
Dynamics in Morbidity Markers and Cytological Observations Made in Urine of Schistosoma haematobium-Infected Children: Pre- and Post-Praziquantel Treatment in an Endemic Setting

 , , , ,
, , , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Study Sites
2.2. Examination of Morbidity Markers and Detection of S. haematobium Ova
2.3. Cytological Examination of Urine Deposit
2.4. Statistical Analysis
2.5. Ethical Statement
3. Results
3.1. S. haematobium Detection and Morphological Forms
3.2. Clinical Morbidity Markers Detected among S. haematobium-Infected Children
3.3. Cytological Observations Made in the Urine
3.4. Cytological Abnormalities at Baseline
3.5. Cytological Changes in the Post-Treatment Weekly Follow-Ups
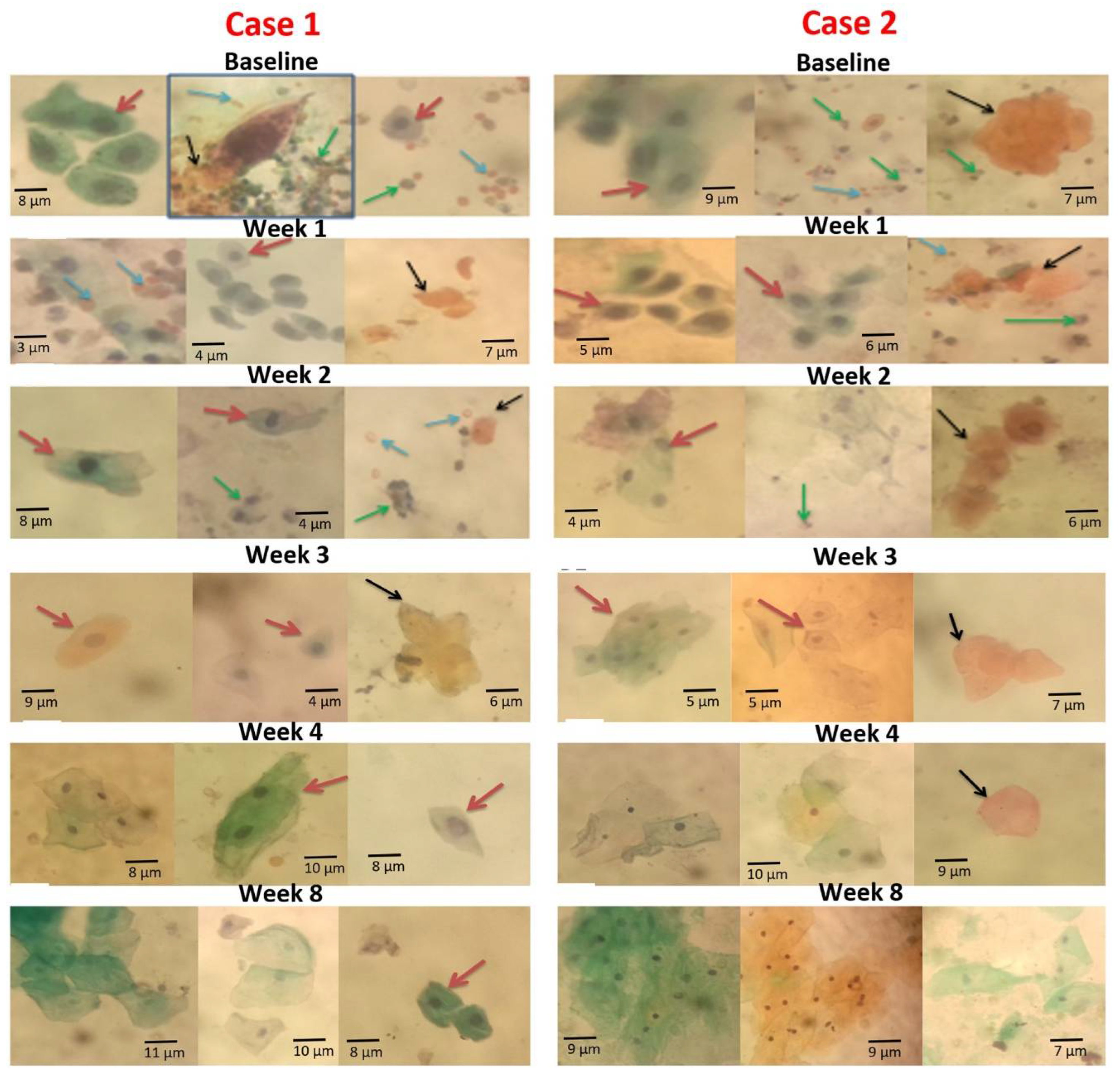
3.6. Case Representation of Observation at Baseline and Reduction in Cytological Abnormalities in the Weekly Post-Treatment Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tetteh-Quarcoo, P.B.; Akuetteh, B.K.; Owusu, I.A.; Quayson, S.E.; Attah, S.K.; Armah, R.; Afutu, E.; Afrah, A.; Addo-Osafo, K.; Smith, C.; et al. Cytological and Wet Mount Microscopic Observations Made in Urine of Schistosoma haematobium-Infected Children: Hint of the Implication in Bladder Cancer. Can. J. Infect. Dis. Med. Microbiol. 2019, 2019, 7912186. [Google Scholar] [CrossRef] [PubMed]
- Tetteh-Quarcoo, B.P.; Simon KAEric, S.D.; Marian, N.; Andrew, A.M.; Afutu, E.; Edward, T.H.; Ayeh-Kumi, P.F. Urinary Schistosomiasis in Children—Still a Concern in Part of the Ghanaian Capital City. Open J. Med. Microbiol. 2013, 3, 151–158. [Google Scholar] [CrossRef]
- Gryseels, B.; Polman, K.; Klerinx, J.; Kestens, L. Human schistosomiasis. Lancet 2006, 368, 1106–1118. [Google Scholar] [CrossRef]
- Mott, K.E.; Desjeux, P.; Moncayo, A. Parasitic diseases and urban development. Bull. WHO 1990, 68, 691–698. [Google Scholar]
- World Health Organization (W.H.O.). Schistosomiasis, Fact Sheet No. 115. February 2010. Available online: http://www.who.int/mediacentre/factsheets/fs115/en/index.html (accessed on 16 March 2019).
- Midzi, N.; Sangweme, D.; Zinyowera, S.; Mapingure, M.P.; Brouwer, K.C.; Kumar, N.; Mutapi, F.; Woelk, G.; Mduluza, T. Efficacy and side effects of Praziquantel treatment against Schistosoma haematobium infection among primary school children in Zimbabwe. Trans. R Soc. Trop. Med. Hyg. 2008, 102, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Barakat, R.; El-Morshedy, H. Efficacy of two Praziquantel treatments among primary school children in an area of high Schistosoma mansoni endemicity, Nile Delta, Egypt. Parasitology 2011, 138, 440–446. [Google Scholar] [CrossRef]
- McManus, D.P.; Loukas, A. Current Status of Vaccines for Schistosomiasis. Clin. Microbiol. 2008, 21, 225–242. [Google Scholar] [CrossRef]
- Seto EY, W.; Wong, B.K.; Lu, D.; Zhong, B. Human Schistosomiasis resistance to Praziquantel in China: Should we be worried. Am. J. Trop. Med. Hyg. 2011, 85, 74–82. [Google Scholar] [CrossRef]
- Afifi, M.A.; Asif, A.; Jiman, F.; Nabeel, H.; Al-Hussainya Mohammed, W.; Al-Rabiaa, A.A. Genetic diversity among natural populations of Schistosoma haematobium might contribute to inconsistent virulence and diverse clinical outcomes. Jmau 2016, 4, 222–227. [Google Scholar] [CrossRef]
- Tetteh-Quarcoo, P.B.; Forson, P.O.; Amponsah, S.K.; Ahenkorah, J.; Opintan, J.A.; Ocloo, J.E.Y.; Okine, E.N.; Aryee, R.; Afutu, E.; Anang, A.K.; et al. Persistent urogenital schistosomiasis and its associated morbidity in endemic communities within southern Ghana: Suspected praziquantel resistance or reinfection? Med. Sci. 2020, 8, 10. [Google Scholar] [CrossRef]
- Muscheck, M.; Abol-Enein, H.; Chew, K.; Moore, D.; VBhargava, I.I.; Ghonei, M.A. Comparison of Genetic Changes in Schistosome-Related Transitional and Squamous Bladder Cancers Using Comparative Genomic Hybridization. Carcinogen 2000, 21, 1721–1726. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Akinwale, O.P.; Oliveira, G.C.; Ajayi, M.B.; Akande, D.C.; Oyebadejo, S.; Okereke, K.C. Squamous cell abnormalities in ex-foliated cells from urine of Schistosoma haematobium infected adults in a rural fishing community in Nigeria. World Health Popul. 2008, 10, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Flezar, M.S. Urine and bladder washing cytology for detection of urothelial carcinoma: Standard test with new possibilities. Radiol. Oncol. 2010, 44, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Grossfeld, G.D.; Litwin, M.S.; Wolf, J.S.; Jr Hricak, H.; Shuler, C.L.; Agerter, D.C.; Carroll, P.R. Evaluation of asymptomatic microscopic hematuria in adults: The American Urological Association best practice policy-part II: Patient evaluation, cytology, voided markers, imaging, cystoscopy, nephrology evaluation, and follow-up. Urology 2001, 57, 604–610. [Google Scholar] [CrossRef]
- Yameny, A.A. The validity of haematuria and proteinuria by chemical reagent strip for diagnosis of Schistosoma haematobium infection. J. Biosci. Appl. Res. 2017, 3, 229–236. [Google Scholar] [CrossRef]
- Kim, J.Y.; Kim, H.J. A Comparison Between ThinPrep Monolayer and Cytospin Cytology for the Detection of Bladder Cancer. Korean, J. Urol. 2014, 55, 390–394. [Google Scholar] [CrossRef]
- Presti, J.C.; Weyrauch, H.M. Papanicolaou Examination of Urine in Diagnosis of Urinary Cancer. I. as a Test in Mass Screening. J. Urol. 1955, 73, 430–434. [Google Scholar] [CrossRef]
- Bogoch, I.I.; Andrews, J.R.; Dadzie ER, K.; Utzinger, J. Simple questionnaire and urine reagent strips compared to microscopy for the diagnosis of Schistosoma haematobium in a community in northern Ghana. Trop. Med. Int. Health 2012, 17, 1217–1221. [Google Scholar] [CrossRef]
- Stete, K.; Krauth, S.J.; Coulibaly, J.T.; Knopp, S.; Hattendorf, J.; Müller, I.; Lohourignon, L.K.; Kern, W.V.; Goran EK, N.; Utzinger, J. Dynamics of Schistosoma haematobium egg output and associated infection parameters following treatment with Praziquantel in school-aged children. Parasites Vectors 2012, 5, 298–301. [Google Scholar] [CrossRef]
- Wilkins, H.A.; Goll, P.; Marshall, C.; Moore, P. The significance of proteinuria and haematuria in Schistosoma haematobium infection. Trans. R. Soc. Trop. Med. Hyg. 1979, 73, 74–80. [Google Scholar] [CrossRef]
- Sacko, M.; Magnussen, P.; Adama, D.K.; Mamadou, S.T.; Aly, L. Impact of Schistosoma haematobium infection on urinary tract pathology, nutritional status and anaemia in school-aged children in two different endemic areas of the Niger River Basin, Mali. Acta Tropica 2011, 120, 142–150. [Google Scholar] [CrossRef] [PubMed]
- Neale, T.J.; Ojha, P.P.; Exner, M.; Poczewski, H.; Rüger, B.; Witztum, J.L.; Davis, P.; Kerjaschki, D. Proteinuria in passive Heymann nephritis is associated with lipid peroxidation and formation of adducts on type IV collagen. J. Clin. Investig. 1994, 94, 1577–1584. [Google Scholar] [CrossRef] [PubMed]
- Fu, C.; Odegaard, J.I.; Herbert, D.R.; Hsieh, M.H. A Novel Mouse Model of Schistosoma haematobium Egg-Induced Immunopathology. PLoS Pathog. 2012, 10, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Wami, W.M.; Nausch, N.; Midzi, N.; Gwisai, R.; Mduluza, T.; Woolhouse ME, J.; Mutapi, F. Comparative Assessment of Health Benefits of Praziquantel Treat. of Urogenital Schistosomiasis in Pre-school Children and Primary School Aged Children. Biomed. Reseach Int. 2016, 91, 626–631. [Google Scholar]
- Hodder, S.L.; Mahmoud, K.; Sorenso, D.M.; Weinert, R.I.; Stein, J.H. Predisposition to Urinary Tract Epithelial Metaplasia in Schistosoma haematobium Infection. Am. J. Trop. Med. Hyg. 2000, 63, 133–138. [Google Scholar] [CrossRef]
- Botelho, M.E.; Machado, J.C.; Da Costa JM, C. Schistosoma haematobium and bladder cancer. Virulence 2009, 1, 84–87. [Google Scholar] [CrossRef][Green Version]
- Der, E.M.; Quayson, S.E.; Mensah, J.E.; Tettey, Y. Tissue schistosomiasis in Accra Ghana: A retrospective histopathologic review at the Korle-bu Teaching Hospital (2004–2011). Pathol. Discov. 2015, 3, 1–20. [Google Scholar] [CrossRef]
- Slack, J.M. Metaplasia and trans-differentiation: From pure biology to the clinic. Nat. Rev. Mol. Cell Biol. 2007, 8, 369–378. [Google Scholar] [CrossRef]
- Gower, C.M.; Gabrielli, A.F.; Sacko, M.; Dembele, R.; Golan, R.; Emery, A.M.; Rollinson, D.; Webster, J.P. Population genetics of Schistosoma haematobium: Development of novel microsatellite markers and their application to schistosomiasis control in Mali. Parasitology 2011, 138, 978–994. [Google Scholar] [CrossRef]
- Khurana, S.; Dubey, M.L.; Malla, N. Association of parasitic infection and cancer. Indian J. Med. Microbiol. 2005, 23, 74–79. [Google Scholar] [CrossRef]
- Murare, H.M.; Taylor, P. Haematuria and proteinuria during Schistosoma haematobium infection: Relationship to intensity of infection and the value of chemical reagent strips for pre-and post-treatment diagnosis. Trans. R. Soc. Trop. Med. Hyg. 1987, 81, 426–430. [Google Scholar] [CrossRef]
- Papanicolaou, G.N.; Marshall, V.F. Urine sediment smears as a diagnostic procedure in cancers of the urinary tract. Science 1945, 101, 519–520. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.G. Immune Responses in Parasitic Infections: Trematodes and Cestodes; CRC Press: Boca Raton, FL, USA, 1987; pp. 49–90. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytological Abnormality | n (%) |
|---|---|
| Squamous metaplastic cells | 8 (26.7%) |
| Inflammatory cells | 21 (70.0%) |
| Hyperkeratotic cells | 14 (46.7%) |
| Red blood cells | 18 (60.0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tetteh-Quarcoo, P.B.; Ampong, A.; Dayie, N.T.K.D.; Ahenkorah, J.; Udofia, E.A.; Afutu, E.; Aryee, R.; Niriwa, B.P.; Kotey, F.C.N.; Donkor, E.S.; et al. Dynamics in Morbidity Markers and Cytological Observations Made in Urine of Schistosoma haematobium-Infected Children: Pre- and Post-Praziquantel Treatment in an Endemic Setting. Med. Sci. 2022, 10, 14. https://doi.org/10.3390/medsci10010014
Tetteh-Quarcoo PB, Ampong A, Dayie NTKD, Ahenkorah J, Udofia EA, Afutu E, Aryee R, Niriwa BP, Kotey FCN, Donkor ES, et al. Dynamics in Morbidity Markers and Cytological Observations Made in Urine of Schistosoma haematobium-Infected Children: Pre- and Post-Praziquantel Treatment in an Endemic Setting. Medical Sciences. 2022; 10(1):14. https://doi.org/10.3390/medsci10010014
Chicago/Turabian StyleTetteh-Quarcoo, Patience B., Asamoah Ampong, Nicholas T. K. D. Dayie, John Ahenkorah, Emilia A. Udofia, Emmanuel Afutu, Robert Aryee, Benjamin P. Niriwa, Fleischer C. N. Kotey, Eric S. Donkor, and et al. 2022. "Dynamics in Morbidity Markers and Cytological Observations Made in Urine of Schistosoma haematobium-Infected Children: Pre- and Post-Praziquantel Treatment in an Endemic Setting" Medical Sciences 10, no. 1: 14. https://doi.org/10.3390/medsci10010014
APA StyleTetteh-Quarcoo, P. B., Ampong, A., Dayie, N. T. K. D., Ahenkorah, J., Udofia, E. A., Afutu, E., Aryee, R., Niriwa, B. P., Kotey, F. C. N., Donkor, E. S., & Ayeh-Kumi, P. F. (2022). Dynamics in Morbidity Markers and Cytological Observations Made in Urine of Schistosoma haematobium-Infected Children: Pre- and Post-Praziquantel Treatment in an Endemic Setting. Medical Sciences, 10(1), 14. https://doi.org/10.3390/medsci10010014