Biomechanical Analysis of Two Types of Osseointegrated Transfemoral Prosthesis

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Evaluation of Loads
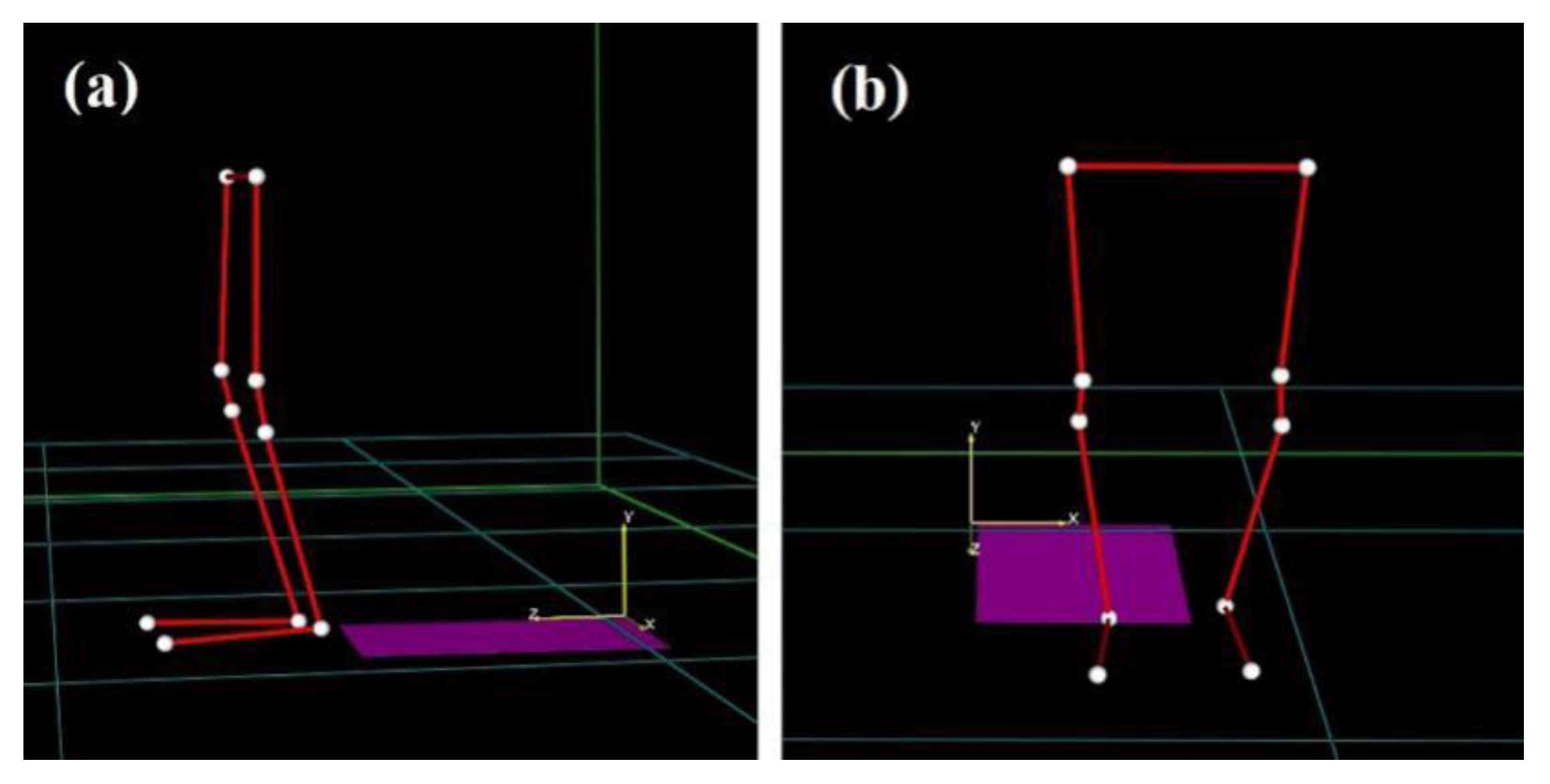
- Fall Forward (FF): during walking, the subject falls forward and impacts both knees on the ground;
- Fall Forward with Balance Loss (FF BL): during walking, the subject loses balance and falls forward with his hands on the ground and leans on the prosthetic limb by bending the hip and the knee;
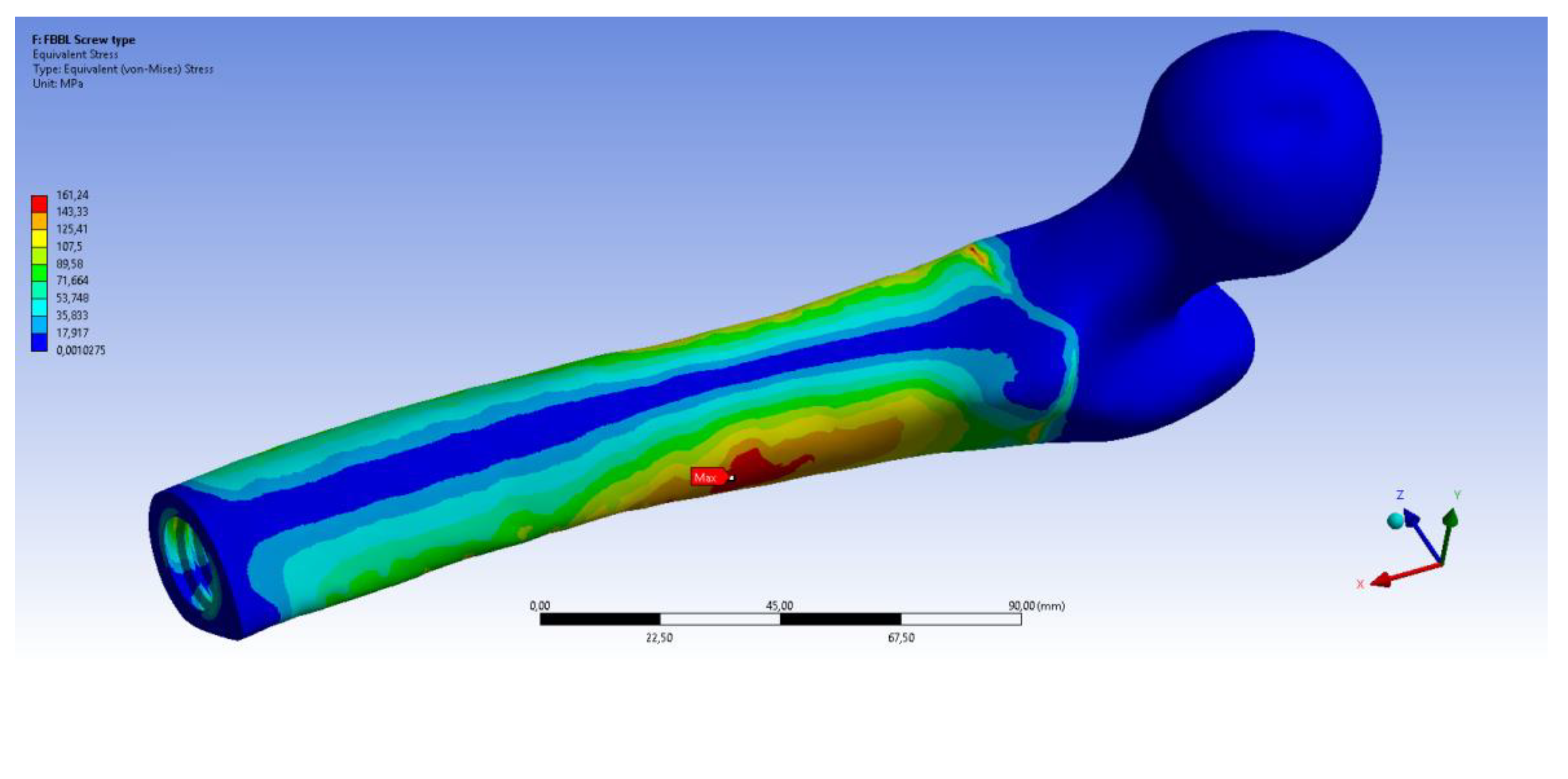
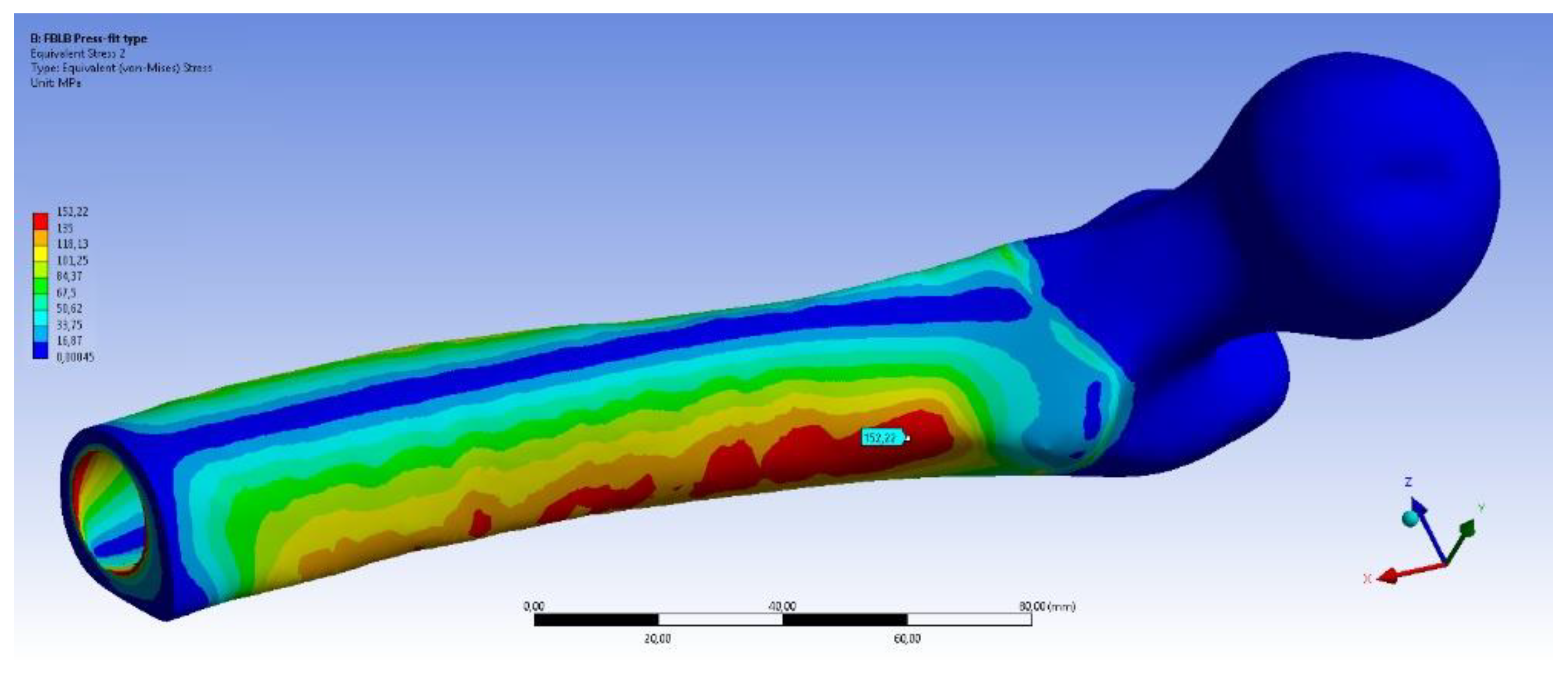
- Fall Backwards with Balance Loss (FB BL): from an orthostatic position, the subject goes back, impacts his healthy foot against an obstacle and loses balance. To restore it, the subject extends the hip and leans on his prosthetic limb;
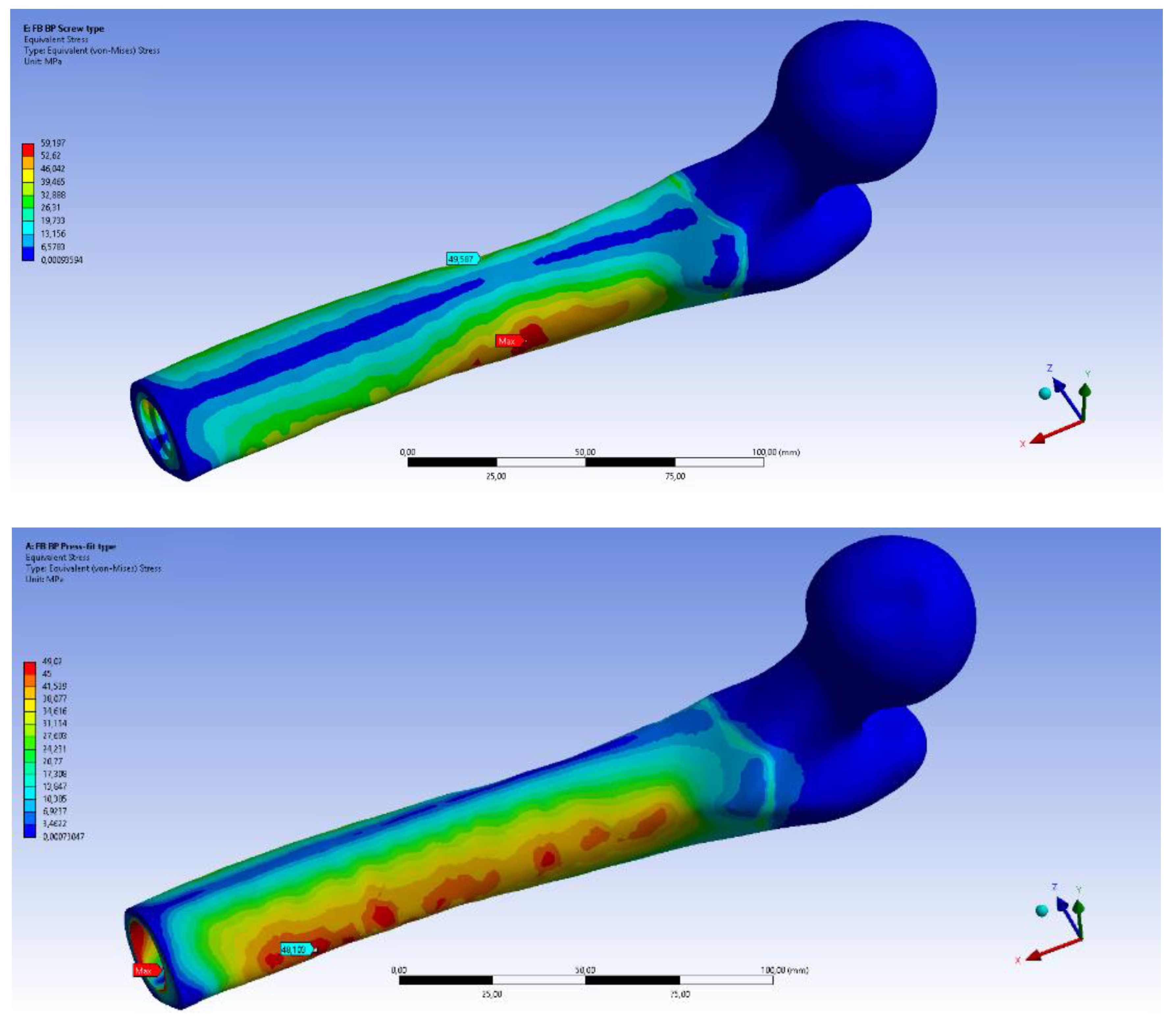
- Fall Backwards “By Push” (FB BP): from an orthostatic position, the subject experiences a sudden push along the sagittal plane. The subject loses balance, and steps back with the contralateral limb lifted and the prosthetic limb on the ground.
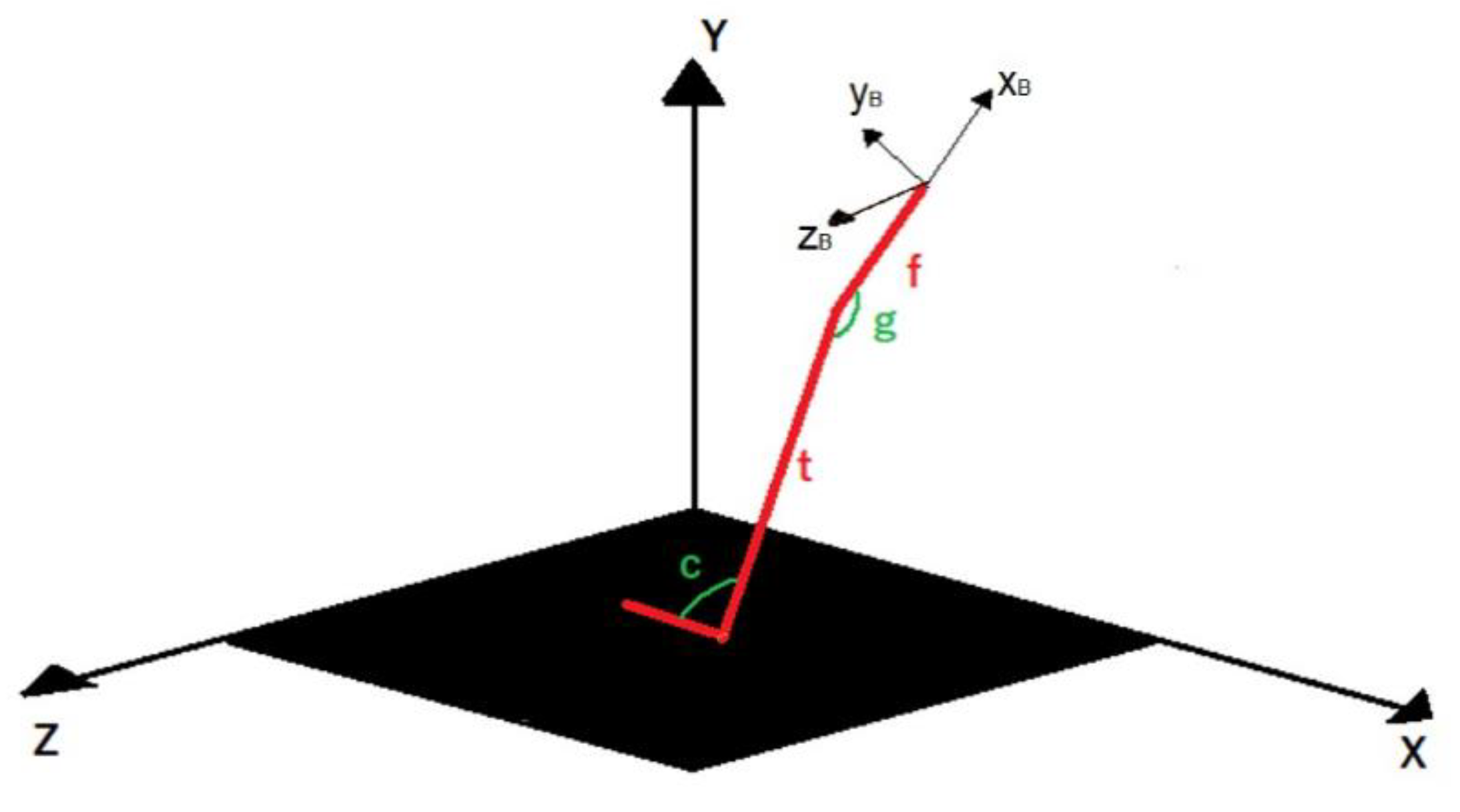
- The lower limb is schematically represented with three uniaxial and infinitely rigid elements (red in Figure 4);
- X-Y-Z is the reference system of the force plate;
- xB-yB-zB is the reference system of the bone (femur);
- t is the length of tibia;
- f is the distance between the knee and the implant position along the femur;
- c and g represent, respectively, the angle between foot and tibia and the angle between tibia and femur.
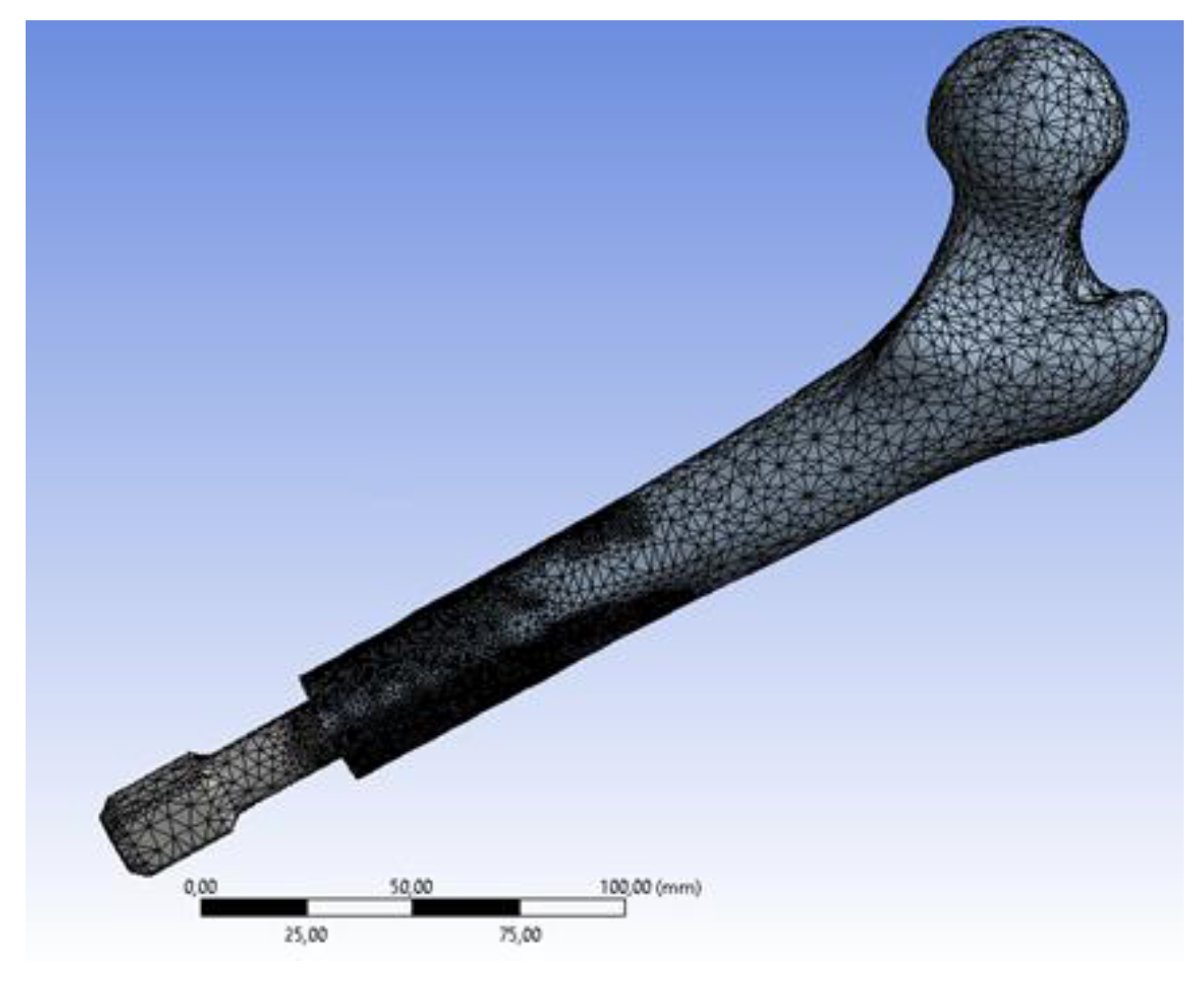
2.2. 3D CAD Modelling and FEM Model
2.3. Data Post Processing: Failure Analysis
3. Results
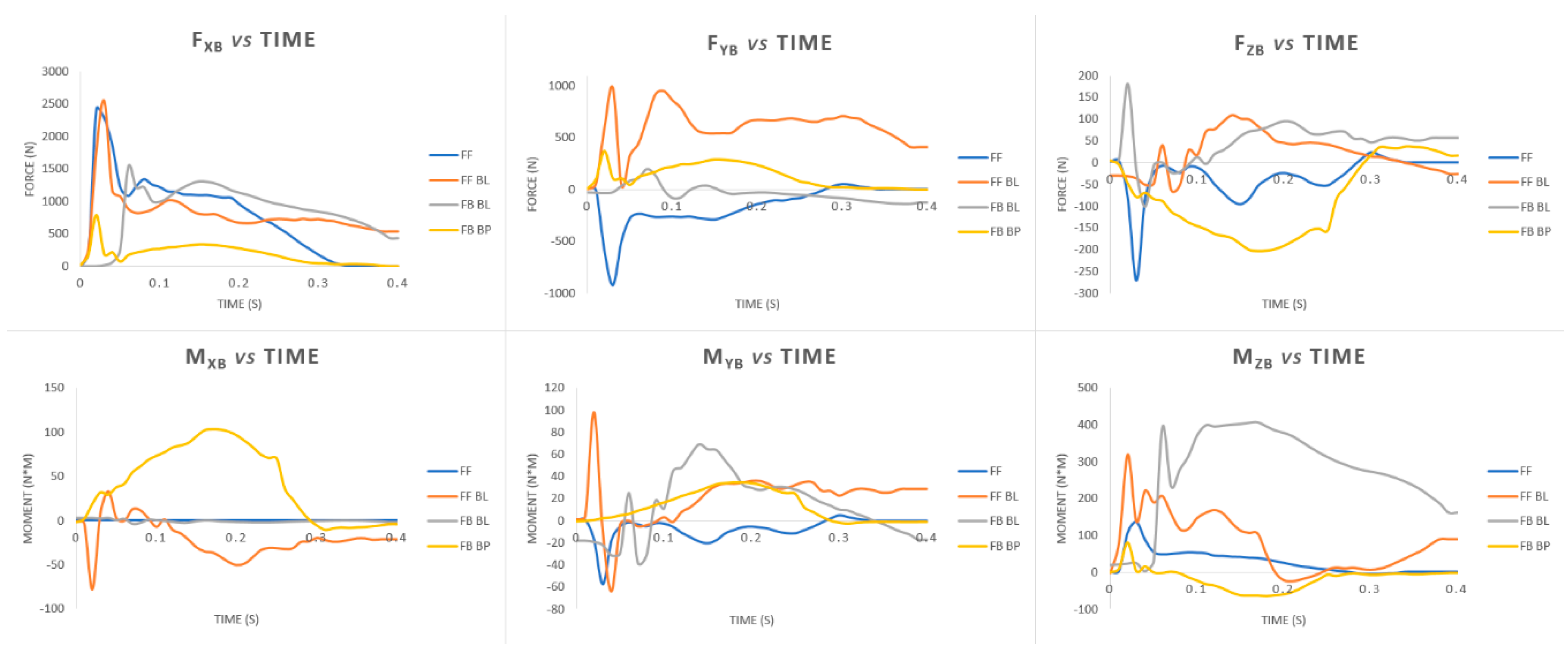
3.1. Loads during Falls
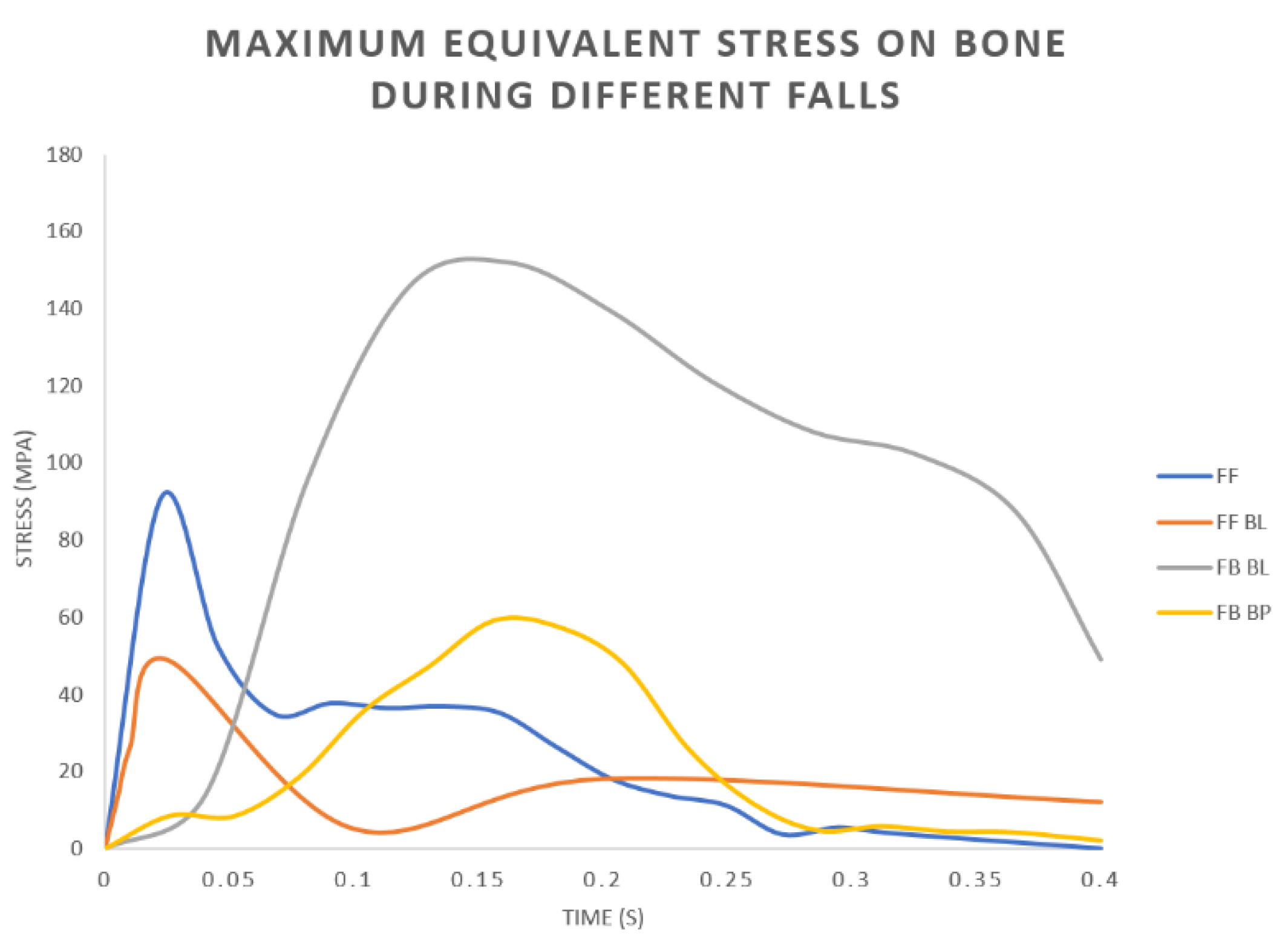
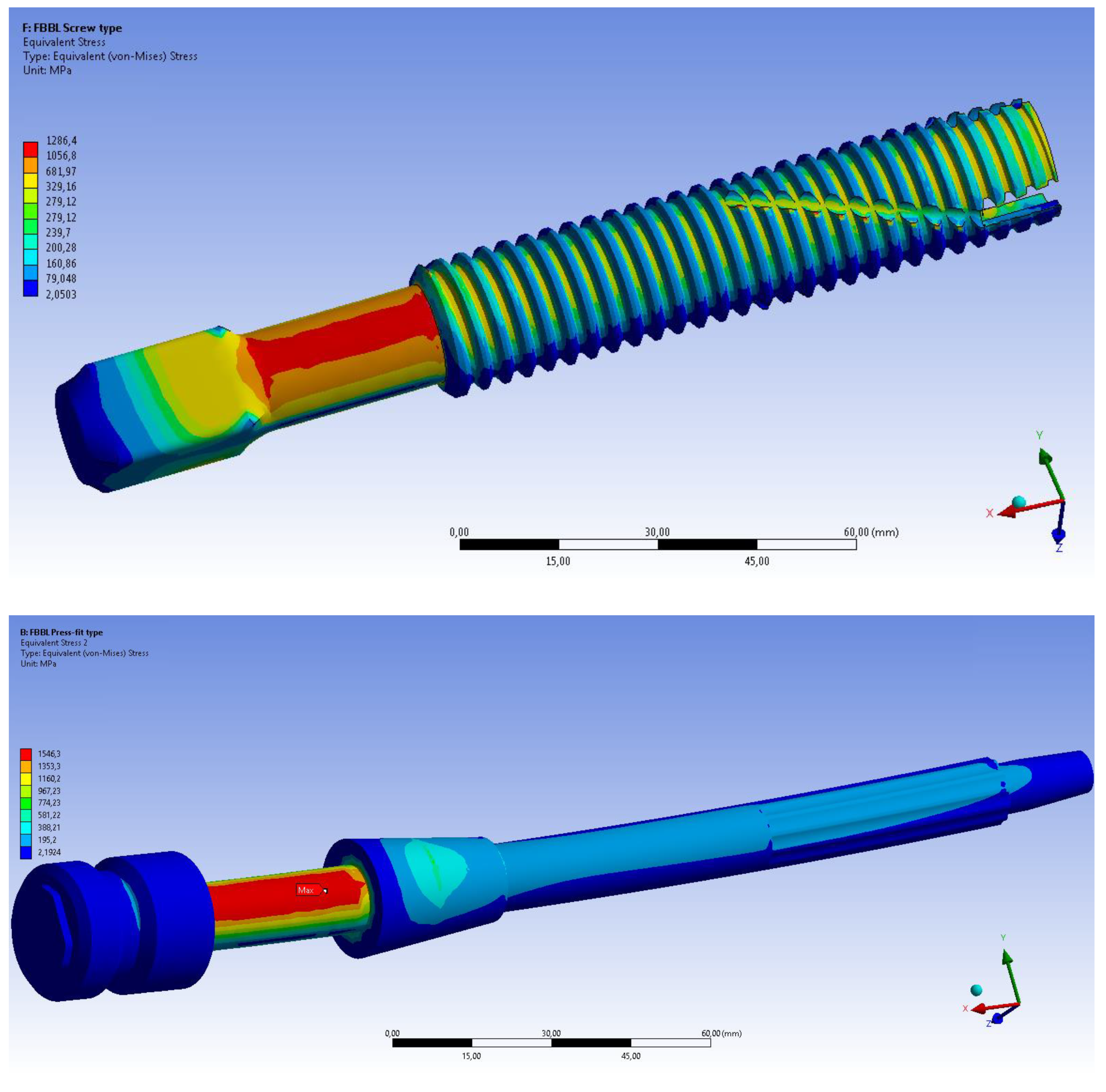
3.2. FEM Analyses
4. Discussion
- Peak values of the longitudinal force occur during falls forward;
- Very high values of the anteroposterior flexion moment on the limb occur in the FB BL fall scenario.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thesleff, A.; Brånemark, R.; Håkansson, B.; Ortiz-Catalan, M. Biomechanical Characterisation of Bone-anchored Implant Systems for Amputation Limb Prostheses: A Systematic Review. Ann. Biomed. Eng. 2018, 46, 377–391. [Google Scholar] [CrossRef]
- Robinson, D.L.; Safai, L.; Harandi, V.J.; Graf, M.; Lizama, L.E.C.; Lee, P.; Galea, M.P.; Khan, F.; Tse, K.M.; Ackland, D.C. Load response of an osseointegrated implant used in the treatment of unilateral transfemoral amputation: An early implant loosening case study. Clin. Biomech. 2020, 73, 201–212. [Google Scholar] [CrossRef]
- Hagberg, K.; Brånemark, R. Consequences of non-vascular trans-femoral amputation: A survey of quality of life, prosthetic use and problems. Prosthet. Orthot. Int. 2001, 25, 186–194. [Google Scholar] [CrossRef]
- Tomaszewski, P.; Van Diest, M.; Bulstra, S.; Verdonschot, N.; Verkerke, G. Numerical analysis of an osseointegrated prosthesis fixation with reduced bone failure risk and periprosthetic bone loss. J. Biomech. 2012, 45, 1875–1880. [Google Scholar] [CrossRef]
- Tomaszewski, P.; Verdonschot, N.; Bulstra, S.; Rietman, J.; Verkerke, G. Simulated bone remodeling around two types of osseointegrated implants for direct fixation of upper-leg prostheses. J. Mech. Behav. Biomed. Mater. 2012, 15, 167–175. [Google Scholar] [CrossRef]
- Jönsson, S.; Caine-Winterberger, K.; Brånemark, R. Osseointegration amputation prostheses on the upper limbs: Methods, prosthetics and rehabilitation. Prosthet. Orthot. Int. 2011, 35, 190–200. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Brånemark, P.-I.; Hansson, H.-A.; Lindström, J. Osseointegrated Titanium Implants:Requirements for Ensuring a Long-Lasting, Direct Bone-to-Implant Anchorage in Man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Häggström, E.; Hagberg, K.; Rydevik, B.; Brånemark, R. Vibrotactile evaluation: Osseointegrated versus socket-suspended transfemoral prostheses. J. Rehabil. Res. Dev. 2013, 50, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Brånemark, R.; Berlin, Ö.; Hagberg, K.; Bergh, P.; Gunterberg, B.; Rydevik, B. A novel osseointegrated percutaneous prosthetic system for the treatment of patients with transfemoral amputation. Bone Jt. J. 2014, 96, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, J.; Uden, M.; Robinson, K.P.; Sooriakumaran, S.; Robinson, P.K.P. Rehabilitation of the trans femoral amputee with an osseointegrated prosthesis: The United Kingdom experience. Prosthet. Orthot. Int. 2003, 27, 114–120. [Google Scholar] [CrossRef]
- Welke, B.; Schwarze, M.; Hurschler, C.; Calliess, T.; Seehaus, F. Multi-body simulation of various falling scenarios for determining resulting loads at the prosthesis interface of transfemoral amputees with osseointegrated fixation. J. Orthop. Res. 2013, 31, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Van De Meent, H.; Hopman, M.T.; Frölke, J.P. Walking Ability and Quality of Life in Subjects With Transfemoral Amputation: A Comparison of Osseointegration With Socket Prostheses. Arch. Phys. Med. Rehabil. 2013, 94, 2174–2178. [Google Scholar] [CrossRef] [PubMed]
- Leijendekkers, R.A.; Van Hinte, G.; Frölke, J.P.; Van De Meent, H.; Der Sanden, M.W.N.-V.; Staal, J.B. Comparison of bone-anchored prostheses and socket prostheses for patients with a lower extremity amputation: A systematic review. Disabil. Rehabil. 2016, 39, 1045–1058. [Google Scholar] [CrossRef] [PubMed]
- Al Muderis, M.M.; Lu, W.Y.; Li, J.J.; Kaufman, K.R.; Orendurff, M.; Highsmith, M.J.; Lunseth, P.A.; Kahle, J.T. Clinically Relevant Outcome Measures Following Limb Osseointegration; Systematic Review of the Literature. J. Orthop. Trauma 2018, 32, e64–e75. [Google Scholar] [CrossRef]
- Shelton, T.J.; Beck, J.P.; Bloebaum, R.D.; Bachus, K.N. Percutaneous osseointegrated prostheses for amputees: Limb compensation in a 12-month ovine model. J. Biomech. 2011, 44, 2601–2606. [Google Scholar] [CrossRef]
- Leijendekkers, R.A.; Van Hinte, G.; Der Sanden, M.W.N.-V.; Staal, J.B. Gait rehabilitation for a patient with an osseointegrated prosthesis following transfemoral amputation. Physiother. Theory Pract. 2017, 33, 147–161. [Google Scholar] [CrossRef]
- Aschoff, A.H.H.; Clausen, A.; Hoffmeister, T. The Endo-Exo Femur Prosthesis—A New Concept of Bone-Guided, Prosthetic Rehabilitation Following Above-Knee Amputation. Z. Orthop. Unfallchir. 2009, 8, 610–615. [Google Scholar] [CrossRef]
- Brånemark, R.; I Brånemark, P.; Rydevik, B.; Myers, R.R. Osseointegration in skeletal reconstruction and rehabilitation: A review. J. Rehabil. Res. Dev. 2001, 38, 175–181. [Google Scholar]
- Nebergall, A.; Bragdon, C.; Antonellis, A.; Kärrholm, J.; Brånemark, R.; Malchau, H. Stable fixation of an osseointegated implant system for above-the-knee amputees: Titel RSA and radiographic evaluation of migration and bone remodeling in 55 cases. Acta Orthop. 2012, 83, 121–128. [Google Scholar] [CrossRef]
- Hagberg, K.; Brånemark, R.; Stråket, B. One hundred patients treated with osseointegrated transfemoral amputation prostheses—Rehabilitation perspective. J. Rehabil. Res. Dev. 2009, 46, 331–344. [Google Scholar] [CrossRef]
- Aschoff, H.H.; Kennon, R.E.; Keggi, J.M.; Rubin, L.E. Transcutaneous, Distal Femoral, Intramedullary Attachment for Above-the-Knee Prostheses: An Endo-Exo Device. J. Bone Jt. Surg. 2010, 92, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Al Muderis, M.; Lu, W.; Li, J.J. Osseointegrated Prosthetic Limb for the treatment of lower limb amputations: Experience and outcomes. Der Unfallchirurg 2017, 120, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Frölke, J.P.M.; Leijendekkers, R.A.; Van De Meent, H. Osseointegrated prosthesis for patients with an amputation Multidisciplinary team approach in the Netherlands. Der Unfallchirurg 2017, 120, 293–299. [Google Scholar] [CrossRef] [PubMed]
- Mirulla, A.; Bragonzoni, L.; Zaffagnini, S.; Bontempi, M.; Nigrelli, V.; Ingrassia, T. Virtual simulation of an osseointegrated trans-humeral prosthesis: A falling scenario. Injury 2018, 49, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Tomaszewski, P.K.; Verdonschot, N.; Bulstra, S.K.; Verkerke, G.J. A Comparative Finite-Element Analysis of Bone Failure and Load Transfer of Osseointegrated Prostheses Fixations. Ann. Biomed. Eng. 2010, 38, 2418–2427. [Google Scholar] [CrossRef]
- Prochor, P. Finite element analysis of stresses generated in cortical bone during implantation of a novel Limb Prosthesis Osseointegrated Fixation System. Biocybern. Biomed. Eng. 2017, 37, 255–262. [Google Scholar] [CrossRef]
- Lee, W.C.; Doocey, J.M.; Brånemark, R.; Adam, C.J.; Evans, J.H.; Pearcy, M.J.; Frossard, L.A. FE stress analysis of the interface between the bone and an osseointegrated implant for amputees—Implications to refine the rehabilitation program. Clin. Biomech. 2008, 23, 1243–1250. [Google Scholar] [CrossRef]
- Cerniglia, D.; Ingrassia, T.; D’Acquisto, L.; Saporito, M.; Tumino, D. Contact between the components of a knee prosthesis: Numerical and experimental study. Frattura ed Integrità Strutturale 2012, 6, 56–68. [Google Scholar] [CrossRef]
- Chen, F.; Huang, X.; Ya, Y.; Ma, F.; Qian, Z.; Shi, J.; Guo, S.; Yu, B. Finite element analysis of intramedullary nailing and double locking plate for treating extra-articular proximal tibial fractures. J. Orthop. Surg. Res. 2018, 13, 12. [Google Scholar] [CrossRef]
- Ingrassia, T.; Nigrelli, V.; Pecorella, D.; Bragonzoni, L.; Ricotta, V. Influence of the Screw Positioning on the Stability of Locking Plate for Proximal Tibial Fractures: A Numerical Approach. Appl. Sci. 2020, 10, 4941. [Google Scholar] [CrossRef]
- Anderson, D.D.; Thomas, T.P.; Marin, A.C.; Elkins, J.M.; Lack, W.D.; Lacroix, D. Computational techniques for the assessment of fracture repair. Injury 2014, 45, S23–S31. [Google Scholar] [CrossRef] [PubMed]
- Tumino, D.; Ingrassia, T.; Nigrelli, V.; Pitarresi, G.; Miano, V.U. Mechanical behavior of a sandwich with corrugated GRP core: Numerical modeling and experimental validation. Frattura ed Integrità Strutturale 2014, 8, 317–326. [Google Scholar] [CrossRef]
- Dickinson, A.S.; Steer, J.W.; Worsley, P.R. Finite element analysis of the amputated lower limb: A systematic review and recommendations. Med. Eng. Phys. 2017, 43, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Helgason, B.; Pálsson, H.; Rúnarsson, T.P.; Frossard, L.; Viceconti, M. Risk of failure during gait for direct skeletal attachment of a femoral prosthesis: A finite element study. Med. Eng. Phys. 2009, 31, 595–600. [Google Scholar] [CrossRef]
- Newcombe, L.; Dewar, M.; Blunn, G.; Fromme, P. Effect of amputation level on the stress transferred to the femur by an artificial limb directly attached to the bone. Med. Eng. Phys. 2013, 35, 1744–1753. [Google Scholar] [CrossRef]
- Tomaszewski, P.; Lasnier, B.; Hannink, G.; Verkerke, G.J.; Verdonschot, N. Experimental assessment of a new direct fixation implant for artificial limbs. J. Mech. Behav. Biomed. Mater. 2013, 21, 77–85. [Google Scholar] [CrossRef]
- Xu, W.; Crocombe, A.D.; Hughes, S.C. Finite element analysis of bone stress and strain around a distal osseointegrated implant for prosthetic limb attachment. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2000, 214, 595–602. [Google Scholar] [CrossRef]
- Xu, W.; Xu, D.H.; Crocombe, A.D. Three-dimensional finite element stress and strain analysis of a transfemoral osseointegration implant. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2006, 220, 661–670. [Google Scholar] [CrossRef]
- Zheng, L.; Luo, J.; Yang, B.C.; Chen, J.Y.; Zhang, X.D. 3D Finite Element Analysis of Bone Stress around Distally Osteointegrated Implant for Artificial Limb Attachment. Key Eng. Mater. 2005, 288, 653–656. [Google Scholar] [CrossRef]
- Blumentritt, S.; Schmalz, T.; Jarasch, R. The Safety of C-Leg: Biomechanical Tests. JPO J. Prosthet. Orthot. 2009, 21, 2–15. [Google Scholar] [CrossRef]
- Ingrassia, T.; Nalbone, L.; Nigrelli, V.; Pisciotta, D.; Ricotta, V. Influence of the metaphysis positioning in a new reverse shoulder prosthesis. Lect. Notes Mech. Eng. 2017, 469–478. [Google Scholar]
- Chen, P.; Lü, H.; Shen, H.; Wang, W.; Ni, B.; Chen, J. Newly designed anterolateral and posterolateral locking anatomic plates for lateral tibial plateau fractures: A finite element study. J. Orthop. Surg. Res. 2017, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- Ingrassia, T.; Nigrelli, V.; Ricotta, V.; Nalbone, L.; D’Arienzo, A.; Porcellini, G.; D’Arienzo, M. A new method to evaluate the influence of the glenosphere positioning on stability and range of motion of a reverse shoulder prosthesis. Injury 2019, 50, S12–S17. [Google Scholar] [CrossRef] [PubMed]
- Ingrassia, T.; Nalbone, L.; Nigrelli, V.; Ricotta, V.; Pisciotta, D. Biomechanical analysis of the humeral tray positioning in reverse shoulder arthroplasty design. Int. J. Interact. Des. Manuf. 2018, 12, 651–661. [Google Scholar] [CrossRef]
- Inzana, J.A.; Varga, P.; Windolf, M. Implicit modeling of screw threads for efficient finite element analysis of complex bone-implant systems. J. Biomech. 2016, 49, 1836–1844. [Google Scholar] [CrossRef] [PubMed]
- Cirello, A.; Cucinotta, F.; Ingrassia, T.; Nigrelli, V.; Sfravara, F. Fluid–structure interaction of downwind sails: A new computational method. J. Mar. Sci. Technol. 2019, 24, 86–97. [Google Scholar] [CrossRef]
- Jacquet, C.; Marret, A.; Myon, R.; Ehlinger, M.; Bahlouli, N.; Wilson, A.; Kley, K.; Rossi, J.-M.; Parratte, S.; Ollivier, M. Adding a protective screw improves hinge’s axial and torsional stability in High Tibial Osteotomy. Clin. Biomech. 2020, 74, 96–102. [Google Scholar] [CrossRef]
- Ji, W.; Luo, C.F.; Zhan, S.; Zhan, Y.; Xie, X.; Zhang, B. Combined proximal tibial osteotomy for varus osteoarthritis of the knee: Biomechanical tests and finite-element analyses. Knee 2020, 27, 863–870. [Google Scholar] [CrossRef]
- Perez, A.; Mahar, A.; Negus, C.; Newton, P.; Impelluso, T. A computational evaluation of the effect of intramedullary nail material properties on the stabilization of simulated femoral shaft fractures. Med. Eng. Phys. 2008, 30, 755–760. [Google Scholar] [CrossRef]
- Ingrassia, T.; Lombardo, B.; Nigrelli, V.; Ricotta, V.; Nalbone, L.; D’Arienzo, A.; D’Arienzo, M.; Porcellini, G. Influence of sutures configuration on the strength of tendon-patch joints for rotator cuff tears treatment. Injury 2019, 50, S18–S23. [Google Scholar] [CrossRef]
- Keyak, J.; Falkinstein, Y. Comparison of in situ and in vitro CT scan-based finite element model predictions of proximal femoral fracture load. Med. Eng. Phys. 2003, 25, 781–787. [Google Scholar] [CrossRef]
- Anwar, A.; Lv, D.; Zhao, Z.; Zhang, Z.; Lu, M.; Nazir, M.U.; Qasim, W. Finite element analysis of the three different posterior malleolus fixation strategies in relation to different fracture sizes. Injury 2017, 48, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-N.; Chang, C.-W.; Li, C.-T.; Chen, C.-H.; Chung, C.-R.; Peng, Y.-T. Biomechanical investigation of the type and configuration of screws used in high tibial osteotomy with titanium locking plate and screw fixation. J. Orthop. Surg. Res. 2019, 14, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Simo, J.; Laursen, T. An augmented lagrangian treatment of contact problems involving friction. Comput. Struct. 1992, 42, 97–116. [Google Scholar] [CrossRef]
- Hoffman, O. The Brittle Strength of Orthotropic Materials. J. Compos. Mater. 1967, 1, 200–206. [Google Scholar] [CrossRef]
- Van Rietbergen, B.B.; Huiskes, H.R. Load transfer and stress shielding of the hydroxyapatite-ABG hip: A study of stem length and proximal fixation. J. Arthroplast. 2001, 16 (Suppl. 1), 55–63. [Google Scholar] [CrossRef]
- Schwarze, M.; Hurschler, C.; Seehaus, F.; Correa, T.A.; Welke, B. Influence of transfemoral amputation length on resulting loads at the osseointegrated prosthesis fixation during walking and falling. Clin. Biomech. 2014, 29, 272–276. [Google Scholar] [CrossRef]
- Stenlund, P.; Trobos, M.; Lausmaa, J.; Brånemark, R.; Thomsen, P.; Palmquist, A. Effect of load on the bone around bone-anchored amputation prostheses. J. Orthop. Res. 2017, 35, 1113–1122. [Google Scholar] [CrossRef]
- Tsikandylakis, G.; Berlin, Ö.; Brånemark, R. Implant Survival, Adverse Events, and Bone Remodeling of Osseointegrated Percutaneous Implants for Transhumeral Amputees. Clin. Orthop. Relat. Res. 2014, 472, 2947–2956. [Google Scholar] [CrossRef]
- Van Eck, C.F.; McGough, R.L. Clinical outcome of osseointegrated prostheses for lower extremity amputations: A systematic review of the literature. Curr. Orthop. Pract. 2015, 26, 349–357. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| E1 (GPa) | E2 (GPa) | E3 (GPa) | G12 (GPa) | G13 (GPa) | G23 (GPa) | n12 | n13 | n23 |
|---|---|---|---|---|---|---|---|---|
| 6.91 | 8.51 | 18.4 | 2.41 | 3.56 | 4.91 | 0.49 | 0.12 | 0.14 |
| Material | E (GPa) | n | σy (MPa) |
|---|---|---|---|
| Ti6Al4V | 115 | 0.33 | 890 |
| Femur | Implant | |||
|---|---|---|---|---|
| Screw-Type | Press Fit | Screw-Type | Press Fit | |
| FF | 93 | 91 | 607 | 723 |
| FF BL | 59 | 49 | 913 | 855 |
| FB BL | 161 | 152 | 1286 | 1546 |
| FB BP | 63 | 59 | 602 | 557 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mirulla, A.I.; Di Paolo, S.; Di Simone, F.; Ingrassia, T.; Nigrelli, V.; Zaffagnini, S.; Bragonzoni, L. Biomechanical Analysis of Two Types of Osseointegrated Transfemoral Prosthesis. Appl. Sci. 2020, 10, 8263. https://doi.org/10.3390/app10228263
Mirulla AI, Di Paolo S, Di Simone F, Ingrassia T, Nigrelli V, Zaffagnini S, Bragonzoni L. Biomechanical Analysis of Two Types of Osseointegrated Transfemoral Prosthesis. Applied Sciences. 2020; 10(22):8263. https://doi.org/10.3390/app10228263
Chicago/Turabian StyleMirulla, Agostino Igor, Stefano Di Paolo, Francesco Di Simone, Tommaso Ingrassia, Vincenzo Nigrelli, Stefano Zaffagnini, and Laura Bragonzoni. 2020. "Biomechanical Analysis of Two Types of Osseointegrated Transfemoral Prosthesis" Applied Sciences 10, no. 22: 8263. https://doi.org/10.3390/app10228263
APA StyleMirulla, A. I., Di Paolo, S., Di Simone, F., Ingrassia, T., Nigrelli, V., Zaffagnini, S., & Bragonzoni, L. (2020). Biomechanical Analysis of Two Types of Osseointegrated Transfemoral Prosthesis. Applied Sciences, 10(22), 8263. https://doi.org/10.3390/app10228263