
Treatment of Equine Tarsus Long Medial Collateral Ligament Desmitis with Allogenic Synovial Membrane Mesenchymal Stem/Stromal Cells Enhanced by Umbilical Cord Mesenchymal Stem/Stromal Cell-Derived Conditioned Medium: Proof of Concept

 ,
,  , ,
, ,  , , , , ,
, , , , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethics and Regulation
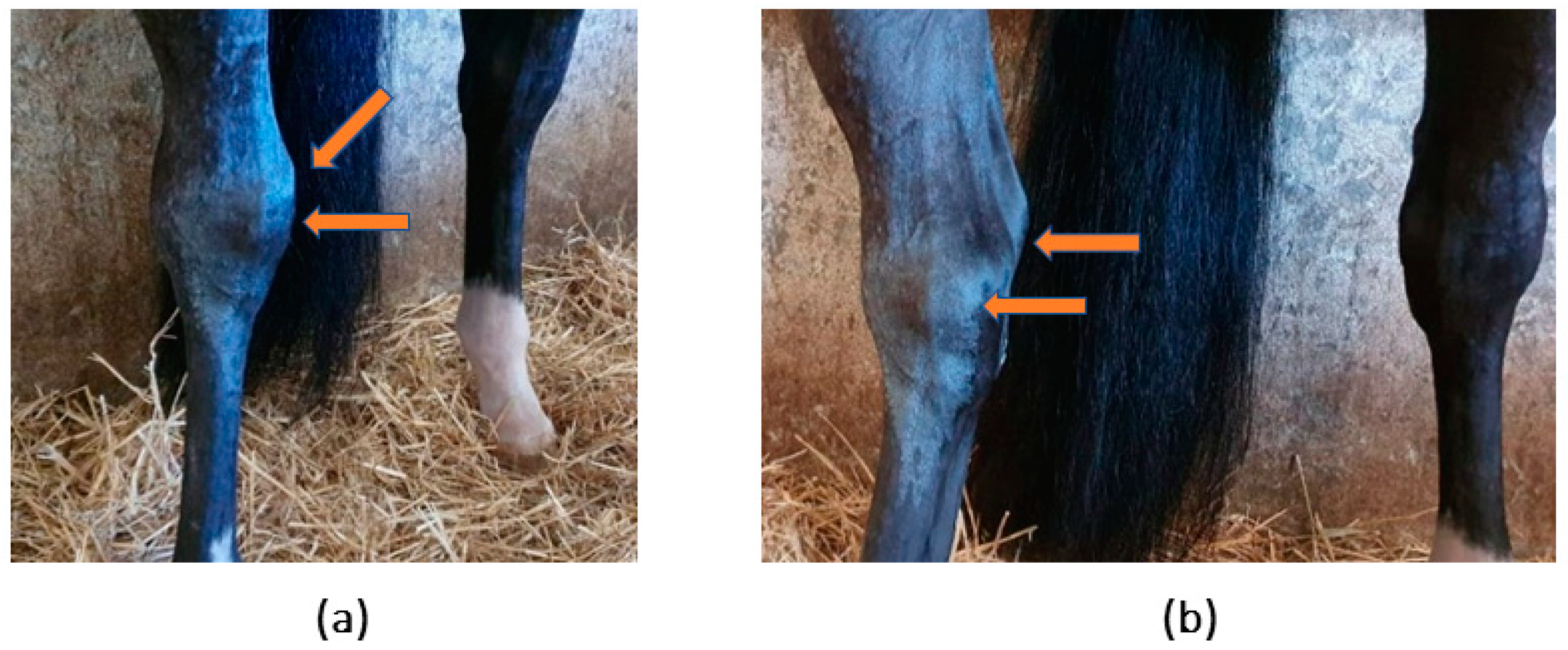
2.2. Patient Identification and Clinical Evaluation
2.3. Complementary Diagnostic Exams
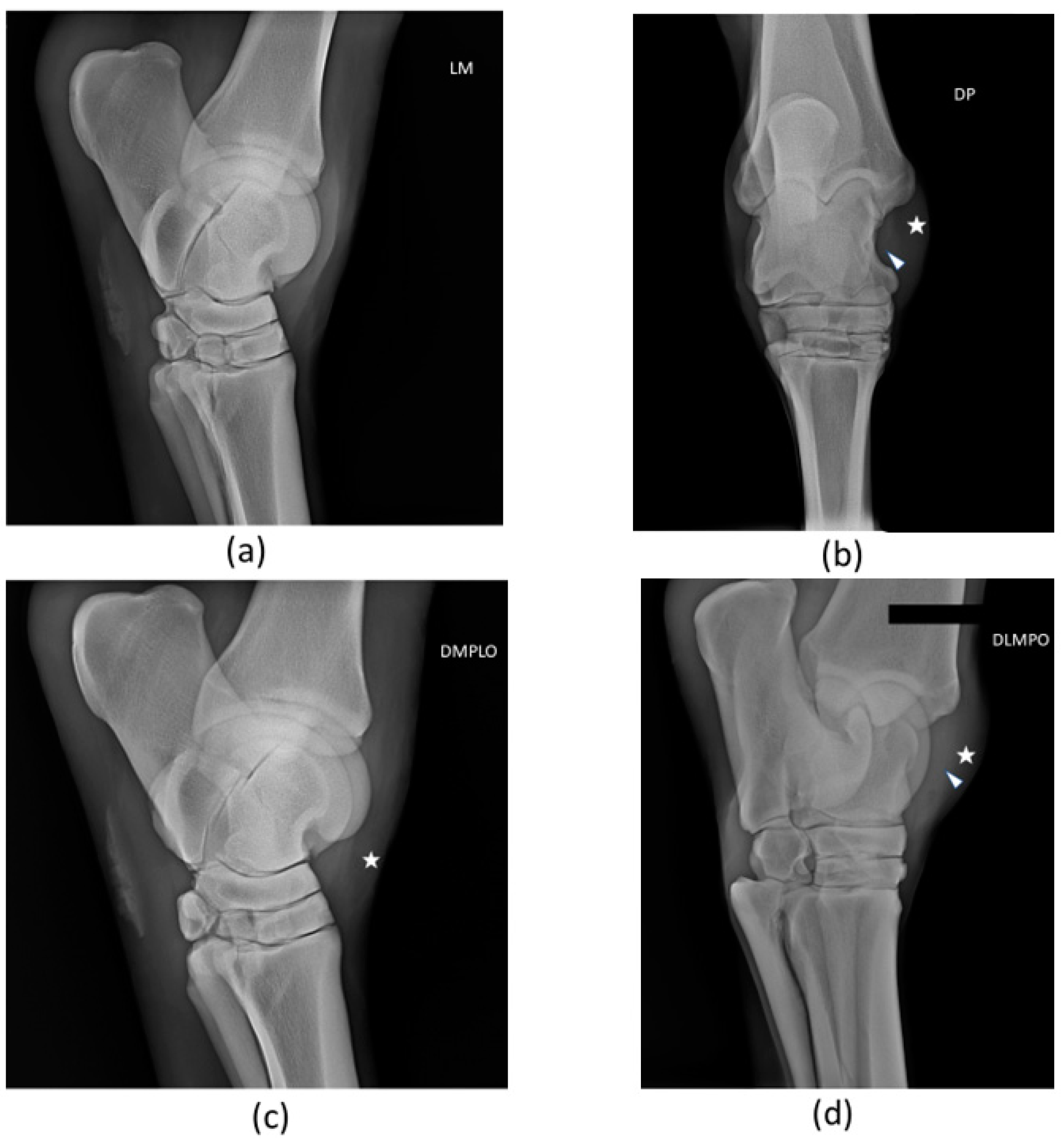
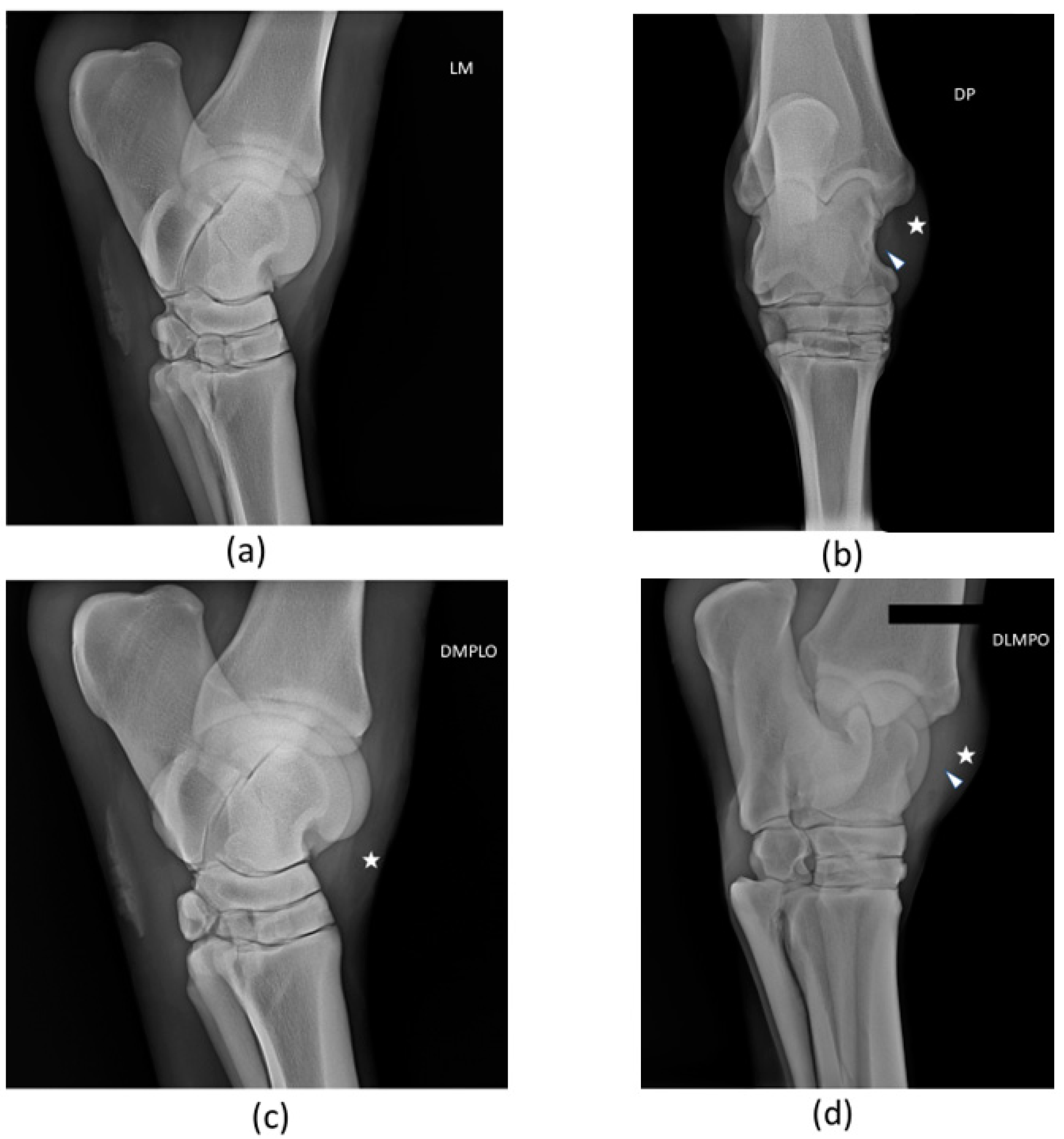
2.3.1. Radiological Examination
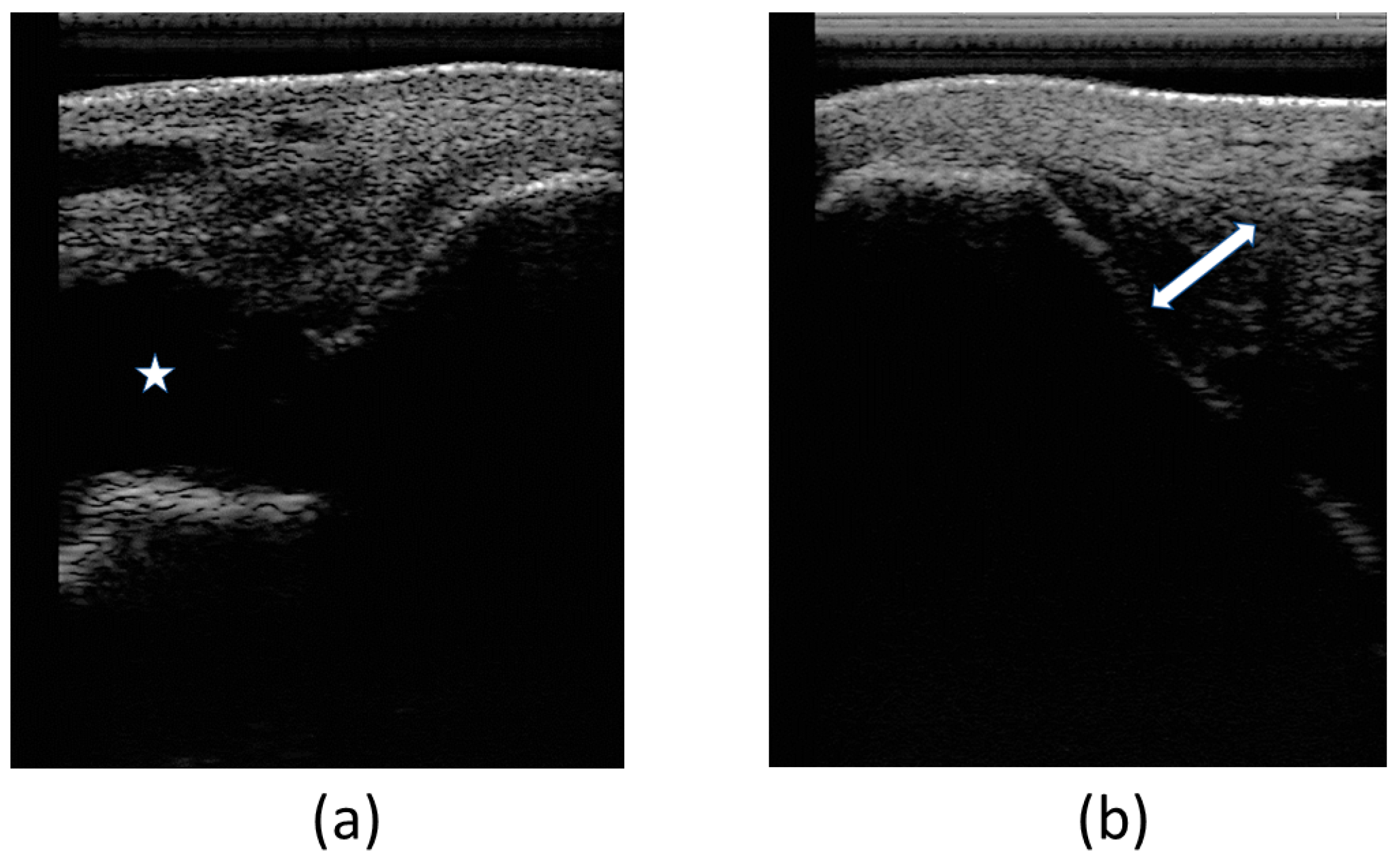
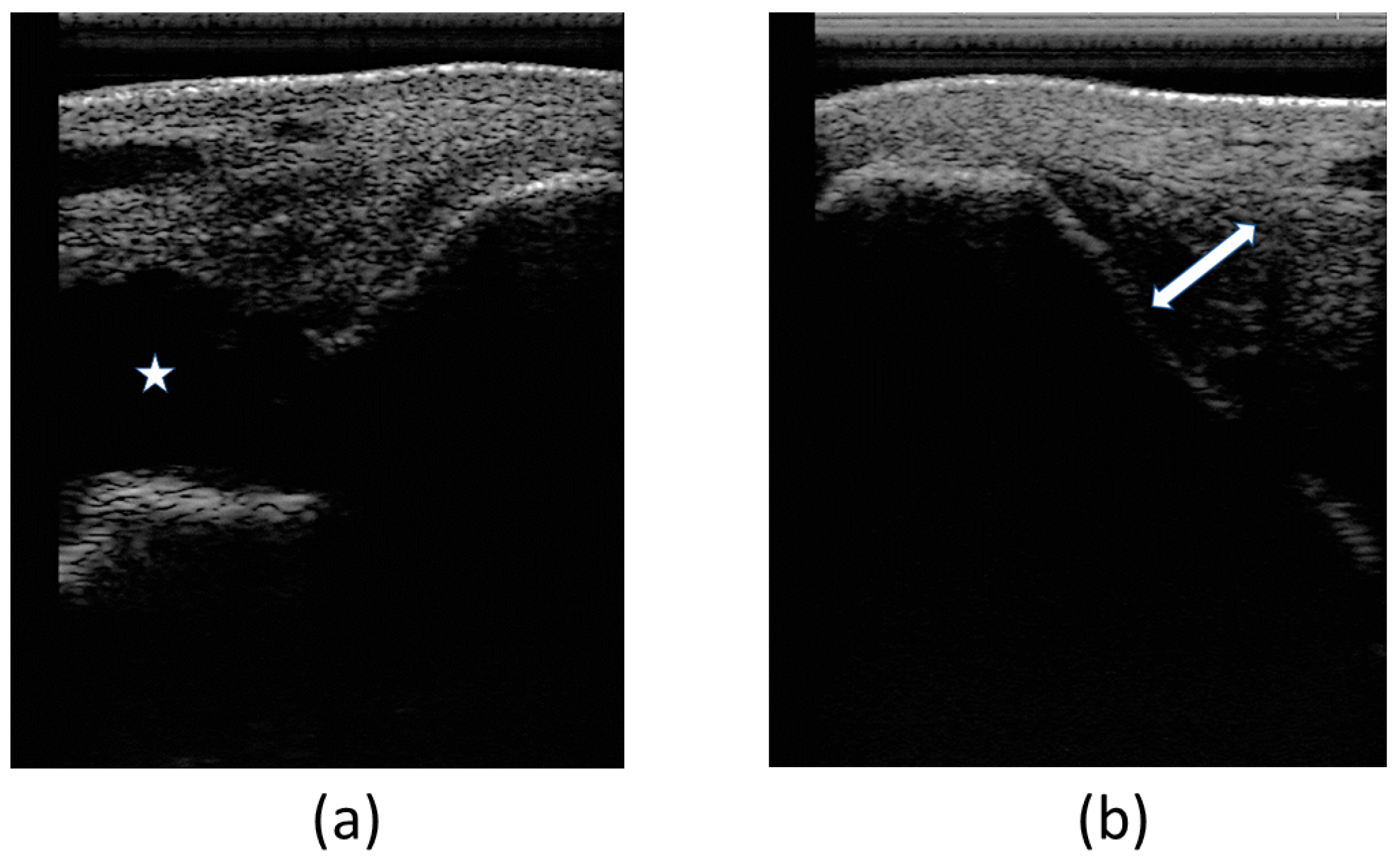
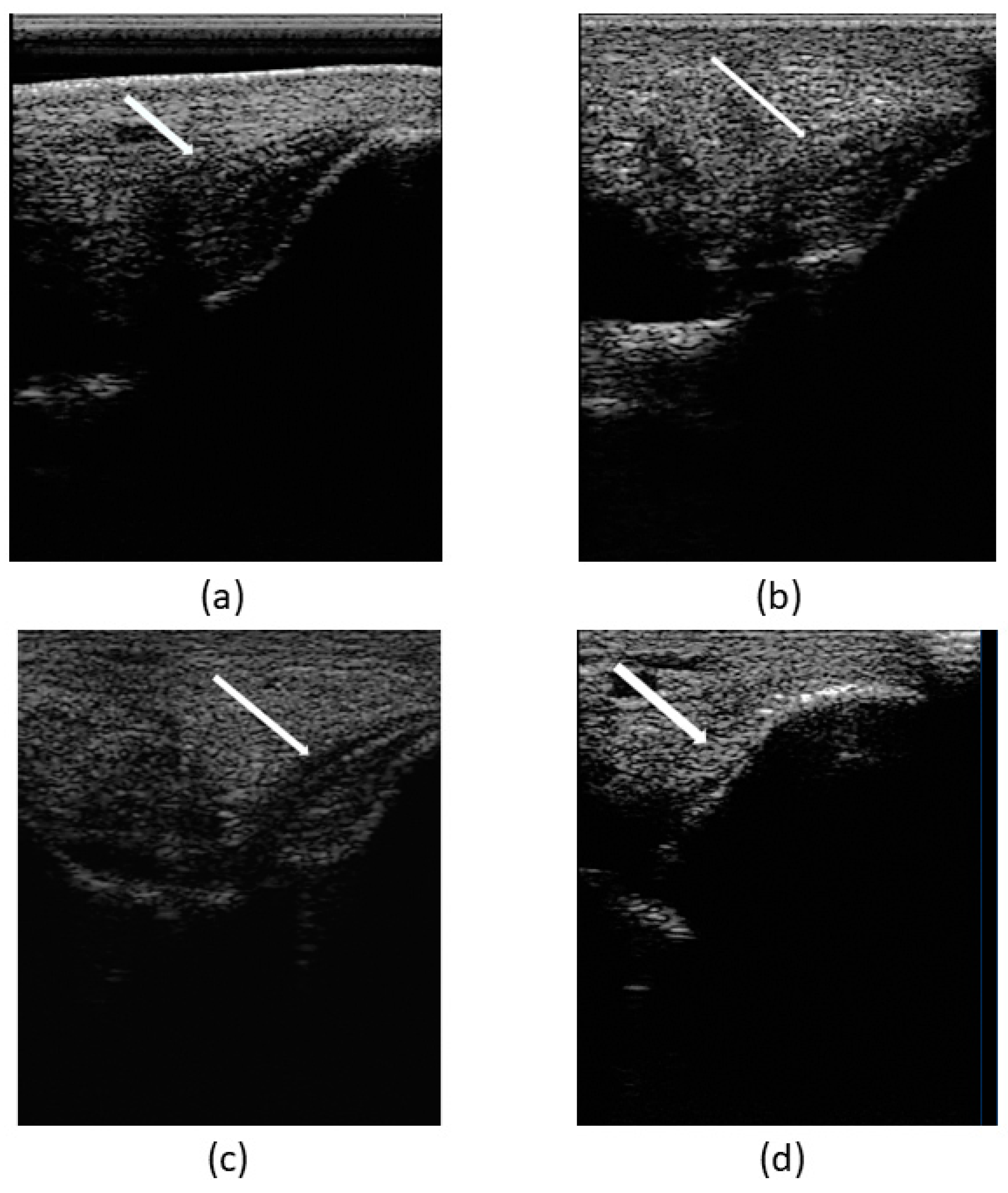
2.3.2. Ultrasound Examination
2.4. Donor Selection and SM Collection
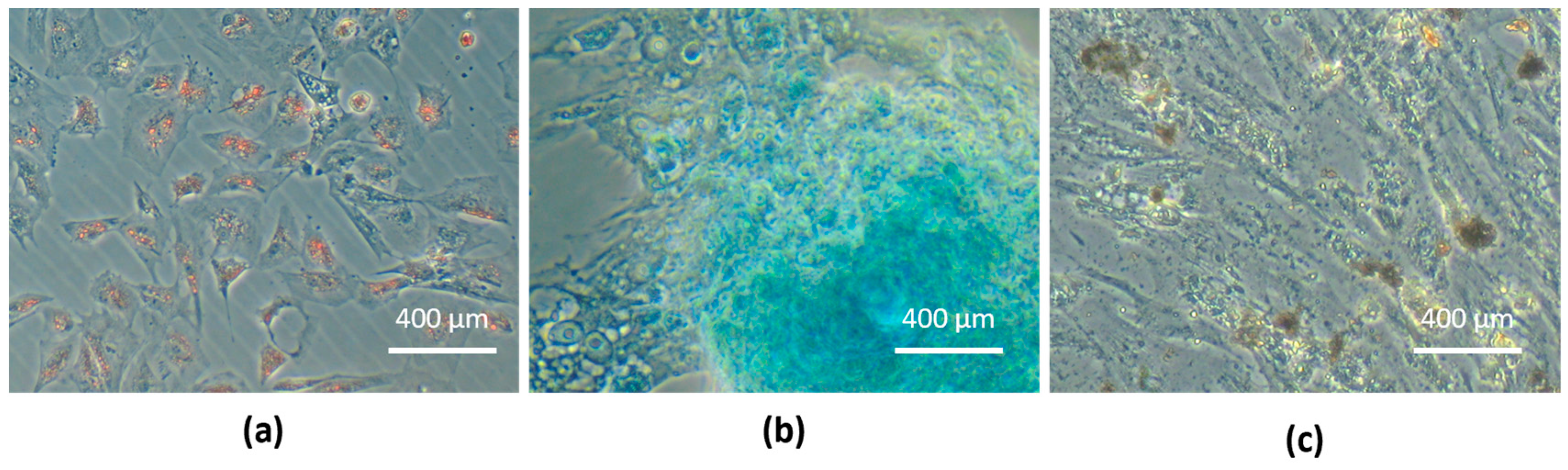
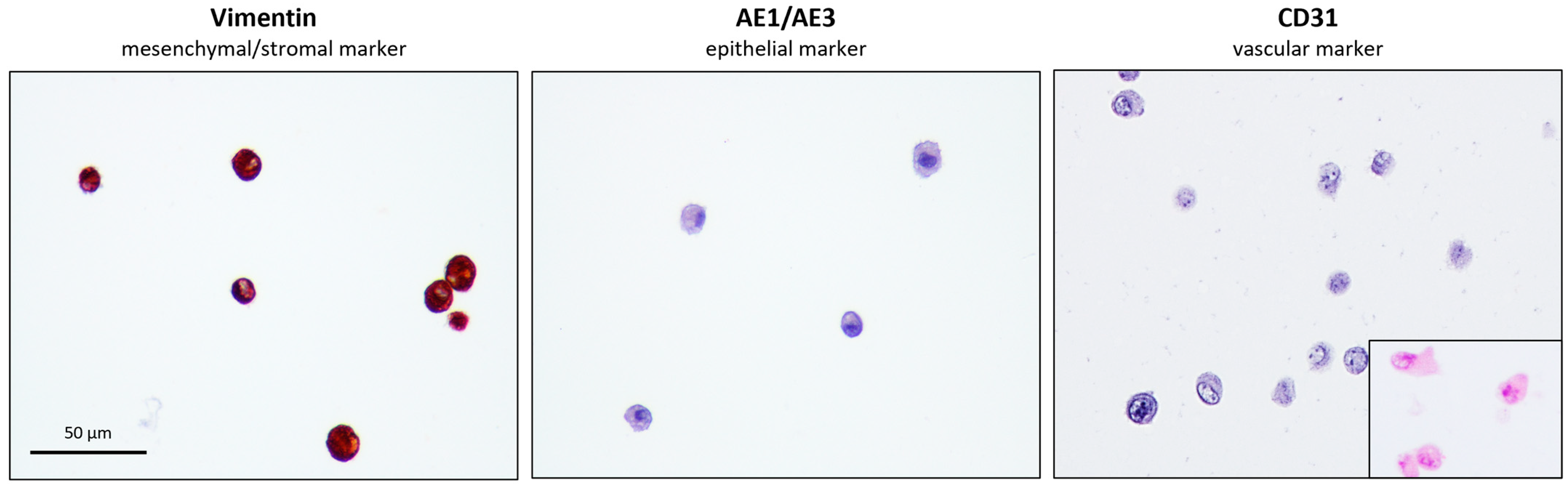
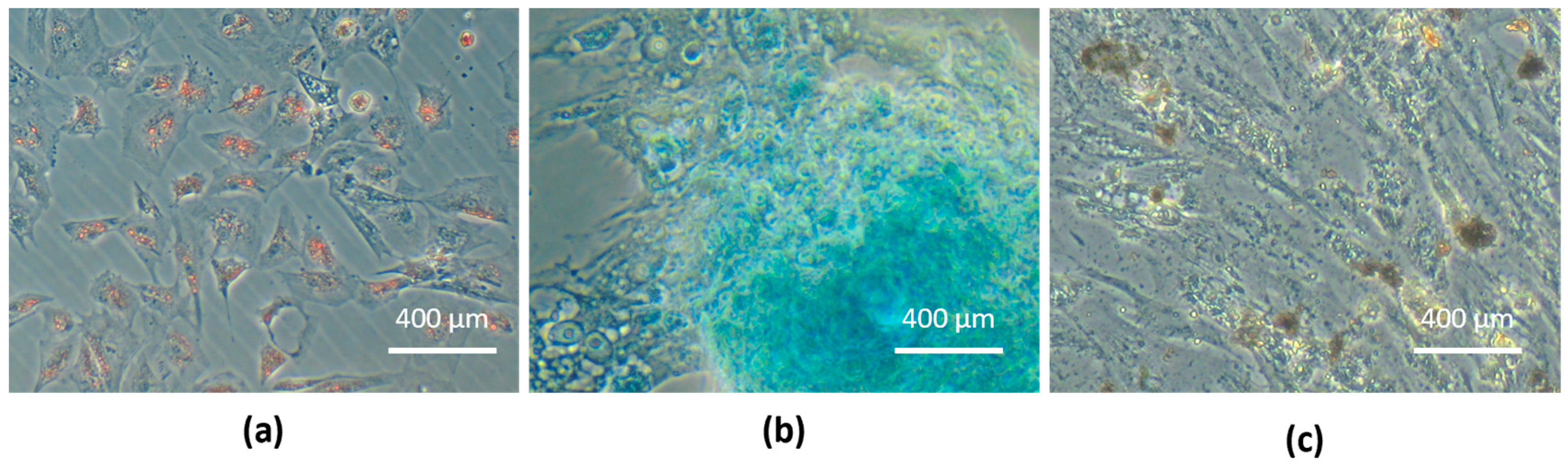
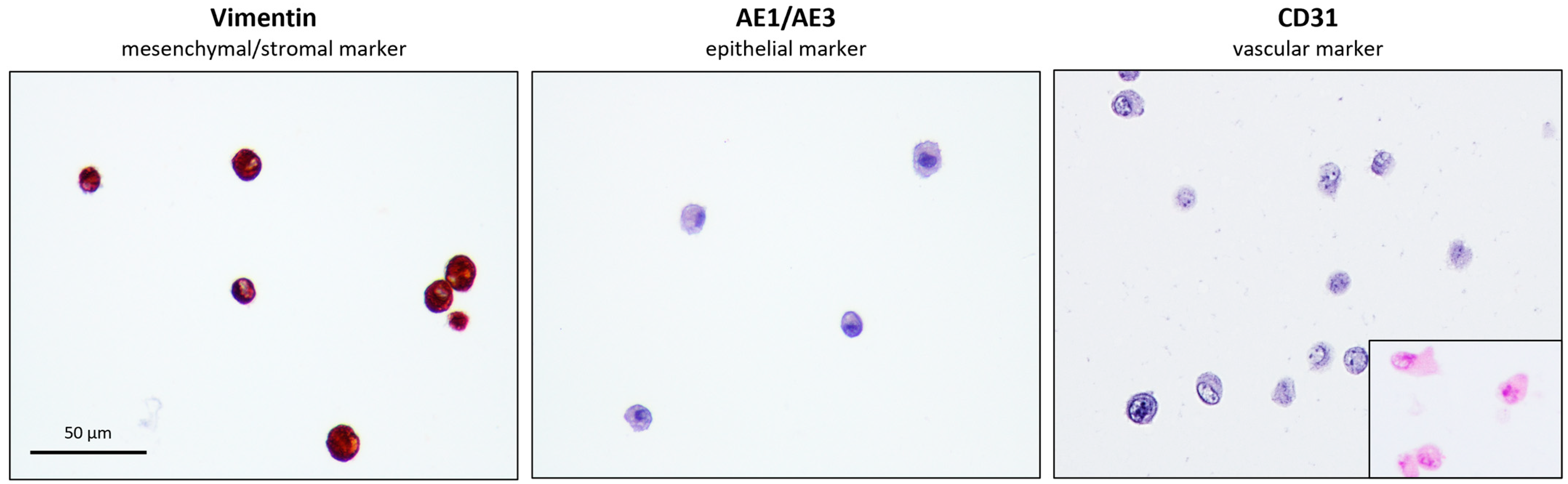
2.5. Equine SM-MSCs’ Isolation, Culture, and Characterization
2.6. Equine UC-MSCs’ Isolation, Culture, and Characterization
2.7. Secretome—Conditioned Medium Preparation and Analysis
2.8. Equine SM-MSCs + eUC-MSC CM Solution Preparation
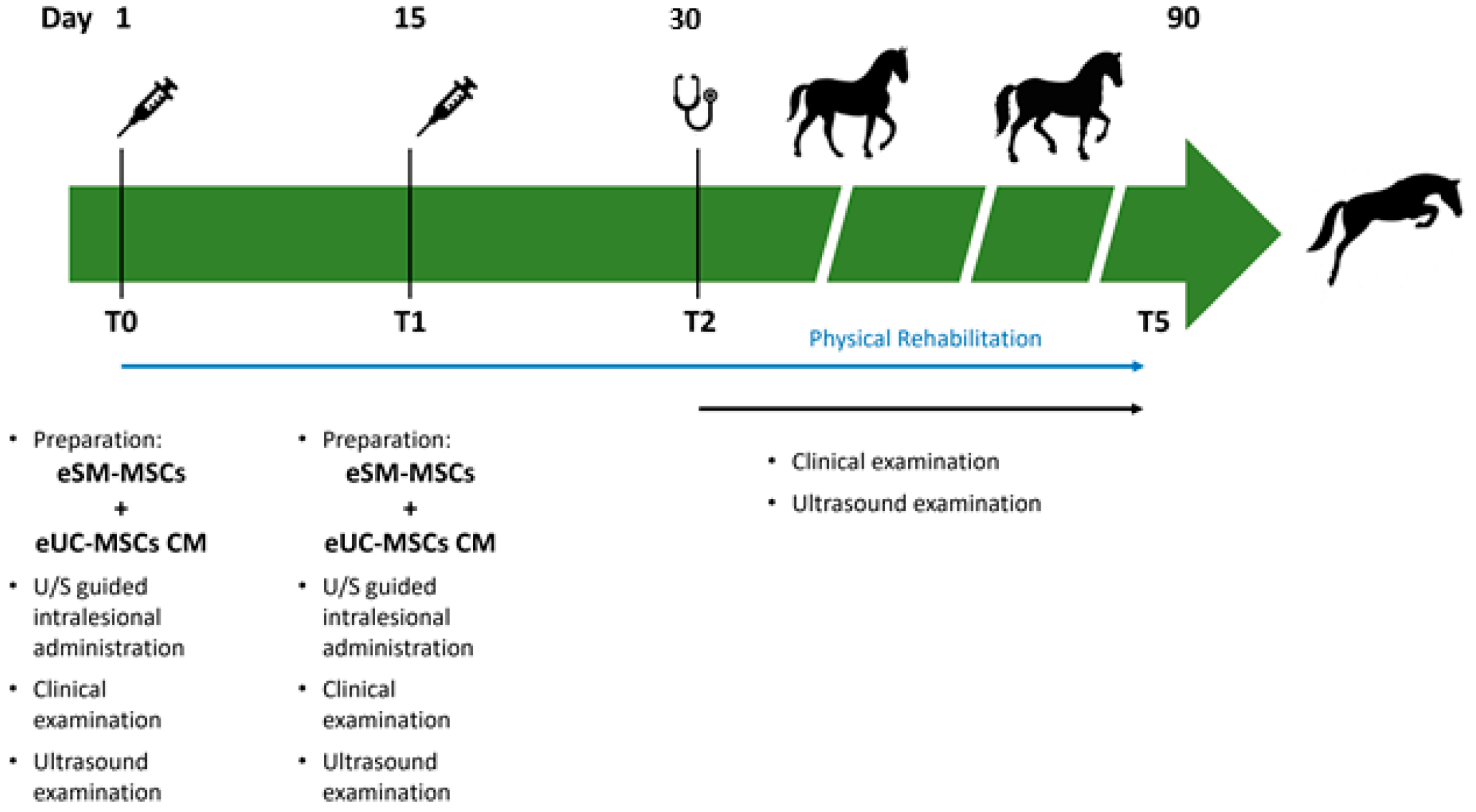
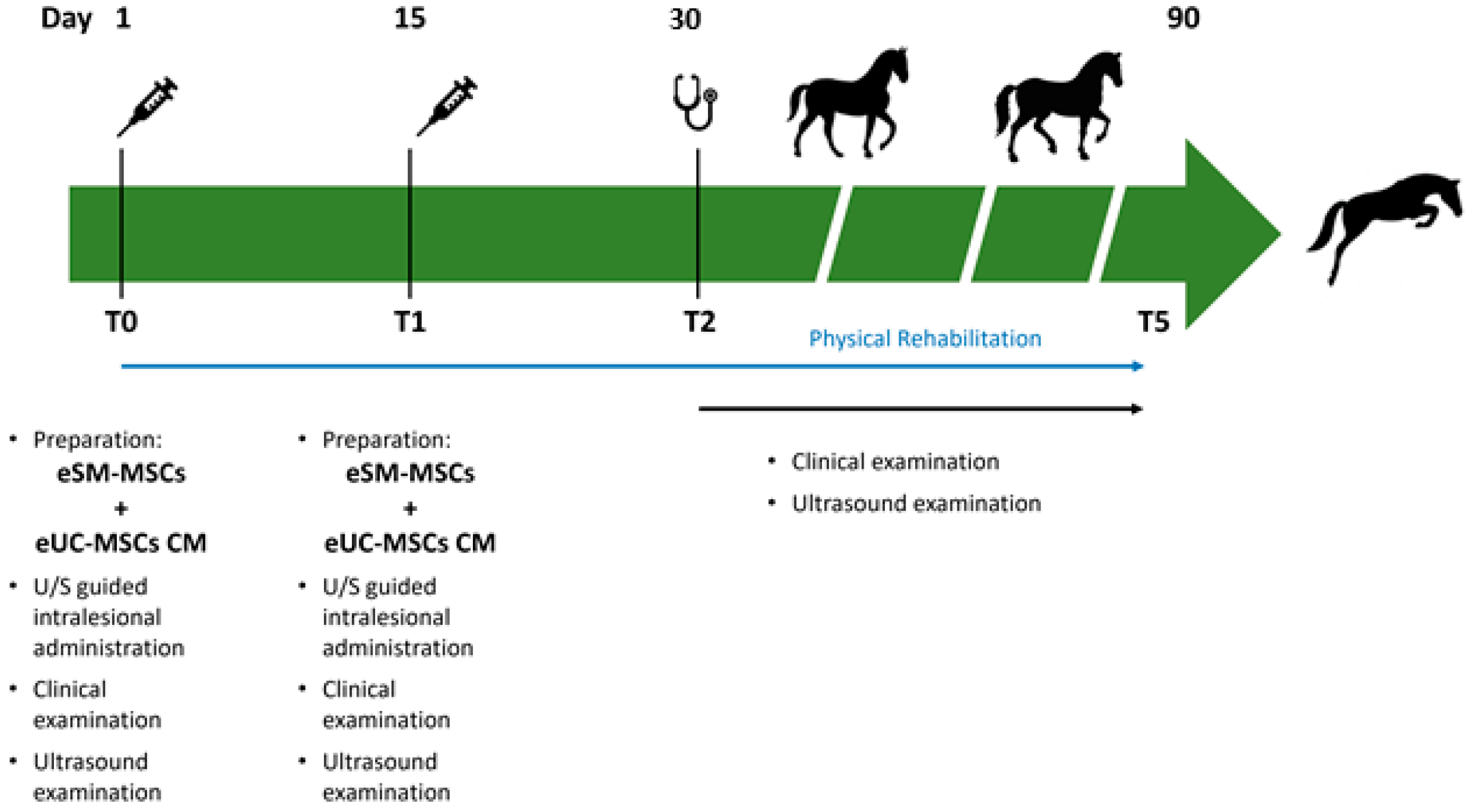
2.9. Treatment Protocol
Intralesional eSM-MSCs + eUC-MSCs CM Administration
2.10. Post-Treatment Monitoring—Clinical Evaluations
3. Results
3.1. Clinical Evaluation
3.2. Complementary Diagnostic Examinations
3.2.1. Radiological Examination
3.2.2. Ultrasound Examination
3.3. MSCs Isolation and Characterization
3.4. Secretome: Conditioned Medium Analysis
3.5. Treatment Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| 2D | Bidimensional |
| 3D | Tridimensional |
| AAEP | American Association of Equine Practitioners |
| BM | MSC bone marrow multipotent mesenchymal stromal cells |
| CL | Collateral ligament |
| CM | Conditioned medium |
| cm2 | Square centimeter |
| d | Days |
| DLPMO | Oblique dorsolateral-plantaromedial |
| DMEM | Dulbecco’s modified eagle medium |
| DMPLO | Oblique dorsomedial-plantarolateral |
| DMSO | Dimethylsulphoxide |
| DP | Dorso plantar |
| DPBS | Dulbecco′s phosphate-buffered saline |
| eSM | MSCs equine synovial membrane-derived multipotent mesenchymal stromal cells |
| eUC | MSCs equine umbilical cord-stroma-derived mesenchymal stem cell |
| EV | Extracellular vesicles |
| FBS | Fetal bovine serum |
| FGF-2 | Basic fibroblast growth factor |
| G-CSF | Granulocyte colony stimulating factor |
| GM-CSF | Granulocyte-macrophage colony stimulating factor |
| IL | Interleukins |
| IL-1Ra | Interleukin one receptor antagonist |
| IRAP | Interleukin receptor antagonist protein |
| ISCT | International Society for Cellular Therapy |
| IV | Endovenous |
| KC/GRO | Human growth-regulated oncogene/keratinocyte chemoattractant |
| Kg | Kilogram |
| Kv | Kilovolts |
| LLCL | Long lateral collateral ligament |
| LM | Lateromedial |
| LMCL | Long medial collateral ligament |
| mA | Milliamperes |
| MCB | Master cell banks |
| MCP-1 | Monocyte chemoattractant Protein-1 |
| mg | Milligram |
| MHz | Megahertz |
| min | Minutes |
| mL | Milliliter |
| MMP-3 | Matrix metaloproteinase-3 |
| MSCs | Mesenchymal stem cells |
| OA | Osteoarthritis |
| ORBEA | Organismo Responsável pelo Bem-estar Animal |
| P | Passage |
| PBS | Phosphate-buffered saline |
| pg | Picograms |
| PRP | Platelet-rich plasma |
| rpm | Rotations per minute |
| SEM | Standard error mean |
| SLCL | Short lateral collateral ligament |
| SMCL | Short medial collateral ligament |
| TGF-β | Transforming growth factor-β |
| TNF-α | Tumor necrosis factor-α |
| U/S | Ultrasound |
| VEGF-R1 | Vascular endothelial growth factor |
References
- Ortved, K.F. Regenerative medicine and rehabilitation for tendinous and ligamentous injuries in sport horses. Vet. Clin. Equine Pract. 2018, 34, 359–373. [Google Scholar] [CrossRef] [PubMed]
- Duddy, H.; Schoonover, M.; Hague, B. Outcome following local injection of a liquid amnion allograft for treatment of equine tendonitis or desmitis—100 cases. BMC Vet. Res. 2022, 18, 391. [Google Scholar] [CrossRef] [PubMed]
- Bramlage, L.R. Traumatic and developmental lesions of the tarsus. Proc. Am. Assoc. Equine Pract 2006, 52, 1–4. [Google Scholar]
- Stashak, T.S. Adams’ Lameness in Horses; Verlag M. & H. Schaper: Alfeld, Germany, 2008. [Google Scholar]
- Lamb, L.; Zubrod, C.; Hague, B.; Brakenhoff, J.; Major, M. Clinical outcome of collateral ligament injuries of the tarsus. Can. Vet. J. 2012, 53, 518. [Google Scholar] [PubMed]
- Tokateloff, N.; Carmalt, J.; Manning, S. Trauma resulting in hemarthrosis and long medial collateral ligament desmitis of the tarsocrural joint in a horse. Can. Vet. J. 2011, 52, 519. [Google Scholar]
- Dik, K.J. Ultrasonography of the equine tarsus. Vet. Radiol. Ultrasound 1993, 34, 36–43. [Google Scholar] [CrossRef]
- Bell, C.; Torske, K.; Lobb, B. Collateral ligament reconstruction in two horses following traumatic avulsion fracture using a knotless suture anchor construct. Equine Vet. Educ. 2018, 30, 360–366. [Google Scholar] [CrossRef]
- Fraschetto, C.; Dancot, M.; Vandersmissen, M.; Denoix, J.-M.; Coudry, V. Conservative management of equine tarsal collateral ligament injuries may allow return to normal performance. J. Am. Vet. Med. Assoc. 2023, 261, 995–1003. [Google Scholar] [CrossRef]
- Bogatcheva, N.; Coleman, M. Conditioned medium of mesenchymal stromal cells: A new class of therapeutics. Biochemistry 2019, 84, 1375–1389. [Google Scholar] [CrossRef]
- Harrell, C.R.; Fellabaum, C.; Jovicic, N.; Djonov, V.; Arsenijevic, N.; Volarevic, V. Molecular mechanisms responsible for therapeutic potential of mesenchymal stem cell-derived secretome. Cells 2019, 8, 467. [Google Scholar] [CrossRef]
- Maguire, G. Stem cell therapy without the cells. Commun. Integr. Biol. 2013, 6, e26631. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Jiang, J.; Gu, Z.; Zhang, J.; Chen, Y.; Liu, X. Mesenchymal stromal cell therapies: Immunomodulatory properties and clinical progress. Stem Cell Res. Ther. 2020, 11, 345. [Google Scholar] [CrossRef]
- Dominici, M.; Le Blanc, K.; Mueller, I.; Slaper-Cortenbach, I.; Marini, F.; Krause, D.; Deans, R.; Keating, A.; Prockop, D.; Horwitz, E. Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 2006, 8, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Prockop, D.J.; Oh, J.Y. Medical therapies with adult stem/progenitor cells (MSCs): A backward journey from dramatic results in vivo to the cellular and molecular explanations. J. Cell. Biochem. 2012, 113, 1460–1469. [Google Scholar] [CrossRef] [PubMed]
- Caplan, A.I. Mesenchymal stem cells: Time to change the name! Stem Cells Transl. Med. 2017, 6, 1445–1451. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.M.; Kalamegam, G.; Pushparaj, P.N.; Matta, C.; Memic, A.; Khademhosseini, A.; Mobasheri, R.; Poletti, F.L.; Hoyland, J.A.; Mobasheri, A. Mesenchymal stem cells in regenerative medicine: Focus on articular cartilage and intervertebral disc regeneration. Methods 2016, 99, 69–80. [Google Scholar] [CrossRef]
- Scala, M.; Lenarduzzi, S.; Spagnolo, F.; Trapasso, M.; Ottonello, C.; Muraglia, A.; Barla, A.; Strada, P. Regenerative medicine for the treatment of Teno-desmic injuries of the equine. A series of 150 horses treated with platelet-derived growth factors. In Vivo 2014, 28, 1119–1123. [Google Scholar]
- Mocchi, M.; Dotti, S.; Del Bue, M.; Villa, R.; Bari, E.; Perteghella, S.; Torre, M.L.; Grolli, S. Veterinary regenerative medicine for musculoskeletal disorders: Can mesenchymal stem/stromal cells and their secretome be the new frontier? Cells 2020, 9, 1453. [Google Scholar] [CrossRef]
- Madrigal, M.; Rao, K.S.; Riordan, N.H. A review of therapeutic effects of mesenchymal stem cell secretions and induction of secretory modification by different culture methods. J. Transl. Med. 2014, 12, 260. [Google Scholar] [CrossRef]
- Al Naem, M.; Bourebaba, L.; Kucharczyk, K.; Röcken, M.; Marycz, K. Therapeutic mesenchymal stromal stem cells: Isolation, characterization and role in equine regenerative medicine and metabolic disorders. Stem Cell Rev. Rep. 2020, 16, 301–322. [Google Scholar] [CrossRef]
- Han, C.; Sun, X.; Liu, L.; Jiang, H.; Shen, Y.; Xu, X.; Li, J.; Zhang, G.; Huang, J.; Lin, Z. Exosomes and their therapeutic potentials of stem cells. Stem Cells Int. 2016, 2016, 7653489. [Google Scholar] [CrossRef] [PubMed]
- Pawitan, J.A. Prospect of stem cell conditioned medium in regenerative medicine. BioMed Res. Int. 2014, 2014, 65849. [Google Scholar] [CrossRef]
- Li, J.J.; Hosseini-Beheshti, E.; Grau, G.E.; Zreiqat, H.; Little, C.B. Stem cell-derived extracellular vesicles for treating joint injury and osteoarthritis. Nanomaterials 2019, 9, 261. [Google Scholar] [CrossRef] [PubMed]
- Sun, D.Z.; Abelson, B.; Babbar, P.; Damaser, M.S. Harnessing the mesenchymal stem cell secretome for regenerative urology. Nat. Rev. Urol. 2019, 16, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Raik, S.; Kumar, A.; Bhattacharyya, S. Insights into cell-free therapeutic approach: Role of stem cell “soup-ernatant”. Biotechnol. Appl. Biochem. 2018, 65, 104–118. [Google Scholar] [CrossRef]
- Markov, A.; Thangavelu, L.; Aravindhan, S.; Zekiy, A.O.; Jarahian, M.; Chartrand, M.S.; Pathak, Y.; Marofi, F.; Shamlou, S.; Hassanzadeh, A. Mesenchymal stem/stromal cells as a valuable source for the treatment of immune-mediated disorders. Stem Cell Res. Ther. 2021, 12, 192. [Google Scholar] [CrossRef]
- Leal Reis, I.; Lopes, B.; Sousa, P.; Sousa, A.C.; Branquinho, M.; Caseiro, A.R.; Pedrosa, S.S.; Rêma, A.; Oliveira, C.; Porto, B. Allogenic Synovia-Derived Mesenchymal Stem Cells for Treatment of Equine Tendinopathies and Desmopathies—Proof of Concept. Animals 2023, 13, 1312. [Google Scholar] [CrossRef]
- Bami, M.; Sarlikiotis, T.; Milonaki, M.; Vikentiou, M.; Konsta, E.; Kapsimali, V.; Pappa, V.; Koulalis, D.; Johnson, E.O.; Soucacos, P.N. Superiority of synovial membrane mesenchymal stem cells in chondrogenesis, osteogenesis, myogenesis and tenogenesis in a rabbit model. Injury 2020, 51, 2855–2865. [Google Scholar] [CrossRef]
- De Bari, C.; Dell’Accio, F.; Tylzanowski, P.; Luyten, F.P. Multipotent mesenchymal stem cells from adult human synovial membrane. Arthritis Rheum. 2001, 44, 1928–1942. [Google Scholar] [CrossRef]
- Yea, J.-H.; Kim, Y.; Jo, C.H. Comparison of mesenchymal stem cells from bone marrow, umbilical cord blood, and umbilical cord tissue in regeneration of a full-thickness tendon defect in vitro and in vivo. Biochem. Biophys. Rep. 2023, 34, 101486. [Google Scholar] [CrossRef]
- Partan, R.U.; Putra, K.M.; Kusuma, N.F.; Darma, S.; Reagan, M.; Muthia, P.; Radiandina, A.S.; Saleh, M.I.; Salim, E.M. Umbilical Cord Mesenchymal Stem Cell Secretome Improves Clinical Outcomes and Changes Biomarkers in Knee Osteoarthritis. J. Clin. Med. 2023, 12, 7138. [Google Scholar] [CrossRef] [PubMed]
- Chouw, A.; Sartika, C.R.; Milanda, T.; Faried, A. Interleukins profiling in umbilical cord mesenchymal stem cell-derived secretome. Stem Cells Cloning Adv. Appl. 2022, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- AAEP Horse Show Committee. Guide to Veterinary Services for Horse Shows, 7th ed.; American Association of Equine Practitioners: Lexington, KY, USA, 1999. [Google Scholar]
- Thomopoulos, S.; Parks, W.C.; Rifkin, D.B.; Derwin, K.A. Mechanisms of tendon injury and repair. J. Orthop. Res. 2015, 33, 832–839. [Google Scholar] [CrossRef] [PubMed]
- Schils, S.; Turner, T. Review of early mobilization of muscle, tendon, and ligament after injury in equine rehabilitation. In Proceedings of the 56th Annual Convention of the American Association of Equine Practitioners, Baltimore, MD, USA, 4–8 December 2010; pp. 374–380. [Google Scholar]
- Kaneps, A.J. Practical rehabilitation and physical therapy for the general equine practitioner. Vet. Clin. Equine Pract. 2016, 32, 167–180. [Google Scholar] [CrossRef]
- Davidson, E.J. Controlled exercise in equine rehabilitation. Vet. Clin. Equine Pract. 2016, 32, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Sherlock, C.; Eggleston, R.; Peroni, J.; Parks, A. Desmitis of the medial tarsal collateral ligament in 7 horses. Equine Vet. Educ. 2012, 24, 72–80. [Google Scholar] [CrossRef]
- Fan, J.; Varshney, R.R.; Ren, L.; Cai, D.; Wang, D.-A. Synovium-derived mesenchymal stem cells: A new cell source for musculoskeletal regeneration. Tissue Eng. Part B Rev. 2009, 15, 75–86. [Google Scholar] [CrossRef] [PubMed]
- Murata, D.; Miyakoshi, D.; Hatazoe, T.; Miura, N.; Tokunaga, S.; Fujiki, M.; Nakayama, K.; Misumi, K. Multipotency of equine mesenchymal stem cells derived from synovial fluid. Vet. J. 2014, 202, 53–61. [Google Scholar] [CrossRef]
- Nagamura-Inoue, T.; He, H. Umbilical cord-derived mesenchymal stem cells: Their advantages and potential clinical utility. World J. Stem Cells 2014, 6, 195. [Google Scholar] [CrossRef]
- Zhang, Y.-J.; Chen, X.; Li, G.; Chan, K.-M.; Heng, B.C.; Yin, Z.; Ouyang, H.-W. Concise review: Stem cell fate guided by bioactive molecules for tendon regeneration. Stem Cells Transl. Med. 2018, 7, 404–414. [Google Scholar] [CrossRef]
- Shiomi, A.; Usui, T.; Mimori, T. GM-CSF as a therapeutic target in autoimmune diseases. Inflamm. Regen. 2016, 36, 8. [Google Scholar] [CrossRef] [PubMed]
- Wright, C.R.; Ward, A.C.; Russell, A.P. Granulocyte colony-stimulating factor and its potential application for skeletal muscle repair and regeneration. Mediat. Inflamm. 2017, 2017, 7517350. [Google Scholar] [CrossRef] [PubMed]
- Paredes, J.; Marvin, J.C.; Vaughn, B.; Andarawis-Puri, N. Innate tissue properties drive improved tendon healing in MRL/MpJ and harness cues that enhance behavior of canonical healing cells. FASEB J. 2020, 34, 8341–8356. [Google Scholar] [CrossRef] [PubMed]
- Al-Sadi, O.; Schulze-Tanzil, G.; Kohl, B.; Lohan, A.; Lemke, M.; Ertel, W.; John, T. Tenocytes, pro-inflammatory cytokines and leukocytes: A relationship? Muscles Ligaments Tendons J. 2011, 1, 68. [Google Scholar]
- Abumaree, M.; Al Jumah, M.; Pace, R.A.; Kalionis, B. Immunosuppressive properties of mesenchymal stem cells. Stem Cell Rev. Rep. 2012, 8, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Hofer, H.R.; Tuan, R.S. Secreted trophic factors of mesenchymal stem cells support neurovascular and musculoskeletal therapies. Stem Cell Res. Ther. 2016, 7, 131. [Google Scholar] [CrossRef] [PubMed]
- Galun, E.; Rose-John, S. The regenerative activity of interleukin-6. Tissue-Prot. Cytokines Methods Protoc. 2013, 59–77. [Google Scholar] [CrossRef]
- Hirota, H.; Kiyama, H.; Kishimoto, T.; Taga, T. Accelerated Nerve Regeneration in Mice by upregulated expression of interleukin (IL) 6 and IL-6 receptor after trauma. J. Exp. Med. 1996, 183, 2627–2634. [Google Scholar] [CrossRef]
- Ackermann, P.W.; Domeij-Arverud, E.; Leclerc, P.; Amoudrouz, P.; Nader, G. Anti-inflammatory cytokine profile in early human tendon repair. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 1801–1806. [Google Scholar] [CrossRef]
- Chen, S.; Deng, G.; Li, K.; Zheng, H.; Wang, G.; Yu, B.; Zhang, K. Interleukin-6 promotes proliferation but inhibits tenogenic differentiation via the Janus kinase/signal transducers and activators of transcription 3 (JAK/STAT3) pathway in tendon-derived stem cells. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2018, 24, 1567. [Google Scholar] [CrossRef]
- Lin, T.W.; Cardenas, L.; Glaser, D.L.; Soslowsky, L.J. Tendon healing in interleukin-4 and interleukin-6 knockout mice. J. Biomech. 2006, 39, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Andersen, M.B.; Pingel, J.; Kjær, M.; Langberg, H. Interleukin-6: A growth factor stimulating collagen synthesis in human tendon. J. Appl. Physiol. 2011, 110, 1549–1554. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-O.; Sim, J.A.; Choi, J.U.; Lee, B.K.; Park, H.G. The effect of interleukin-8 in the early stage after anterior cruciate ligament reconstruction with remnant preservation. Knee Surg. Relat. Res. 2020, 32, 5. [Google Scholar] [CrossRef] [PubMed]
- Ohls, R.K.; Maheshwari, A. Hematology, Immunology and Infectious Disease: Neonatology Questions and Controversies: Expert Consult-Online and Print; Elsevier Health Sciences: London, UK, 2012. [Google Scholar]
- Amable, P.R.; Teixeira, M.V.T.; Carias, R.B.V.; Granjeiro, J.M.; Borojevic, R. Protein synthesis and secretion in human mesenchymal cells derived from bone marrow, adipose tissue and Wharton’s jelly. Stem Cell Res. Ther. 2014, 5, 53. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Score | Clinical Implication |
|---|---|---|
| AAEP Grading | 0 | No Lameness |
| 1 | Lameness not consistent | |
| 2 | Lameness consistent under certain circumstances | |
| 3 | Lameness consistently observable on a straight line | |
| 4 | Obvious lameness at walk: marked nodding or shortened stride | |
| 5 | Minimal weight-bearing lameness in motion or at rest | |
| Flexion Test | 0 | No flexion response |
| 1 | Mild flexion response | |
| 2 | Moderate flexion response | |
| 3 | Severe flexion response |
| Week | Exercise |
|---|---|
| 0–2 | 2 days: stall confinement Handwalk: 10 min Day 15: new treatment |
| 3–4 | 2 days: stall confinement Handwalk: 10 min VET-CHECK + U/S |
| 5 | Handwalk: 15 min |
| 6 | Handwalk: 20 min VET-CHECK + U/S |
| 7 | Handwalk: 25 min |
| 8 | Handwalk: 30 min VET-CHECK + U/S |
| 9–10 | Handwalk: 30 min + 5 min trot |
| 11–12 | Handwalk: 30 min + 10 min trot VET-CHECK + U/S |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leal Reis, I.; Lopes, B.; Sousa, P.; Sousa, A.C.; Branquinho, M.V.; Caseiro, A.R.; Rêma, A.; Briote, I.; Mendonça, C.M.; Santos, J.M.; et al. Treatment of Equine Tarsus Long Medial Collateral Ligament Desmitis with Allogenic Synovial Membrane Mesenchymal Stem/Stromal Cells Enhanced by Umbilical Cord Mesenchymal Stem/Stromal Cell-Derived Conditioned Medium: Proof of Concept. Animals 2024, 14, 370. https://doi.org/10.3390/ani14030370
Leal Reis I, Lopes B, Sousa P, Sousa AC, Branquinho MV, Caseiro AR, Rêma A, Briote I, Mendonça CM, Santos JM, et al. Treatment of Equine Tarsus Long Medial Collateral Ligament Desmitis with Allogenic Synovial Membrane Mesenchymal Stem/Stromal Cells Enhanced by Umbilical Cord Mesenchymal Stem/Stromal Cell-Derived Conditioned Medium: Proof of Concept. Animals. 2024; 14(3):370. https://doi.org/10.3390/ani14030370
Chicago/Turabian StyleLeal Reis, Inês, Bruna Lopes, Patrícia Sousa, Ana Catarina Sousa, Mariana V. Branquinho, Ana Rita Caseiro, Alexandra Rêma, Inês Briote, Carla M. Mendonça, Jorge Miguel Santos, and et al. 2024. "Treatment of Equine Tarsus Long Medial Collateral Ligament Desmitis with Allogenic Synovial Membrane Mesenchymal Stem/Stromal Cells Enhanced by Umbilical Cord Mesenchymal Stem/Stromal Cell-Derived Conditioned Medium: Proof of Concept" Animals 14, no. 3: 370. https://doi.org/10.3390/ani14030370
APA StyleLeal Reis, I., Lopes, B., Sousa, P., Sousa, A. C., Branquinho, M. V., Caseiro, A. R., Rêma, A., Briote, I., Mendonça, C. M., Santos, J. M., Atayde, L. M., Alvites, R. D., & Maurício, A. C. (2024). Treatment of Equine Tarsus Long Medial Collateral Ligament Desmitis with Allogenic Synovial Membrane Mesenchymal Stem/Stromal Cells Enhanced by Umbilical Cord Mesenchymal Stem/Stromal Cell-Derived Conditioned Medium: Proof of Concept. Animals, 14(3), 370. https://doi.org/10.3390/ani14030370