
Pulse Oximetry as a Diagnostic Tool to Determine Pulp Vitality: A Systematic Review

 , ,
, ,  , and
, and
Featured Application
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy

{kind=link}
| Database | Search Strategy | Findings |
|---|---|---|
| Medline | #1 (pulse oximetry OR pulse oximeter) | 20.599 |
| #2 (pulp vitality test?) OR (pulp vitality OR vitality OR endod *) | 81.205 | |
| #1 AND #2 | 83 | |
| Web of Science | #1 TS = (pulse oximetry OR pulse oximeter) | 10.241 |
| #2 TS = (pulp vitality test? OR pulp vitality OR vitality OR endod *) | 55.169 | |
| #1 AND #2 | 65 | |
| Scopus | #1 ALL (pulse oximetry OR pulse oximeter) | 5.028 |
| #2 ALL (pulp vitality test? OR pulp vitality OR vitality OR endod *) | 1.305 | |
| #1 AND #2 | 89 | |
| Embase | #1 (pulse oximetry OR pulse oximeter) | 22.203 |
| #2 (pulp vitality test? OR pulp vitality OR vitality OR endod *) | 105.375 | |
| #1 AND #2 | 75 |
2.2. Eligibility Criteria
2.3. Study Selection
2.4. Data Extraction
2.5. Quality Assessment
3. Results
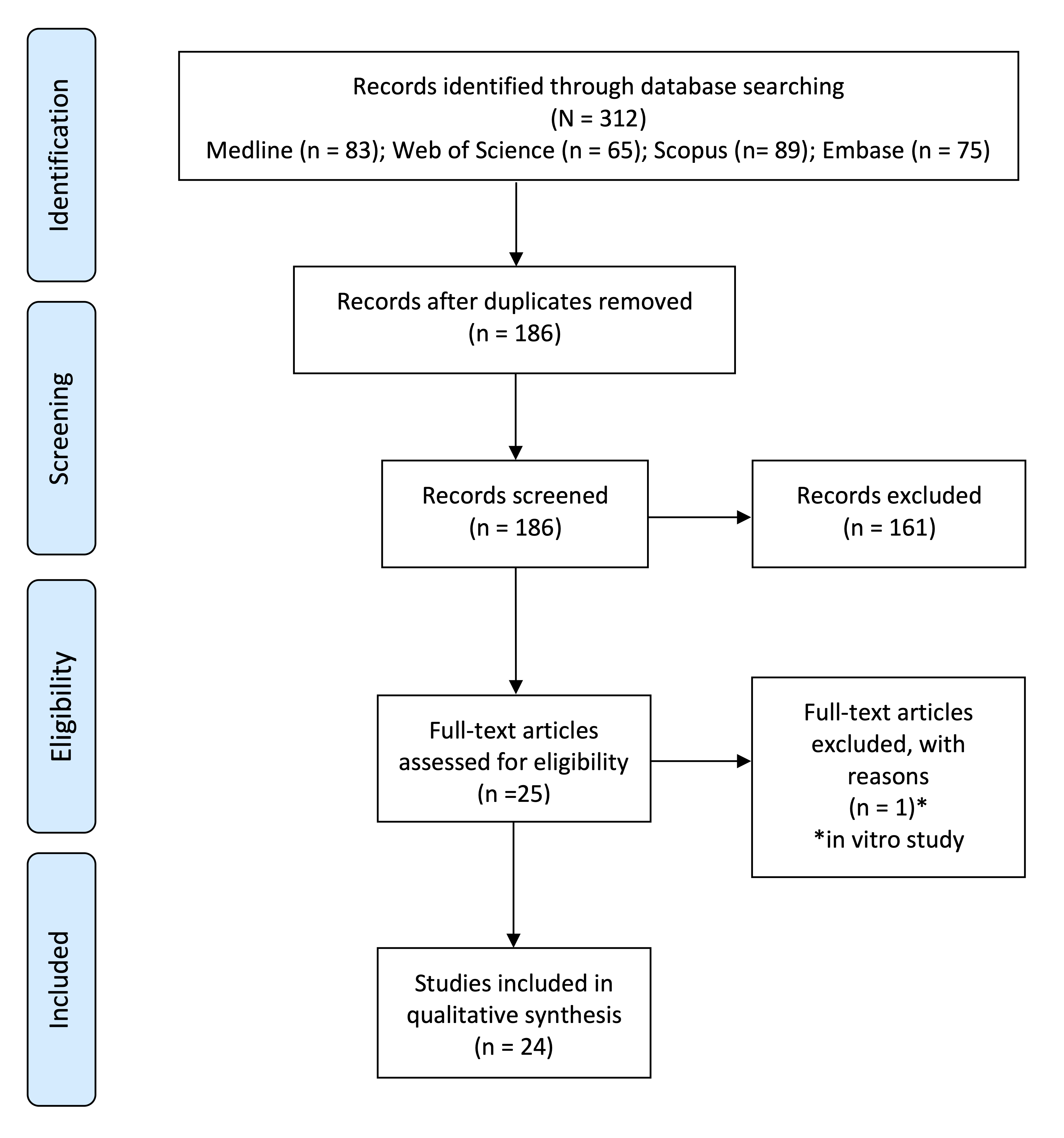
3.1. Search Results and Study Selection
3.2. Study Characteristics and Methodology
| Author | Country | Institution | Journal | Type of Study |
|---|---|---|---|---|
| J. Schnettler (1991) [25] | USA | Case Western Reserve University | Journal of Endodontics | Cross-Sectional |
| R. Kahan (1996) [11] | UK | University College Hospital | Journal of Endodontics | Cross-Sectional |
| V. Gopikrishna (2007) A [10] | India | Meenakshi Ammal Dental College | Journal of Endodontics | Cross-Sectional |
| V. Gopikrishna (2007) B [20] | India | Meenakshi Ammal Dental College | Journal of Endodontics | Cross-Sectional |
| E. Calil (2008) [17] | Brazil | University of São Paulo | International Endodontic Journal | Cross-Sectional |
| H. Karayilmaz (2011) [29] | Turkey | Süleyman Demirel Universitesi | Journal of Oral Rehabilitation | Cross-Sectional |
| S. Kataoka (2011) [21] | Brazil | University of São Paulo | Journal of Endodontics | Cross-Sectional |
| N. Dastmalchi (2012) [9] | Iran | Mashland University of Medical Sciences | Journal of Endodontics | Cross-Sectional |
| F. Setzer (2012) [26] | USA | University of Pennsylvania | Journal of Endodontics | Cross-Sectional |
| M. Sadique (2014) [32] | India | Kunhitharuvai Memorial Charitable Trust Dental College | Journal of International Oral Health | Cross-Sectional |
| L. Bergesch (2014) [16] | Brazil | Lutheran University of Brazil | Journal of Endodontics | Cross-Sectional |
| J. Stella (2015) [33] | Brazil | Lutheran University of Brazil | Journal of Endodontics | Cross-Sectional |
| D. Kosturkov (2015) [31] | Bulgaria | Medical University of Sofia | Journal of IMAB | Cross-Sectional |
| C. Caldeira (2016) [4] | Brazil | University of São Paulo | Journal of Clinical and Diagnostic Research | Cross-Sectional |
| H-J Kong (2016) [24] | Korea | Chungman National University Hospital | Acta Odontologica Scandinavica | Cross-Sectional |
| S. Kataoka (2016) [22] | Brazil | University of São Paulo | Journal of Endodontics | Cross-Sectional |
| A. Khademi (2017) [23] | Iran | Torabinejad Dental Center of Investigation | The Journal of Craniofacial Surgery | Cross-Sectional |
| B. Anusha (2017) [15] | India | Narayana Dental College and Hospital | Journal of Clinical and Diagnostic Research | Cross-Sectional |
| C. Estrela (2017) A [18] | Brazil | Ferederal university of Goiás | Brazilian Dental Journal | Cross-Sectional |
| C. Estrela (2017) B [19] | Brazil | Ferederal University of Goiás | Brazilian Dental Journal | Cross-Sectional |
| S. Souza (2017) [28] | Brazil | Federal University of Maranhão | Journal of Endodontics | Cross-Sectional |
| D. Kosturkov (2017) [30] | Bulgaria | Medical University of Sofia | Acta Medica Bulgarica | Cross-Sectional |
| C. Solda (2018) [27] | Brazil | School of Dentistry | Brazilian Dental Journal | Cross-Sectional |
| K. Janani (2020) [2] | India | Saveetha Dental College and Hospital | Brazilian Dental Science | Cross-Sectional |
| Author | Teeth | Sample | Age | Patients | Test | Measure | Pulse Oximeter |
|---|---|---|---|---|---|---|---|
| J. Schnettler (1991) [25] | UCI | Study: 44 PCG: - NCG: 5 | - | 49 | PO CT EPT | SpO2 | Novametrix pulse oximeter |
| R. Kahan (1996) [11] | UCI LCI | Study: 20 PCG: 10 (finger) NCG: - | - | 10 | PO CT EPT | SpO2 | Ohmeda Biox 3740 (Ohmeda, BOC HEalth Care, Louisville, CO, USA) |
| V. Gopikrishna (2007) A [10] | UI | Study: 17 PCG: 30 NCG: 30 | - | 47 | PO CT | SpO2 | Nellcor OxiMax 550 5th generation (Tycor Healthcare Group LP) Nellcor OxiMaxTM Dura-Y D-YS Sensor (Tyco Healthcare Group LP). A probe was fabricated. |
| V. Gopikrishna (2007) B [20] | I C P | Study: 80 PCG: 80 NCG: - | - | 80 | PO CT | SpO2 | Nellcor OxiMax 550 5th generation (Tycor Healthcare Group LP) Sensor Nellcor OxiMaxTM Dura-Y D-YS (Tyco Healthcare Group LP). A probe was fabricated |
| E. Calil (2008) [17] | UCI UC | Study: 60 PCG: - NCG: 10 | 26–38 | 17 | PO CT | SaO2 | Oxygraph System Partner Ltd.a., (São Caetano do Sul, SP, Brazil) Adapted sensor for ental use (System Partner Ltd.a). |
| H. Karayilmaz (2011) [29] | UCI ULI | Study: 59 PCG: 59 NCG: - | 12–18 | 28 w 23 m | PO LDF EPT | Sensitivity Specificity | Life Scope I, Multiparameter Bedside Monitor (Modelo BSM-2301K (Nihon Kohden Corp., Tokyo, Japan) A probe was fabricated |
| S. Kataoka (2011) [21] | UI UC LI LC | Study: 40 PCG: - NCG: - | 35–55 | 20 | PO CT | SpO2 | Oxygraph pulse oximeter (System Partner, São Paulo, Brazil) with tyte Y modificed sensors |
| N. Dastmalchi (2012) [9] | P | Study: 24 PCG: 24 NCG: - | 18–50 | 24 | PO CT HT EPT | Sensitivity Specificity PPV NPV | 520a pulse oximeter, (Novametrix, Wallingford, CT, USA) |
| F. Setzer (2012) [26] | UP LP UM LM | Study: 60 PCG: 60 NCG: 60 | 25–55 | 28 w 30 m | PO CT HT | SpO2 | Oxygraph, System Partner (São Paulo, Brazil) Modified type Y sensors |
| M. Sadique (2014) [32] | UCI ULI UC | Study: 60 PCG: 60 (finger) NCG: 30 | 15–40 | 60 | PO | SpO2 | Criticare 504-US oxygen sensor |
| L. Bergesch (2014) [16] | Anterior | Study: 67 PCG: 30 NCG: - | 32–64 | 35 | PO CT EPT | SpO2 | Portabel pediatric pulse oximeter (3301; Smiths Medical PM INC., Waukesha, WI, USA) Sensors: 3025 (tooth) y 3026 (finger) A probe was fabricated |
| J. Stella (2015) [33] | CI | Study: 110 PCG: - NCG: - | 7–36 | 57 | PO | SpO2 | BCI 3301 pediatric (Smiths Medical PM Inc., Waukesha, WI, USA)Sensor 3025 A probe was fabricated |
| D. Kosturkov (2015) [31] | Anterior | Study: 1058 PCG: - NCG: - | 18–25 | 31 | PO EPT | SpO2 | Pulse oximeter ConectTM—CMS60DSpecial holder fabricated |
| C. Caldeira (2016) [4] | I C P | Study: 59 PCG: 46 NCG: 10 | 14–42 | 46 | PO CT | SpO2 | Oxigraph, System Partner (Sao Caetano do Sul, Brazil) |
| H-J Kong (2016) [24] | UCI | Study: 30 PCG: - NCG: - | 24–40 | 15 | PO CT EPT | Perfusion index SpO2 | Modified Nellcor sensor compatible with a comercial pulse oximeter (MP-570T, MEKICS Co., Paju, Korea) |
| S. Kataoka (2016) [22] | I C | Study: 693 PCG: 693 NCG: - | 35–65 | 180 | PO CT | SpO2 | Oxygraph pulse oximeter (System Partner, São Paulo, Brazil) with type Y modified sensors. |
| A. Khademi (2017) [23] | UC | PCG: 20 NCG: 20 | 13–24 | 11 w 9 m | PO CT EPT | SpO2 | Criticare 504 (Criticare, Waukesha, WI) |
| B. Anusha (2017) [15] | UCI ULI UC LCI LLI LC | Study: 60 PCG: 20 NCG: 20 | 25–40 | 48 w 52 m | PO CT GT | SpO2 | Monitor: B20, GE, Finland Sensor: B20, GE, Finland |
| C. Estrela (2017) A [18] | UM LM | Study: 112 PCG: - NCG: 10 | 17–40 | 11 w 11 m | PO CT | SaO2 | BCI 3301 pediatric (Smiths Medical PM Inc., Waukesha, WI, USA) Sensor: 3025 (tooth), 3026 (finger) A probe was fabricated |
| C. Estrela (2017) B [19] | UP | Study: 120 PCG: - NCG: - | 20–44 | 100 | PO CT | SaO2 | BCI 3301 pediatric (Smiths Medical PM Inc., Waukesha, WI, USA) Sensor: 3025 (tooth), 3026 (finger) A probe was fabricated |
| S. Souza (2017) [28] | I C P M | Study: 728 PCG: - NCG: 1815 | Mean: 30 | 359 | PO CT | SpO2 | MD300A (IMFtec Tecnologia para Saúde LTDA, São Paulo, SP, Brazil) |
| D. Kosturkov (2017) [30] | Anterior and posterior | Study: 31 PCG: 78 NCG: - | - | 45 | PO EPT | SpO2 | Contect CMS 60D with modified probe |
| C. Solda (2018) [27] | UCI | Study: 68 PCG: - NCG: 10 | 19–36 | 41 w 27 m | PO CT | SaO2 | Portable pediatric pulse oximeter (BCI 3301, Smiths Medical PM Inc., Waukesha, WI, USA) 3026 sensors (for fingers) Adapter specifically fabricated |
| K. Janani (2020) [2] | I C LP | Study: 37 PCN: Finger (17) NCG: - | 18–50 | 37 | PO CT HT EPT | SpO2 | Monitor: Nellcor N-600 (Healthcare group LP, Pleasanton, CA, USA). Sensor: N3 oxy sensor (Healthcare group LP, Pleasanton, CA, USA). Sensor holder designed and custom made. |
3.3. Study Results
| Author | UI | UC | UP | UM | LI | LC | LP | LM |
|---|---|---|---|---|---|---|---|---|
| R. Kahan (1996) [11] | 28.95% (10) | - | - | - | 50.28% (10) | - | - | - |
| E. Calil (2008) [17] | 91.29% (30) | 90.69% (30) | - | - | - | - | - | - |
| M. Sadique (2014) [32] | UCI: 85.11% (15) ULI:80.21% (15) | 89.55% | - | - | - | - | - | - |
| J. Stella (2015) [33] | 81.25% | - | - | - | - | - | - | - |
| D. Kosturkov (2015) [31] | UCI: 84.4% ULI: 83.4% | 83.4% | - | - | LCI: 83.5% LLI: 82% | 84.5% | - | - |
| S. Kataoka (2016) [22] | SG UCI: 89–98% ULI: 90–98% CG UCI: 89–98% ULI: 90–98% | SG: 89–96% CG: 89–95% | - | - | SG LCI: 89–96% LLI: 88–96% CG LCI: 89–96% LLI: 89–97% | SG: 89–95% CG: 90–96% | - | - |
| C. Estrela (2017) A [18] | - | - | - | 83.59% (61) | - | - | - | 86.89% (51) |
| S. Souza (2017) [28] | HbSS UCI: 78% ULI: 79% HbAA UCI: 89% ULI: 87% | HbSS: 87% HbAA: 86% | HbSS: 87% HbAA: 91% | HbSS: 75% HbAA: 89% | HbSS LCI: 86% LLI: 93% HbAA: LCI:83% LLI:91% | HbSS: 93% HbAA: 90% | HbSS: 88% HbAA: 88% | HbSS: 89% HbAA: 89% |
| C. Solda (2018) [27] | UCI: 84.9% ULI: 85.4% | - | - | - | - | - | - | - |
| Author | PC | RP | IP | PN | NC |
|---|---|---|---|---|---|
| F. Setzer (2012) [26] | 92.2% | 87.4% | 83.1% | 74.6% | 0% |
| C. Caldeira (2016) [4] | 93% | 92% | 89% | 71% | 0% |
| B. Anusha (2017) [15] | 94.6% | 85.45% | 81.6% | 70.7% | 0% |
| D. Kosturkov (2017) [30] | 81.47% | 93.81% | - | - | - |
3.4. Quality Assessment
| Study | Risk of Bias | Applicability Concerns | |||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
| J. Schnettler (1991) [25] |  | | | | | | |
| R. Kahan (1996) [11] | |  | | | | | |
| V. Gopikrishna (2007) A [10] | | | | | | | |
| V. Gopikrishna (2007) B [20] | | | | | | | |
| E. Calil (2008) [17] | | | | | | | |
| H. Karayilmaz (2011) [29] | | | | | | | |
| S. Kataoka (2011) [21] | | | | | | | |
| N. Dastmalchi (2012) [9] | | | | | | | |
| F. Setzer (2012) [26] | | | | | | | |
| M. Sadique (2014) [32] | | | | | | | |
| L. Bergesch (2014) [16] | | | | | | | |
| J. Stella (2015) [33] | | | | | | | |
| D. Kosturkov (2015) [31] | | | | | | | |
| C. Caldeira (2016) [4] | | | | | | | |
| H-J Kong (2016) [24] | | | | | | | |
| S. Kataoka (2016) [22] | | | | | | | |
| A. Khademi (2017) [23] | | | | | | | |
| B. Anusha (2017) [15] | | | | | | | |
| C. Estrela (2017) A [18] | | | | | | | |
| C. Estrela (2017) B [19] | | | | | | | |
| S. Souza (2017) [28] | | | | | | | |
| D. Kosturkov (2017) [30] | | | | | | | |
| C. Solda (2018) [27] | | | | | | | |
| K. Janani (2020) [2] | | | | | | | |
Low Risk, High Risk.4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alghaithy, R.A.; Qualtrough, A. Pulp sensibility and vitality tests for diagnosing pulpal health in permanent teeth: A critical review. Int. Endod. J. 2017, 50, 135–142. [Google Scholar] [CrossRef]
- Janani, K.; Palanivelu, A.; Sandhya, R. Diagnostic accuracy of dental oximeter with customized sensor holder, thermal test and electric pulp test for the evaluation of pulp vitality: An in vivo study. Braz. Dent. Sci. 2020, 23, 1–8. [Google Scholar] [CrossRef]
- Ghouth, N.; Duggal, M.S.; BaniHani, A.; Nazzal, H. The diagnostic accuracy of laser Doppler flowmetry in assessing pulp blood flow in permanent teeth: A systematic review. Dent. Traumatol. 2018, 34, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Caldeira, C.L.; Barletta, F.B.; Ilha, M.C.; Abrão, C.V.; Gavini, G. Pulse oximetry: A useful test for evaluating pulp vitality in traumatized teeth. Dent. Traumatol. 2016, 32, 385–389. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Abbott, P.V. Dental pulp testing: A Review. Int. J. Dent. 2009. [Google Scholar] [CrossRef] [PubMed]
- Pozzobon, M.H.; Sousa Vieira, R.; Hecke Alves, A.M.; Reyes-Carmona, J.; Silveira Teixeira, C.; Mendes de Souza, B.C.; Tadeu Felippe, W. Assessment of pulp blood flow in primary and permanent teeth using pulse oximetry. Dent. Traumatol. 2011, 27, 184–188. [Google Scholar] [CrossRef]
- Jafarzadeh, H.; Rosenberg, P. Pulse Oximetry: Review of a potential aid in endodontic diagnosis. J. Endod. 2009, 35, 329–333. [Google Scholar] [CrossRef] [PubMed]
- Bargrizan, M.; Ashari, M.A.; Ahmadi, M.; Ramezani, J. The use of pulse oximetry in evaluation of pulp vitality in immature permanent teeth. Dent. Traumatol. 2016, 32, 43–47. [Google Scholar] [CrossRef] [PubMed]
- Dastmalchi, N.; Jafarzadeh, H.; Moradi, S. Comparison of the efficacy of a custom-made pulse oximeter probe with digital electric pulp tester, cold spray, and rubber cup for assessing pulp vitality. J. Endod. 2012, 38, 1182–1186. [Google Scholar] [CrossRef]
- Gopikrishna, V.; Tinagupta, K.; Kandaswamy, D. Comparison of electrical, thermal and pulse oximetry methods for assessing pulp vitality in recently traumatized teeth. J. Endod. 2007, 35, 531–535. [Google Scholar] [CrossRef]
- Kahan, R.S.; Gulabivala, K.; Snook, M.; Setchell, D.J. Evaluation of a pulse oximeter and customized probe for pulp vitality testing. J. Endod. 1996, 22, 105–109. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.; Loannidis, J.; Clarke, M.; Devereauz, J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M.; the QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Anusha, B.; Madhusudhana, K.; Kumar Chinni, S.; Paramesh, Y. Assessment of pulp oxygen saturation levels by pulse oximetry for pulpal diseases—A diagnostic study. J. Clin. Diagn. Res. 2017, 11, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Bergesch, L.; Barletta, F.B.; Felippe, W.T.; Bruno, K.F.; Gonçalves de Alencar, A.H.; Estrela, C. Assessment of oxygen saturation in dental pulp of permanent teeth with periodontal disease. J. Endod. 2014, 40, 1927–1931. [Google Scholar]
- Calil, E.; Caldeira, C.L.; Gavini, G.; Lemos, E.M. Determination of pulp vitality in vivo with pulse oximetry. Int. Endod. J. 2008, 41, 741–746. [Google Scholar] [CrossRef]
- Estrela, C.; Oliveira, K.; Alencar, A.H.G.; Barletta, F.B.; Estrela, C.; Felippe, W.T. Oxygen saturation in the dental pulp of maxillary premolars in different age groups—Part 2. Braz. Dent. J. 2017, 28, 704–709. [Google Scholar] [CrossRef]
- Estrela, C.; Serpa, G.C.; Alencar, A.H.; Bruno, K.F.; Barletta, F.B.; Felippe, W.T.; Estrela, C.; Souza, J.B. Oxygen saturation in the dental pulp of maxillary premolars in different age groups—Part 1. Braz. Dent. J. 2017, 28, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Gopikrishna, V.; Tinagupta, K.; Kandaswamy, D. Evaluation of efficacy of a new custom-made pulse oximeter dental probe in comparison with the electrical and thermal tests for assessing pulp vitality. J. Endod. 2007, 33, 411–414. [Google Scholar] [CrossRef]
- Kataoka, S.H.; Setzer, F.C.; Gondim-Junior, E.; Faciola Pessoa, O.; Gavini, G.; Caldeira, C.L. Pulp vitality in patients with intraoral and oropharyngeal malignant tumors undergoing radiation therapy assessed by pulse oximetry. J. Endod. 2011, 36, 1197–1200. [Google Scholar] [CrossRef]
- Kataoka, S.H.; Setzer, F.C.; Gondim-Junior, E.; Fregnani, E.R.; Moraes, C.J.; Faciola Pessoa, O.; Gavini, G.; Caldeira, C.L. Late effects of head and neck radiotherapy on pulp vitality assessed by pulse oximetry. J. Endod. 2016, 42, 886–889. [Google Scholar] [CrossRef] [PubMed]
- Khademi, A.; Shahtouri, M.; Attar, B.; Rikhtergaran, N. Pulp vitality of maxillary canines after alveolar cleft bona grafting: Pulse oximetry versus electric pulp test versus cold test. J. Craniofacial Surg. 2017. [Google Scholar] [CrossRef]
- Kong, H.J.; Jeon Shin, T.; Hyun, H.K.; Kim, Y.J.; Kim, J.K.; Shon, W.J. Oxygen saturation and perfusion index from pulse oximetry in adult volunteers with viable incisors. Acta Odontol. Scand. 2016, 74, 411–415. [Google Scholar] [CrossRef]
- Schnettler, J.; Wallace, J. Pulse oximetry as a diagnostic tool of pulpal vitality. J. Endod. 1991, 17, 488–490. [Google Scholar] [CrossRef]
- Setzer, F.; Kataoka, S.H.; Natrielli, F.; Gondim-Junior, E.; Caldeira, C. Clinical diagnosis of pulp inflammation based on pulp oxygenation rates measured by pulse oximetry. J. Endod. 2012, 38, 880–883. [Google Scholar] [CrossRef] [PubMed]
- Solda, C.; Barletta, F.; Vanni, J.; Lambert, P.; Só, M.; Estrela, C. Effect of at-home bleaching on oxygen saturation levels in the dental pulp of maxilarry central incisors. Braz. Dent. J. 2018, 29, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Souza, S.; Thomaz, E.; Costa, C. Healthy dental pulp oxygen saturation rates in subjects with homozygous sickle cell anemia: A cross-sectional study nested in a cohort. J. Endod. 2017, 43, 1997–2000. [Google Scholar] [CrossRef]
- Karayilmaz, H.; Kirzioglu, Z. Comparison of the reliability of laser doppler flowmetry, pulse oximetry and electric pulp tester in assessing the pulp vitality of human teeth. J. Oral Rehabil. 2011, 38, 340–347. [Google Scholar] [CrossRef]
- Kosturkov, D.; Uzunov, T. Pulse oximetry and electric pulp test in intact teeth and teeth with hyperaemia pulpae. Acta Med. Bulg. 2017, 44, 10–13. [Google Scholar] [CrossRef][Green Version]
- Kosturkov, D.; Uzunov, T.; Grozdanova, R.; Ivancheva, V. Evaluation of condition of the pulp by pulse oximetry. J. IMAB 2015, 21, 1003–1007. [Google Scholar] [CrossRef][Green Version]
- Sadique, M.; Ravi, S.V.; Thomas, K.; Dhanapal, P.; Simon, E.P.; Shaheen, M. Evaluation of efficacy of a pulse oximeter to assess pulp vitality. J. Int. Oral Health 2014, 6, 70–72. [Google Scholar] [PubMed]
- Stella, J.P.; Branco Barletta, F.; Bergesch Giovanella, L.; Grazziotin-Soares, R.; Ferreira Tobo, M.; Tadeu Felippe, W.; Estrela, C. Oxygen saturation in dental pulp of permanent teeth: Difference between children/adolescents and adults. J. Endod. 2015, 41, 1445–1449. [Google Scholar] [CrossRef] [PubMed]
- Levin, L. Pulp and periradicular testing. J. Endod. 2013, 39, 13–19. [Google Scholar] [CrossRef]
- Mainkar, A.; Kim, S.G. Diagnostic accuracy of 5 dental pulp tests: A systematic review and meta-analysis. J. Endod. 2018, 44, 694–702. [Google Scholar] [CrossRef]
- Bruno, K.; Brando Barletta, F.; Tadeau Felippe, W.; Almeida Silva, J.; Gonçalves de Alencar, A.H.; Estrela, C. Oxygen saturation in the dental pulp of permanent teeth: A critical review. J. Endod. 2014, 40, 1054–1057. [Google Scholar] [CrossRef]
- Saoud, T.M.A.; Ricucci, D.; Lin, L.M.; Gaengler, P. Regeneration and Repair in Endodontics—A Special Issue of the Regenerative Endodontics—A New Era in Clinical Endodontics. Dent. J. 2016, 4, 3. [Google Scholar] [CrossRef]
- Palma, P.J.; Martins, J.; Diogo, P.; Sequeira, D.; Ramos, J.C.; Diogenes, A.; Santos, J.M. Does Apical Papilla Survive and Develop in Apical Periodontitis Presence after Regenerative Endodontic Procedures? Appl. Sci. 2019, 9, 3942. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almudever-Garcia, A.; Forner, L.; Sanz, J.L.; Llena, C.; Rodríguez-Lozano, F.J.; Guerrero-Gironés, J.; Melo, M. Pulse Oximetry as a Diagnostic Tool to Determine Pulp Vitality: A Systematic Review. Appl. Sci. 2021, 11, 2747. https://doi.org/10.3390/app11062747
Almudever-Garcia A, Forner L, Sanz JL, Llena C, Rodríguez-Lozano FJ, Guerrero-Gironés J, Melo M. Pulse Oximetry as a Diagnostic Tool to Determine Pulp Vitality: A Systematic Review. Applied Sciences. 2021; 11(6):2747. https://doi.org/10.3390/app11062747
Chicago/Turabian StyleAlmudever-Garcia, Alicia, Leopoldo Forner, José Luis Sanz, Carmen Llena, Francisco Javier Rodríguez-Lozano, Julia Guerrero-Gironés, and María Melo. 2021. "Pulse Oximetry as a Diagnostic Tool to Determine Pulp Vitality: A Systematic Review" Applied Sciences 11, no. 6: 2747. https://doi.org/10.3390/app11062747
APA StyleAlmudever-Garcia, A., Forner, L., Sanz, J. L., Llena, C., Rodríguez-Lozano, F. J., Guerrero-Gironés, J., & Melo, M. (2021). Pulse Oximetry as a Diagnostic Tool to Determine Pulp Vitality: A Systematic Review. Applied Sciences, 11(6), 2747. https://doi.org/10.3390/app11062747