y. Evaluation of Stroke Risk in Patients with Atrial Fibrillation Using Morphological and Hemodynamic Characteristics. Front. Cardiovasc. Med. 2022, 9, 842364. [Google Scholar] [CrossRef]
- Corti, M.; Zingaro, A.; Dede, L.; Quarteroni, A.M. Impact of Atrial Fibrillation on Left Atrium Haemodynamics: A Computational Fluid Dynamics Study. Comput. Biol. Med. 2022, 150, 106143. [Google Scholar] [CrossRef]
- Aguado, A.M.; Olivares, A.L.; Yaguë, C.; Silva, E.; Nuñez-Garciá, M.; Fernandez-Quilez, Á.; Mill, J.; Genua, I.; Arzamendi, D.; de Potter, T.; et al. In Silico Optimization of Left Atrial Appendage Occluder Implantation Using Interactive and Modeling Tools. Front. Physiol. 2019, 10, 237. [Google Scholar] [CrossRef] [PubMed]
- Mill, J.; Olivares, A.L.; Silva, E.; Genua, I.; Fernandez, A.; Aguado, A.; Nuñez-Garcia, M.; de Potter, T.; Freixa, X.; Camara, O. Joint Analysis of Personalized In-Silico Haemodynamics and Shape Descriptors of the Left Atrial Appendage. In Statistical Atlases and Computational Models of the Heart, Proceedings of the Atrial Segmentation and LV Quantification Challenges: 9th International Workshop, STACOM 2018, Held in Conjunction with MICCAI 2018, Granada, Spain, 16 September 2018; Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2019; Volume 11395, pp. 58–66. [Google Scholar]
- Ghodrati-Misek, M.; Schlöglhofer, T.; Gross, C.; Maurer, A.; Zimpfer, D.; Beitzke, D.; Zonta, F.; Moscato, F.; Schima, H.; Aigner, P. Left Atrial Appendage Occlusion in Ventricular Assist Device Patients to Decrease Thromboembolic Events: A Computer Simulation Study. Front. Physiol. 2022, 13, 1010862. [Google Scholar] [CrossRef] [PubMed]
- Alinezhad, L.; Ghalichi, F.; Ahmadlouydarab, M.; Chenaghlou, M. Left Atrial Appendage Shape Impacts on the Left Atrial Flow Hemodynamics: A Numerical Hypothesis Generating Study on Two Cases. Comput. Methods Programs Biomed. 2022, 213, 106506. [Google Scholar] [CrossRef]
- Dillon-Murphy, D.; Marlevi, D.; Ruijsink, B.; Qureshi, A.; Chubb, H.; Kerfoot, E.; O’Neill, M.; Nordsletten, D.; Aslanidi, O.; de Vecchi, A. Modeling Left Atrial Flow, Energy, Blood Heating Distribution in Response to Catheter Ablation Therapy. Front. Physiol. 2018, 9, 1757. [Google Scholar] [CrossRef] [PubMed]
- Dueñas-Pamplona, J.; García, J.G.; Castro, F.; Muñoz-Paniagua, J.; Goicolea, J.; Sierra-Pallares, J. Morphing the Left Atrium Geometry: A Deeper Insight into Blood Stasis within the Left Atrial Appendage. Appl. Math. Model. 2022, 108, 27–45. [Google Scholar] [CrossRef]
- Gonzalo, A.; García-Villalba, M.; Rossini, L.; Durán, E.; Vigneault, D.; Martínez-Legazpi, P.; Flores, O.; Bermejo, J.; McVeigh, E.; Kahn, A.M.; et al. Non-Newtonian Blood Rheology Impacts Left Atrial Stasisin Patient-Specific Simulations. Int. J. Numer. Method. Biomed. Eng. 2022, 38, e3597. [Google Scholar] [CrossRef]
- Wang, Y.; Qiao, Y.; Mao, Y.; Jiang, C.; Fan, J.; Luo, K. Numerical Prediction of Thrombosis Risk in Left Atrium under Atrial Fibrillation. Math. Biosci. Eng. 2020, 17, 2348–2360. [Google Scholar] [CrossRef]
- Yang, J.; Song, C.; Ding, H.; Chen, M.; Sun, J.; Liu, X. Numerical Study of the Risk of Thrombosis in the Left Atrial Appendage of Chicken Wing Shape in Atrial Fibrillation. Front. Cardiovasc. Med. 2022, 9, 985674. [Google Scholar] [CrossRef]
- García-Isla, G.; Olivares, A.L.; Silva, E.; Nuñez-Garcia, M.; Butakoff, C.; Sanchez-Quintana, D.; Morales, H.G.; Freixa, X.; Noailly, J.; de Potter, T.; et al. Sensitivity Analysis of Geometrical Parameters to Study Haemodynamics and Thrombus Formation in the Left Atrial Appendage. Int. J. Numer. Method. Biomed. Eng. 2018, 34, e3100. [Google Scholar] [CrossRef]
- Mill, J.; Agudelo, V.; Olivares, A.L.; Pons, M.I.; Silva, E.; Nuñez-Garcia, M.; Morales, X.; Arzamendi, D.; Freixa, X.; Noailly, J.; et al. Sensitivity Analysis of in Silico Fluid Simulations to Predict Thrombus Formation after Left Atrial Appendage Occlusion. Mathematics 2021, 9, 2304. [Google Scholar] [CrossRef]
- Fang, R.; Li, Y.; Wang, J.; Wang, Z.; Allen, J.; Ching, C.K.; Zhong, L.; Li, Z. Stroke Risk Evaluation for Patients with Atrial Fibrillation: Insights from Left Atrial Appendage. Front. Cardiovasc. Med. 2022, 9, 968630. [Google Scholar] [CrossRef]
- Masci, A.; Barone, L.; Dedè, L.; Fedele, M.; Tomasi, C.; Quarteroni, A.; Corsi, C. The Impact of Left Atrium Appendage Morphology on Stroke Risk Assessment in Atrial Fibrillation: A Computational Fluid Dynamics Study. Front. Physiol. 2019, 9, 1938. [Google Scholar] [CrossRef] [PubMed]
- Polaczek, M.; Szaro, P.; Baranska, I.; Burakowska, B.; Ciszek, B. Morphology and Morphometry of Pulmonary Veins and the Left Atrium in Multi-Slice Computed Tomography. Surg. Radiol. Anat. 2019, 41, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.T.; Gay, M. Characterizing Left Atrial Appendage Functions in Sinus Rhythm and Atrial Fibrillation Using Computational Models. J. Biomech. 2008, 41, 2515–2523. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.K.; Shah, A.M.; Giugliano, R.P.; Ruff, C.T.; Antman, E.M.; Grip, L.T.; Deenadayalu, N.; Hoffman, E.; Patel, I.; Shi, M.; et al. Left Atrial Structure and Function in Atrial Fibrillation: ENGAGE AF-TIMI 48. Eur. Heart J. 2014, 35, 1457–1465. [Google Scholar] [CrossRef] [PubMed]
- Vignon-Clementel, I.E.; Alberto Figueroa, C.; Jansen, K.E.; Taylor, C.A. Outflow Boundary Conditions for Three-Dimensional Finite Element Modeling of Blood Flow and Pressure in Arteries. Comput. Methods Appl. Mech. Eng. 2006, 195, 3776–3796. [Google Scholar] [CrossRef]
- Politis, A.K.; Stavropoulos, G.P.; Christolis, M.N.; Panagopoulos, F.G.; Vlachos, N.S.; Markatos, N.C. Numerical Modeling of Simulated Blood Flow in Idealized Composite Arterial Coronary Grafts: Steady State Simulations. J. Biomech. 2007, 40, 1125–1136. [Google Scholar] [CrossRef]
- Grigoriadis, G.I.; Sakellarios, A.I.; Kosmidou, I.; Naka, K.K.; Ellis, C.; Michalis, L.K.; Fotiadis, D.I. Wall Shear Stress Alterations at Left Atrium and Left Atrial Appendage Employing Abnormal Blood Velocity Profiles. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; Volume 82, pp. 2565–2568. [Google Scholar]
- Belkacemi, D.; Al-Rawi, M.; Abbes, M.T.; Laribi, B. Flow Behaviour and Wall Shear Stress Derivatives in Abdominal Aortic Aneurysm Models: A Detailed CFD Analysis into Asymmetry Effect. CFD Lett. 2022, 14, 60–74. [Google Scholar] [CrossRef]
- Rigatelli, G.; Zuin, M.; Roncon, L. Increased Blood Residence Time as Markers of High-Risk Patent Foramen Ovale. Transl. Stroke Res. 2022, 14, 304–310. [Google Scholar] [CrossRef]
- Morales Ferez, X.; Mill, J.; Juhl, K.A.; Acebes, C.; Iriart, X.; Legghe, B.; Cochet, H.; De Backer, O.; Paulsen, R.R.; Camara, O. Deep Learning Framework for Real-Time Estimation of in-Silico Thrombotic Risk Indices in the Left Atrial Appendage. Front. Physiol. 2021, 12, 694945. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).