Sleep Bruxism Episodes in Patients with Obstructive Sleep Apnea Syndrome Determined by In-Laboratory Polysomnography




Abstract
1. Introduction
2. Materials and Methods
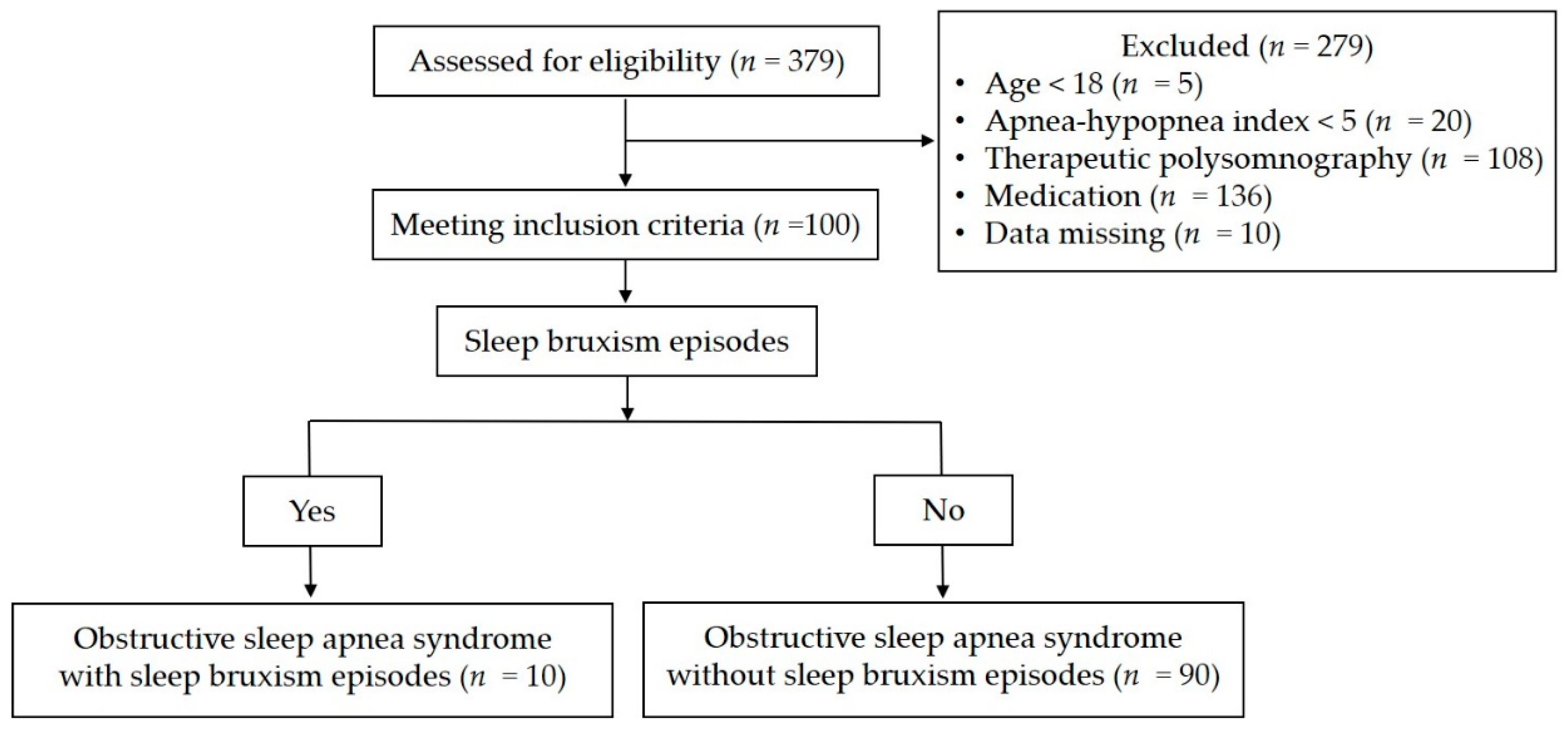
2.1. Study Design and Study Population
- they were aged <18 years;
- AHI was <5;
- they used any medications known to affect sleep or breathing;
- In-laboratory PSG was performed for a therapeutic purpose, such as the titration of CPAP; or
- the patient had neurological disorders, epilepsy, neuromuscular disease, a history of upper airway surgery, or any severe mental illness.
2.2. Ethics Statement
2.3. In-Laboratory PSG
2.4. SB Episodes
2.5. Statistical Analysis
3. Results
3.1. General Characteristics in Patients with OSAS with and without SB Episodes
3.2. Comparative Analysis of PSG Indices in Patients with OSAS with and without SB Episodes
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hou, H.; Zhao, Y.; Yu, W.; Dong, H.; Xue, X.; Ding, J.; Xing, W.; Wang, W. Association of obstructive sleep apnea with hypertension: A systematic review and meta-analysis. J. Glob. Heal. 2018, 8, 010405. [Google Scholar] [CrossRef] [PubMed]
- Vasheghani-Farahani, A.; Kazemnejad, F.; Haghighi, K.S.; Saadat, S.; Tavakolipoor, P.; Yazdani, T.; Alidoosti, M.; Ghasem-Amooeian, V.; Ashraf, H. Obstructive sleep apnea and severity of coronary artery disease. Casp. J. Intern. Med. 2018, 9, 276–282. [Google Scholar]
- Lobbezoo, F.; Ahlberg, J.; Raphael, K.G.; Wetselaar, P.; Glaros, A.G.; Kato, T.; Santiago, V.; Winocur, E.; De Laat, A.; De Leeuw, R.; et al. International consensus on the assessment of bruxism: Report of a work in progress. J. Oral Rehabil. 2018, 45, 837–844. [Google Scholar] [CrossRef] [PubMed]
- Clark, G.T.; Sohn, J.-W.; Hong, C.N. TREATING OBSTRUCTIVE SLEEP APNEA AND SNORING: ASSESSMENT OF an anterior mandibular positioning device. J. Am. Dent. Assoc. 2000, 131, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Dieltjens, M.; Vanderveken, O.M. Oral Appliances in Obstructive Sleep Apnea. Healthcare 2019, 7, 141. [Google Scholar] [CrossRef] [PubMed]
- Ng, J.H.; Yow, M. Oral Appliances in the Management of Obstructive Sleep Apnea. Sleep Med. Clin. 2019, 14, 109–118. [Google Scholar] [CrossRef] [PubMed]
- Randerath, W.J.; Heise, M.; Hinz, R.; Ruehle, K.-H. An individually adjustable oral appliance vs continuous positive airway pressure in mild-to-moderate obstructive sleep apnea syndrome. Chest 2002, 122, 569–575. [Google Scholar] [CrossRef]
- Gagnadoux, F.; Fleury, B.; Vielle, B.; Pételle, B.; Meslier, N.; N’Guyen, X.L.; Trzepizur, W.; Racineux, J.L. Titrated mandibular advancement versus positive airway pressure for sleep apnoea. Eur. Respir. J. 2009, 34, 914–920. [Google Scholar] [CrossRef]
- Landry, M.-L.; Rompré, P.H.; Manzini, C.; Guitard, F.; De Grandmont, P.; Lavigne, G.J. Reduction of sleep bruxism using a mandibular advancement device: An experimental controlled study. Int. J. Prosthodont. 2006, 19, 549–556. [Google Scholar]
- Landry-Schönbeck, A.; De Grandmont, P.; Rompré, P.H.; Lavigne, G.J. Effect of an adjustable mandibular advancement appliance on sleep bruxism: A crossover sleep laboratory study. Int. J. Prosthodont. 2009, 22, 251–259. [Google Scholar]
- Sjöholm, T.; Lowe, A.; Miyamoto, K.; Fleetham, J.; Ryan, C. Sleep bruxism in patients with sleep-disordered breathing. Arch. Oral Biol. 2000, 45, 889–896. [Google Scholar] [CrossRef]
- Saito, M.; Yamaguchi, T.; Mikami, S.; Watanabe, K.; Gotouda, A.; Okada, K.; Hishikawa, R.; Shibuya, E.; Lavigne, G. Temporal association between sleep apnea-hypopnea and sleep bruxism events. J. Sleep Res. 2013. [Google Scholar] [CrossRef] [PubMed]
- Jokubauskas, L.; Baltrušaitytė, A. Relationship between obstructive sleep apnoea syndrome and sleep bruxism: A systematic review. J. Oral Rehabil. 2017, 44, 144–153. [Google Scholar] [CrossRef] [PubMed]
- Martynowicz, H.; Gać, P.; Brzecka, A.; Poręba, R.; Wojakowska, A.; Mazur, G.; Smardz, J.; Wieckiewicz, M. The Relationship between Sleep Bruxism and Obstructive Sleep Apnea Based on Polysomnographic Findings. J. Clin. Med. 2019, 8, 1653. [Google Scholar] [CrossRef] [PubMed]
- Tan, M.W.Y.; Yap, A.U.-J.; Chua, A.P.; Wong, J.C.M.; Parot, M.V.J.; Tan, K.B.C. Prevalence of Sleep Bruxism and Its Association with Obstructive Sleep Apnea in Adult Patients: A Retrospective Polysomnographic Investigation. J. Oral Facial Pain Headache 2019, 33, 269–277. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.J.D.C.; Cunha, T.C.A.; Monteiro, M.C.M.; Serra-Negra, J.M.; Cabral, L.C.; Júnior, P.C.S. Is there an association between sleep bruxism and obstructive sleep apnea syndrome? A systematic review. Sleep Breath. 2019, 24, 913–921. [Google Scholar] [CrossRef]
- Toraldo, D.; Passali, D.; Sanna, A.; De Nuccio, F.; Conte, L.; De Benedetto, M. Cost-effectiveness strategies in OSAS management: A short review. Acta Otorhinolaryngol. Ital. 2017, 37, 447–453. [Google Scholar]
- Walters, A.S.; Lavigne, G.; Hening, W.; Picchietti, D.L.; Allen, R.P.; Chokroverty, S.; Kushida, C.A.; Bliwise, D.L.; Mahowald, M.W.; Schenck, C.H.; et al. The Scoring of Movements in Sleep. J. Clin. Sleep Med. 2007, 3, 155–167. [Google Scholar] [CrossRef]
- Iber, C. American Academy of Sleep Medicine. The AASM Manual for the Scoring of Sleep and Associated Events: Rules, Terminology and Technical Specifications; American Academy of Sleep Medicine: Westchester, IL, USA, 2007; p. 59. [Google Scholar]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for Scoring Respiratory Events in Sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef]
- Lavigne, G.; Rompre, P.; Montplaisir, J. Sleep Bruxism: Validity of Clinical Research Diagnostic Criteria in a Controlled Polysomnographic Study. J. Dent. Res. 1996, 75, 546–552. [Google Scholar] [CrossRef]
- Manfredini, D.; Guarda-Nardini, L.; Marchese-Ragona, R.; Lobbezoo, F. Theories on possible temporal relationships between sleep bruxism and obstructive sleep apnea events. An expert opinion. Sleep Breath. 2015, 19, 1459–1465. [Google Scholar] [CrossRef] [PubMed]
- Miyawaki, S.; Lavigne, G.J.; Pierre, M.; Guitard, F.; Montplaisir, J.Y.; Kato, T. Association between sleep bruxism, swallowing-related laryngeal movement, and sleep positions. Sleep 2003, 26, 461–465. [Google Scholar] [PubMed]
- A Phillips, B.; Okeson, J.; Paesani, D.; Gilmore, R. Effect of Sleep Position on Sleep Apnea and Parafunctional Activity. Chest 1986, 90, 424–429. [Google Scholar] [CrossRef] [PubMed]
- Tago, C.; Aoki, S.; Sato, S. Status of occlusal contact during sleep bruxism in patients who visited dental clinics—A study using a Bruxchecker®. CRANIO® 2017, 36, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Lavigne, G.J.; Kato, T.; Kolta, A.; Sessle, B.J. Neurobiological Mechanisms Involved in Sleep Bruxism. Crit. Rev. Oral Biol. Med. 2003, 14, 30–46. [Google Scholar] [CrossRef] [PubMed]
- Yap, A.U.; Chua, A.P. Sleep bruxism: Current knowledge and contemporary management. J. Conserv. Dent. 2016, 19, 383. [Google Scholar] [CrossRef]
- Ohayon, M.M.; Li, K.K.; Guilleminault, C. Risk factors for sleep bruxism in the general population. Chest 2001, 119, 53–61. [Google Scholar] [CrossRef]
- Manfredini, D.; Winocur, E.; Guarda-Nardini, L.; Paesani, D.; Lobbezoo, F. Epidemiology of Bruxism in Adults: A Systematic Review of the Literature. J. Orofac. Pain 2013, 27, 99–110. [Google Scholar] [CrossRef]
- Manfredini, D.; Serra-Negra, J.; Carboncini, F.; Lobbezoo, F. Current Concepts of Bruxism. Int. J. Prosthodont. 2017, 30, 437–438. [Google Scholar] [CrossRef]
- Pontes, L.D.S.; Prietsch, S.O.M. Bruxismo do sono: Estudo de base populacional em pessoas com 18 anos ou mais na cidade de Rio Grande, Rio Grande do Sul. Rev. Bras. Epidemiol. 2019, 22, e190038. [Google Scholar] [CrossRef]
- Smardz, J.; Wieckiewicz, M.; Gać, P.; Poreba, R.; Wojakowska, A.; Mazur, G.; Martynowicz, H. Influence of age and gender on sleep bruxism and snoring in non-apneic snoring patients: A polysomnographic study. J. Sleep Res. 2020, 13178. [Google Scholar] [CrossRef]
- Valipour, A. Gender-related Differences in the Obstructive Sleep Apnea Syndrome. Pneumologie 2012, 66, 584–588. [Google Scholar] [CrossRef] [PubMed]
- Fietze, I.; Laharnar, N.; Obst, A.; Ewert, R.; Felix, S.B.; Garcia, C.; Gläser, S.; Glos, M.; Schmidt, C.O.; Stubbe, B.; et al. Prevalence and association analysis of obstructive sleep apnea with gender and age differences - Results of SHIP-Trend. J. Sleep Res. 2019, 28, e12770. [Google Scholar] [CrossRef]
- Miettinen, T.; Myllymaa, K.; Hukkanen, T.; Töyräs, J.; Sipilä, K.; Myllymaa, S. Home Polysomnography Reveals a First-Night Effect in Patients with Low Sleep Bruxism Activity. J. Clin. Sleep Med. 2018, 14, 1377–1386. [Google Scholar] [CrossRef]
- Koo, S.K.; Kwon, S.B.; Kim, Y.J.; Moon, J.S.; Kim, Y.J.; Jung, S.H. Acoustic analysis of snoring sounds recorded with a smartphone according to obstruction site in OSAS patients. Eur. Arch. Oto-Rhino-Laryngol. 2016, 274, 1735–1740. [Google Scholar] [CrossRef]
- Manfredini, D.; Ahlberg, J.; Castroflorio, T.; E Poggio, C.; Guarda-Nardini, L.; Lobbezoo, F. Diagnostic accuracy of portable instrumental devices to measure sleep bruxism: A systematic literature review of polysomnographic studies. J. Oral Rehabil. 2014, 41, 836–842. [Google Scholar] [CrossRef]
- Saczuk, K.; Lapinska, B.; Wilmont, P.; Pawlak, L.; Łukomska-Szymańska, M. The Bruxoff Device as a Screening Method for Sleep Bruxism in Dental Practice. J. Clin. Med. 2019, 8, 930. [Google Scholar] [CrossRef]
- Doering, S.; Boeckmann, J.A.; Hugger, S.; Young, P. Ambulatory polysomnography for the assessment of sleep bruxism. J. Oral Rehabil. 2008, 35, 572–576. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Demographics | With SB Episodes | Without SB Episodes | p |
|---|---|---|---|
| (n = 10) | (n = 90) | ||
| Age (years) | 43.4 (16.1) | 48.5 (13.9) | 0.29 |
| Gender (male/female) | 10/0 | 80/10 | 0.59 |
| Height (cm) | 173.8 (9.0) | 169.5 (7.7) | 0.11 |
| Weight (kg) | 82.2 (12.5) | 80.5 (19.3) | 0.34 |
| BMI (kg/m2) | 27.3 (4.3) | 27.9 (5.7) | 0.91 |
| Neck circumstance (cm) | 40.1 (3.2) | 39.6 (3.9) | 0.68 |
| Waist circumstance (cm) | 98.3 (11.0) | 99.3 (13.7) | 0.90 |
| Hip circumstance (cm) | 103.3 (8.2) | 103.3 (10.5) | 0.84 |
| Self-reported SB (−/+) | 7/3 | 77/13 | 0.20 |
| Hypertension (−/+) | 6/4 | 54/36 | 1.00 |
| Diabetes mellitus (−/+) | 9/1 | 76/14 | 1.00 |
| Index | With SB Episodes | Without SB Episodes | p |
|---|---|---|---|
| (n = 10) | (n = 90) | ||
| TST (min) | 363.2 (72.7) | 331.6 (56.0) | 0.03 |
| SE (%) | 86.2 (14.1) | 81.5 (14.7) | 0.14 |
| SL (min) | 3.5 (2.3) | 6.4 (6.5) | 0.25 |
| Stage N1 sleep (% of TST) | 24.2 (13.3) | 34.3 (16.5) | 0.06 |
| Stage N2 sleep (% of TST) | 50.0 (10.6) | 41.4 (11.5) | 0.03 |
| Stage N3 sleep (% of TST) | 9.3 (7.0) | 7.7 (7.7) | 0.33 |
| Stage REM sleep (% of TST) | 16.5 (6.7) | 16.6 (6.9) | 0.96 |
| ST in the nonsupine position (min) | 46.9 (71.5) | 104.6 (86.9) | 0.04 |
| ST in the supine position (min) | 316.4 (92.8) | 227.2 (97.0) | 0.01 |
| AI (events/h) | 6.9 (9.3) | 21.0 (26.3) | 0.13 |
| AHI (events/h) | 25.5 (16.6) | 45.1 (28.2) | 0.03 |
| AHI of NREM sleep (events/h) | 23.4 (18.1) | 44.7 (30.2) | 0.02 |
| AHI of REM sleep (events/h) | 34.6 (19.8) | 45.2 (25.4) | 0.25 |
| AHI in the nonsupine position(events/h) | 7.6 (17.2) | 23.1 (30.3) | 0.02 |
| AHI in the supine position (events/h) | 28.3 (17.8) | 56.0 (30.7) | 0.01 |
| Mean oxygen saturation (%) | 94.8 (2.0) | 91.6 (5.1) | 0.03 |
| Lowest oxygen saturation (%) | 83.8 (8.5) | 80.4 (9.6) | 0.26 |
| Mean oxygen desaturation (%) | 14.5 (8.5) | 17.6 (9.5) | 0.28 |
| Sound intensity of snoring (dB) | 59.9 (9.1) | 60.3 (14.0) | 0.69 |
| Index | Coefficient (β) | SE | t | p |
|---|---|---|---|---|
| Stage N2 sleep (% of TST) | 0.003 | 0.003 | 1.080 | 0.28 |
| ST in the supine position (min) | 0.001 | 0.001 | 2.871 | 0.01 |
| AHI (events/h) | –0.001 | 0.002 | –0.471 | 0.64 |
| Mean oxygen saturation (%) | 0.006 | 0.010 | 0.574 | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.H.; Lee, S.H.; Lee, S.H. Sleep Bruxism Episodes in Patients with Obstructive Sleep Apnea Syndrome Determined by In-Laboratory Polysomnography. Appl. Sci. 2020, 10, 8587. https://doi.org/10.3390/app10238587
Kim DH, Lee SH, Lee SH. Sleep Bruxism Episodes in Patients with Obstructive Sleep Apnea Syndrome Determined by In-Laboratory Polysomnography. Applied Sciences. 2020; 10(23):8587. https://doi.org/10.3390/app10238587
Chicago/Turabian StyleKim, Dong Hyun, Sang Hwa Lee, and Sang Haak Lee. 2020. "Sleep Bruxism Episodes in Patients with Obstructive Sleep Apnea Syndrome Determined by In-Laboratory Polysomnography" Applied Sciences 10, no. 23: 8587. https://doi.org/10.3390/app10238587
APA StyleKim, D. H., Lee, S. H., & Lee, S. H. (2020). Sleep Bruxism Episodes in Patients with Obstructive Sleep Apnea Syndrome Determined by In-Laboratory Polysomnography. Applied Sciences, 10(23), 8587. https://doi.org/10.3390/app10238587