
Anti-Acid Drug Treatment Induces Changes in the Gut Microbiome Composition of Hemodialysis Patients

 ,
,  , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Comorbidity, Laboratory, and Clinical Variables
2.3. Fecal Sample Collection and Bacterial 16S rRNA Amplicon Sequencing
2.4. Statistical and Bioinformatics Analyses
2.5. Functional Annotation
3. Results
3.1. Patient Characteristics
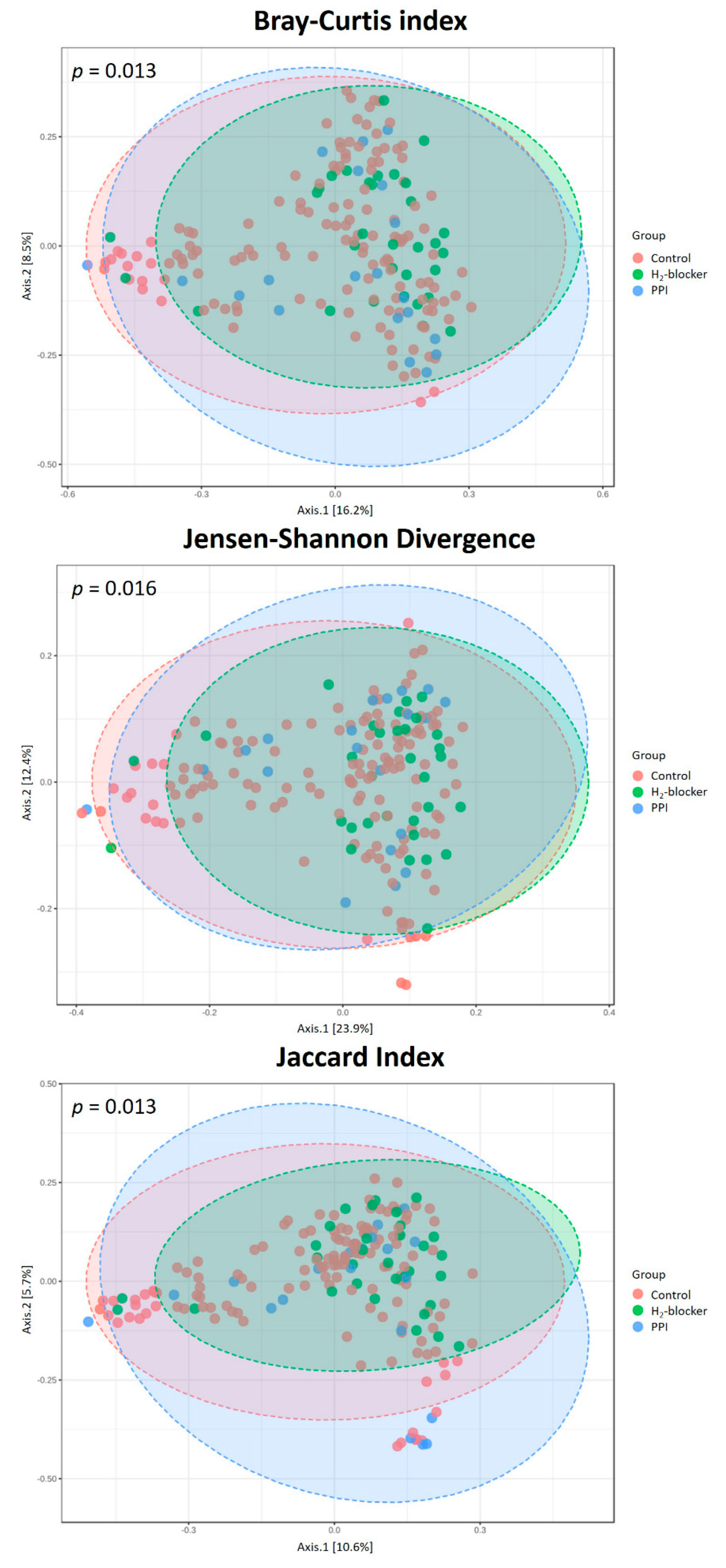
3.2. Differences in the Gut Microbiota Profile in HD Patients
3.3. Co-Occurrence Pattern Analysis of the Intestinal Ecosystems of HD Patients Treated with H2-Blocker, PPI and Control
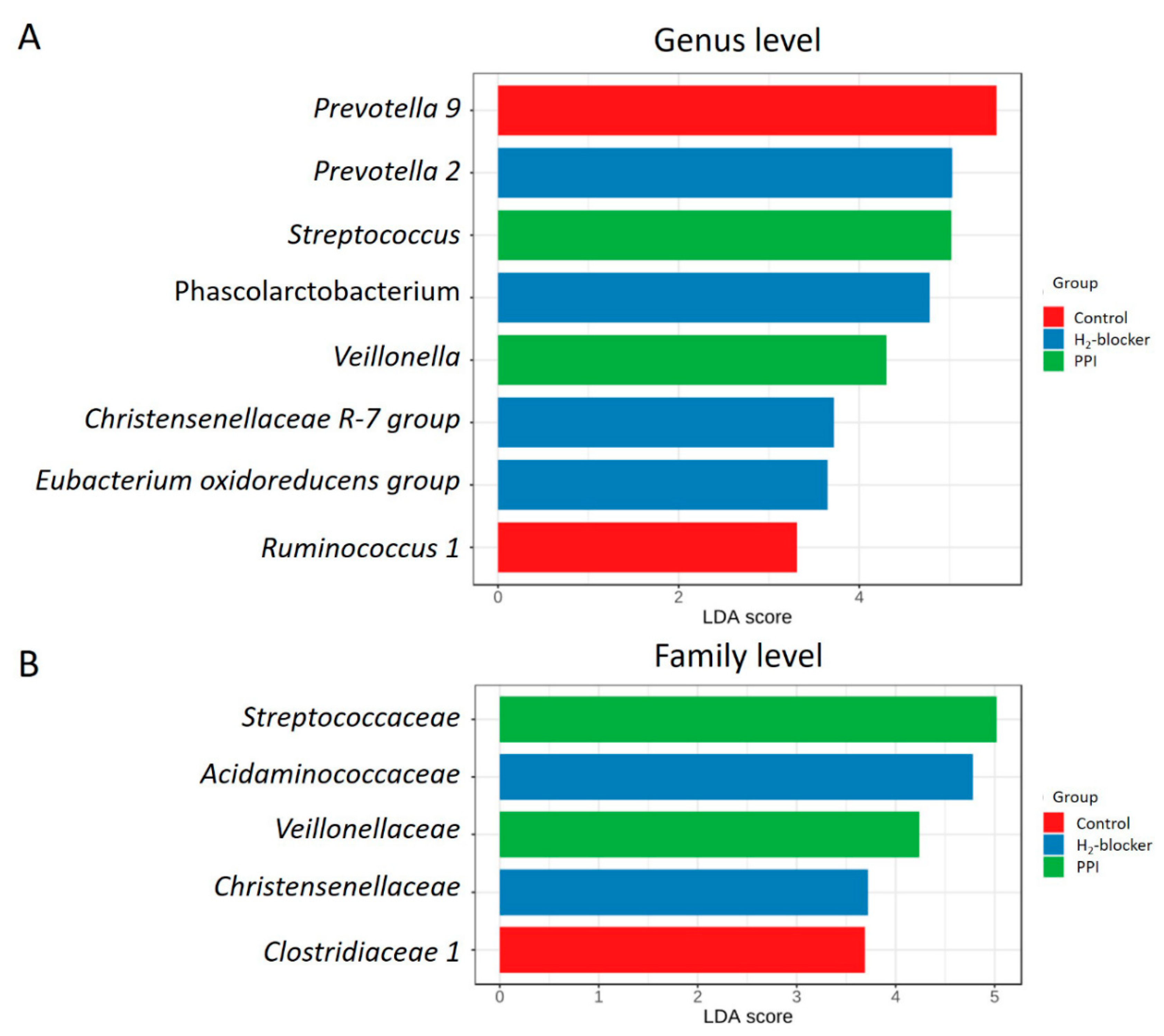
3.4. Specific Microbial Taxa Are Associated with H2-Blocker and PPI Use
3.5. Comparison of the Microbiome Differences between H2-Blocker Users and PPI Users
3.6. Oral Bacterial Translocation in Anti-Acid Users
3.7. Functional Characterization of the Microbiome of H2-Blocker or PPI Users Compared to Controls
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vaziri, N.D.; Wong, J.; Pahl, M.; Piceno, Y.M.; Yuan, J.; DeSantis, T.Z.; Ni, Z.; Nguyen, T.H.; Andersen, G.L. Chronic kidney disease alters intestinal microbial flora. Kidney Int. 2013, 83, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Jackson, M.A.; Verdi, S.; Maxan, M.E.; Shin, C.M.; Zierer, J.; Bowyer, R.C.E.; Martin, T.; Williams, F.M.K.; Menni, C.; Bell, J.T.; et al. Gut microbiota associations with common diseases and prescription medications in a population-based cohort. Nat. Commun. 2018, 9, 2655. [Google Scholar] [CrossRef] [PubMed]
- Vangala, C.; Niu, J.; Lenihan, C.R.; Mitch, W.E.; Navaneethan, S.D.; Winkelmayer, W.C. Proton Pump Inhibitors, Histamine-2 Receptor Antagonists, and Hip Fracture Risk among Patients on Hemodialysis. Clin. J. Am. Soc. Nephrol. 2018, 13, 1534–1541. [Google Scholar] [CrossRef] [PubMed]
- Nehra, A.K.; Alexander, J.A.; Loftus, C.G.; Nehra, V. Proton Pump Inhibitors: Review of Emerging Concerns. Mayo Clin. Proc. 2018, 93, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Freedberg, D.E.; Kim, L.S.; Yang, Y.X. The Risks and Benefits of Long-term Use of Proton Pump Inhibitors: Expert Review and Best Practice Advice From the American Gastroenterological Association. Gastroenterology 2017, 152, 706–715. [Google Scholar] [CrossRef]
- Vaezi, M.F.; Yang, Y.X.; Howden, C.W. Complications of Proton Pump Inhibitor Therapy. Gastroenterology 2017, 153, 35–48. [Google Scholar] [CrossRef]
- De Francisco, A.L.M.; Varas, J.; Ramos, R.; Merello, J.I.; Canaud, B.; Stuard, S.; Pascual, J.; Aljama, P.; Optimizing Results in Dialysis (ORD) Group. Proton Pump Inhibitor Usage and the Risk of Mortality in Hemodialysis Patients. Kidney Int. Rep. 2018, 3, 374–384. [Google Scholar] [CrossRef]
- Tsai, I.J.; Lai, T.S.; Shiao, C.C.; Huang, T.M.; Wang, C.H.; Chen, L.W.; Lin, Y.H.; Chen, L.; Wu, V.C.; Chu, T.S.; et al. Proton-Pump Inhibitors Augment the Risk of Major Adverse Cardiovascular Events and End-Stage Renal Disease in Patients with Acute Kidney Injury After Temporary Dialysis. Clin. Pharmacol. Ther. 2020, 10.1002/cpt.1762. [Google Scholar] [CrossRef]
- Okamoto, T.; Hatakeyama, S.; Hosogoe, S.; Tanaka, Y.; Imanishi, K.; Takashima, T.; Saitoh, F.; Suzuki, T.; Ohyama, C. Proton pump inhibitor as an independent factor of progression of abdominal aortic calcification in patients on maintenance hemodialysis. PLoS ONE 2018, 13, e0199160. [Google Scholar] [CrossRef]
- Imhann, F.; Bonder, M.J.; Vich Vila, A.; Fu, J.; Mujagic, Z.; Vork, L.; Tigchelaar, E.F.; Jankipersadsing, S.A.; Cenit, M.C.; Harmsen, H.J.; et al. Proton pump inhibitors affect the gut microbiome. Gut 2016, 65, 740–748. [Google Scholar] [CrossRef]
- Jackson, M.A.; Goodrich, J.K.; Maxan, M.E.; Freedberg, D.E.; Abrams, J.A.; Poole, A.C.; Sutter, J.L.; Welter, D.; Ley, R.E.; Bell, J.T.; et al. Proton pump inhibitors alter the composition of the gut microbiota. Gut 2016, 65, 749–756. [Google Scholar] [CrossRef] [PubMed]
- Bavishi, C.; Dupont, H.L. Systematic review: The use of proton pump inhibitors and increased susceptibility to enteric infection. Aliment. Pharmacol. Ther. 2011, 34, 1269–1281. [Google Scholar] [CrossRef] [PubMed]
- Clooney, A.G.; Bernstein, C.N.; Leslie, W.D.; Vagianos, K.; Sargent, M.; Laserna-Mendieta, E.J.; Claesson, M.J.; Targownik, L.E. A comparison of the gut microbiome between long-term users and non-users of proton pump inhibitors. Aliment. Pharmacol. Ther. 2016, 43, 974–984. [Google Scholar] [CrossRef] [PubMed]
- Freedberg, D.E.; Toussaint, N.C.; Chen, S.P.; Ratner, A.J.; Whittier, S.; Wang, T.C.; Wang, H.H.; Abrams, J.A. Proton Pump Inhibitors Alter Specific Taxa in the Human Gastrointestinal Microbiome: A Crossover Trial. Gastroenterology 2015, 149, 883–885.e889. [Google Scholar] [CrossRef] [PubMed]
- Takagi, T.; Naito, Y.; Inoue, R.; Kashiwagi, S.; Uchiyama, K.; Mizushima, K.; Tsuchiya, S.; Okayama, T.; Dohi, O.; Yoshida, N.; et al. The influence of long-term use of proton pump inhibitors on the gut microbiota: An age-sex-matched case-control study. J. Clin. Biochem. Nutr. 2018, 62, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Herlemann, D.P.; Labrenz, M.; Jurgens, K.; Bertilsson, S.; Waniek, J.J.; Andersson, A.F. Transitions in bacterial communities along the 2000 km salinity gradient of the Baltic Sea. ISME J. 2011, 5, 1571–1579. [Google Scholar] [CrossRef]
- Lozupone, C.A.; Hamady, M.; Kelley, S.T.; Knight, R. Quantitative and qualitative beta diversity measures lead to different insights into factors that structure microbial communities. Appl. Environ. Microbiol. 2007, 73, 1576–1585. [Google Scholar] [CrossRef]
- Gevers, D.; Kugathasan, S.; Denson, L.A.; Vazquez-Baeza, Y.; Van Treuren, W.; Ren, B.; Schwager, E.; Knights, D.; Song, S.J.; Yassour, M.; et al. The treatment-naive microbiome in new-onset Crohn’s disease. Cell Host Microbe 2014, 15, 382–392. [Google Scholar] [CrossRef]
- Segata, N.; Izard, J.; Waldron, L.; Gevers, D.; Miropolsky, L.; Garrett, W.S.; Huttenhower, C. Metagenomic biomarker discovery and explanation. Genome Biol. 2011, 12, R60. [Google Scholar] [CrossRef]
- Foster, Z.S.; Sharpton, T.J.; Grunwald, N.J. Metacoder: An R package for visualization and manipulation of community taxonomic diversity data. PLoS Comput. Biol. 2017, 13, e1005404. [Google Scholar] [CrossRef]
- Svetnik, V.; Liaw, A.; Tong, C.; Culberson, J.C.; Sheridan, R.P.; Feuston, B.P. Random forest: A classification and regression tool for compound classification and QSAR modeling. J. Chem. Inf. Comput. Sci. 2003, 43, 1947–1958. [Google Scholar] [CrossRef] [PubMed]
- Love, M.I.; Huber, W.; Anders, S. Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol. 2014, 15, 550. [Google Scholar] [CrossRef] [PubMed]
- Dhariwal, A.; Chong, J.; Habib, S.; King, I.L.; Agellon, L.B.; Xia, J. MicrobiomeAnalyst: A web-based tool for comprehensive statistical, visual and meta-analysis of microbiome data. Nucleic Acids Res. 2017, 45, W180–W188. [Google Scholar] [CrossRef] [PubMed]
- Chong, J.; Liu, P.; Zhou, G.; Xia, J. Using MicrobiomeAnalyst for comprehensive statistical, functional, and meta-analysis of microbiome data. Nat. Protoc. 2020, 10.1038/s41596-019-0264-1. [Google Scholar] [CrossRef] [PubMed]
- Asshauer, K.P.; Wemheuer, B.; Daniel, R.; Meinicke, P. Tax4Fun: Predicting functional profiles from metagenomic 16S rRNA data. Bioinformatics 2015, 31, 2882–2884. [Google Scholar] [CrossRef]
- Lau, W.L.; Vaziri, N.D.; Nunes, A.C.F.; Comeau, A.M.; Langille, M.G.I.; England, W.; Khazaeli, M.; Suematsu, Y.; Phan, J.; Whiteson, K. The Phosphate Binder Ferric Citrate Alters the Gut Microbiome in Rats with Chronic Kidney Disease. J. Pharmacol. Exp. Ther. 2018, 367, 452–460. [Google Scholar] [CrossRef]
- Macke, L.; Schulz, C.; Koletzko, L.; Malfertheiner, P. Systematic review: The effects of proton pump inhibitors on the microbiome of the digestive tract-evidence from next-generation sequencing studies. Aliment. Pharmacol. Ther. 2020. [Google Scholar] [CrossRef]
- Naito, Y.; Kashiwagi, K.; Takagi, T.; Andoh, A.; Inoue, R. Intestinal Dysbiosis Secondary to Proton-Pump Inhibitor Use. Digestion 2018, 97, 195–204. [Google Scholar] [CrossRef]
- Dong, T.; Pisegna, J. Passing the “Acid Test”: Do Proton Pump Inhibitors Affect the Composition of the Microbiome? Dig. Dis. Sci. 2018, 63, 2817–2819. [Google Scholar] [CrossRef]
- Andersson, A.F.; Lindberg, M.; Jakobsson, H.; Backhed, F.; Nyren, P.; Engstrand, L. Comparative analysis of human gut microbiota by barcoded pyrosequencing. PLoS ONE 2008, 3, e2836. [Google Scholar] [CrossRef]
- Fujimori, S. What are the effects of proton pump inhibitors on the small intestine? World J. Gastroenterol. 2015, 21, 6817–6819. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.X.; Metz, D.C. Safety of proton pump inhibitor exposure. Gastroenterology 2010, 139, 1115–1127. [Google Scholar] [CrossRef] [PubMed]
- Markovits, N.; Loebstein, R.; Halkin, H.; Bialik, M.; Landes-Westerman, J.; Lomnicky, J.; Kurnik, D. The association of proton pump inhibitors and hypomagnesemia in the community setting. J. Clin. Pharmacol. 2014, 54, 889–895. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Cui, Y.; Qu, X. Mechanisms and improvement of acid resistance in lactic acid bacteria. Arch. Microbiol. 2018, 200, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Cui, Y.; Miao, K.; Niyaphorn, S.; Qu, X. Production of Gamma-Aminobutyric Acid from Lactic Acid Bacteria: A Systematic Review. Int. J. Mol. Sci. 2020, 21, 995. [Google Scholar] [CrossRef]
- Van der Loo, B.; Bachschmid, M.; Spitzer, V.; Brey, L.; Ullrich, V.; Luscher, T.F. Decreased plasma and tissue levels of vitamin C in a rat model of aging: Implications for antioxidative defense. Biochem. Biophys. Res. Commun. 2003, 303, 483–487. [Google Scholar] [CrossRef]
- Hutchinson, C.; Geissler, C.A.; Powell, J.J.; Bomford, A. Proton pump inhibitors suppress absorption of dietary non-haem iron in hereditary haemochromatosis. Gut 2007, 56, 1291–1295. [Google Scholar] [CrossRef]
- Handa, P.; Kowdley, K.V. A Proton Pump Inhibitor a Day Keeps the Iron Away. Clin. Gastroenterol. Hepatol. 2016, 14, 153–155. [Google Scholar] [CrossRef]
- Lynch, S.V.; Pedersen, O. The Human Intestinal Microbiome in Health and Disease. N. Engl. J. Med. 2016, 375, 2369–2379. [Google Scholar] [CrossRef]
- Belizario, J.E.; Faintuch, J.; Garay-Malpartida, M. Gut Microbiome Dysbiosis and Immunometabolism: New Frontiers for Treatment of Metabolic Diseases. Mediators Inflamm. 2018, 2018, 2037838. [Google Scholar] [CrossRef]
- DeGruttola, A.K.; Low, D.; Mizoguchi, A.; Mizoguchi, E. Current Understanding of Dysbiosis in Disease in Human and Animal Models. Inflamm. Bowel Dis. 2016, 22, 1137–1150. [Google Scholar] [CrossRef] [PubMed]
- Nallu, A.; Sharma, S.; Ramezani, A.; Muralidharan, J.; Raj, D. Gut microbiome in chronic kidney disease: Challenges and opportunities. Transl. Res. 2017, 179, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Stadlbauer, V.; Horvath, A.; Ribitsch, W.; Schmerbock, B.; Schilcher, G.; Lemesch, S.; Stiegler, P.; Rosenkranz, A.R.; Fickert, P.; Leber, B. Structural and functional differences in gut microbiome composition in patients undergoing haemodialysis or peritoneal dialysis. Sci. Rep. 2017, 7, 15601. [Google Scholar] [CrossRef] [PubMed]
- Cigarran Guldris, S.; Gonzalez Parra, E.; Cases Amenos, A. Gut microbiota in chronic kidney disease. Nefrologia 2017, 37, 9–19. [Google Scholar] [CrossRef]
- Eom, C.S.; Jeon, C.Y.; Lim, J.W.; Cho, E.G.; Park, S.M.; Lee, K.S. Use of acid-suppressive drugs and risk of pneumonia: A systematic review and meta-analysis. CMAJ 2011, 183, 310–319. [Google Scholar] [CrossRef]
- De Jager, C.P.; Wever, P.C.; Gemen, E.F.; van Oijen, M.G.; van Gageldonk-Lafeber, A.B.; Siersema, P.D.; Kusters, G.C.; Laheij, R.J. Proton pump inhibitor therapy predisposes to community-acquired Streptococcus pneumoniae pneumonia. Aliment. Pharmacol. Ther. 2012, 36, 941–949. [Google Scholar] [CrossRef]
- Xu, H.B.; Wang, H.D.; Li, C.H.; Ye, S.; Dong, M.S.; Xia, Q.J.; Zhang, A.Q.; Pan, K.; Ge, X.L.; Dong, J.H. Proton pump inhibitor use and risk of spontaneous bacterial peritonitis in cirrhotic patients: A systematic review and meta-analysis. Genet. Mol. Res. 2015, 14, 7490–7501. [Google Scholar] [CrossRef]
- Zhou, S.J.; Wang, S.Q.; Ma, Y.Y.; Tang, L.Y.; Shi, Y.F.; Liang, B.; Chen, Y.; Yu, K. Association of proton pump inhibitors with the occurrence of gut-derived bacteraemia in patients with haematological malignancy after chemotherapy. Hematology 2016, 21, 332–337. [Google Scholar] [CrossRef][Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Histamine-2 Blocker Users (N = 32) | Proton Pump Inhibitor Users (N = 23) | Control Subjects (N = 138) | p-Value |
|---|---|---|---|---|
| Age (years) | 65 ± 11.5 | 68.3 ± 12.1 | 64.1 ± 11.0 | 0.309 |
| Male | 17 (73.9%) | 12 (37.5%) | 77 (55.8%) | 0.026 |
| Dialysis vintage (months) | 84.37 ± 52.55 | 98.09 ± 61.51 | 92.02 ± 61.73 | 0.778 |
| Cause of ESRD | ||||
| Hypertension | 1 (4.3%) | 2 (6.3%) | 14 (10.1%) | 0.566 |
| Diabetes mellitus | 11 (47.8%) | 12 (37.5%) | 43 (31.2%) | 0.270 |
| Glomerulonephritis | 6 (26.1%) | 13 (40.6%) | 56 (40.6%) | 0.408 |
| Others * | 5 (21.7%) | 5 (15.6%) | 25 (18.1%) | 0.845 |
| Comorbidities | ||||
| Diabetes mellitus | 13 (56.5%) | 12 (37.5%) | 54 (39.1%) | 0.265 |
| Hypertension | 18 (78.3%) | 27 (84.4%) | 122 (88.4%) | 0.388 |
| Dyslipidemia | 9 (39.1%) | 12 (37.5%) | 34 (24.6%) | 0.169 |
| Medications | ||||
| Anti-hypertensive drugs | 17 (73.9%) | 22 (68.8%) | 79 (57.2%) | 0.198 |
| Diabetes treatment medications | 9 (39.1%) | 9 (28.1%) | 39 (28.3%) | 0.561 |
| Calcium carbonate | 18 (78.3%) | 23 (71.9%) | 120 (87.0%) | 0.092 |
| Clinical laboratory data | ||||
| Hemoglobin (g/dL) | 10.51 ± 1.10 | 10.64 ± 1.09 | 10.7 ± 1.38 | 0.517 |
| Albumin (g/dL) | 3.54 ± 0.71 | 3.52 ± 0.52 | 3.55 ± 0.42 | 0.832 |
| High sensitivity CRP (mg/dL) | 3.4 ± 4.04 | 1.65 ± 4.12 | 2.35 ± 4.50 | 0.574 |
| Total calcium (mg/dL) | 9.27 ± 0.99 | 9.14 ± 1.10 | 9.24 ± 0.85 | 0.901 |
| Phosphate (mg/dL) | 4.63 ± 1.35 | 4.69 ± 1.19 | 5.14 ± 1.20 | 0.020 |
| Single pool Kt/V | 1.55 ± 0.14 | 1.65 ± 0.29 | 1.68 ± 0.28 | 0.046 |
| Dietary intake (serving/day) | ||||
| Meat | 0.86 ± 0.63 | 0.91 ± 0.63 | 0.82 ± 0.51 | 0.695 |
| Vegetable | 1.51 ± 1.20 | 1.8 ± 1.01 | 2.02 ± 1.09 | 0.083 |
| Fruit | 0.8 ± 0.90 | 0.84 ± 0.54 | 0.99 ± 0.72 | 0.399 |
| Bristol stool scale | 3.96 ± 1.77 | 4 ± 1.95 | 3.76 ± 1.78 | 0.745 |
| Anti-acid drugs indication | ||||
| Peptic ulcer disease | 8 (25%) | 11 (47.8%) | ||
| Gastroesophageal reflux disease | 15 (46.9%) | 10 (43.5%) | ||
| Others ** | 9 (28.1%) | 2 (8.7%) |
| Taxonomic Level | Taxon | PPI Users (n = 23) Reads Count, Mean ± SD | Controls (n = 138) Reads Count, Mean ± SD | p-Value, Crude | p-Value, Adjusted * |
|---|---|---|---|---|---|
| Class | Bacilli | 1093.1 ± 2121.2 | 34.9 ± 76.9 | <0.001 | <0.001 |
| Order | Lactobacillales | 1092.5 ± 2120.5 | 34.6 ± 76.9 | <0.001 | <0.001 |
| Family | Streptococcaceae | 826.4 ± 2047.8 | 20.5 ± 36.9 | <0.001 | <0.001 |
| Genus | Streptococcus | 826.4 ± 2047.8 | 20.5 ± 36.9 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, Y.-T.; Lin, T.-Y.; Hung, S.-C.; Liu, P.-Y.; Wu, P.-H.; Chuang, Y.-S.; Hung, W.-C.; Chiu, Y.-W.; Kuo, M.-C.; Wu, C.-Y. Anti-Acid Drug Treatment Induces Changes in the Gut Microbiome Composition of Hemodialysis Patients. Microorganisms 2021, 9, 286. https://doi.org/10.3390/microorganisms9020286
Lin Y-T, Lin T-Y, Hung S-C, Liu P-Y, Wu P-H, Chuang Y-S, Hung W-C, Chiu Y-W, Kuo M-C, Wu C-Y. Anti-Acid Drug Treatment Induces Changes in the Gut Microbiome Composition of Hemodialysis Patients. Microorganisms. 2021; 9(2):286. https://doi.org/10.3390/microorganisms9020286
Chicago/Turabian StyleLin, Yi-Ting, Ting-Yun Lin, Szu-Chun Hung, Po-Yu Liu, Ping-Hsun Wu, Yun-Shiuan Chuang, Wei-Chun Hung, Yi-Wen Chiu, Mei-Chuan Kuo, and Chun-Ying Wu. 2021. "Anti-Acid Drug Treatment Induces Changes in the Gut Microbiome Composition of Hemodialysis Patients" Microorganisms 9, no. 2: 286. https://doi.org/10.3390/microorganisms9020286
APA StyleLin, Y.-T., Lin, T.-Y., Hung, S.-C., Liu, P.-Y., Wu, P.-H., Chuang, Y.-S., Hung, W.-C., Chiu, Y.-W., Kuo, M.-C., & Wu, C.-Y. (2021). Anti-Acid Drug Treatment Induces Changes in the Gut Microbiome Composition of Hemodialysis Patients. Microorganisms, 9(2), 286. https://doi.org/10.3390/microorganisms9020286