1. Introduction
The determination and the maintenance of a correct working length (WL) are the most important factors for the success of root canal treatment [
1]. WL is defined as the distance from a coronal reference to the point at which canal preparation and obturation should terminate [
2]. A major concern in the prevention of technical errors and endodontic failures is the maintenance of appropriate WL throughout clinical practice [
3].
Electronic apex locators are precise and reliable in more than 90% of cases [
4,
5]. They are ergonomically advantageous, as they allow the WL to be checked several times during the clinical procedures without increasing the overall treatment time [
6]. WL should be checked three times during treatment: first after the initial canal scouting with manual K-files (KF), then after glide path and immediately after root canal coronal enlargement, because WL changes are expected due to straightening of the canal curvatures (CC) [
7,
8,
9]. Therefore, WL transfer between the KF and the subsequent mechanical shaping instruments should be extremely precise in order to equally prevent over- and under-instrumentation. Over-instrumentation with nickel–titanium (NiTi) rotary or reciprocating files of augmented taper may have clinical implications, including apical transportation [
10] and overfilling [
11] with defective apical seal control, especially in curved canals, and greater incidence of post-operative pain [
12,
13]. On the other hand, under-instrumentation may predispose the creation of blocks and ledges, which can negatively influence the long-term prognosis of the endodontic treatment, leaving a residual bacterial load inside the root canal [
3]. Therefore, during the clinical practice, WL is usually checked electronically and radiographically with a manual K-File (KF) and determined by the position of a rubber stop at the coronal reference point. Afterwards, the WL is measured with a manual endodontic gauge and transferred to the NiTi mechanical instrument selected for shaping [
5,
6]. A careful WL transfer procedure is required to ensure measurement reliability [
14], but this clinical procedure may be prone to errors. The objective of this study was to evaluate the accuracy of two different clinical methods of transferring WL between endodontic instruments. This aspect could be crucial for the optimization of clinical practice and for improvements in treatment outcomes. The null hypothesis is that both methods are comparable in transferring WL measurements.
2. Materials and Methods
Thirty root canals of extracted permanent teeth with fully formed apex (first and second upper molar buccal canals, and first and second lower molar mesial canals) that had not undergone prior endodontic treatment were selected. The patients signed an informed consent for the treatment and for the use of the extracted tooth for research purposes and the Local Scientific Committee authorized the in vitro study. A sample size of 15 per group was calculated with G*Power 3.1.4 (Kiel University, Kiel, Germany) with alpha error = 0.05 and ß = 0.95. After debriding the root surface, specimens were immersed in a 0.01% NaOCl solution for 1 h and then stored in saline solution until preparation. Pre-operative X-rays were taken (Planmeca Intra—Helsinki, Finland) using photostimulable phosphor imaging plates and were processed and archived by a dedicated scanner and software interface (OpTime Soredex, Helsinki, Finland). Root canals were divided according to canal curvature factor (CC) into moderate (10°–25°) and severe (>25°) groups.
After access cavity preparation, the appropriate reference cusp and the root terminus were flattened using 3.5× Galilean loupes with a grinding/polishing wheel to provide reproducible and accurate measurements. A flat glass surface was placed in contact with the flattened root end and the WL was established by an expert endodontist under microscopic vision (OPMI Pro Ergo, Carl Zeiss, Oberkochen, Germany) at 10× magnification when the tip of a #10 k-file was visible at the root tip that was in contact with the glass surface. WL was obtained with K-files (KF) and the silicone stop position was fixed with cyanoacrylate cement. Root canals were divided according to canal length factor (CL) into short (15.56–17.88 mm), medium (17.89–19.29 mm) and long (19.48–20.45 mm) groups. Afterwards, WL was transferred to the NiTi reciprocating files (WaveOne Primary, W1) using both clinical methods.
In method I, WL was checked with a traditional endodontic millimetric gauge with a bar for each millimeter; the reference K-file was measured using a graduated ruler (Endo M Block, Densply Sirona, York, PA, USA) and then a W1 instrument was set to the same length with the same gauge.
In method II, corresponding files were matched by placing them side by side from tip to shank in opposite directions in order to compare the length of the two instruments. The silicone stop position was adjusted until the right measure was reached (
Figure 1).
The digital images of the KF and the corresponding two W1 files, one for each method, were acquired by a digital reflex camera (Canon EOS 350D (8 Mpx resolution, ISO 100, f/18, 1/60 s)). For each instrument and method, two measures were taken by two examiners using Rhino (ver. 4.0, McNeel, Seattle, WA, USA) software for a total of 360 measures. The agreement between operators was calculated by applying the Cohen weighted kappa coefficient (SPSS v.24.0; IBM Corp, Armonk, NY, USA). The kappa results were interpreted as follows: values ≤0 indicated no agreement, 0.01–0.20 none to slight agreement, 0.21–0.40 fair agreement, 0.41–0.60 moderate agreement, 0.61–0.80 substantial agreement and 0.81–0.99 almost perfect agreement. Analysis of variance was performed by taking the difference in length (Delta WL, DWL) between files of the same canal. For each canal, seven DWL were independently performed for each method, which resulted in a total of 420 DWL measures. A balanced hierarchical ANOVA was used to evaluate the influence of the three main factors (method, CC, and CL). Other root canal properties included in CC and CL were considered by taking into account a further random factor canal (C). The significance level was set to 5% (p < 0.05). All statistical analyses were performed using the Minitab 15 software package (Minitab Inc., State College, PA, USA).
3. Results
The difference between methods I and II for transferring WL was found to be statistically significant (df = 1; F = 71.52;
p < 0.001).
Figure 2 shows that method I tended to underestimate reported WL, leading to a mean error of 0.20 mm. On the contrary, method II overestimated WL by approximately 0.09 mm. Therefore, the DWL absolute values obtained with method II were found to be closer to 0 mm (i.e., the same length as the corresponding KF) than those obtained with method I.
The parameters CL (df = 2; F = 1.27;
p = 0.300>0.05), CC (df = 1; F = 2.22;
p = 0.149 > 0.05) and the interactions involving them (method*CC (df = 1; F = 4.06;
p = 0.055 > 0.05); method*CL (df = 2; F = 2.31;
p = 0.121 > 0.05); CC*CL (df = 2; F = 0.20;
p = 0.823>0.05); and method*CC*CL (df = 2; F = 0.75;
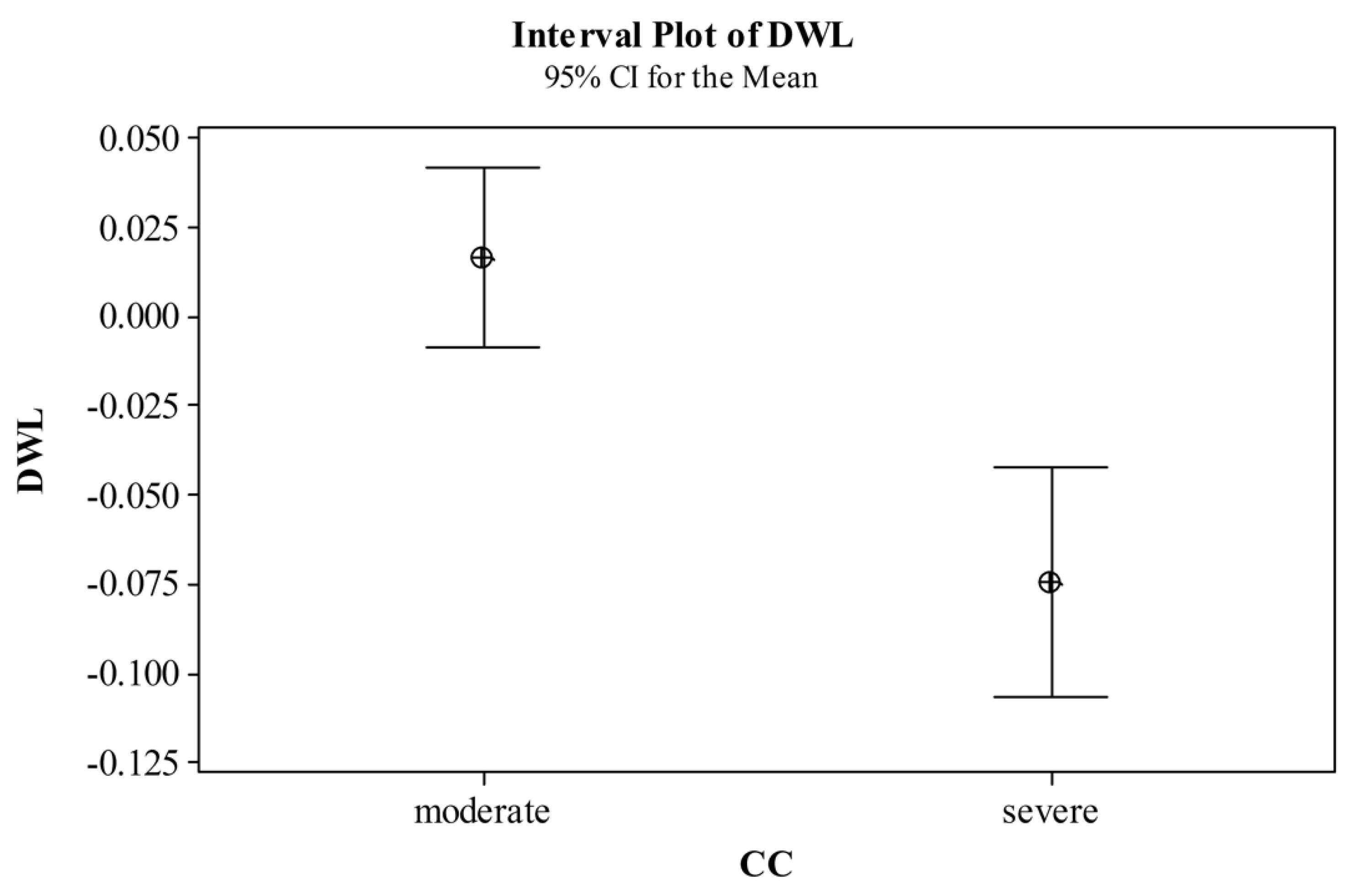
p = 0.482 > 0.05)) did not significantly influence the WL measurement. However, as shown in
Figure 3, moderate CC generally led to smaller DWL absolute values, while severe CC led to larger negative DWL (i.e., W1 length was smaller than the corresponding KF length). It is worth noting that the random factor C was found to significantly influence the DWL response (df = 24; F = 5.16;
p < 0.001), as expected. The overall kappa coefficient was 0.88 (asymptotic standard error of 0.03), corresponding to an almost perfect agreement between observations.
4. Discussion
Based on the results from the present study, the WL transfer that matches the instruments side by side from tip to shank in opposite directions may be more accurate than the use of a manual endodontic gauge during endodontic clinical practice.
The correct WL should be preserved in order to avoid inner or outer apical transportation, particularly when shaping instruments of augmented taper are used [
15,
16]. Over-instrumentation may cause an irregular foramen widening, a lack of sealing with a high rate of debris extrusion and post-operative discomfort [
17,
18]. Alternatively, under-instrumentation can create ledges, blocks and other canal aberrations that may lead to inadequate shaping and filling, negatively affecting the disinfection and the long-term prognosis of the root canal treatment [
1,
3,
15,
19]. Therefore, over- and under-instrumentation should be both equally reduced in order to achieve antimicrobial and sealing efficiency [
10,
11,
12,
13].
However, the canal anatomy and the coronal flaring may influence WL variations during shaping, especially in the mesial root of the mandibular molars and in the mesio-buccal root of the maxillary molars [
20,
21]. In those roots, where the original anatomy is particularly complex, the preliminary flaring of the canal coronal portion is suggested in order to facilitate WL achievement [
22,
23,
24]. Nevertheless, the electronic apex locator’s accuracy is improved by canal flaring [
25,
26,
27]. However, it can lead to a variation in the initial WL, which is independent from the root canal preparation technique [
28,
29,
30,
31]. The present findings reported that severe canal curvatures (CC factor) may lead to larger negative DWL, confirming the influence of canal anatomy on WL transfers, as discussed in a previous study [
31]. Therefore, the WL measure transfer is constantly repeated during clinical practice and a possible error may dramatically influence the quality of the endodontic treatment [
31].
The precise transfer of a correct WL from the manual KF to the subsequent shaping instruments is mandatory for an adequate shaping and filling of the root canal system. However, it could be challenging even for an expert operator using magnification devices. No previous studies have reported the precision of different WL transfer clinical methods between endodontic instruments.
Clinically, most operators use a manual endodontic gauge to report the WL measurement from the KF to the following shaping instruments, but this method can lead to a mean error of 0.20 mm, even with the use of a proper optical magnification. On the contrary, the matching of the instruments side by side to compare the WL (method II) may decrease this discrepancy to a negligible value of 0.09 mm, which is reasonably too low to influence the clinical outcomes. Instrument matching is intended as a visual appraisal of the position of the silicone stops for both instruments. Therefore, the two instruments are placed side by side in order to compare the position of the silicone stops until they are perfectly congruent and to prevent the shift in the silicone stop using the tips of the files. This way, it is possible to prevent any risk of puncture wounds, addressing safety concerns for the clinician. However, with respect to the maximum precision in WL maintenance, it is important to consider the necessity to maintain the silicone stop perpendicular to the instruments’ axis and prevent touching of the coronal reference point during shaping.
Reducing the errors in WL transfer during clinical practice may be significant for the improvement of the endodontic long-term prognosis [
32,
33,
34]. Both over- and under-instrumentation are equally detrimental for treatment success and, therefore, they should be evenly prevented [
16,
17].
5. Conclusions
Within the limits of this study, endodontic WL transfer matching of the instruments side by side may help to reduce clinical discrepancies, subsequently better preserving the correct WL during shaping. Further studies should be encouraged to confirm these preliminary results.
Author Contributions
Conceptualization, M.A. and E.B.; data curation, M.A., M.D., D.S.P., G.C. and E.B.; formal analysis, G.C., M.C.D.; methodology, M.A., D.S.P. and G.C., M.C.D.; project administration, E.B.; software, M.C., D.S.P. and G.C.; supervision, E.B.; visualization, M.A., M.D., M.C., M.C.D. and G.T.; writing—original draft, M.A., M.D., M.C. and G.T.; writing—review and editing, M.D., M.C., M.C.D. and G.T. All authors have read and agreed to the published version of the manuscript.
Funding
No funds were received for the development of this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- De Chevigny, C.; Dao, T.T.; Basrani, B.R.; Marquis, V.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment outcome in endodontics: The Toronto study—Phase 4: Initial treatment. J. Endod. 2008, 34, 258–263. [Google Scholar] [CrossRef]
- Vieyra, J.P.; Acosta, J. Comparison of working length determination with radiographs and four electronic apex locators. Int. Endod. J. 2011, 44, 510–518. [Google Scholar] [CrossRef]
- Peters, O.A. Current challenges and concepts in the preparation of root canal systems: A review. J. Endod. 2004, 30, 559–567. [Google Scholar] [CrossRef]
- Gordon, M.P.; Chandler, N.P. Electronic apex locators. Int. Endod. J. 2004, 37, 425–437. [Google Scholar] [CrossRef]
- ElAyouti, A.; Weiger, R.; Lost, C. The ability of root ZX apex locator to reduce the frequency of overestimated radiographic working length. J. Endod. 2002, 28, 116–119. [Google Scholar] [CrossRef]
- ElAyouti, A.; Dima, E.; Ohmer, J.; Sperl, K.; von Ohle, C.; Lost, C. Consistency of apex locator function: A clinical study. J. Endod. 2009, 35, 179–181. [Google Scholar] [CrossRef]
- Caldwell, J.L. Change in working length following instrumentation of molar canals. Oral Surg. Oral Med. Oral Pathol. 1976, 41, 114–118. [Google Scholar] [CrossRef]
- Davis, R.D.; Marshall, J.G.; Baumgartner, J.C. Effect of early coronal flaring on working length change in curved canals using rotary nickel-titanium versus stainless steel instruments. J. Endod. 2002, 28, 438–442. [Google Scholar] [CrossRef]
- Yun, H.H.; Kim, S.K. A comparison of the shaping abilities of 4 nickel-titanium rotary instruments in simulated root canals. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 95, 228–233. [Google Scholar] [CrossRef]
- Iqbal, M.K.; Firic, S.; Tulcan, J.; Karabucak, B.; Kim, S. Comparison of apical transportation between ProFile and ProTaper NiTi rotary instruments. Int. Endod. J. 2004, 37, 359–364. [Google Scholar] [CrossRef]
- Javaheri, H.H.; Javaheri, G.H. A comparison of three Ni-Ti rotary instruments in apical transportation. J. Endod. 2007, 33, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Pak, J.G.; White, S.N. Pain prevalence and severity before, during, and after root canal treatment: A systematic review. J. Endod. 2011, 37, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, J.H.; Brizuela, C.; Villota, E. Human teeth with periapical pathosis after overinstrumentation and overfilling of the root canals: A scanning electron microscopic study. Int. Endod. J. 1999, 32, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Arias, A.; Azabal, M.; Hidalgo, J.J.; de la Macorra, J.C. Relationship between postendodontic pain, tooth diagnostic factors, and apical patency. J. Endod. 2009, 35, 189–192. [Google Scholar] [CrossRef]
- Loizides, A.L.; Kakavetsos, V.D.; Tzanetakis, G.N.; Kontakiotis, E.G.; Eliades, G. A comparative study of the effects of two nickel-titanium preparation techniques on root canal geometry assessed by microcomputed tomography. J. Endod. 2007, 33, 1455–1459. [Google Scholar] [CrossRef]
- Jafarzadeh, H.; Abbott, P.V. Ledge formation: Review of a great challenge in endodontics. J. Endod. 2007, 33, 1155–1162. [Google Scholar] [CrossRef]
- Wu, M.K.; Fan, B.; Wesselink, P.R. Leakage along apical root fillings in curved root canals. Part I: Effects of apical transportation on seal of root fillings. J. Endod. 2000, 26, 210–216. [Google Scholar] [CrossRef]
- Siqueira, J.F., Jr.; Rocas, I.N.; Favieri, A.; Machado, A.G.; Gahyva, S.M.; Oliveira, J.C.; Abad, E.C. Incidence of postoperative pain after intracanal procedures based on an antimicrobial strategy. J. Endod. 2002, 28, 457–460. [Google Scholar] [CrossRef]
- Moore, J.; Fitz-Walter, P.; Parashos, P. A micro-computed tomographic evaluation of apical root canal preparation using three instrumentation techniques. Int. Endod. J. 2009, 42, 1057–1064. [Google Scholar] [CrossRef]
- Weine, F.S.; Kelly, R.F.; Lio, P.J. The effect of preparation procedures on original canal shape and on apical foramen shape. J. Endod. 1975, 1, 255–262. [Google Scholar] [CrossRef]
- Leeb, J. Canal orifice enlargement as related to biomechanical preparation. J. Endod. 1983, 9, 463–470. [Google Scholar] [CrossRef]
- Tan, B.T.; Messer, H.H. The effect of instrument type and preflaring on apical file size determination. Int. Endod. J. 2002, 35, 752–758. [Google Scholar] [CrossRef]
- Pruett, J.P.; Clement, D.J.; Carnes, D.L., Jr. Cyclic fatigue testing of nickel-titanium endodontic instruments. J. Endod. 1997, 23, 77–85. [Google Scholar] [CrossRef]
- Sattapan, B.; Nervo, G.J.; Palamara, J.E.; Messer, H.H. Defects in rotary nickel-titanium files after clinical use. J. Endod. 2000, 26, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Ibarrola, J.L.; Chapman, B.L.; Howard, J.H.; Knowles, K.I.; Ludlow, M.O. Effect of preflaring on Root ZX apex locators. J. Endod. 1999, 25, 625–626. [Google Scholar] [CrossRef]
- Ravanshad, S.; Adl, A.; Anvar, J. Effect of working length measurement by electronic apex locator or radiography on the adequacy of final working length: A randomized clinical trial. J. Endod. 2010, 36, 1753–1756. [Google Scholar] [CrossRef]
- Williams, C.B.; Joyce, A.P.; Roberts, S. A comparison between in vivo radiographic working length determination and measurement after extraction. J. Endod. 2006, 32, 624–627. [Google Scholar] [CrossRef]
- Schroeder, K.P.; Walton, R.E.; Rivera, E.M. Straight line access and coronal flaring: Effect on canal length. J. Endod. 2002, 28, 474–476. [Google Scholar] [CrossRef]
- Peters, O.A.; Laib, A.; Gohring, T.N.; Barbakow, F. Changes in root canal geometry after preparation assessed by high-resolution computed tomography. J. Endod. 2001, 27, 1–6. [Google Scholar] [CrossRef]
- Peters, O.A.; Schonenberger, K.; Laib, A. Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. Int. Endod. J. 2001, 34, 221–230. [Google Scholar] [CrossRef]
- Berutti, E.; Chiandussi, G.; Paolino, D.S.; Scotti, N.; Cantatore, G.; Castellucci, A.; Pasqualini, D. Effect of canal length and curvature on working length alteration with WaveOne reciprocating files. J. Endod. 2011, 37, 1687–1690. [Google Scholar] [CrossRef] [PubMed]
- Robert, S.; Ilan, R. Endodontic Treatment Outcomes in a Large Patient Population in the USA: An Epidemiological Study. J. Endod. 2004, 30, 846–850. [Google Scholar] [CrossRef]
- Robert, S.; Ilan, R. Epidemiologic Evaluation of the Outcomes of Orthograde Endodontic Retreatment. J. Endod. 2010, 36, 790–792. [Google Scholar] [CrossRef]
- Marquis, V.L.; Dao, T.; Farzaneh, M.; Abitbol, S.; Friedman, S. Treatment outcome in endodontics: The Toronto Study. Phase III: Initial treatment. J. Endod. 2006, 32, 299–306. [Google Scholar] [CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 




{kind=link}
{kind=link}
{kind=link}


