
Including the Excluded in Antenatal Care: A Systematic Review of Concerns for D/deaf Pregnant Women



Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
- I.
- Studies on D/deaf pregnant women;
- II.
- Studies published between the years 2000 and 2020;
- III.
- Studies published in the English language;
- IV.
- Studies that collected data from the D/deaf on issues of antenatal care; and
- V.
- Full text articles.
- I.
- Studies published before 2000 and after 2020;
- II.
- Abstracts, editorial comments, letters to the editor, and review articles;
- III.
- Studies on postnatal care or other reproductive health issues;
- IV.
- Non-English-language articles on D/deaf pregnant women and antenatal care; and
- V.
- Studies on antenatal issues that incorporated pregnant women with other forms of disability.
2.2. Search Strategy
2.3. Selection of Studies
2.4. Data Extraction
3. Results
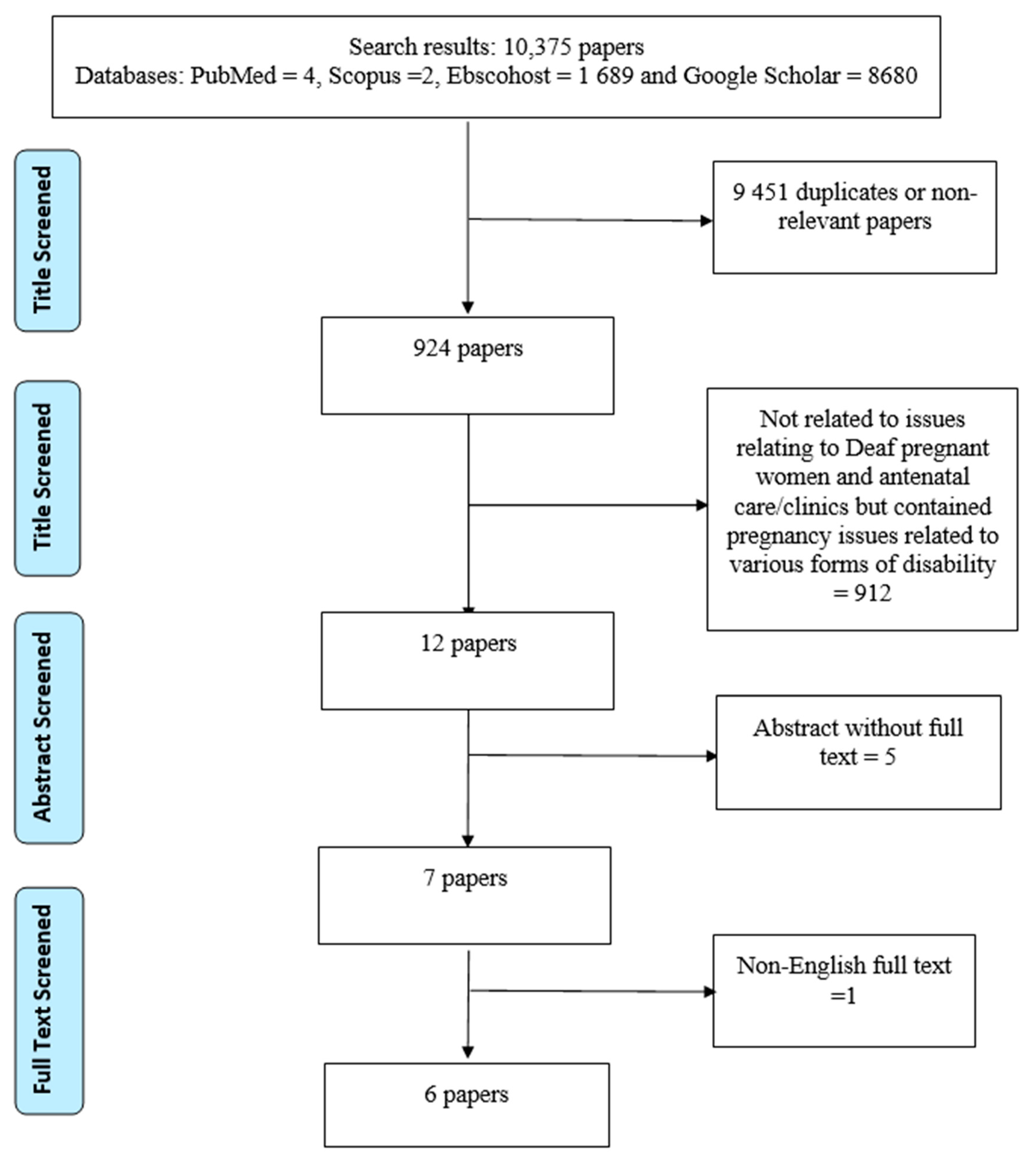
3.1. Search Outcome
3.2. Study Design
3.3. Participants
3.4. Cumulative Main Findings
4. Discussion
5. Implications and Recommendations for Research, Policy, and Practice in Health Care
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Maternal Health in Nigeria: Generating Information for Action. 2021. Available online: https://www.who.int/reproductivehealth/maternal-health-nigeria/en/ (accessed on 8 February 2021).
- UNICEF. Under Five Mortality. 2021. Available online: https://data.unicef.org/topic/child-survival/under-five-mortality/ (accessed on 8 February 2021).
- National Bureau of Statistics. Demographic Statistics Bulletin. 2018. Available online: http://nigerianstat.gov.ng/download/775 (accessed on 10 February 2021).
- Stevens, G.; Flaxman, S.; Brunskill, E.; Mascarenhas, M.; Mathers, C.D.; Finucane, M. Global and regional hearing impairment prevalence: An analysis of 42 studies in 29 countries. Eur. J. Public Health 2013, 23, 146–152. [Google Scholar] [CrossRef]
- World Health Organization. Deafness and Hearing Loss; WHO: Geneva, Switzerland, 2013; Available online: www.who.int/mediacentre/factsheets/fs300/en/ (accessed on 9 February 2021).
- Adigun, O.T.; Iheme, U.M. Mathematics Anxiety among Deaf Learners: An Analysis of Predictive Factors. Int. J. Sci. Math. Technol. Learn. 2020, 28, 1–13. [Google Scholar] [CrossRef]
- Treat, S. Deaf Education: Gallaudet University: How Deaf Education and Special Education Is Being Advanced in Nigeria. 2016. Available online: https://prezi.com/ckdvqq0rv5cx/deaf-education/ (accessed on 9 February 2021).
- Mba, P.O. Fundamentals of Special Education and Vocational Rehabilitation; Codat Publications: Ibadan, Nigeria, 1995. [Google Scholar]
- Adigun, O.T. Some psychosocial determinants of cyber-intimate image diffusion: A cross-sectional study among in-school Deaf adolescents. Pertanika J. Soc. Sci. Humanit. 2020, 28, 2601–2621. [Google Scholar] [CrossRef]
- Moroe, N.F.; de Andrade, V. ‘We were our parents’ ears and mouths’: Reflecting on the language brokering experiences of hearing children born to deaf parents. S. Afr. J. Child Health 2018, 12, 75–78. [Google Scholar] [CrossRef]
- Hogan, A. Hearing Rehabilitation for Deafened Adults: A Psychosocial Approach; Wiley-Blackwell: Oxford, UK, 2001. [Google Scholar]
- Pizzo, L. d/Deaf and Hard of Hearing Multilingual Learners: The development of communication and language. Am. Ann. Deaf 2016, 161, 17–32. [Google Scholar] [CrossRef] [PubMed]
- Woodward, J. Implications for sociolinguistics research among the Deaf. Sign Lang. Stud. 1972, 1, 1–5. [Google Scholar] [CrossRef]
- Harmer, L. Health care delivery and deaf people: Practice, problems, and recommendations for change. J. Deaf Stud. Deaf Educ. 1999, 4, 73–110. [Google Scholar] [CrossRef]
- Meador, H.E.; Zazove, P. Health care interactions with deaf culture. J. Am. Board Fam. Pract. 2005, 18, 218–222. [Google Scholar] [CrossRef]
- Ochieng, J.A.; Atieli, H.; Abongo, B.; Ouma, C. Systems of communicating sexual and reproductive health issues between hearing parents and their Deaf adolescent children in Western Kenya. Int. J. Trop. Dis. Health 2019, 37, 1–12. [Google Scholar] [CrossRef]
- Oyewumi, A.M.; Adigun, O.T. Accessibility, usage of reproductive health information and attitude towards reproductive health practices of female adolescents with hearing impairment towards reproductive health practices in Oyo and Lagos States, Nigeria. IOSR J. Humanit. Soc. Sci. 2013, 6, 1–7. [Google Scholar]
- Mills, A.A. Navigating sexual and reproductive health issues: Voices of deaf adolescents in a residential school in Ghana. Child. Youth Serv. Rev. 2020, 118, 105441. [Google Scholar] [CrossRef]
- Mprah, W.K. Sexual and reproductive health needs assessment with deaf people in Ghana: Methodological challenges and ethical concerns. Afr. J. Disabil. 2013, 2, 55. [Google Scholar] [CrossRef] [PubMed]
- Adigun, O.T.; Mngomezulu, T.P. ‘They Forget I’m Deaf’: Exploring the experience and perception of deaf pregnant women attending antenatal clinic/care in Ibadan, Nigeria. Ann. Glob. Health 2020, 86, 96. [Google Scholar] [CrossRef] [PubMed]
- Arulogun, O.S.; Titiloye, M.A.; Desmenu, A. Barriers faced by service providers in meeting the sexual and reproductive health needs of deaf persons in Ibadan metropolis: A qualitative study. J. Med. Med. Sci. 2013, 4, 433–438. [Google Scholar] [CrossRef]
- Frier, A.; Barnett, F.; Devine, S.; Barker, R. Understanding disability and the ‘social determinants of health’: How does disability affect peoples’ social determinants of health? Disabil. Rehabil. 2018, 40, 538–547. [Google Scholar] [CrossRef]
- Williamson, H.J.; Contreras, G.M.; Rodriguez, E.S.; Smith, J.M.; Perkins, E.A. Health care access for adults with intellectual and developmental disabilities: A scoping review. Occup. Particip. Health 2017, 37, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Mitra, M.; Akobirshoev, I.; McKee, M.M.; Iezzoni, L.I. Birth outcomes among US women with hearing loss. Am. J. Prev. Med. 2016, 51, 865–873. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience; World Health Organization: Geneva, Switzerland, 2016. [Google Scholar]
- Kaswa, R.; Rupesinghe, G.F.; Longo-Mbenza, B. Exploring the pregnant women’s perspective of late booking of antenatal care services at Mbekweni Health Centre in Eastern Cape, South Africa. Afr. J. Prim. Health Care Fam. Med. 2018, 10, 1–9. [Google Scholar] [CrossRef]
- Iezzoni, L.I.; Wint, A.J.; Smeltzer, S.C.; Ecker, J.L. Physical accessibility of routine prenatal care for women with mobility disability. J. Women’s Health 2015, 24, 1006–1012. [Google Scholar] [CrossRef]
- Redshaw, M.; Malouf, R.; Gao, H.; Gray, R. Women with disability: The experience of maternity care during pregnancy, labour and birth and the postnatal period. BMC Pregnancy Childbirth 2013, 13, 174. [Google Scholar] [CrossRef]
- Signore, C.C. Pregnancy in women with physical disabilities. In Queenan’s Management of High-Risk Pregnancy: An Evidence-Based Approach; John Wiley & Sons: Hoboken, NJ, USA, 2012; pp. 253–259. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Mitra, M.; McKee, M.M.; Akobirshoev, I.; Valentine, A.; Ritter, G.; Zhang, J.; McKee, K.; Iezzoni, L.I. Pregnancy, birth, and infant outcomes among women who are deaf or hard of hearing. Am. J. Prev. Med. 2020, 58, 418–426. [Google Scholar] [CrossRef] [PubMed]
- Schiff, M.A.; Doody, D.R.; Crane, D.A.; Mueller, B.A. Pregnancy outcomes among deaf women in Washington State, 1987–2012. Obstet. Gynecol. 2017, 130, 953. [Google Scholar] [CrossRef] [PubMed]
- O’Hearn, A. Deaf women’s experiences and satisfaction with prenatal care: A comparative study. Med. Care 2006, 12, 13. [Google Scholar]
- Gichane, M.W.; Heap, M.; Fontes, M.; London, L. “They must understand we are people”: Pregnancy and maternity service use among signing Deaf women in Cape Town. Disabil. Health J. 2017, 10, 434–439. [Google Scholar] [CrossRef]
- Mustafa, M.S.; Addar, M.H. Obstetric handling of a deaf patient. Saudi Med. J. 2000, 21, 1185–1188. [Google Scholar] [PubMed]
- Jackson, M. Deafness and antenatal care: Understanding issues with access. Br. J. Midwifery 2011, 19, 280–284. [Google Scholar] [CrossRef]
- Equy, V.; Derore, A.; Vassort, N.; Branchet, F.; Mongourdin, B. Evaluation of Measures to Facilitate Access to Care for Pregnant Deaf Patients: Use of Interpreters and Training of Caregivers in Sign Language. Commun. Disord. Deaf Stud. Hear. Aids 2013, 1, 103. [Google Scholar] [CrossRef]
- Allen, T.E.; Letteri, A.; Choi, S.H.; Dang, D. Early visual language exposure and emergent literacy in preschool deaf children: Findings from a national longitudinal study. Am. Ann. Deaf 2014, 159, 346–358. [Google Scholar] [CrossRef]
- Hall, M.L.; Hall, W.C.; Caselli, N.K. Deaf children need language, not (just) speech. First Lang. 2019, 39, 367–395. [Google Scholar] [CrossRef]
- Lass, G.; Franklin, R.; Bertrand, W.; Baker, J. Health knowledge, attitudes and practices of the deaf population in greater New Orleans—A pilot study. Am. Ann. Deaf 1978, 123, 960–967. [Google Scholar] [PubMed]
- Witte, T.N.; Kuzel, A.J. Elderly deaf patients’ health care experiences. J. Am. Board Fam. Pract. 2000, 13, 17–21. [Google Scholar] [CrossRef]
- Iezzoni, L.I.; O’Day, B.L.; Killeen, M.; Harker, H. Communicating about health care: Observations from persons who are deaf or hard of hearing. Ann. Intern. Med. 2004, 140, 356–362. [Google Scholar] [CrossRef]
- Steinberg, A.; Wiggins, E.; Barmada, C.; Sullivan, V. Deaf women: Experiences and perceptions of healthcare system access. J. Women’s Health 2002, 11, 729–741. [Google Scholar] [CrossRef]
- Karliner, L.S.; Jacobs, E.A.; Chen, A.H.; Mutha, S. Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health Serv. Res. 2007, 42, 727–754. [Google Scholar] [CrossRef] [PubMed]
- Rofé, Y.; Littner, M.B.; Lewin, I. Emotional experiences during the three trimesters of pregnancy. J. Clin. Psychol. 1993, 49, 3–12. [Google Scholar] [CrossRef]
- Welch, L.; Miller, L. Emotional and educational components of pregnancy. Glob. Libr. Women’s Med. 2008, 1–8. [Google Scholar] [CrossRef]
- Bjelica, A.; Kapor-Stanulović, N. Pregnancy as a psychological event. Med. Pregl. 2004, 57, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Hammarberg, K.; Fisher, J.R.W.; Wynter, K.H. Psychological and social aspects of pregnancy, childbirth and early parenting after assisted conception: A systematic review. Hum. Reprod. Update 2008, 14, 395–414. [Google Scholar] [CrossRef]


{kind=link}
| Author(s) | Year | Title of Paper | Country | Study Aim | Study Design | Participants | Main Findings |
|---|---|---|---|---|---|---|---|
| Mustafa and Addar [35] | 2000 | Obstetric handling of a deaf patient | Saudi Arabia | To examine the experiences of obstetric handling of a deaf pregnant patient antenatally, during labor, and postpartum. | A case report. | One deaf woman. | Uneventful antenatal visits. |
| Communication with patient through pen and paper could be difficult and time-consuming, and required a lot of patience. | |||||||
| The clinical, psychological, and human aspects of the management were gratifying. | |||||||
| O’Hearn [33] | 2006 | Deaf women’s experiences and satisfaction with prenatal care: a comparative study | USA | To investigate factors impacting deaf patients’ satisfaction with prenatal care and prenatal care disparities between deaf and hearing women. | Quantitative research design. | 23 deaf and 32 hearing women. | Deaf women were less satisfied than hearing women with physician communication and less satisfied with their overall care. |
| Deaf women’s expectations about the provision of interpreter services being met or exceeded were significantly associated with their overall satisfaction. | |||||||
| Hearing women had more prenatal care appointments and reported receiving more information from their doctors. | |||||||
| Schiff, Doody, Crane and Mueller [32] | 2017 | Pregnancy outcomes among deaf women in Washington State, 1987–2012 | USA | To evaluate the association between deafness among pregnant women and selected adverse pregnancy and neonatal outcomes. | A retrospective cohort study | 645 deaf women with single live births | Deaf women were more likely to have a delivery hospitalization of four or more days. |
| Deaf women had a modestly increased risk of cesarean delivery. | |||||||
| Gichane, Heap, Fontes and London [34] | 2017 | “They must understand we are people”: Pregnancy and maternity service use among signing Deaf women in Cape Town | South Africa | To describe and compare the pregnancy outcomes and maternity service use of a sample of signing Deaf women of child-bearing age in Cape Town to the population of the Western Cape of South Africa. | Mixed method design. | 42 Deaf women. | Almost all participants attended at least one antenatal appointment during their pregnancies, and all deliveries occurred at a health facility. |
| Participants primarily relied on writing to communicate during antenatal visits and labor/delivery. | |||||||
| Limited sign language interpretation services. | |||||||
| Mistreatment by hospital staff. | |||||||
| Adigun and Mngomezulu [20] | 2020 | ‘They forget I’m Deaf’: exploring the experience and perception of Deaf Pregnant women attending antenatal clinics/care | Nigeria | To explore the experiences and satisfaction of pregnant deaf women with antenatal care in Nigeria. | Qualitative research design. | Nine deaf pregnant women. | Participants registered/booked for antenatal care in their second trimester. |
| Communication difficulties during their ANC (antenatal care) visits. | |||||||
| Distance and location of the clinics, finance/cost, and health care professionals’ attitudes towards Deaf pregnant women. | |||||||
| Satisfaction with ANC services at privately owned health care facilities as compared with publicly owned health care facilities. | |||||||
| Mitra, McKee, Akobirshoev, Valentine, Ritter, Zhang, McKee, and Iezzoni [31] | 2020 | Pregnancy, birth, and infant outcomes among women who are Deaf or Hard of hearing | USA | To conduct a more rigorous study using population-based, longitudinal linked data to compare pregnancy complications, birth characteristics, and neonatal outcomes between deaf or hard of hearing and non-deaf or hard of hearing women. | A retrospective cohort study. | 1385 women who were Deaf and or Hard of hearing. | The deaf or hard of hearing women had an increased risk of chronic medical conditions and pregnancy complications. |
| Deliveries of deaf or hard of hearing women were significantly associated with adverse birth outcomes. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adigun, O.T.; Akinrinoye, O.; Obilor, H.N. Including the Excluded in Antenatal Care: A Systematic Review of Concerns for D/deaf Pregnant Women. Behav. Sci. 2021, 11, 67. https://doi.org/10.3390/bs11050067
Adigun OT, Akinrinoye O, Obilor HN. Including the Excluded in Antenatal Care: A Systematic Review of Concerns for D/deaf Pregnant Women. Behavioral Sciences. 2021; 11(5):67. https://doi.org/10.3390/bs11050067
Chicago/Turabian StyleAdigun, Olufemi Timothy, Olugbenga Akinrinoye, and Helen Ngozichukwuka Obilor. 2021. "Including the Excluded in Antenatal Care: A Systematic Review of Concerns for D/deaf Pregnant Women" Behavioral Sciences 11, no. 5: 67. https://doi.org/10.3390/bs11050067
APA StyleAdigun, O. T., Akinrinoye, O., & Obilor, H. N. (2021). Including the Excluded in Antenatal Care: A Systematic Review of Concerns for D/deaf Pregnant Women. Behavioral Sciences, 11(5), 67. https://doi.org/10.3390/bs11050067