The Combined Effect of Exercise and Behavioral Therapy for Depression and Anxiety: Systematic Review and Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Selection Criteria
2.3. Data Extraction and Outcome Assessment
2.4. Bias and Limitations
2.5. Statistical Analysis
3. Results
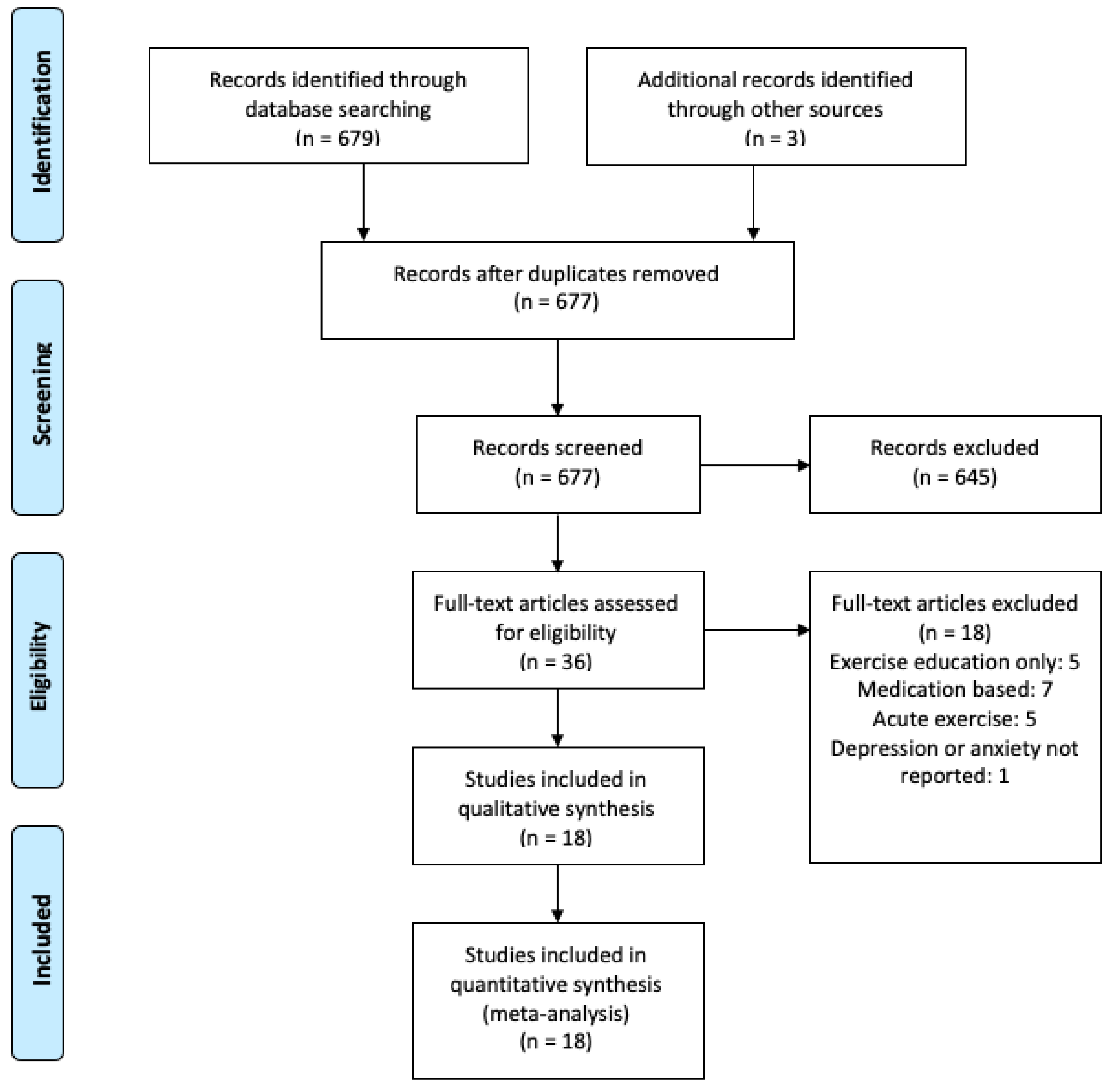
3.1. Literature Search and Publication Bias
3.2. Participants
3.3. Intervention Characteristics
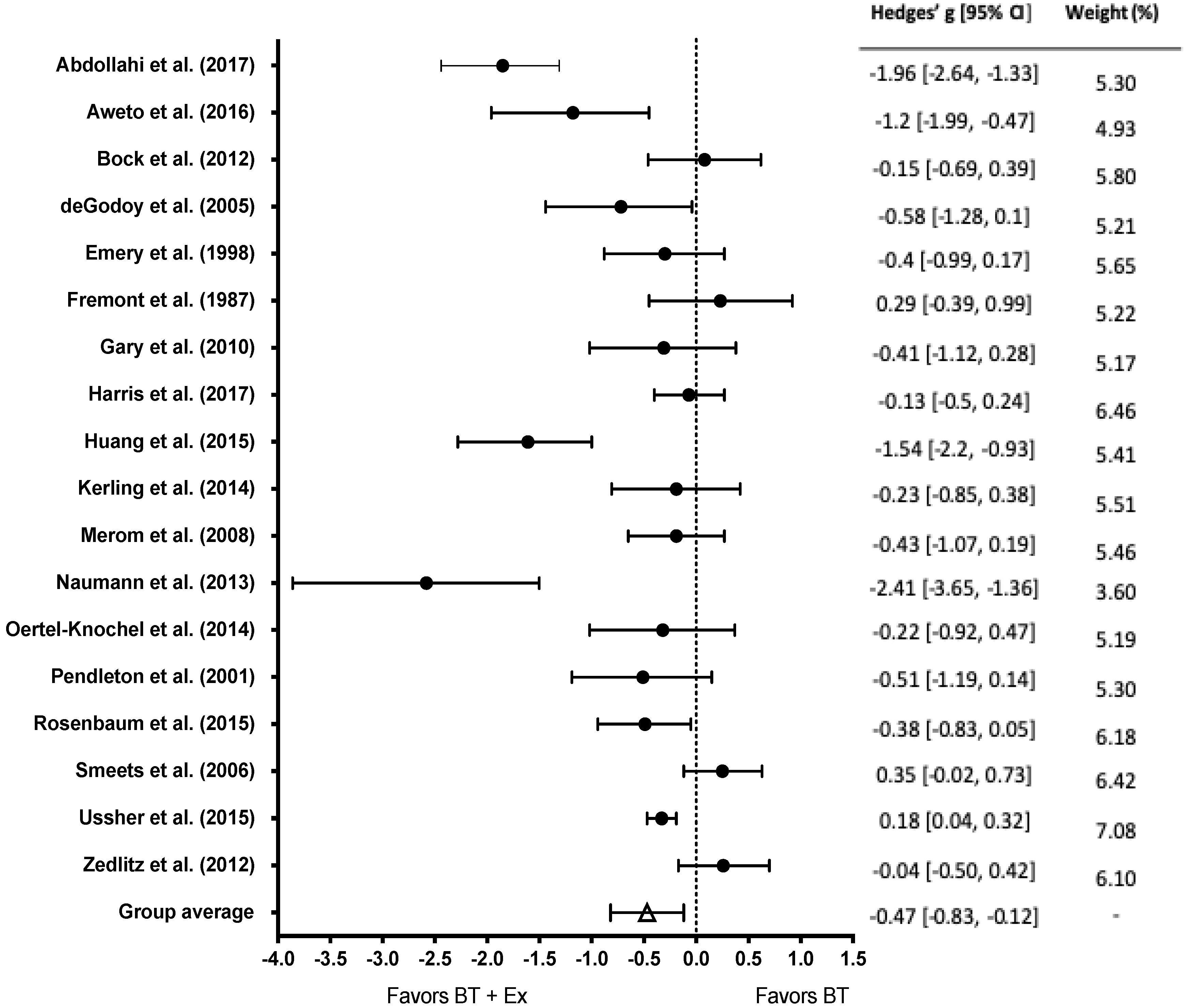
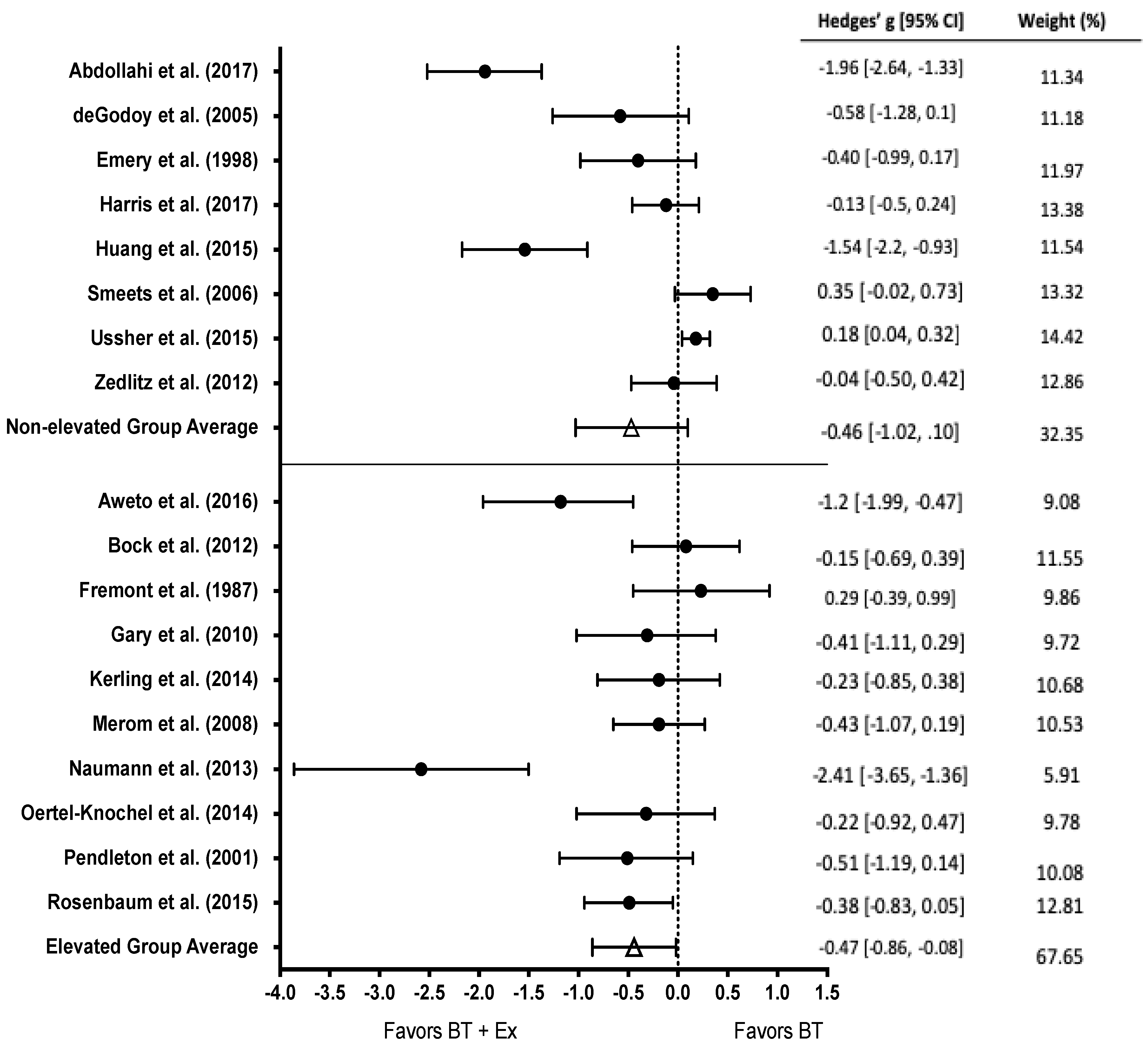
3.4. Effects of BT and BT+Ex on Depression
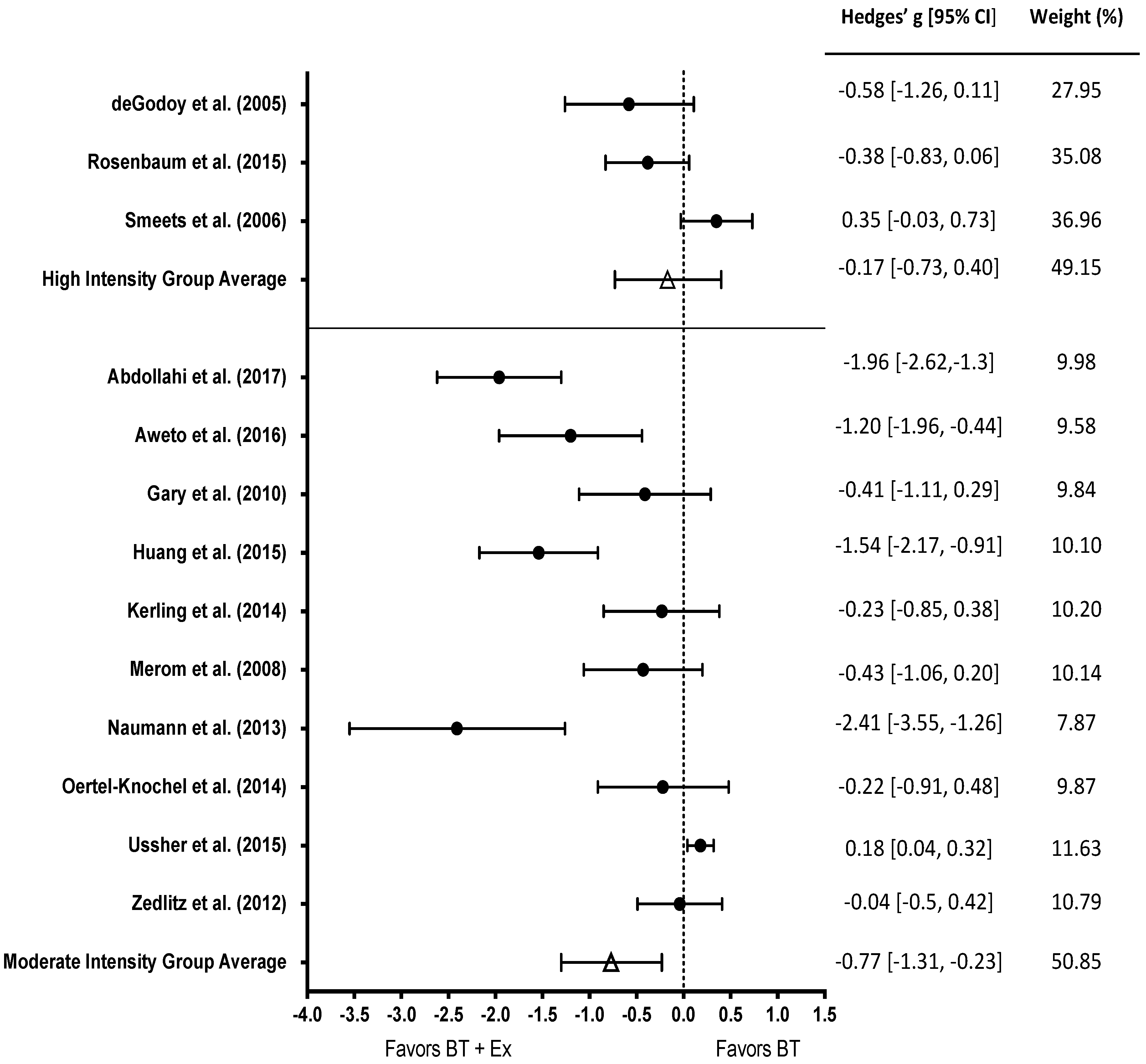
3.5. Subgroup Analysis of Exercise Intensity
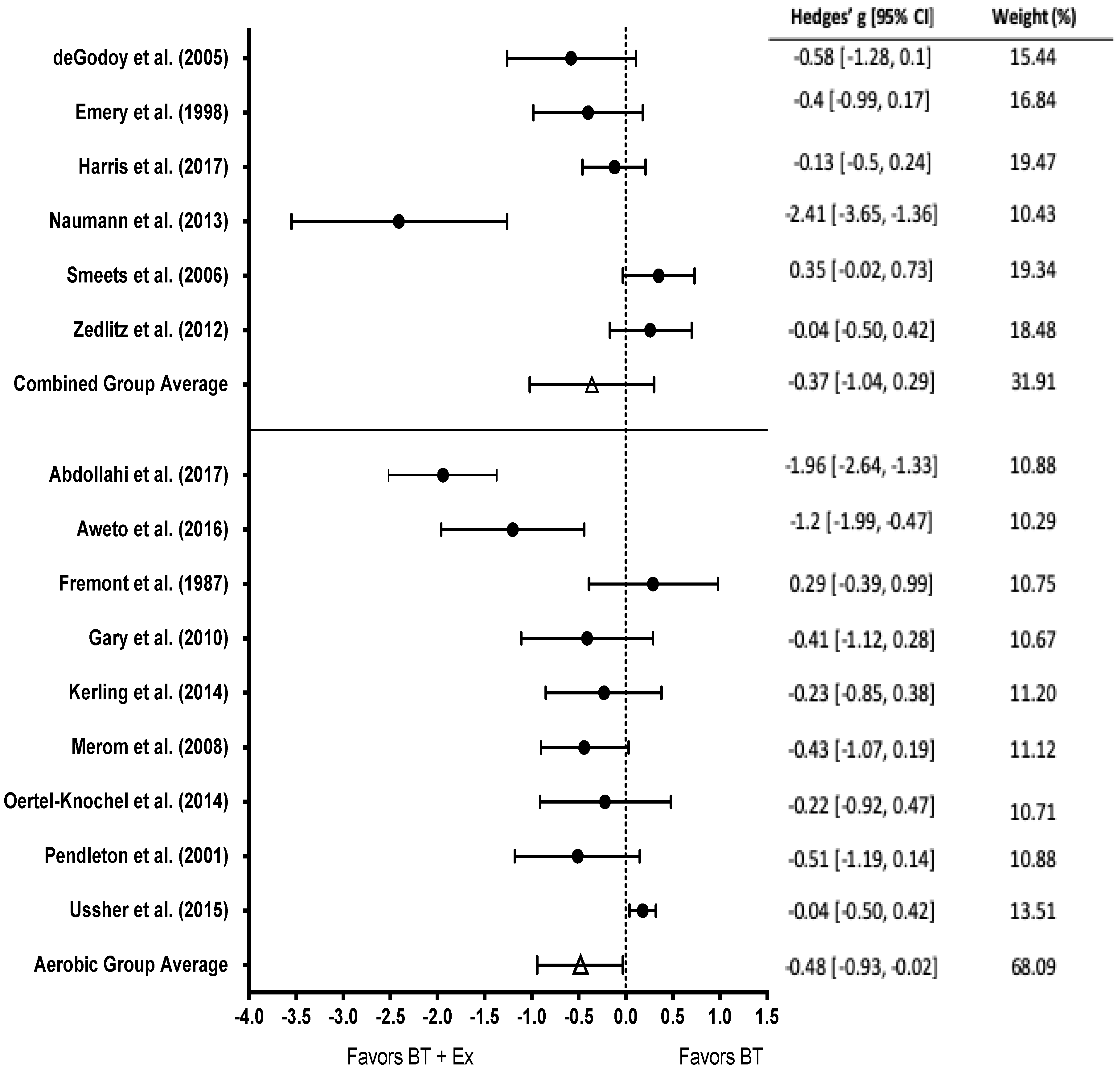
3.6. Subgroup Analysis of Type of Exercise
3.7. Subgroup Analysis of Baseline Level of Depression
3.8. Depression Moderator Analysis
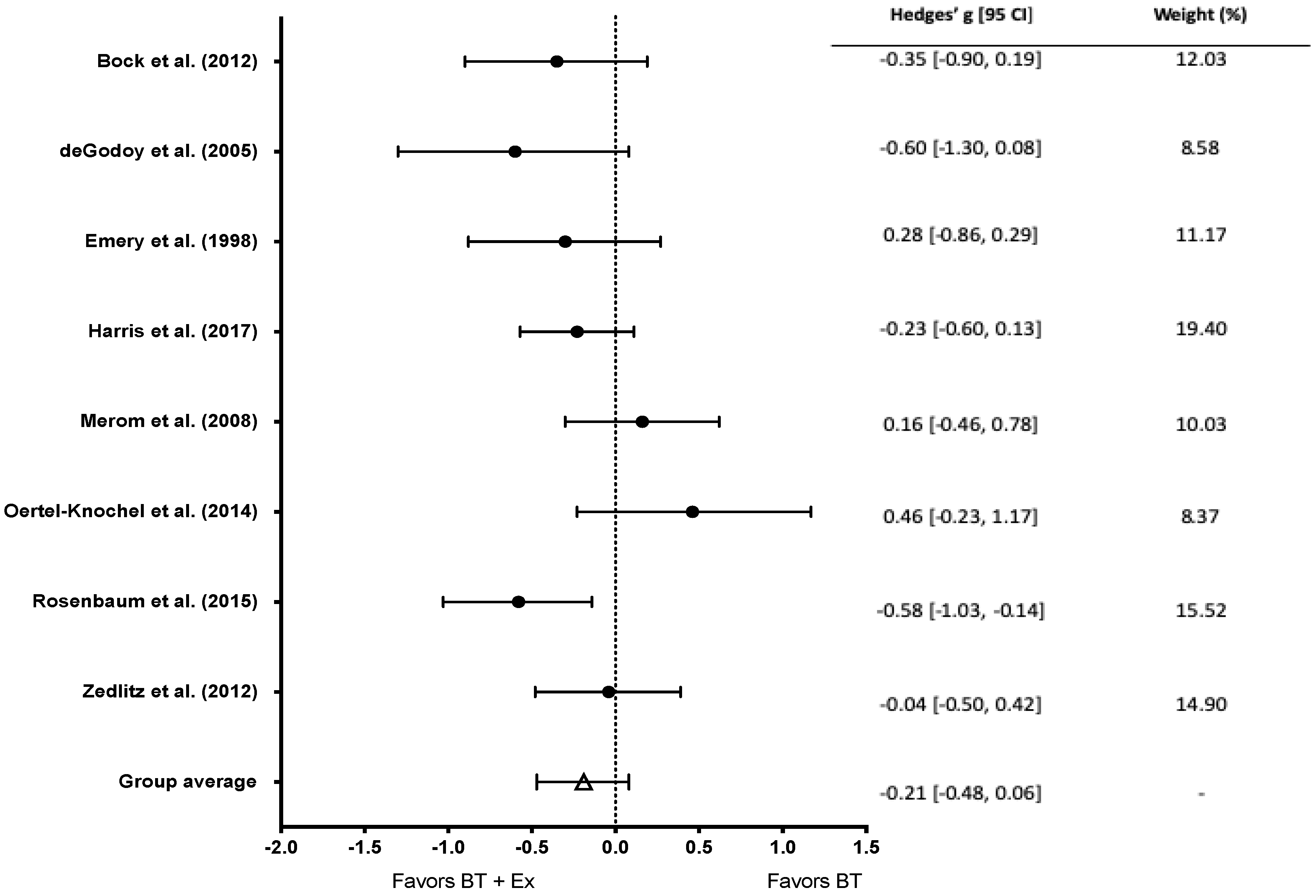
3.9. Effects of BT and BT+Ex on Anxiety
3.10. Anxiety Moderator Analysis
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Walker, E.R.; McGee, R.E.; Druss, B.G. Mortality in mental disorders and global disease burden implications: A systematic review and meta-analysis. JAMA Psychiatry 2015, 72, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Gili, M.; Comas, A.; García-García, M.; Monzón, S.; Antoni, S.-B.; Roca, M. Comorbidity between common mental disorders and chronic somatic diseases in primary care patients. Gen. Hosp. Psychiatry 2010, 32, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Seldenrijk, A.; Vogelzangs, N.; Batelaan, N.M.; Wieman, I.; van Schaik, D.J.F.; Penninx, B.J.W.H. Depression, anxiety and 6-year risk of cardiovascular disease. J. Psychosom. Res. 2015, 78, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Roest, A.M.; Martens, E.J.; de Jonge, P.; Denollet, J. Anxiety and risk of incident coronary heart disease: A meta-analysis. J. Am. Coll. Cardiol. 2010, 56, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Knol, M.J.; Twisk, J.W.R.; Beekman, A.T.F.; Heine, R.J.; Snoek, F.J.; Pouwer, F. Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia 2006, 49, 837. [Google Scholar] [CrossRef]
- Engum, A. The role of depression and anxiety in onset of diabetes in a large population-based study. J. Psychosom. Res. 2007, 62, 31–38. [Google Scholar] [CrossRef]
- Meng, L.; Chen, D.; Yang, Y.; Zheng, Y.; Hui, R. Depression increases the risk of hypertension incidence: A meta-analysis of prospective cohort studies. J. Hypertens. 2012, 30, 842–851. [Google Scholar] [CrossRef]
- Barger, S.D.; Sydeman, S.J. Does generalized anxiety disorder predict coronary heart disease risk factors independently of major depressive disorder? J. Affect. Disord. 2005, 88, 87–91. [Google Scholar] [CrossRef]
- Doering, L.V.; Moser, D.K.; Riegel, B.; McKinley, S.; Davidson, P.; Baker, H.; Meischke, H.; Dracup, K. Persistent comorbid symptoms of depression and anxiety predict mortality in heart disease. Int. J. Cardiol. 2010, 145, 188–192. [Google Scholar] [CrossRef]
- Herrmann-Lingen, C.; Klemme, H.; Meyer, T. Depressed mood, physician-rated prognosis, and comorbidity as independent predictors of 1-year mortality in consecutive medical inpatients. J. Psychosom. Res. 2001, 50, 295–301. [Google Scholar] [CrossRef]
- Kok, R.M.; Reynolds, C.F. Management of depression in older adults: A review. JAMA 2017, 317, 2114–2122. [Google Scholar] [CrossRef] [PubMed]
- Bandelow, B.; Michaelis, S.; Wedekind, D. Treatment of anxiety disorders. Dialogues Clin. Neurosci. 2017, 19, 93. [Google Scholar] [PubMed]
- Powers, M.B.; de Kleine, R.A.; Smits, J.A.J. Core mechanisms of cognitive behavioral therapy for anxiety and depression: A review. Psychiatr. Clin. N. Am. 2017, 40, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Hansen, N.B.; Lambert, M.J.; Forman, E.M. The psychotherapy dose-response effect and its implications for treatment delivery services. Clin. Psychol. Sci. Pract. 2002, 9, 329–343. [Google Scholar] [CrossRef]
- Hunot, V.; Churchill, R.; Teixeira, V.; de Lima, M.S. Psychological therapies for generalised anxiety disorder. Cochrane Database Syst. Rev. 2007. [Google Scholar] [CrossRef] [PubMed]
- Durham, R.C.; Chambers, J.A.; Power, K.G.; Sharp, D.M.; Macdonald, R.R.; Major, K.A.; Dow, M.G.T.; Gumley, A.I. Long-term outcome of cognitive behaviour therapy clinical trials in central Scotland. Health Technol. Assess. 2005, 9, 1–174. [Google Scholar] [CrossRef]
- Stonerock, G.L.; Hoffman, B.M.; Smith, P.J.; Blumenthal, J.A. Exercise as treatment for anxiety: Systematic review and analysis. Ann. Behav. Med. 2015, 49, 542–556. [Google Scholar] [CrossRef]
- American Psychiatric, A. Diagnostic and statistical manual of mental disorders. BMC Med. 2013, 17, 133–137. [Google Scholar]
- Bernard, P.; Romain, A.-J.; Caudroit, J.; Chevance, G.; Carayol, M.; Gourlan, M.; Needham Dancause, K.; Moullec, G. Cognitive behavior therapy combined with exercise for adults with chronic diseases: Systematic review and meta-analysis. Health Psychol. 2018, 37, 433. [Google Scholar] [CrossRef] [PubMed]
- Ernst, C.; Olson, A.K.; Pinel, J.P.J.; Lam, R.W.; Christie, B.R. Antidepressant effects of exercise: Evidence for an adult-neurogenesis hypothesis? J. Psychiatry Neurosci. 2006, 31, 84–92. [Google Scholar]
- Oertel-Knöchel, V.; Mehler, P.; Thiel, C.; Steinbrecher, K.; Malchow, B.; Tesky, V.; Ademmer, K.; Prvulovic, D.; Banzer, W.; Zopf, Y. Effects of aerobic exercise on cognitive performance and individual psychopathology in depressive and schizophrenia patients. Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264, 589–604. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; van Praag, H. Exercise and the brain: Neurogenesis, synaptic plasticity, spine density, and angiogenesis. In Functional Neuroimaging in Exercise and Sport Sciences; Springer: Berlin/Heidelberg, Germany, 2012; pp. 3–24. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Van Rhee, H.; Suurmond, R.; Hak, T. User manual for Meta-Essentials: Workbooks for meta-analysis. SSRN Electron. J. 2015. [Google Scholar] [CrossRef]
- Thompson, S.G.; Higgins, J.P.T. How should meta-regression analyses be undertaken and interpreted? Stat. Med. 2002, 21, 1559–1573. [Google Scholar] [CrossRef]
- Oxman, A.D.; Guyatt, G.H. A consumer’s guide to subgroup analyses. Ann. Intern. Med. 1992, 116, 78–84. [Google Scholar] [CrossRef]
- Bock, B.C.; Fava, J.L.; Gaskins, R.; Morrow, K.M.; Williams, D.M.; Jennings, E.; Becker, B.M.; Tremont, G.; Marcus, B.H. Yoga as a complementary treatment for smoking cessation in women. J. Womens Health 2012, 21, 240–248. [Google Scholar] [CrossRef]
- Naumann, F.; Martin, E.; Philpott, M.; Smith, C.; Groff, D.; Battaglini, C. Can counseling add value to an exercise intervention for improving quality of life in breast cancer survivors? A feasibility study. J. Support. Oncol. 2012, 10, 188–194. [Google Scholar] [CrossRef]
- Pendleton, V.R.; Goodrick, G.K.; Poston, W.S.C.; Reeves, R.S.; Foreyt, J.P. Exercise augments the effects of cognitive-behavioral therapy in the treatment of binge eating. Int. J. Eat. Disord. 2002, 31, 172–184. [Google Scholar] [CrossRef]
- Ussher, M.; Lewis, S.; Aveyard, P.; Manyonda, I.; West, R.; Lewis, B.; Marcus, B.; Riaz, M.; Taylor, A.H.; Barton, P. The London Exercise And Pregnant smokers (LEAP) trial: A randomised controlled trial of physical activity for smoking cessation in pregnancy with an economic evaluation. Health Technol. Assess. 2015, 19, 1–135. [Google Scholar] [CrossRef]
- Aweto, H.A.; Aiyegbusi, A.I.; Ugonabo, A.J.; Adeyemo, T.A. Effects of aerobic exercise on the pulmonary functions, respiratory symptoms and psychological status of people living with HIV. J. Res. Health Sci. 2016, 16, 17–21. [Google Scholar] [PubMed]
- DeGodoy, D.V.; DeGodoy, R.F.d.; Becker Júnior, B.; Vaccari, P.F.; Michelli, M.; Teixeira, P.J.Z.; Palombini, B.C. The effect of psychotherapy provided as part of a pulmonary rehabilitation program for the treatment of patients with chronic obstructive pulmonary disease. J. Bras. Pneumol. 2005, 31, 499–505. [Google Scholar]
- Emery, C.F.; Schein, R.L.; Hauck, E.R.; MacIntyre, N.R. Psychological and cognitive outcomes of a randomized trial of exercise among patients with chronic obstructive pulmonary disease. Health Psychol. 1998, 17, 232. [Google Scholar] [CrossRef]
- Gary, R.A.; Dunbar, S.B.; Higgins, M.K.; Musselman, D.L.; Smith, A.L. Combined exercise and cognitive behavioral therapy improves outcomes in patients with heart failure. J. Psychosom. Res. 2010, 69, 119–131. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Moe, T.F.; Eriksen, H.R.; Tangen, T.; Lie, S.A.; Tveito, T.H.; Reme, S.E. Brief intervention, physical exercise and cognitive behavioural group therapy for patients with chronic low back pain (The CINS trial). Eur. J. Pain 2017, 21, 1397–1407. [Google Scholar] [CrossRef]
- Smeets, R.J.E.M.; Vlaeyen, J.W.S.; Hidding, A.; Kester, A.D.M.; van der Heijden, G.J.M.G.; van Geel, A.C.M.; Knottnerus, J.A. Active rehabilitation for chronic low back pain: Cognitive-behavioral, physical, or both? First direct post-treatment results from a randomized controlled trial [ISRCTN22714229]. BMC Musculoskelet. Disord. 2006, 7, 5. [Google Scholar] [CrossRef]
- Rosenbaum, S.; Sherrington, C.; Tiedemann, A. Exercise augmentation compared with usual care for post-traumatic stress disorder: A randomized controlled trial. Acta Psychiatr. Scand. 2015, 131, 350–359. [Google Scholar] [CrossRef]
- Zedlitz, A.M.E.E.; Rietveld, T.C.M.; Geurts, A.C.; Fasotti, L. Cognitive and graded activity training can alleviate persistent fatigue after stroke: A randomized, controlled trial. Stroke 2012, 43, 1046–1051. [Google Scholar] [CrossRef]
- Abdollahi, A.; LeBouthillier, D.M.; Najafi, M.; Asmundson, G.J.G.; Hosseinian, S.; Shahidi, S.; Carlbring, P.; Kalhori, A.; Sadeghi, H.; Jalili, M. Effect of exercise augmentation of cognitive behavioural therapy for the treatment of suicidal ideation and depression. J. Affect. Disord. 2017, 219, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Fremont, J.; Craighead, L.W. Aerobic exercise and cognitive therapy in the treatment of dysphoric moods. Cognit. Ther. Res. 1987, 11, 241–251. [Google Scholar] [CrossRef]
- Huang, T.-T.; Chung, M.-L.; Chen, F.-R.; Chin, Y.-F.; Wang, B.-H. Evaluation of a combined cognitive-behavioural and exercise intervention to manage fear of falling among elderly residents in nursing homes. Aging Ment. Health 2016, 20, 2–12. [Google Scholar] [CrossRef]
- Kerling, A.; Tegtbur, U.; Gützlaff, E.; Kück, M.; Borchert, L.; Ates, Z.; von Bohlen, A.; Frieling, H.; Hüper, K.; Hartung, D. Effects of adjunctive exercise on physiological and psychological parameters in depression: A randomized pilot trial. J. Affect. Disord. 2015, 177, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Merom, D.; Phongsavan, P.; Wagner, R.; Chey, T.; Marnane, C.; Steel, Z.; Silove, D.; Bauman, A. Promoting walking as an adjunct intervention to group cognitive behavioral therapy for anxiety disorders—A pilot group randomized trial. J. Anxiety Disord. 2008, 22, 959–968. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, L.H.J.M.; Müller, V.N.L.S.; Arntz, A.; Huibers, M.J.H. Mechanisms of change in psychotherapy for depression: An empirical update and evaluation of research aimed at identifying psychological mediators. Clin. Psychol. Rev. 2016, 50, 95–107. [Google Scholar] [CrossRef]
- Liu, W.; Ge, T.; Leng, Y.; Pan, Z.; Fan, J.; Yang, W.; Cui, R. The role of neural plasticity in depression: From hippocampus to prefrontal cortex. Neural Plast. 2017, 2017, 6871089. [Google Scholar] [CrossRef] [PubMed]
- Colcombe, S.J.; Erickson, K.I.; Scalf, P.E.; Kim, J.S.; Prakash, R.; McAuley, E.; Elavsky, S.; Marquez, D.X.; Hu, L.; Kramer, A.F. Aerobic exercise training increases brain volume in aging humans. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 1166–1170. [Google Scholar] [CrossRef]
- Erickson, K.I.; Voss, M.W.; Prakash, R.S.; Basak, C.; Szabo, A.; Chaddock, L.; Kim, J.S.; Heo, S.; Alves, H.; White, S.M. Exercise training increases size of hippocampus and improves memory. Proc. Natl. Acad. Sci. USA 2011, 108, 3017–3022. [Google Scholar] [CrossRef] [PubMed]
- Gujral, S.; Aizenstein, H.; Reynolds Iii, C.F.; Butters, M.A.; Erickson, K.I. Exercise effects on depression: Possible neural mechanisms. Gen. Hosp. Psychiatry 2017, 49, 2–10. [Google Scholar] [CrossRef]
- Anderson, E.H.; Shivakumar, G. Effects of exercise and physical activity on anxiety. Front. Psychiatry 2013, 4, 27. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Behavioral Therapy | Exercise Therapy | Disorder | Diagnostic Criteria | Comorbidity | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CBT | Psy | SM | Edu | Other | AE | RE | Yoga | |||||||
| Abdollahi | 2017 | • | ◦ | ◦ | ◦ | ◦ | Group CBT, 90 min, 1×/week, 12 weeks | • | ◦ | ◦ | Supervised moderate intensity, 35 min, 3×/week, 12 weeks | Depression | BDI-II | None |
| Aweto | 2016 | ◦ | • | ◦ | ◦ | ◦ | Group counselling, 30 min, 1×/2 weeks, 6 weeks | • | ◦ | ◦ | Supervised, moderate intensity, 30 min, 3×/week, 6 weeks | Depression | BDI | HIV |
| Bock | 2012 | • | ◦ | ◦ | ◦ | ◦ | Group CBT for smoking cessation, 60 min, 1×/week, 8 weeks | ◦ | ◦ | • | Supervised vinyasa yoga, 60 min, 2×/week, 8 weeks | Depression, Anxiety | CES-D, STAI | None |
| De Godoy | 2005 | • | • | ◦ | ◦ | ◦ | Individual psychotherapy and CBT, 1×/week, 12 weeks | • | • | ◦ | Supervised, moderate to high intensity, 2×/week, 12 weeks | Depression, Anxiety | BDI, BAI | COPD |
| Emery | 1998 | ◦ | ◦ | • | • | ◦ | Group SM, 60 min, 4×/week, 5 weeks followed by 60 min, 1×/week, 5 weeks | • | • | ◦ | Group exercise, 45 min, 5×/week, 5 weeks followed by 60-90 min, 3×/week, 5 weeks | Depression, Anxiety | CES-D, STAI | COPD |
| Fremont | 1987 | • | ◦ | ◦ | ◦ | ◦ | Individual CBT, 60 min, 1×/week, 10 weeks | • | ◦ | ◦ | Supervised group exercise, 20 min, 3×/week, 10 weeks | Depression | BDI | None |
| Gary | 2010 | • | ◦ | ◦ | ◦ | ◦ | Individual, home-based CBT, 30-45 min, 1×/week, 12 weeks | • | ◦ | ◦ | Home-based exercise, 60 min, 3×/week, 12 weeks | Depression | HAM-D | Heart Failure |
| Harris | 2017 | ◦ | ◦ | ◦ | ◦ | • | Individual, brief cognitive program, 2-4 sessions, 5-day period | • | • | ◦ | Supervised, individualized exercise 90 min, 3×/week, 12 weeks | Depression, Anxiety | HADS | Chronic low back pain |
| Huang | 2015 | • | ◦ | ◦ | ◦ | ◦ | Group CBT, 20-25 min, 1×/week, 8 weeks | ◦ | • | ◦ | Supervised exercise, 30 min, 2×/week, 8 weeks | Depression | TDQ | None |
| Kerling | 2014 | • | ◦ | ◦ | ◦ | ◦ | Unspecified CBT | • | ◦ | ◦ | Supervised exercise, 45 min, 3×/week, 6 weeks | Depression | BDI | None |
| Merom | 2008 | • | ◦ | ◦ | ◦ | ◦ | Group CBT, 90 min, 1×/week, 10 weeks | • | ◦ | ◦ | Supervised group exercise, 30 min, 5×/week, 10 weeks | Depression, Anxiety | DASS | None |
| Naumann | 2013 | ◦ | • | ◦ | ◦ | ◦ | Individual counselling, 60 min, 1×/week, 8 weeks | • | • | ◦ | Supervised exercise, 45-60 min, 3×/week, 8 weeks | Depression | BDI | Breast cancer survivors |
| Oertel-Knochel | 2014 | ◦ | ◦ | ◦ | ◦ | • | Group cognitive training, 30 min, 3×/week, 12 weeks | • | ◦ | ◦ | Supervised exercise, 45 min, 3×/week, 4 weeks | Depression, Anxiety | BDI-II, STAI | Schizophrenia |
| Pendleton | 2010 | • | ◦ | ◦ | ◦ | ◦ | Individual CBT, 90 min, 1×/week, 16 weeks | • | ◦ | ◦ | Unsupervised exercise, 45 min, 3×/week, 16 weeks | Depression | BDI-II | Binge eating disorder |
| Rosenbaum | 2015 | ◦ | • | ◦ | ◦ | ◦ | Psychotherapy and group therapy | ◦ | • | ◦ | Supervised exercise, 30 min, 3×/week, 12 weeks | Depression, Anxiety | DASS | Post-traumatic stress disorder |
| Smeets | 2006 | • | ◦ | ◦ | ◦ | ◦ | Individual CBT, 11.5 h total, 10 weeks | • | • | ◦ | Supervised exercise, 105 min, 3×/week, 10 weeks | Depression | BDI-II | Chronic low back pain |
| Ussher | 2015 | ◦ | ◦ | ◦ | ◦ | • | Individual behavioral support, 20 min, 1×/week, 6 weeks | • | ◦ | ◦ | Supervised, moderate intensity exercise, 30 min, 2×/week, 6 weeks | Depression | EPDS | Pregnancy |
| Zedlitz | 2012 | • | ◦ | ◦ | ◦ | ◦ | Group CBT, 120 min, 2×/week, 12 weeks | • | • | ◦ | Supervised exercise, 120 min, 2×/week, 12 weeks | Depression, Anxiety | HADS | Stroke |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bourbeau, K.; Moriarty, T.; Ayanniyi, A.; Zuhl, M. The Combined Effect of Exercise and Behavioral Therapy for Depression and Anxiety: Systematic Review and Meta-Analysis. Behav. Sci. 2020, 10, 116. https://doi.org/10.3390/bs10070116
Bourbeau K, Moriarty T, Ayanniyi A, Zuhl M. The Combined Effect of Exercise and Behavioral Therapy for Depression and Anxiety: Systematic Review and Meta-Analysis. Behavioral Sciences. 2020; 10(7):116. https://doi.org/10.3390/bs10070116
Chicago/Turabian StyleBourbeau, Kelsey, Terence Moriarty, Akeisha Ayanniyi, and Micah Zuhl. 2020. "The Combined Effect of Exercise and Behavioral Therapy for Depression and Anxiety: Systematic Review and Meta-Analysis" Behavioral Sciences 10, no. 7: 116. https://doi.org/10.3390/bs10070116
APA StyleBourbeau, K., Moriarty, T., Ayanniyi, A., & Zuhl, M. (2020). The Combined Effect of Exercise and Behavioral Therapy for Depression and Anxiety: Systematic Review and Meta-Analysis. Behavioral Sciences, 10(7), 116. https://doi.org/10.3390/bs10070116