Abstract
Behavioral therapy (BT) and exercise are efficacious treatments for depression and anxiety when employed separately. The combination of BT and exercise (BT+Ex) may augment improvements but the combined effect of these therapies is not fully elucidated. The purpose of this meta-analysis was to determine if BT+Ex yielded a significant reduction in depression and anxiety symptoms compared to BT alone (BT). Randomized controlled studies published prior to September 2019 were searched among several databases (PUBMED, MEDLINE, PsychArticle, and Cochrane Central Register of Clinical Trials). Studies that measured depression and anxiety symptoms following BT+Ex vs. BT were extracted and analyzed. The effect of these therapies on depression and anxiety were analyzed. Subgroup analyses were performed to evaluate the effect of exercise intensity (moderate and high), exercise type (aerobic and combined exercise), and baseline levels of depression. The moderating effects of gender, age, and treatment duration were performed. Data were extracted from 18 studies (1686 participants, mean age = 47 years, 65% female). There was a significant effect of BT+Ex on symptoms of depression. The effect of BT+Ex was significant for moderate intensity exercise and elevated baseline levels of depression. Age moderated the effect for depression. There was a significant effect of BT+Ex on depressive symptoms in humans. Exercise intensity and elevated depressive symptoms may play a role in the effect of exercise.
1. Introduction
The World Health Organization estimates that globally, 322 million individuals suffer from depression and 264 million individuals suffer from anxiety [1]. Depressive disorders are ranked as the single largest contributor to non-fatal health loss and are also linked to an estimated 14.3% of deaths worldwide [2]. In addition, depression and anxiety occur comorbidly with several diseases (e.g., cardiovascular, respiratory, neurological, and metabolic) [3] and increase the risk of cardiovascular disease [4,5], type 2 diabetes mellitus [6,7], and hypertension [8,9]. Further, comorbid depression and anxiety have been shown to predict poor disease outcomes [10,11].
Behavioral therapy (BT) (i.e., cognitive behavioral therapy, interpersonal therapy, counselling) is a common treatment for anxiety and depression [12,13]. Despite widespread use, not all individuals respond to this type of treatment [14,15]. Findings from a review by Hunot et al. [16] suggest that only 46% of individuals with generalized anxiety disorder (GAD) showed a positive response to BT [16]. As a result, clinicians commonly use combined therapies such as multiple forms of BT and/or medication; however, these combination therapies may not provide long-term mitigation of anxiety and depression [17].
Physical exercise has emerged as an efficacious treatment for symptoms of anxiety and depression [18,19]. While the majority of these studies have been done to compare the effectiveness of BT to exercise interventions, fewer studies have been employed to examine the combined effect of exercise and BT (BT+Ex). Researchers have hypothesized that BT+Ex may augment the effectiveness of treatment [20]. Ernst et al. [21] hypothesized that the exercise-induced upregulation of brain-derived neurotrophic factor (BDNF) promotes brain neurogenesis, resulting in a reduction of symptoms associated with depression and anxiety [21]. Physical exercise also improves cognitive functioning (e.g., processing speed, memory, learning), which would support the retention of skills learned in BT [22,23]. In addition, improved self-efficacy and mood state as a result of exercise may also improve BT treatment outcomes. Thus, the combination of exercise with BT may enhance symptom reduction through neurophysiological, cognitive, and improved self-worth mechanisms. It is important to note that the purported mechanisms that explain the benefits of exercise appear to be influenced by components of the exercise intervention, such as type of exercise (aerobic, resistance), duration of each session, and intensity.
A recent meta-analysis examined the effect of exercise combined with BT on depression and anxiety [20]. However, the research group focused on the adjunct effect of cognitive behavioral therapy (CBT) thereby excluding other forms of behavioral therapy [20]. To date, we are unaware of a previous meta-analysis that has systematically examined the adjunct effect of exercise when combined with various types of BT. Thus, the purpose of this systematic review and meta-analysis is (1) summarizing the literature on the effects of BT+Ex compared to BT alone on depression and anxiety, and (2) identifying potential moderators (exercise programming variables) that may influence the effect of adjunctive exercise. Bernard et al. [20] recently analyzed the effect of exercise combined with cognitive behavioral therapy (but not other types of BT) on various symptoms among adults with chronic illness. Several types of BT treatment are used to treat symptoms of depression and anxiety; therefore, the current aim is to provide a more thorough review of the effects of BT+Ex.
2. Materials and Methods
2.1. Search Strategy
A systematic literature review was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [24]. Searches were conducted in September 2019, thus identifying articles published prior to this date. No restrictions were placed on how long ago the study was published. Potential studies were identified using electronic databases including MEDLINE, PUBMED, PsychArticles, and the Cochrane Central Register of Clinical Trials. Search terms included “depression”, “anxiety”, “behavioral therapy”, “cognitive behavioral therapy”, “physical activity”, and “exercise” in various combinations along with movement-based meditation activities such as “yoga” and “tai-chi”. An example search query included “depression” OR “anxiety” AND “exercise” OR “physical activity” AND “behavioral therapy” OR “cognitive behavioral therapy” AND “randomized controlled trial”. In addition, reference lists of original and review articles were manually evaluated for studies not identified during the database search. After an initial screening of titles and abstracts, studies were assessed for inclusion and exclusion criteria.
2.2. Selection Criteria
Included in this meta-analysis were randomized controlled trials (RCT) that (1) enrolled human subjects that were evaluated for depression or anxiety or elevated symptoms of depression or anxiety (by any established criteria or validated screening measure), (2) enrolled subjects aged 18 and above, or (3) compared the effects of behavioral therapy (BT) to the effects of behavioral therapy treatment combined with exercise (BT+Ex) (i.e., aerobic, resistance, mind-body). Studies were excluded if (1) they compared acute treatments (single session of exercise or traditional treatment), (2) the intervention (traditional treatment or exercise) was only educational (i.e., teaching behavioral strategies or how to exercise), or (3) they were cross-sectional or observational in nature.
2.3. Data Extraction and Outcome Assessment
Data extraction was carried out independently by two authors and disagreements were resolved by consensus. The following information was extracted from each article: Subject characteristics (sex, age, race, disease condition), study characteristics (publication year, country of origin, intervention), and change in depressive or anxiety symptoms. The primary outcome was a change in symptoms of anxiety or depression after a BT or BT+Ex intervention.
2.4. Bias and Limitations
A bias assessment was performed using the Cochrane Collaboration’s Tool for Assessing Risk of Bias [25]. Studies were evaluated for six domains of bias: selection, performance, detection, attrition, reporting, and other biases.
2.5. Statistical Analysis
Using a random effects model, a meta-analysis was conducted using Meta Essentials for Microsoft Excel [26]. For each reported depression and anxiety outcome, mean change was calculated as percent change from the baseline symptom score to account for variation in depression or anxiety scales between studies. Effect size (ES) for change in depression and anxiety symptoms was determined as the mean difference of BT and BT+Ex divided by pooled standard deviation. Studies were weighted using a random effects model to calculate a combined ES (Hedge’s g). Subgroup analyses were performed only if 10 studies were included for each outcome [27,28]. Targeted covariates within depression included exercise type (aerobic or combined aerobic and resistance exercise), exercise intensity (moderate or high intensity), and baseline depression level (elevated or non-elevated). Mind-body exercise was not included in covariate analysis of exercise type as there were too few studies. Additionally, no subgroup analyses could be performed within the anxiety studies due to the small number of studies. Meta-regression analyses were performed with total study duration (in weeks), percent of female subjects, and participant age as moderators. Statistical significance was set at p < 0.05.
3. Results
3.1. Literature Search and Publication Bias
The initial electronic searches yielded 679 records. A search of reference lists from retrieved review articles was manually reviewed and yielded an additional 3 records. After deletion of duplicates (n = 5), titles and abstracts were read to remove irrelevant records. A search in additional sources yielded 3 additional studies. An assessment of full text articles was performed for 36 articles; 18 studies met the inclusion criteria (Figure 1). All studies evaluated either depression, anxiety, or both using validated symptom scales. Study characteristics are presented in Table 1. Overall, the quality of studies was moderate to high. Randomization methods (random sequence generation) were reported in all studies. It was difficult to assess allocation concealment as details were not provided regarding the role of investigators enrolling patients. Participants and personnel were not blinded to the exercise study and outcomes, which indicates a high risk for bias; however, it is unlikely that this caused bias. All studies reported attrition, but evaluation of dropouts was not completed across all studies, and therefore the bias created is uncertain. All included studies reported clinically relevant outcomes.
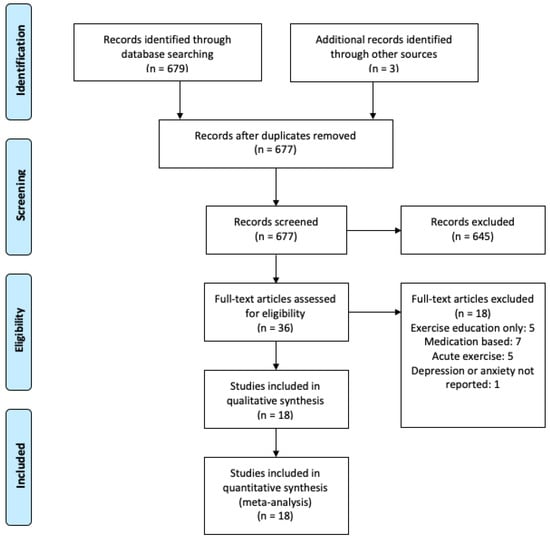
Figure 1.
Process of publication selection.

Table 1.
Study Characteristics.
3.2. Participants
Sample sizes of included studies varied from 23 to 785 participants (total = 1686, mean = 94), with an average age of 47.5 years (excluding subjects from non-BT or BT+Ex groups, i.e., control and exercise only). The majority of studies recruited both males and females with females comprising 65% of the study sample. Four studies recruited only female subjects [29,30,31,32]. A total of 12 RCTs reported comorbid conditions. Comorbidities included HIV [33], chronic obstructive pulmonary disease [34,35], heart failure [36], chronic low back pain [37,38], breast cancer [30], schizophrenia [22], binge eating disorder [31], PTSD [39], pregnancy [32] and stroke [40].
3.3. Intervention Characteristics
Behavioral therapy interventions included cognitive behavioral therapy (CBT), psychotherapy (Psy), stress management (SM), education (Edu), cognitive training, and a brief cognitive program classified as ‘‘other’’. The majority of studies employed CBT (n = 11) [29,31,34,36,38,40,41,42,43,44,45]. Two studies used mixed behavioral therapies (CBT+Psy [34], SM+Edu [35]). Nine studies employed aerobic exercise (AE) as the sole exercise type [22,31,32,33,36,41,42,44,45], two studies used resistance exercise (RE) [39,43], six studies combined AE and RE [30,34,35,37,38,40], and one study employed yoga [29]. No studies were identified that implemented Tai Chi exercise. Nine studies required participants to perform exercise in a supervised setting while two studies were home or gym based (not supervised by member of the research team).
Studies varied regarding the specific questionnaire used to assess depression and anxiety. Depression questionnaires included Beck Depression Inventory (BDI, n = 9), Center for Epidemiologic Studies Depression Scale (CES-D, n = 2), Hamilton Depression Rating Scale (HAM-D, n = 1), Hospital Anxiety and Depression Scale (HADS-D, n = 2), Taiwanese Depression Questionnaire (TDQ, n = 1), Depression Anxiety Stress Scales (DASS-D, n = 2), and Edinburgh Postnatal Depression Scale (EPDS, n = 1). Anxiety questionnaires included Hospital Anxiety and Depression Scale (HADS-A, n = 2), Depression Anxiety Stress Scales (DASS-A, n = 2), State-Trait Anxiety Inventory (STAI, n = 3) and Beck Anxiety Inventory (BAI, n = 1).
3.4. Effects of BT and BT+Ex on Depression
All studies examined the impact of BT (mean n of subjects = 46) vs. BT+Ex (mean n of subjects = 47) on depressive symptoms (n = 18). The effect of BT+Ex on depression was significant (g = −0.47; 95% CI [−0.83, −0.12]; p = 0.005), as displayed in Figure 2.
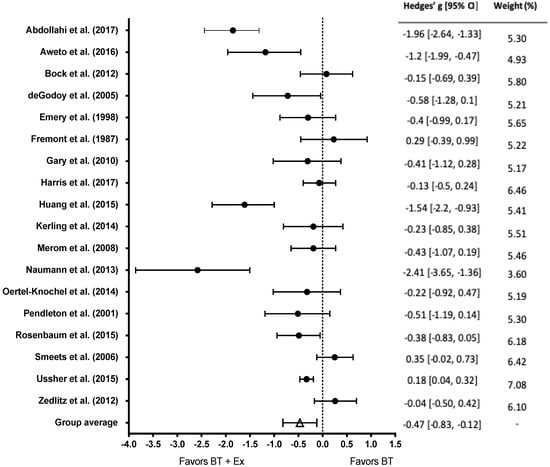
Figure 2.
Overall effect of BT+Ex on depression. Test for overall effect g = −0.47, p = 0.005; BT+Ex = Behavioral Therapy + Exercise, BT = Behavioral Therapy only.
3.5. Subgroup Analysis of Exercise Intensity
In total, 13 studies reported exercise intensity and were included in the intensity subgroup analysis. Ten studies investigated the effect of moderate intensity exercise while three studies investigated the effect of high intensity exercise on depression (Figure 3). The effect of moderate intensity exercise was significant (g = −0.77, 95% CI [−1.31, −0.23]; p < 0.01); however, the effect of high intensity exercise interventions was not (g = −0.17, 95% CI [−0.73, −0.40]; p > 0.05).
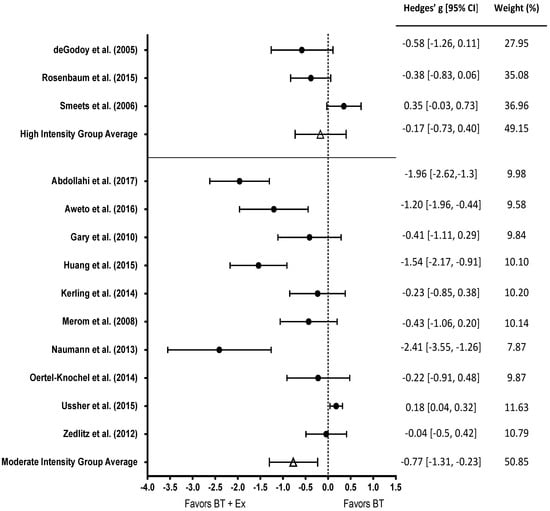
Figure 3.
Subgroup analysis of BT+ high intensity (top) and BT+ moderate intensity exercise (bottom) among studies that measured depression. Test for overall effect of high intensity g = −0.17, p > 0.05. Test for overall effect of moderate intensity g = −0.77, p < 0.01. BT+Ex = Behavioral Therapy + Exercise, BT = Behavioral Therapy only.
3.6. Subgroup Analysis of Type of Exercise
Nine studies employed an aerobic exercise intervention, six studies combined aerobic and resistance exercise (Figure 4). There was a significant effect for aerobic exercise (g = −0.48, 95% CI [−0.93, −0.02]; p = 0.03); however, there was no effect for combined exercise (g = −0.37, 95% CI [−1.04, 0.29]; p > 0.05).
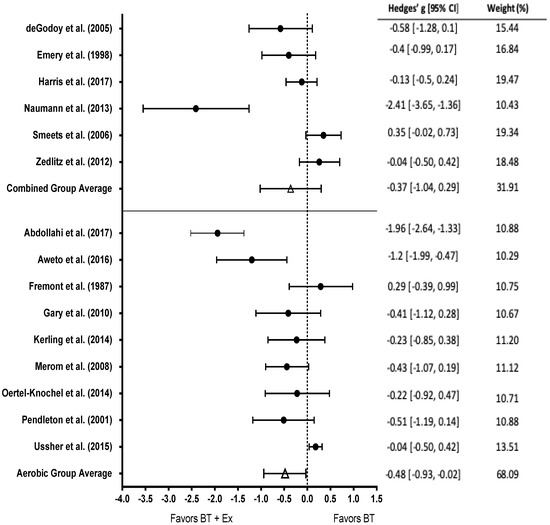
Figure 4.
Subgroup analysis of combined aerobic and resistance (top) and aerobic exercise only (bottom) among studies that measured depression. Test for overall effect of combined exercise g = −0.37, p > 0.05. Test for overall effect of aerobic exercise g = −0.48, p < 0.05. BT+Ex = Behavioral Therapy + Exercise, BT = Behavioral Therapy only.
3.7. Subgroup Analysis of Baseline Level of Depression
Baseline level of depression was characterized according to the guidelines of each questionnaire used. Participants in nine studies were categorized as having elevated baseline depression levels, and nine studies recruited those with healthy baseline depression levels (Figure 5). There was a significant effect among those with elevated depression levels (g = −0.47, 95% CI [−0.86, −0.08]; p = 0.03); however, there was no effect for non-elevated baseline depression (g = −.46, 95% CI [−1.02, 0.10]; p > 0.05).
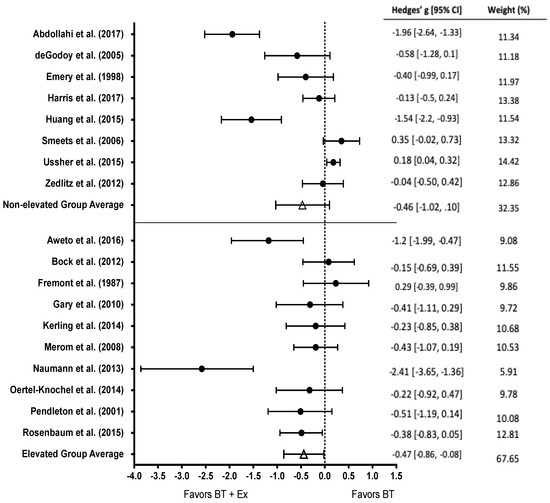
Figure 5.
Subgroup analysis of non-elevated (top) and elevated baseline depression levels (bottom) among studies that measured depression. Test for overall effect of non-elevated baseline depression g = −0.46, p > 0.05. Test for overall effect of elevated baseline depression g = −0.47, p < 0.05. BT+Ex = Behavioral Therapy + Exercise, BT = Behavioral Therapy only.
3.8. Depression Moderator Analysis
Average age of participants significantly moderated change in depression with an increase in age corresponding to a greater effect of BT+Ex on depression (lower depression scores) after the exercise intervention (β = −0.42; 95% CI [−0.05, 0.00]; p = 0.036). Percentage of female subjects (β = 0.14; 95% CI [−0.79, 1.53]; p = 0.498) and duration of intervention (β = 0.00; 95% CI [−0.12, 0.12]; p = 0.990) were not associated with effect size of BT+Ex.
3.9. Effects of BT and BT+Ex on Anxiety
Eight studies reported pre- and post- anxiety scale scores. No significant effect of BT+Ex was observed for anxiety (Hedge’s g = −0.21, CI [−0.48 to 0.06]; p = 0.063, Figure 6).
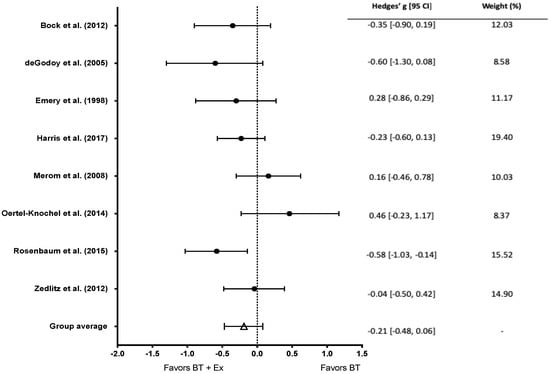
Figure 6.
Overall effect of BT+Ex on anxiety. Test for overall effect g = −0.21, p > 0.05. BT+Ex = Behavioral Therapy + Exercise, BT = Behavioral Therapy only.
3.10. Anxiety Moderator Analysis
Average age of participants (β = −0.46; 95% CI [−0.05, 0.02]; p = 0.237), percentage of female subjects (β = 0.46; 95% CI [−0.45, 1.58]; p = 0.189), and duration of intervention (β = −0.59; 95% CI [−0.17, 0.02]; p = 0.076) did not moderate the effect of BT+Ex on change in anxiety symptoms.
4. Discussion
The purpose of the present meta-analysis was to determine if the addition of exercise to BT results in augmented improvements of depression and anxiety symptoms. Results from this meta-analysis indicate that BT+Ex is a more effective treatment for depression than BT alone with a medium and significant negative effect size (Hedge’s g = −0.47) irrespective of exercise type, intensity, and baseline levels of depression. Further, findings indicate that this relationship is moderated by the average age of subjects with an increase in age corresponding to a greater effect of BT+Ex depression after the exercise intervention. Conversely, BT+Ex does not appear to be significantly more effective than BT for a reduction in anxiety (Hedge’s g = −0.21).
This meta-analysis compared the effectiveness of BT+Ex and BT alone on symptoms of depression and anxiety, when BT is defined as any type of behavioral therapy. A previous meta-analysis compared the effectiveness of CBT+Ex vs. CBT on change in depressive symptoms and found no significant difference between the two intervention groups (CBT+Ex vs. CBT alone) [20]. It is also important to note that the authors included studies that used both exercise interventions and exercise education interventions. The inclusion of studies lacking an active exercise component may explain the differing results with the present study. Further, Bernard et al. [20] included studies that recruited only participants with chronic disease. The inclusion of both healthy and clinical population studies in the present meta-analysis may further explain the differences observed in the current results. For example, BT+Ex had a large effect (g = −2.41) on lowering depression among breast cancer survivors [30]. This population, similar to others, is susceptible to other comorbidities, such as obesity, and low cardiovascular fitness. Exercise may assist with treating these additional abnormalities, which likely improves one’s behavioral state. Interpretations should be made with caution as the sample size, and thus the weight of the included study was small [30].
Depression is characterized by both behavioral and physiological pathologies. The psychobiological nature of depression may, in part, explain why BT+Ex was shown to be effective compared to BT in the present study. Specifically, the therapeutic benefit of psychotherapy is largely attributed to an improvement in psychological constructs, while the therapeutic benefit of exercise may be due to physiological changes. Regarding psychological constructs, depression is related to dysfunctional attitudes, negative thoughts, and rumination. Psychotherapy is proposed to reduce the prevalence of these components, thereby yielding an antidepressant effect through psychological changes [46]. Alternately, depression has been associated with reduced size of brain regions that play a role in emotion regulation including the hippocampus, anterior cingulate cortex, and prefrontal cortex [47]. Interestingly, exercise intervention studies have reported structural changes and increased size of these brain regions in response to the intervention [48,49]. Researchers speculate that the volumetric changes are a result of increased neurogenesis due to exercise-induced expression of neurotrophic factors [50]. Further, the neural benefits of exercise may be augmented in individuals experiencing age-related brain atrophy, which potentially explains the moderating effect of age reported in the present study [50]. The psychological and physiological changes promoted through BT+Ex may explain the greater effect of the combined treatment compared to BT alone.
In contrast to depression, BT+Ex was not significantly more effective than BT alone for reducing symptoms of anxiety. This may be due to a more immediate role of exercise in reducing anxiety. One proposed mechanism regarding the anxiolytic effect of exercise is termed the ‘‘endorphin hypothesis’’. This theory speculates that the acute release of β-endorphins reduces anxiety symptoms, thus explaining the role of exercise on anxiety [51]. Thus, the transient nature of the therapeutic benefit of exercise may explain why no differences were observed between BT+Ex and BT alone, as the anxiolytic effects were not observed after acute exercise, but rather after a chronic exercise intervention.
Limitations
Despite the moderate to high quality of the included studies, there are several limitations that should be noted. First, several studies did not report intensity of exercise (n = 6), potentially masking or skewing the intensity-dependent effect of exercise on depression and anxiety. Second, only 13 of the studies used a sample population with elevated depressive symptoms, which may temper the effect of the BT and BT+Ex intervention. Third, studies used various diagnostic criteria for depression and anxiety, limiting the ability to directly compare the magnitude of effect across all studies. Fourth, high levels of statistical heterogeneity were observed within depression analyses among studies. This may be explained by variations exercise program characteristics (e.g., exercise intensity, type), behavioral therapy characteristics (e.g., type of therapy), and overall intervention characteristics (e.g., duration, group vs. individualized, reason for treatment). Future studies should provide inclusive methodological descriptions of the exercise intervention (type, duration, intensity), recruit individuals with elevated levels of depression or anxiety, measure depression and anxiety using common methods of assessment (i.e., BDI, HADS).
5. Conclusions
The findings of this meta-analysis provide support for the use of exercise as an effective adjunct treatment for depression across a range of comorbidities. Specifically, the addition of moderate intensity exercise to BT may yield superior improvements in depression symptoms. Similarly, aerobic exercise interventions appear to be more beneficial than combined aerobic plus resistance training programs. Further, the moderating effect of age on BT+Ex indicates that the effectiveness of BT+Ex may be augmented in older individuals. Together, exercise may provide an inexpensive, effective addition to traditional behavioral therapy. To develop individualized BT+Ex programs, future research is needed to elucidate the mechanistic changes that explain the benefits of BT+Ex for depression and anxiety reduction.
Author Contributions
Conceptualization, M.Z. and K.B.; methodology, M.Z., T.M., K.B., and A.A.; investigation, M.Z., K.B., T.M., and A.A.; analyses M.Z. and K.B.; writing—original draft preparation, K.B. and M.Z.; writing—review and editing, K.B., M.Z., T.M., and A.A.; supervision, M.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interests.
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Gili, M.; Comas, A.; García-García, M.; Monzón, S.; Antoni, S.-B.; Roca, M. Comorbidity between common mental disorders and chronic somatic diseases in primary care patients. Gen. Hosp. Psychiatry 2010, 32, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Seldenrijk, A.; Vogelzangs, N.; Batelaan, N.M.; Wieman, I.; van Schaik, D.J.F.; Penninx, B.J.W.H. Depression, anxiety and 6-year risk of cardiovascular disease. J. Psychosom. Res. 2015, 78, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Roest, A.M.; Martens, E.J.; de Jonge, P.; Denollet, J. Anxiety and risk of incident coronary heart disease: A meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Knol, M.J.; Twisk, J.W.R.; Beekman, A.T.F.; Heine, R.J.; Snoek, F.J.; Pouwer, F. Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia 2006, 49, 837. [Google Scholar] [CrossRef]
- Engum, A. The role of depression and anxiety in onset of diabetes in a large population-based study. J. Psychosom. Res. 2007, 62, 31–38. [Google Scholar] [CrossRef]
- Meng, L.; Chen, D.; Yang, Y.; Zheng, Y.; Hui, R. Depression increases the risk of hypertension incidence: A meta-analysis of prospective cohort studies. J. Hypertens. 2012, 30, 842–851. [Google Scholar] [CrossRef]
- Barger, S.D.; Sydeman, S.J. Does generalized anxiety disorder predict coronary heart disease risk factors independently of major depressive disorder? J. Affect. Disord. 2005, 88, 87–91. [Google Scholar] [CrossRef]
- Doering, L.V.; Moser, D.K.; Riegel, B.; McKinley, S.; Davidson, P.; Baker, H.; Meischke, H.; Dracup, K. Persistent comorbid symptoms of depression and anxiety predict mortality in heart disease. Int. J. Cardiol. 2010, 145, 188–192. [Google Scholar] [CrossRef]
- Herrmann-Lingen, C.; Klemme, H.; Meyer, T. Depressed mood, physician-rated prognosis, and comorbidity as independent predictors of 1-year mortality in consecutive medical inpatients. J. Psychosom. Res. 2001, 50, 295–301. [Google Scholar] [CrossRef]
- Kok, R.M.; Reynolds, C.F. Management of depression in older adults: A review. JAMA 2017, 317, 2114–2122. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Michaelis, S.; Wedekind, D. Treatment of anxiety disorders. Dialogues Clin. Neurosci. 2017, 19, 93. [Google Scholar] [PubMed]
- Powers, M.B.; de Kleine, R.A.; Smits, J.A.J. Core mechanisms of cognitive behavioral therapy for anxiety and depression: A review. Psychiatr. Clin. N. Am. 2017, 40, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Hansen, N.B.; Lambert, M.J.; Forman, E.M. The psychotherapy dose-response effect and its implications for treatment delivery services. Clin. Psychol. Sci. Pract. 2002, 9, 329–343. [Google Scholar] [CrossRef]
- Hunot, V.; Churchill, R.; Teixeira, V.; de Lima, M.S. Psychological therapies for generalised anxiety disorder. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef] [PubMed]
- Durham, R.C.; Chambers, J.A.; Power, K.G.; Sharp, D.M.; Macdonald, R.R.; Major, K.A.; Dow, M.G.T.; Gumley, A.I. Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland. Health Technol. Assess. 2005, 9, 1–174. [Google Scholar] [CrossRef]
- Stonerock, G.L.; Hoffman, B.M.; Smith, P.J.; Blumenthal, J.A. Exercise as treatment for anxiety: Systematic review and analysis. Ann. Behav. Med. 2015, 49, 542–556. [Google Scholar] [CrossRef]
- American Psychiatric, A. Diagnostic and statistical manual of mental disorders. BMC Med. 2013, 17, 133–137. [Google Scholar]
- Bernard, P.; Romain, A.-J.; Caudroit, J.; Chevance, G.; Carayol, M.; Gourlan, M.; Needham Dancause, K.; Moullec, G. Cognitive behavior therapy combined with exercise for adults with chronic diseases: Systematic review and meta-analysis. Health Psychol. 2018, 37, 433. [Google Scholar] [CrossRef] [PubMed]
- Ernst, C.; Olson, A.K.; Pinel, J.P.J.; Lam, R.W.; Christie, B.R. Antidepressant effects of exercise: Evidence for an adult-neurogenesis hypothesis? J. Psychiatry Neurosci. 2006, 31, 84–92. [Google Scholar]
- Oertel-Knöchel, V.; Mehler, P.; Thiel, C.; Steinbrecher, K.; Malchow, B.; Tesky, V.; Ademmer, K.; Prvulovic, D.; Banzer, W.; Zopf, Y. Effects of aerobic exercise on cognitive performance and individual psychopathology in depressive and schizophrenia patients. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; van Praag, H. Exercise and the brain: Neurogenesis, synaptic plasticity, spine density, and angiogenesis. In Functional Neuroimaging in Exercise and Sport Sciences; Springer: Berlin/Heidelberg, Germany, 2012; pp. 3–24. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Van Rhee, H.; Suurmond, R.; Hak, T. User manual for Meta-Essentials: Workbooks for meta-analysis. SSRN Electron. J. 2015. [Google Scholar] [CrossRef]
- Thompson, S.G.; Higgins, J.P.T. How should meta-regression analyses be undertaken and interpreted? Stat. Med. 2002, 21, 1559–1573. [Google Scholar] [CrossRef]
- Oxman, A.D.; Guyatt, G.H. A consumer’s guide to subgroup analyses. Ann. Intern. Med. 1992, 116, 78–84. [Google Scholar] [CrossRef]
- Bock, B.C.; Fava, J.L.; Gaskins, R.; Morrow, K.M.; Williams, D.M.; Jennings, E.; Becker, B.M.; Tremont, G.; Marcus, B.H. Yoga as a complementary treatment for smoking cessation in women. J. Womens Health 2012, 21, 240–248. [Google Scholar] [CrossRef]
- Naumann, F.; Martin, E.; Philpott, M.; Smith, C.; Groff, D.; Battaglini, C. Can counseling add value to an exercise intervention for improving quality of life in breast cancer survivors? A feasibility study. J. Support. Oncol. 2012, 10, 188–194. [Google Scholar] [CrossRef]
- Pendleton, V.R.; Goodrick, G.K.; Poston, W.S.C.; Reeves, R.S.; Foreyt, J.P. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int. J. Eat. Disord. 2002, 31, 172–184. [Google Scholar] [CrossRef]
- Ussher, M.; Lewis, S.; Aveyard, P.; Manyonda, I.; West, R.; Lewis, B.; Marcus, B.; Riaz, M.; Taylor, A.H.; Barton, P. The London Exercise And Pregnant smokers (LEAP) trial: A randomised controlled trial of physical activity for smoking cessation in pregnancy with an economic evaluation. Health Technol. Assess. 2015, 19, 1–135. [Google Scholar] [CrossRef]
- Aweto, H.A.; Aiyegbusi, A.I.; Ugonabo, A.J.; Adeyemo, T.A. Effects of aerobic exercise on the pulmonary functions, respiratory symptoms and psychological status of people living with HIV. J. Res. Health Sci. 2016, 16, 17–21. [Google Scholar] [PubMed]
- DeGodoy, D.V.; DeGodoy, R.F.d.; Becker Júnior, B.; Vaccari, P.F.; Michelli, M.; Teixeira, P.J.Z.; Palombini, B.C. The effect of psychotherapy provided as part of a pulmonary rehabilitation program for the treatment of patients with chronic obstructive pulmonary disease. J. Bras. Pneumol. 2005, 31, 499–505. [Google Scholar]
- Emery, C.F.; Schein, R.L.; Hauck, E.R.; MacIntyre, N.R. Psychological and cognitive outcomes of a randomized trial of exercise among patients with chronic obstructive pulmonary disease. Health Psychol. 1998, 17, 232. [Google Scholar] [CrossRef]
- Gary, R.A.; Dunbar, S.B.; Higgins, M.K.; Musselman, D.L.; Smith, A.L. Combined exercise and cognitive behavioral therapy improves outcomes in patients with heart failure. J. Psychosom. Res. 2010, 69, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Moe, T.F.; Eriksen, H.R.; Tangen, T.; Lie, S.A.; Tveito, T.H.; Reme, S.E. Brief intervention, physical exercise and cognitive behavioural group therapy for patients with chronic low back pain (The CINS trial). Eur. J. Pain 2017, 21, 1397–1407. [Google Scholar] [CrossRef]
- Smeets, R.J.E.M.; Vlaeyen, J.W.S.; Hidding, A.; Kester, A.D.M.; van der Heijden, G.J.M.G.; van Geel, A.C.M.; Knottnerus, J.A. Active rehabilitation for chronic low back pain: Cognitive-behavioral, physical, or both? First direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet. Disord. 2006, 7, 5. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Sherrington, C.; Tiedemann, A. Exercise augmentation compared with usual care for post-traumatic stress disorder: A randomized controlled trial. Acta Psychiatr. Scand. 2015, 131, 350–359. [Google Scholar] [CrossRef]
- Zedlitz, A.M.E.E.; Rietveld, T.C.M.; Geurts, A.C.; Fasotti, L. Cognitive and graded activity training can alleviate persistent fatigue after stroke: A randomized, controlled trial. Stroke 2012, 43, 1046–1051. [Google Scholar] [CrossRef]
- Abdollahi, A.; LeBouthillier, D.M.; Najafi, M.; Asmundson, G.J.G.; Hosseinian, S.; Shahidi, S.; Carlbring, P.; Kalhori, A.; Sadeghi, H.; Jalili, M. Effect of exercise augmentation of cognitive behavioural therapy for the treatment of suicidal ideation and depression. J. Affect. Disord. 2017, 219, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Fremont, J.; Craighead, L.W. Aerobic exercise and cognitive therapy in the treatment of dysphoric moods. Cognit. Ther. Res. 1987, 11, 241–251. [Google Scholar] [CrossRef]
- Huang, T.-T.; Chung, M.-L.; Chen, F.-R.; Chin, Y.-F.; Wang, B.-H. Evaluation of a combined cognitive-behavioural and exercise intervention to manage fear of falling among elderly residents in nursing homes. Aging Ment. Health 2016, 20, 2–12. [Google Scholar] [CrossRef]
- Kerling, A.; Tegtbur, U.; Gützlaff, E.; Kück, M.; Borchert, L.; Ates, Z.; von Bohlen, A.; Frieling, H.; Hüper, K.; Hartung, D. Effects of adjunctive exercise on physiological and psychological parameters in depression: A randomized pilot trial. J. Affect. Disord. 2015, 177, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Merom, D.; Phongsavan, P.; Wagner, R.; Chey, T.; Marnane, C.; Steel, Z.; Silove, D.; Bauman, A. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—A pilot group randomized trial. J. Anxiety Disord. 2008, 22, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, L.H.J.M.; Müller, V.N.L.S.; Arntz, A.; Huibers, M.J.H. Mechanisms of change in psychotherapy for depression: An empirical update and evaluation of research aimed at identifying psychological mediators. Clin. Psychol. Rev. 2016, 50, 95–107. [Google Scholar] [CrossRef]
- Liu, W.; Ge, T.; Leng, Y.; Pan, Z.; Fan, J.; Yang, W.; Cui, R. The role of neural plasticity in depression: From hippocampus to prefrontal cortex. Neural Plast. 2017, 2017, 6871089. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.J.; Erickson, K.I.; Scalf, P.E.; Kim, J.S.; Prakash, R.; McAuley, E.; Elavsky, S.; Marquez, D.X.; Hu, L.; Kramer, A.F. Aerobic exercise training increases brain volume in aging humans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1166–1170. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [PubMed]
- Gujral, S.; Aizenstein, H.; Reynolds Iii, C.F.; Butters, M.A.; Erickson, K.I. Exercise effects on depression: Possible neural mechanisms. Gen. Hosp. Psychiatry 2017, 49, 2–10. [Google Scholar] [CrossRef]
- Anderson, E.H.; Shivakumar, G. Effects of exercise and physical activity on anxiety. Front. Psychiatry 2013, 4, 27. [Google Scholar] [CrossRef] [PubMed]
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).