
Root Caries Preventive Effect of Varnishes Containing Fluoride or Fluoride + Chlorhexidine/Cetylpyridinium Chloride In Vitro

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
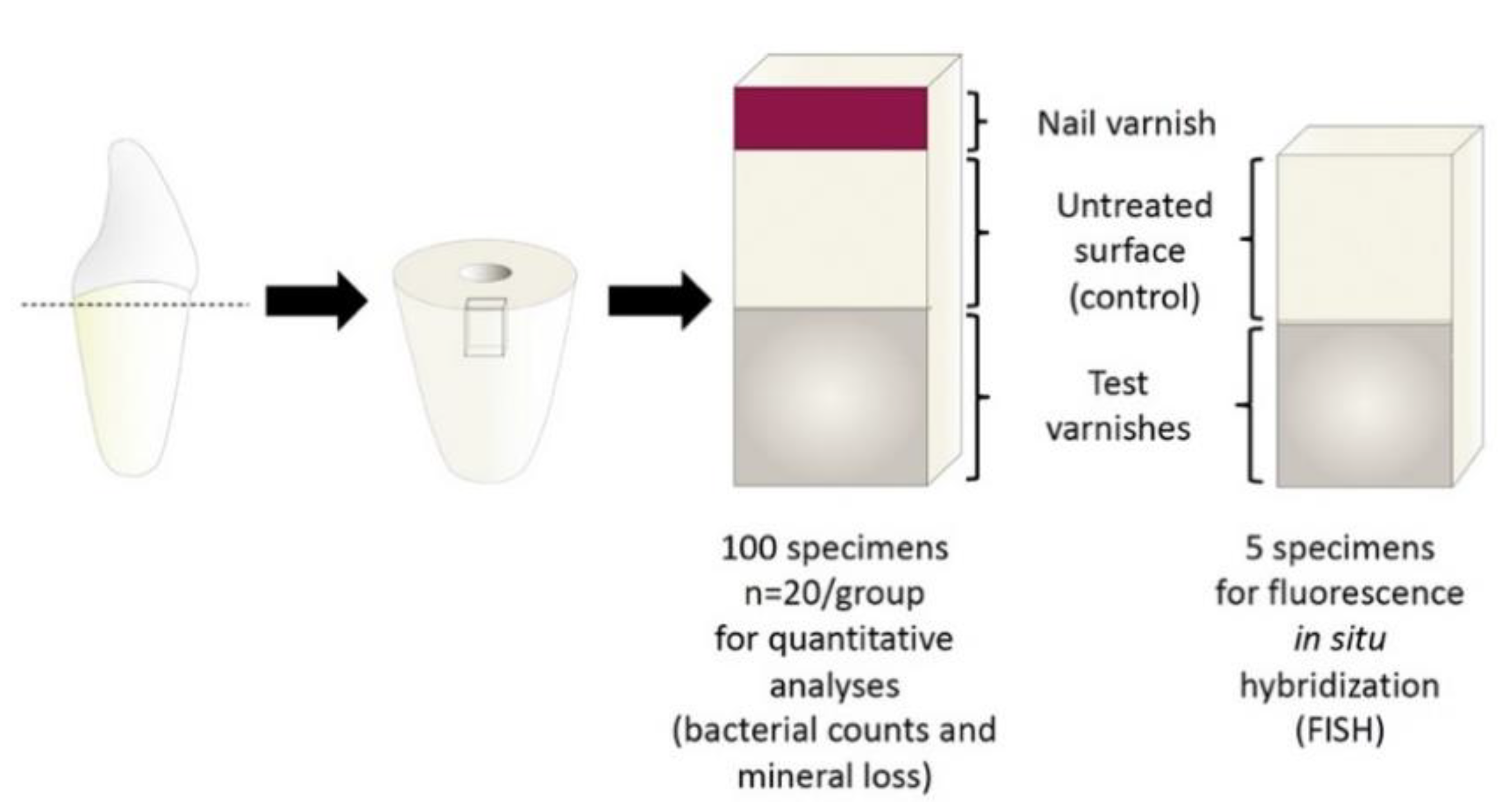
2.1. Specimen Preparation
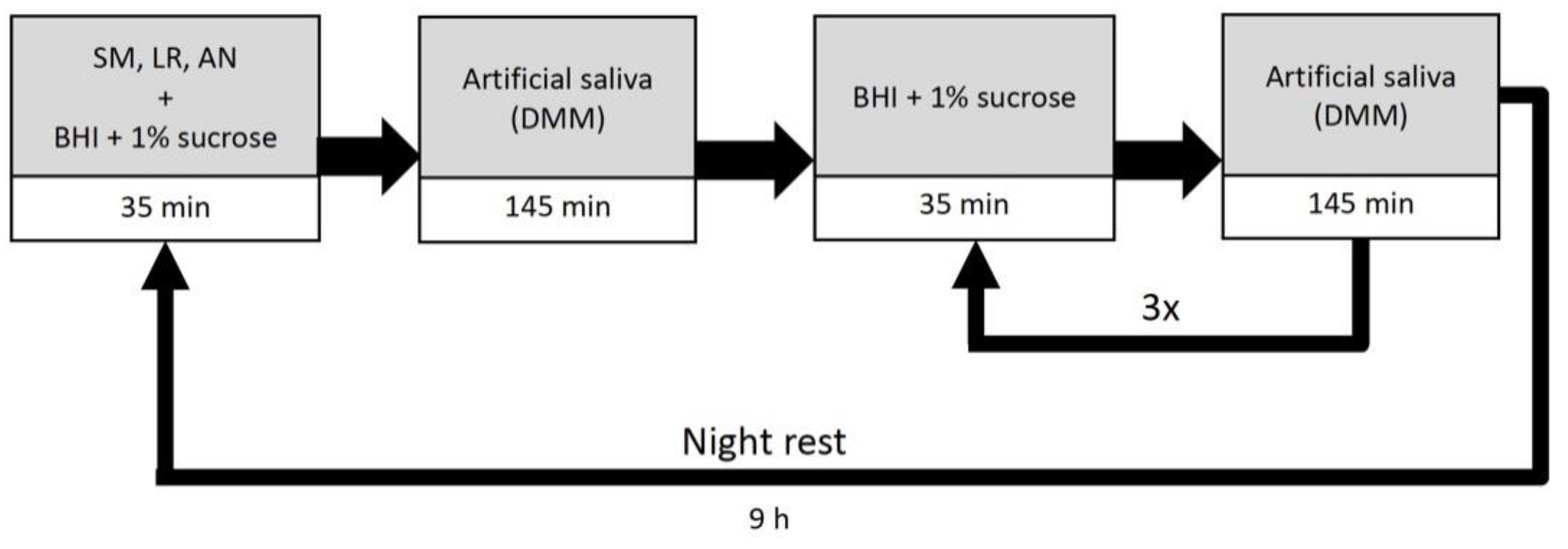
2.2. Cariogenic Challenge
2.3. Assessment of Mineral Loss
2.4. Assessment of Bacterial Counts
2.5. Preparation of Samples for Fluorescence In Situ Hybridization
2.6. FISH
2.7. Confocal Laser Scanning Microscopy
2.8. Statistical Analysis
3. Results
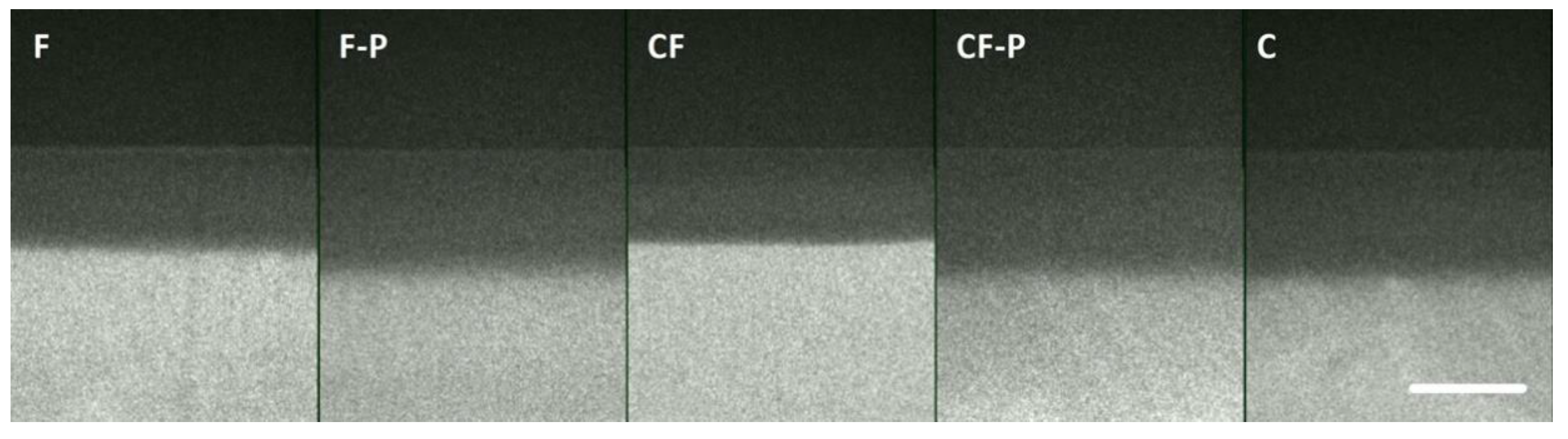
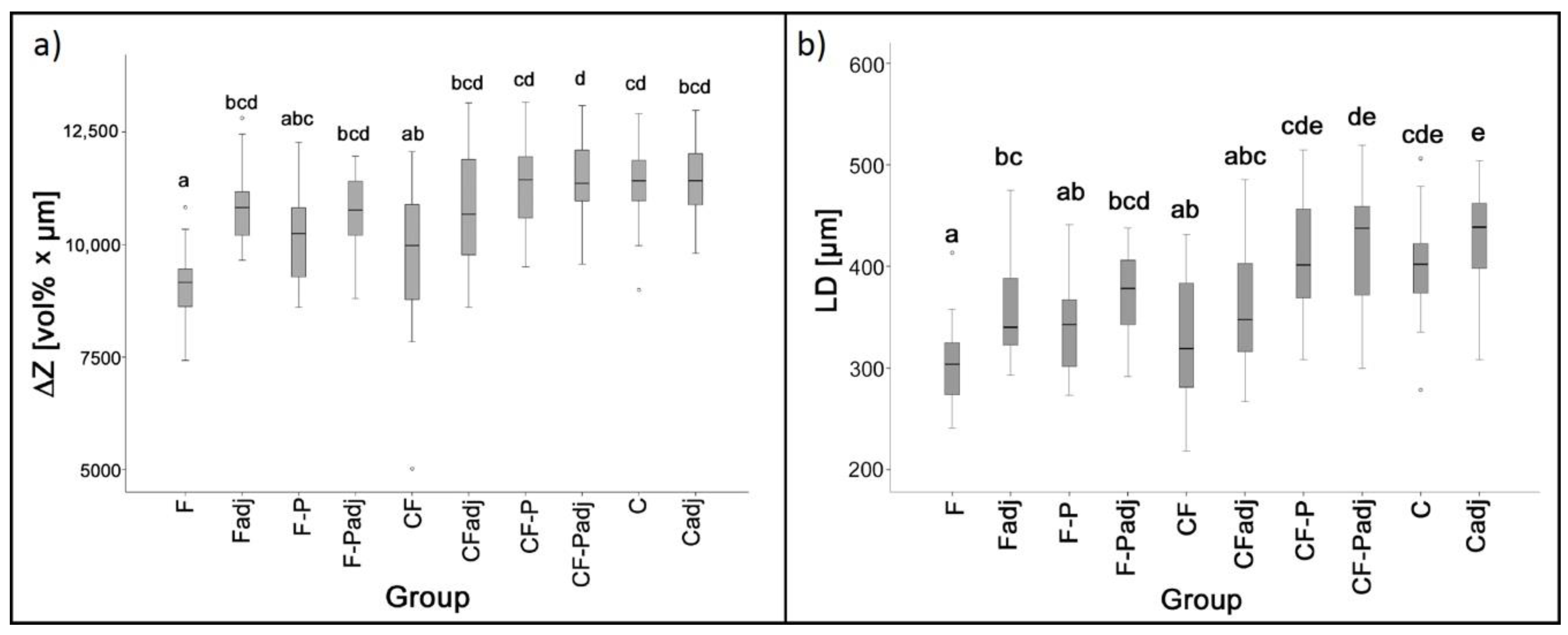
3.1. TMR
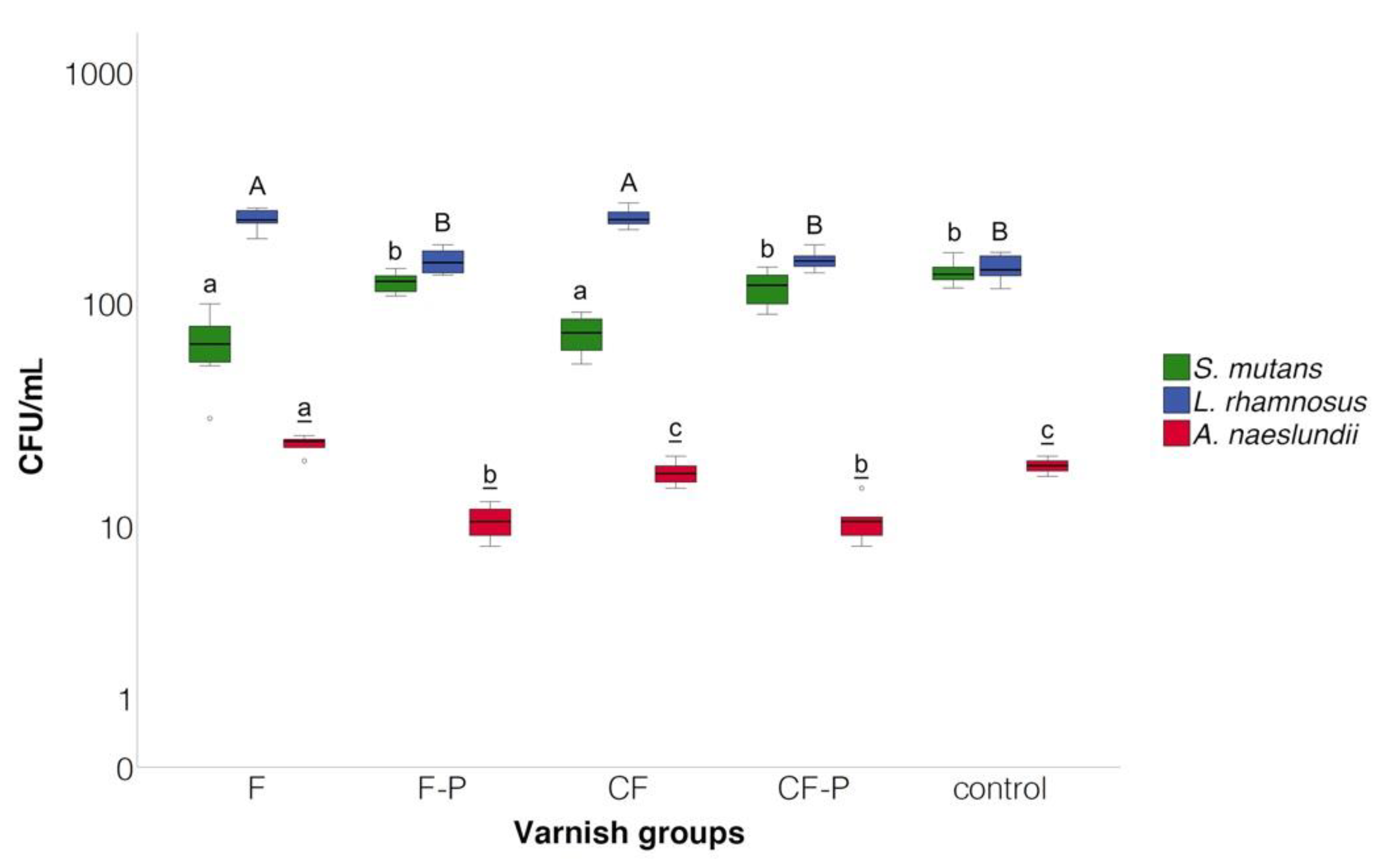
3.2. Bacterial Counts
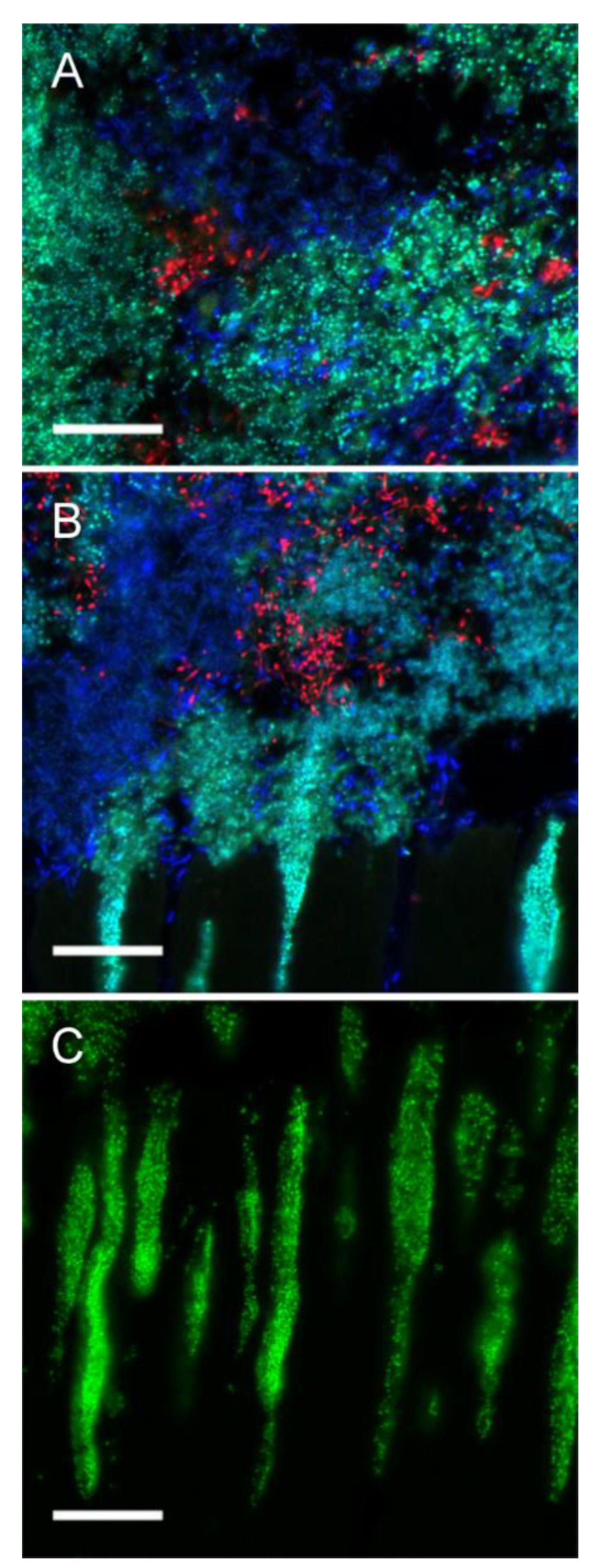
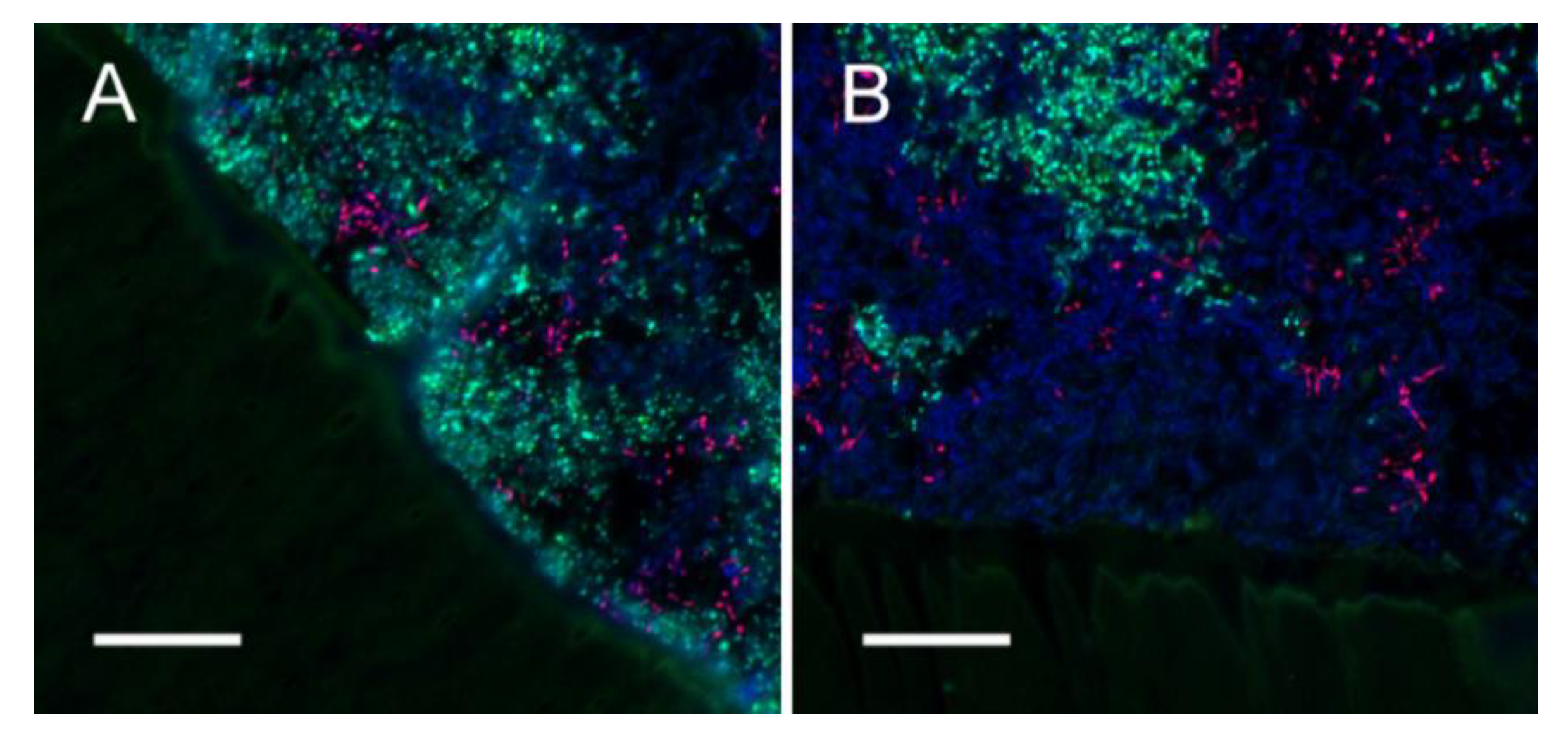
3.3. FISH
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Griffin, S.O.; Griffin, P.M.; Swann, J.L.; Zlobin, N. Estimating Rates of New Root Caries in Older Adults. J. Dent. Res. 2004, 83, 634–638. [Google Scholar] [CrossRef] [PubMed]
- López, R.; Smith, P.C.; Göstemeyer, G.; Schwendicke, F. Ageing, dental caries and periodontal diseases. J. Clin. Periodontol. 2017, 44, S145–S152. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Nyvad, B. Ecological Hypothesis of Dentin and Root Caries. Caries Res. 2016, 50, 422–431. [Google Scholar] [CrossRef]
- White, D.; Pitts, N.; Steele, J.; Sadler, K.; Chadwick, B. Disease and related disorders—A report from the Adult Dental Health Survey 2009. In Adult Dental Health Survey 2009-Summary Report and Thematic Series; National Health Service: London, UK, 2011; pp. 1–55. [Google Scholar]
- Schwendicke, F.; Krois, J.; Schiffner, U.; Micheelis, W.; Jordan, R.A. Root caries experience in Germany 1997 to 2014: Analysis of trends and identification of risk factors. J. Dent. 2018, 78, 100–105. [Google Scholar] [CrossRef]
- Hayes, M.; Brady, P.; Burke, F.M.; Allen, P.F. Failure rates of class V restorations in the management of root caries in adults—A systematic review. Gerodontology 2016, 33, 299–307. [Google Scholar] [CrossRef] [PubMed]
- Göstemeyer, G.; Da Mata, C.; McKenna, G.; Schwendicke, F. Atraumatic vs conventional restorative treatment for root caries lesions in older patients: Meta- and trial sequential analysis. Gerodontology 2019, 36, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Gil-Montoya, J.A.; Mateos-Palacios, R.; Bravo, M.; Gonzalez-Moles, M.A.; Pulgar, R. Atraumatic restorative treatment and Carisolv use for root caries in the elderly: 2-year follow-up randomized clinical trial. Clin. Oral Investig. 2013, 18, 1089–1095. [Google Scholar] [CrossRef]
- Aquilanti, L.; Santarelli, A.; Mascitti, M.; Procaccini, M.; Rappelli, G. Dental Care Access and the Elderly: What Is the Role of Teledentistry? A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 9053. [Google Scholar] [CrossRef]
- Teng, P.-R.; Lin, M.-J.; Yeh, L.-L. Utilization of dental care among patients with severe mental illness: A study of a National Health Insurance database. BMC Oral Health 2016, 16, 87. [Google Scholar] [CrossRef]
- Göstemeyer, G.; Baker, S.R.; Schwendicke, F. Barriers and facilitators for provision of oral health care in dependent older people: A systematic review. Clin. Oral Investig. 2019, 23, 979–993. [Google Scholar] [CrossRef]
- Allen, P.F.; Da Mata, C.; Hayes, M. Minimal intervention dentistry for partially dentate older adults. Gerodontology 2019, 36, 92–98. [Google Scholar] [CrossRef]
- Wierichs, R.J.; Meyer-Lueckel, H. Systematic Review on Noninvasive Treatment of Root Caries Lesions. J. Dent. Res. 2014, 94, 261–271. [Google Scholar] [CrossRef]
- Gluzman, R.; Katz, R.V.; Ma, B.J.F.; McGowan, R. Prevention of root caries: A literature review of primary and secondary preventive agents. Spéc. Care Dent. 2013, 33, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Slot, D.; Vaandrager, N.; Van Loveren, C.; Helderman, W.V.P.; Van Der Weijden, G. The Effect of Chlorhexidine Varnish on Root Caries: A Systematic Review. Caries Res. 2011, 45, 162–173. [Google Scholar] [CrossRef]
- Autio-Gold, J. The Role of Chlorhexidine in Caries Prevention. Oper. Dent. 2008, 33, 710–716. [Google Scholar] [CrossRef]
- Göstemeyer, G.; Kohls, A.; Paris, S.; Schwendicke, F. Root caries prevention via sodium fluoride, chlorhexidine and silver diamine fluoride in vitro. Odontology 2018, 106, 274–281. [Google Scholar] [CrossRef]
- Emilson, C. Potential Efficacy of Chlorhexidine against Mutans Streptococci and Human Dental Caries. J. Dent. Res. 1994, 73, 682–691. [Google Scholar] [CrossRef]
- Takeuchi, Y.; Guggenheim, B.; Filieri, A.; Baehni, P. Effect of chlorhexidine/thymol and fluoride varnishes on dental biofilm formation in vitro. Eur. J. Oral Sci. 2007, 115, 468–472. [Google Scholar] [CrossRef] [PubMed]
- De Souza, B.M.; Neto, C.F.; Salomão, P.M.A.; De Vasconcelos, L.R.S.M.; De Andrade, F.B.; Magalhães, A.C.; Fernandes, C. Analysis of the antimicrobial and anti-caries effects of TiF4 varnish under microcosm biofilm formed on enamel. J. Appl. Oral Sci. 2018, 26, e20170304. [Google Scholar] [CrossRef] [PubMed]
- Göstemeyer, G.; Schulze, F.; Paris, S.; Schwendicke, F. Arrest of Root Carious Lesions via Sodium Fluoride, Chlorhexidine and Silver Diamine Fluoride In Vitro. Materials 2017, 11, 9. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.; Sissions, C. A comparison of human dental plaque microcosm biofilms grown in an undefined medium and a chemically defined artificial saliva. Arch. Oral Biol. 2001, 46, 477–486. [Google Scholar] [CrossRef]
- Sissons, C.; Cutress, T.; Hoffman, M.; Wakefield, J. A Multi-station Dental Plaque Microcosm (Artificial Mouth) for the Study of Plaque Growth, Metabolism, pH, and Mineralization. J. Dent. Res. 1991, 70, 1409–1416. [Google Scholar] [CrossRef]
- Schwendicke, F.; Dorfer, C.; Kneist, S.; Meyer-Lueckel, H.; Paris, S. Cariogenic Effects of Probiotic Lactobacillus rhamnosus GG in a Dental Biofilm Model. Caries Res. 2014, 48, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F.; Diederich, C.; Paris, S. Restoration gaps needed to exceed a threshold size to impede sealed lesion arrest in vitro. J. Dent. 2016, 48, 77–80. [Google Scholar] [CrossRef] [PubMed]
- Arends, J.; Bosch, J.T. Demineralization and Remineralization Evaluation Techniques. J. Dent. Res. 1992, 71, 924–928. [Google Scholar] [CrossRef]
- Dige, I.; Grønkjær, L.; Nyvad, B. Molecular Studies of the Structural Ecology of Natural Occlusal Caries. Caries Res. 2014, 48, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Dige, I.; Raarup, M.K.; Nyengaard, J.R.; Kilian, M.; Nyvad, B. Actinomyces naeslundii in initial dental biofilm formation. Microbiology 2009, 155, 2116–2126. [Google Scholar] [CrossRef]
- Hoedke, D.; Enseleit, C.; Gruner, D.; Dommisch, H.; Schlafer, S.; Dige, I.; Bitter, K. Effect of photodynamic therapy in combination with various irrigation protocols on an endodontic multispecies biofilmex vivo. Int. Endod. J. 2018, 51, e23–e34. [Google Scholar] [CrossRef]
- Zaura-Arite, E.; Cate, J.M.T. Effects of fluoride- and chlorhexidine-containing varnishes on plaque composition and on demineralization of dentinal grooves in situ. Eur. J. Oral Sci. 2000, 108, 154–161. [Google Scholar] [CrossRef]
- Garcia-Godoy, F.; Flaitz, C.; Hicks, J. Role of fluoridated dentifrices in root caries formation in vitro. Am. J. Dent. 2014, 27, 23–28. [Google Scholar]
- Fernández, C.E.; Tenuta, L.M.A.; Cury, J.A. Validation of a Cariogenic Biofilm Model to Evaluate the Effect of Fluoride on Enamel and Root Dentine Demineralization. PLoS ONE 2016, 11, e0146478. [Google Scholar] [CrossRef]
- Steinberg, D.; Rozen, R.; Klausner, E.; Zachs, B.; Friedman, M. Formulation, Development and Characterization of Sustained Release Varnishes Containing Amine and Stannous Fluorides. Caries Res. 2002, 36, 411–416. [Google Scholar] [CrossRef] [PubMed]
- Al Dehailan, L.; Martinez-Mier, E.A.; Lippert, F. The effect of fluoride varnishes on caries lesions: An in vitro investigation. Clin. Oral Investig. 2015, 20, 1655–1662. [Google Scholar] [CrossRef]
- Schaeken, M.; Keltjens, H.; Van Der Hoeven, J. Effects of Fluoride and Chlorhexidine on the Microflora of Dental Root Surfaces and Progression of Root-surface Caries. J. Dent. Res. 1991, 70, 150–153. [Google Scholar] [CrossRef] [PubMed]
- Twetman, S.; Petersson, L. Efficacy of a Chlorhexidine and a Chlorhexidine-Fluoride Varnish Mixture to Decrease Interdental Levels of Mutans Streptococci. Caries Res. 1997, 31, 361–365. [Google Scholar] [CrossRef]
- Yeon, L.S.; Young, L.S. Susceptibility of Oral Streptococci to Chlorhexidine and Cetylpyridinium Chloride. Biocontrol Sci. 2019, 24, 13–21. [Google Scholar] [CrossRef]
- Zheng, C.Y.; Wang, Z.H. Effects of chlorhexidine, listerine and fluoride listerine mouthrinses on four putative root-caries pathogens in the biofilm. Chin. J. Dent. Res. 2011, 14, 135–140. [Google Scholar]
- Schaeken, M.; Beckers, H.; Van Der Hoeven, J. Effect of Chlorhexidine Varnish on Actinomyces naeslundii Genospecies in Plaque from Dental Fissures. Caries Res. 1996, 30, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Cieplik, F.; Jakubovics, N.S.; Buchalla, W.; Maisch, T.; Hellwig, E.; Al-Ahmad, A. Resistance Toward Chlorhexidine in Oral Bacteria—Is There Cause for Concern? Front. Microbiol. 2019, 10, 587. [Google Scholar] [CrossRef] [PubMed]
- Kampf, G. Acquired resistance to chlorhexidine—is it time to establish an ‘antiseptic stewardship’ initiative? J. Hosp. Infect. 2016, 94, 213–227. [Google Scholar] [CrossRef]
- Kaspar, J.R.; Godwin, M.J.; Velsko, I.M.; Richards, V.P.; Burne, R.A. Spontaneously ArisingStreptococcus mutansVariants with Reduced Susceptibility to Chlorhexidine Display Genetic Defects and Diminished Fitness. Antimicrob. Agents Chemother. 2019, 63, e00161-19. [Google Scholar] [CrossRef] [PubMed]
- Al-Ahmad, A.; Wunder, A.; Auschill, T.M.; Follo, M.; Braun, G.; Hellwig, E.; Arweiler, N.B. The in vivo dynamics of Streptococcus spp., Actinomyces naeslundii, Fusobacterium nucleatum and Veillonella spp. in dental plaque biofilm as analysed by five-colour multiplex fluorescence in situ hybridization. J. Med. Microbiol. 2007, 56, 681–687. [Google Scholar] [CrossRef]
- Arends, J.; Duschner, H.; Ruben, J. Penetration of Varnishes into Demineralized Root Dentine in vitro. Caries Res. 1997, 31, 201–205. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Yip, H.-K.; Cutress, T.W.; Samaranayake, L.P. Artificial mouth model systems and their contribution to caries research: A review. J. Dent. 2003, 31, 161–171. [Google Scholar] [CrossRef]
- Shu, M.; Wong, L.; Miller, J.; Sissons, C. Development of multi-species consortia biofilms of oral bacteria as an enamel and root caries model system. Arch. Oral Biol. 2000, 45, 27–40. [Google Scholar] [CrossRef]
- Preza, D.; Olsen, I.; Willumsen, T.; Boches, S.K.; Cotton, S.L.; Grinde, B.; Paster, B.J. Microarray analysis of the microflora of root caries in elderly. Eur. J. Clin. Microbiol. Infect. Dis. 2008, 28, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Lippert, F.; Churchley, D.; Lynch, R.J. Effect of Lesion Baseline Severity and Mineral Distribution on Remineralization and Progression of Human and Bovine Dentin Caries Lesions. Caries Res. 2015, 49, 467–476. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | Name (Manufacturer) | Active Ingredient (s) | Inactive Ingredients (wt.-%) | Batch No. |
|---|---|---|---|---|
| F | Fluor Protector S® (Ivoclar Vivadent AG) | 7700 ppm ammonium fluoride | Ethanol/water (73.4), polymer, additive (25.0), saccharin, mint flavoring (0.1) | X14474 |
| F-P | Placebo varnish for F (Ivoclar Vivadent AG) | Same ingredients as F except for ammonium fluoride | Experimental placebo varnish provided by the manufacturer exclusively for the purpose of this study | |
| CF | Cervitec F® (Ivoclar Vivadent AG) | 0.3% chlorhexidine, 0.5% cetylpyridinium chloride, 1400 ppm ammonium fluoride | Ethanol/water (80–90), Vinyl acetate/crotonic acid copolymer (8–12), saccharin, mint flavoring (<1) | X15712 |
| CF-P | Placebo varnish for CF (Ivoclar Vivadent AG) | Same ingredients as CF except for CHX and ammonium fluoride | Experimental placebo varnish provided by the manufacturer exclusively for the purpose of this study | |
| C | Untreated control | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Göstemeyer, G.; Woike, H.; Paris, S.; Schwendicke, F.; Schlafer, S. Root Caries Preventive Effect of Varnishes Containing Fluoride or Fluoride + Chlorhexidine/Cetylpyridinium Chloride In Vitro. Microorganisms 2021, 9, 737. https://doi.org/10.3390/microorganisms9040737
Göstemeyer G, Woike H, Paris S, Schwendicke F, Schlafer S. Root Caries Preventive Effect of Varnishes Containing Fluoride or Fluoride + Chlorhexidine/Cetylpyridinium Chloride In Vitro. Microorganisms. 2021; 9(4):737. https://doi.org/10.3390/microorganisms9040737
Chicago/Turabian StyleGöstemeyer, Gerd, Helen Woike, Sebastian Paris, Falk Schwendicke, and Sebastian Schlafer. 2021. "Root Caries Preventive Effect of Varnishes Containing Fluoride or Fluoride + Chlorhexidine/Cetylpyridinium Chloride In Vitro" Microorganisms 9, no. 4: 737. https://doi.org/10.3390/microorganisms9040737
APA StyleGöstemeyer, G., Woike, H., Paris, S., Schwendicke, F., & Schlafer, S. (2021). Root Caries Preventive Effect of Varnishes Containing Fluoride or Fluoride + Chlorhexidine/Cetylpyridinium Chloride In Vitro. Microorganisms, 9(4), 737. https://doi.org/10.3390/microorganisms9040737