

Evaluation of the Diagnostic Performance of Two Automated SARS-CoV-2 Neutralization Immunoassays following Two Doses of mRNA, Adenoviral Vector, and Inactivated Whole-Virus Vaccinations in COVID-19 Naïve Subjects
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Laboratory Methods
2.3. Statistical Analysis
3. Results
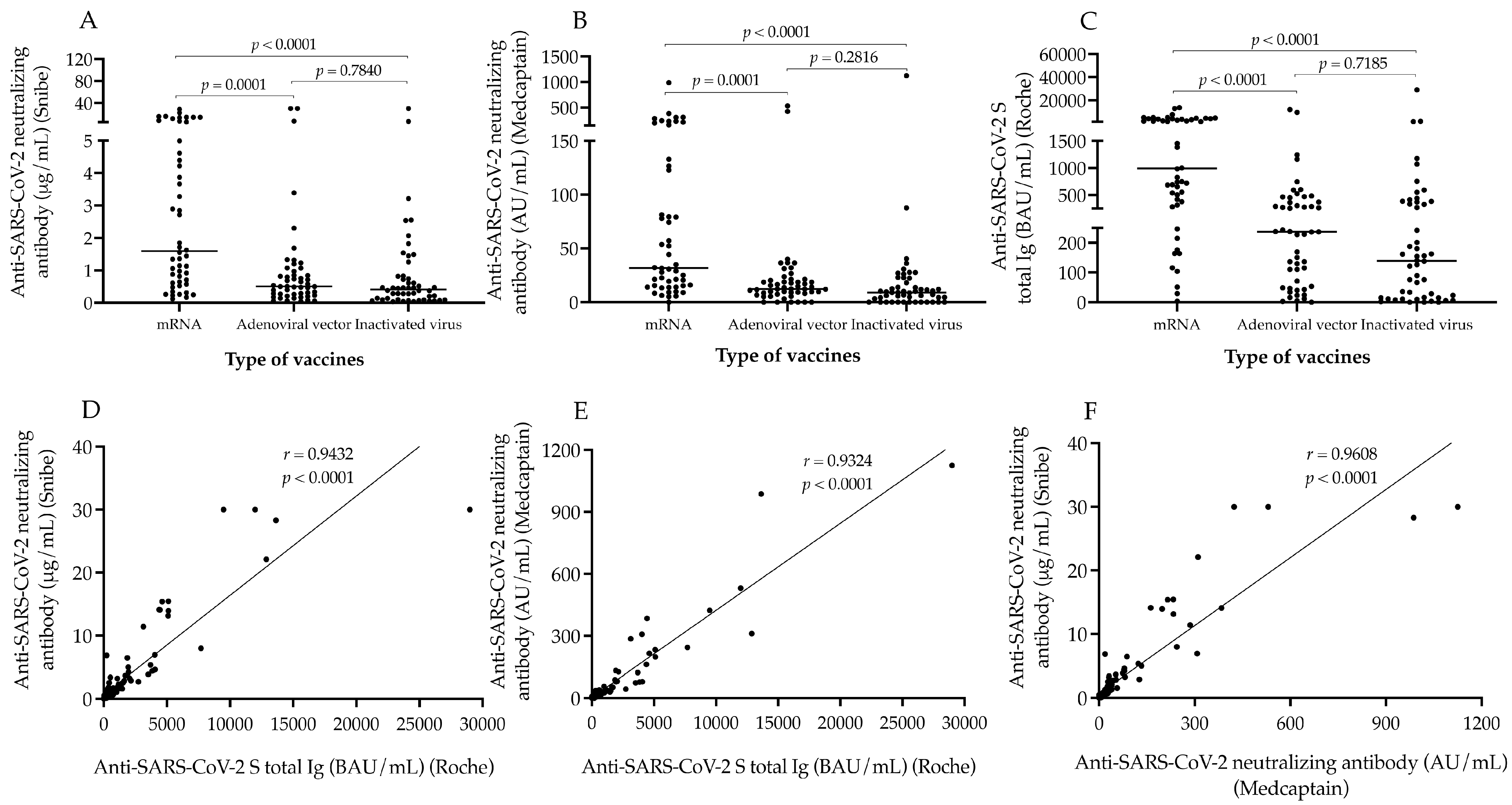
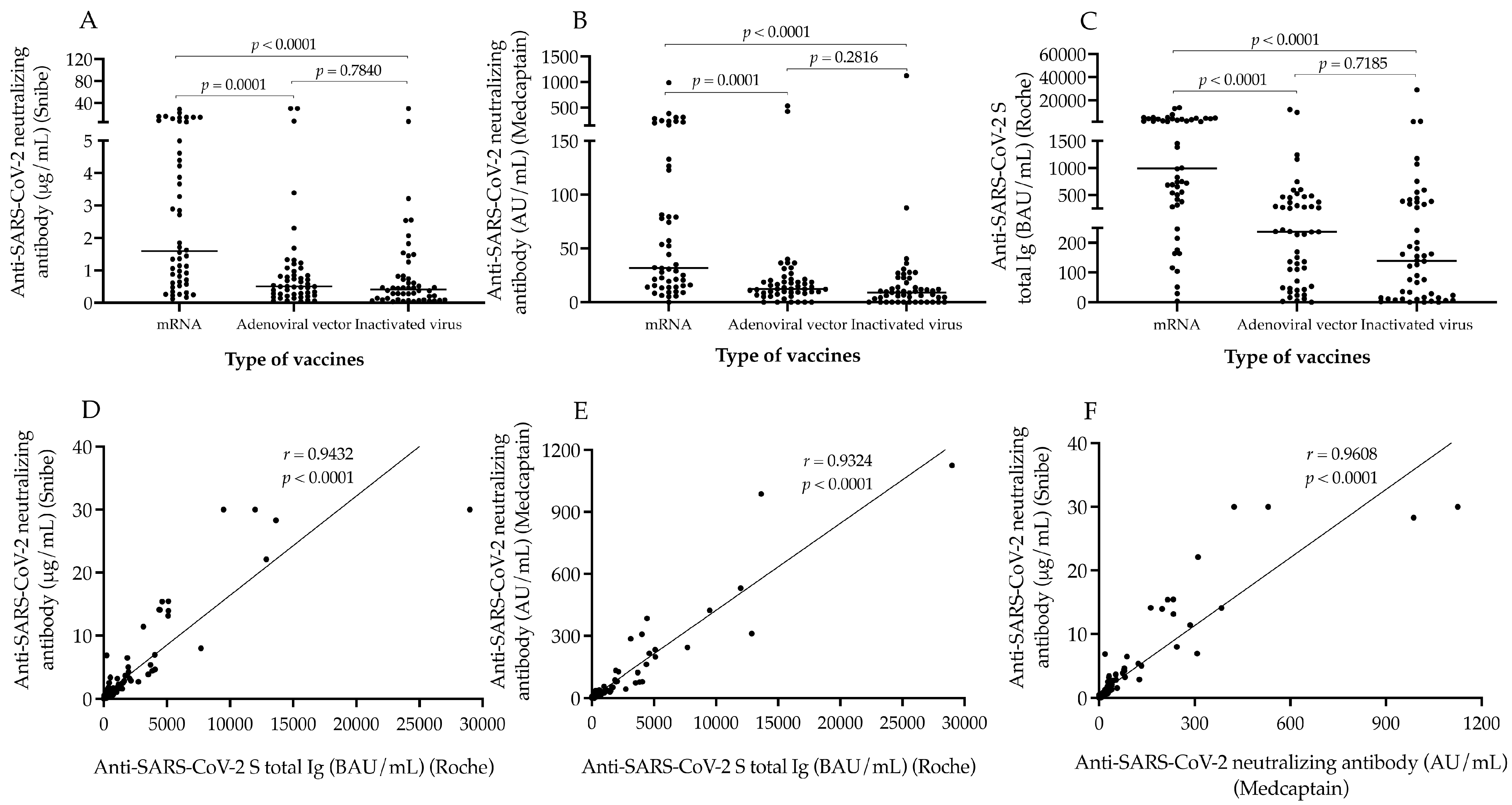
3.1. Comparison of the Levels of Anti-SARS-CoV-2 Neutralizing Antibody by Two Different Neutralization Tests with Total Spike Immunoglobulin following Two Doses of Three Different Vaccinations
3.2. The Effect of Age, Gender and Elapsed Time between Vaccination and Serology on Neutralizing Antibodies and Total Spike Immunoglobulins
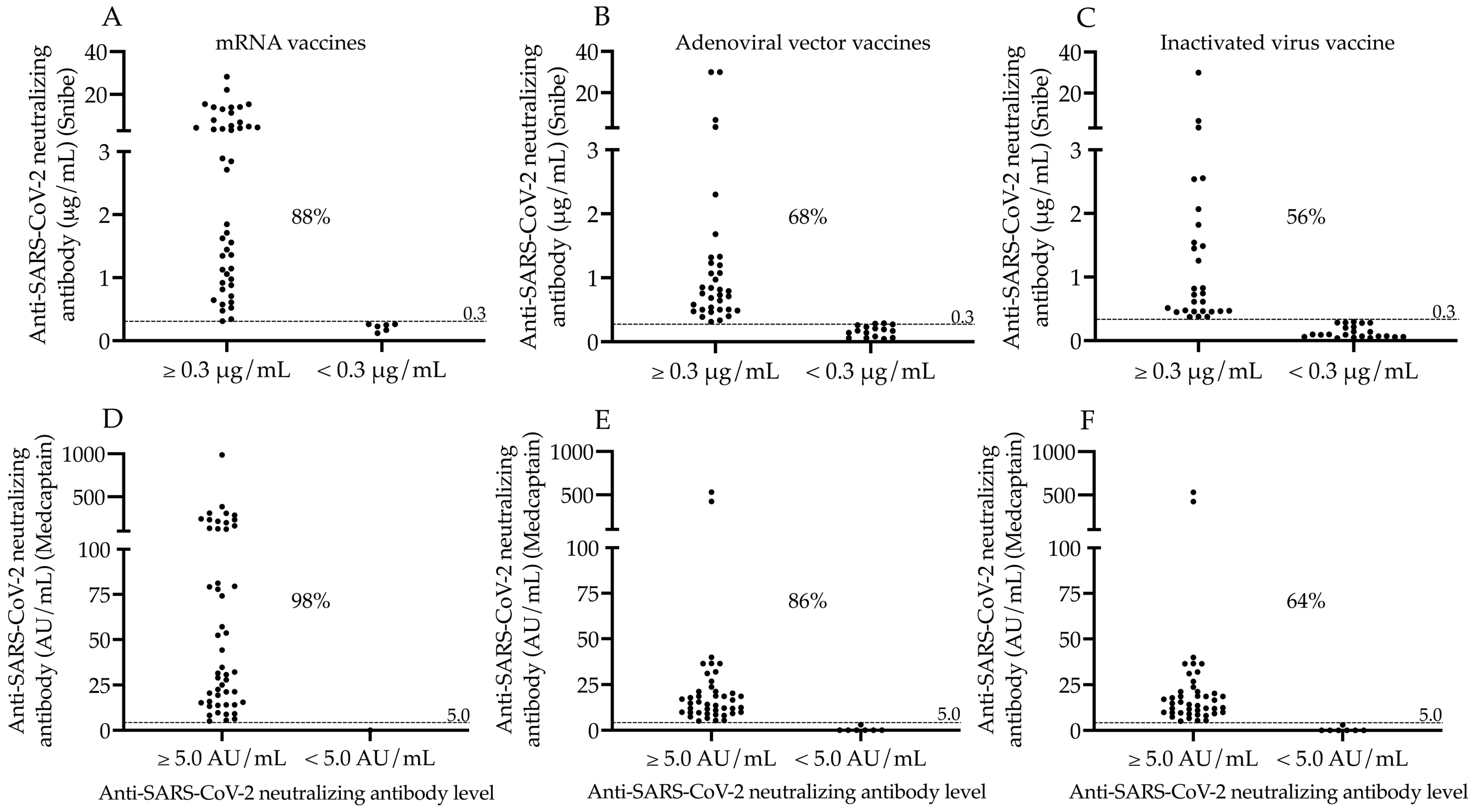
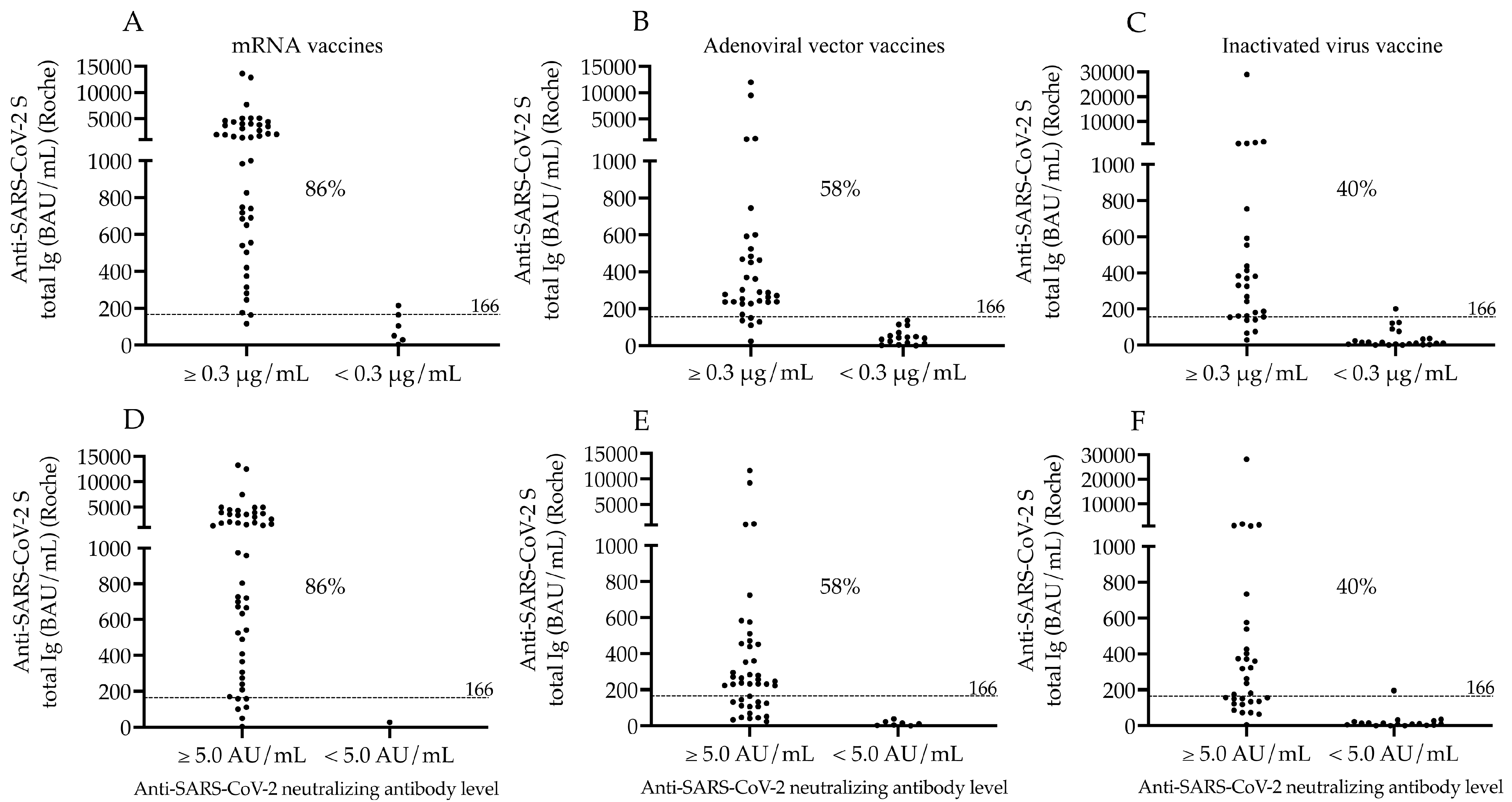
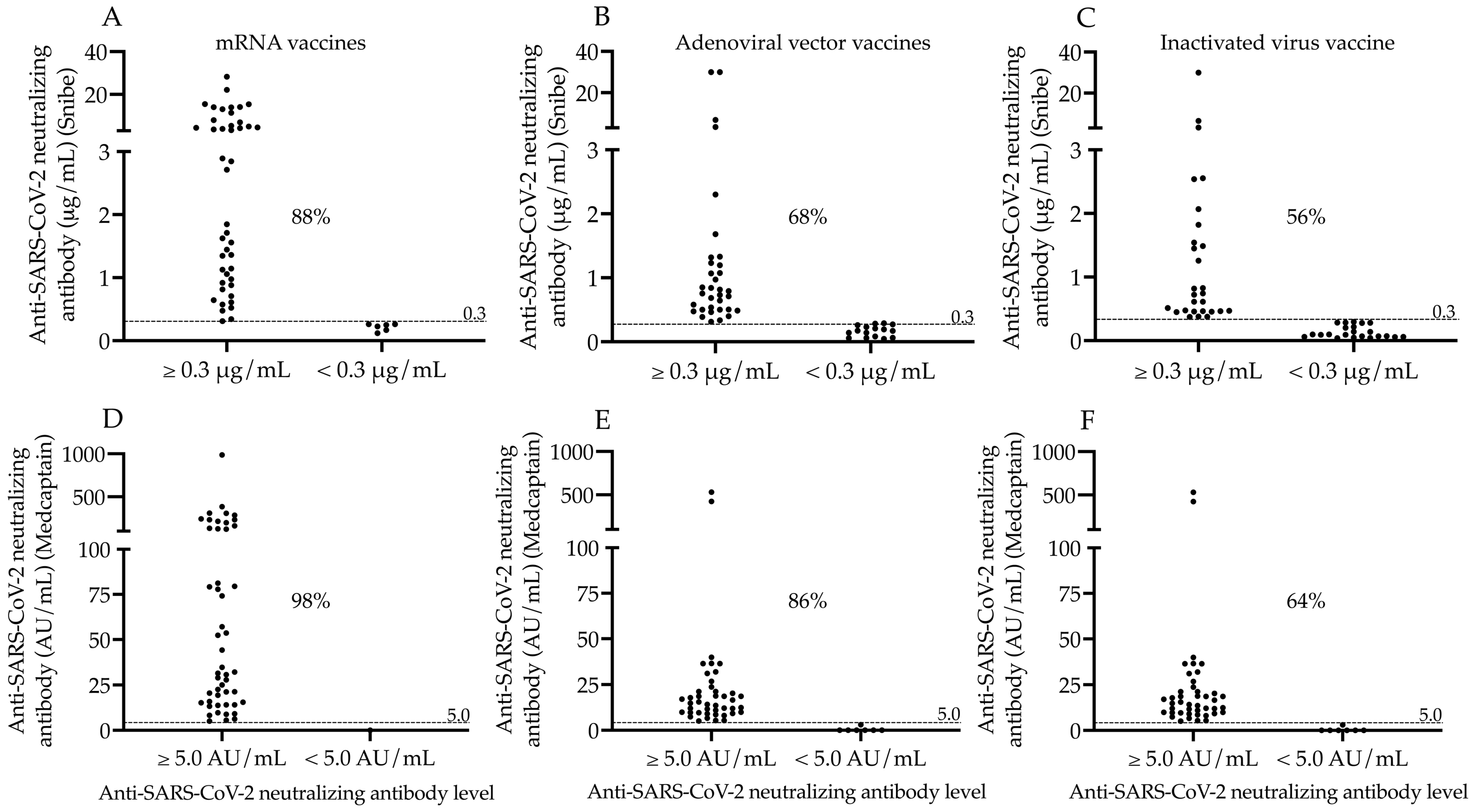
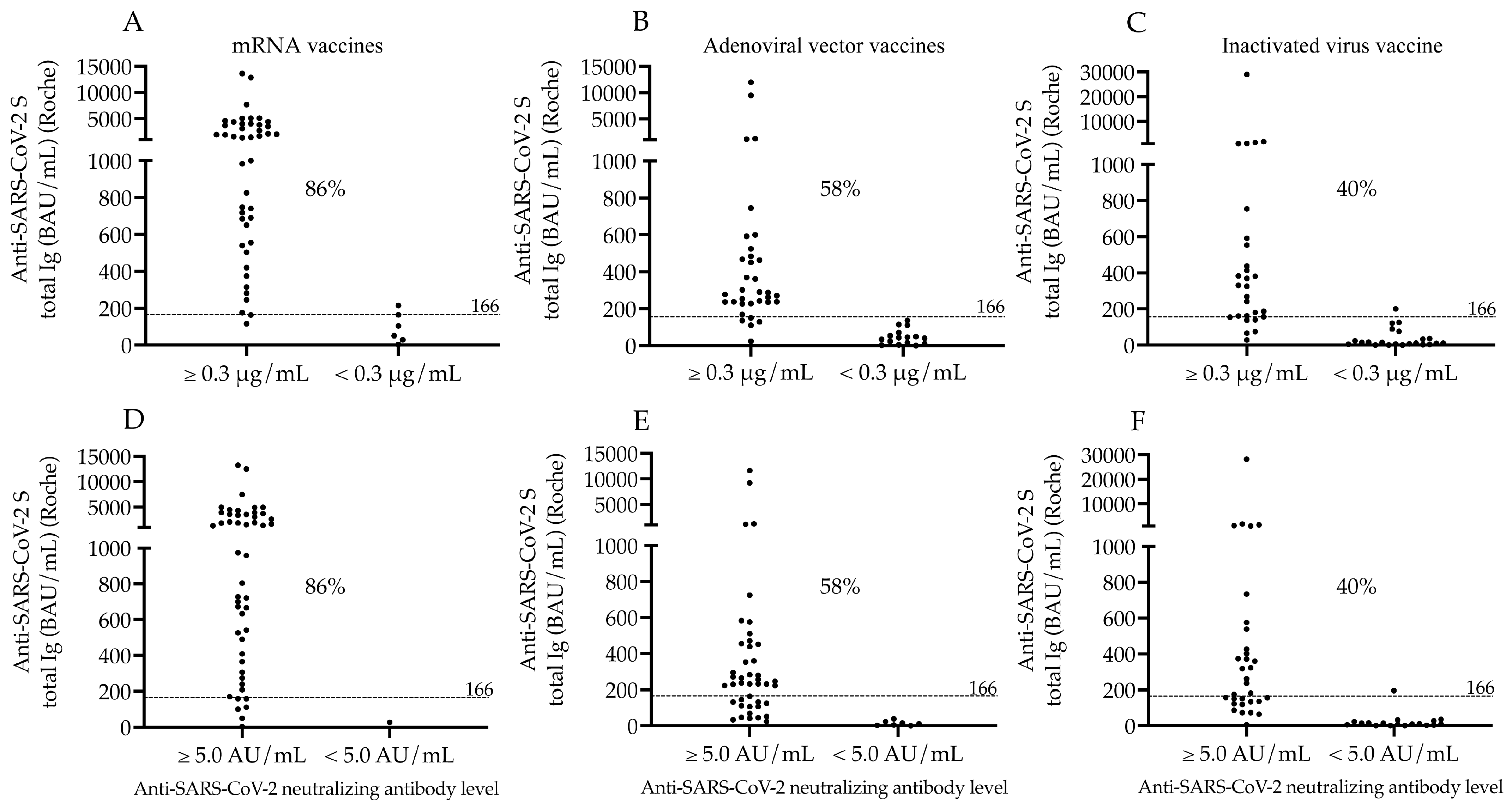
3.3. Ratio of Seropositivity after Two Doses of mRNA, Adenoviral Vector, and Inactivated Whole-Virus Vaccinations Based on Two Different Neutralization Tests
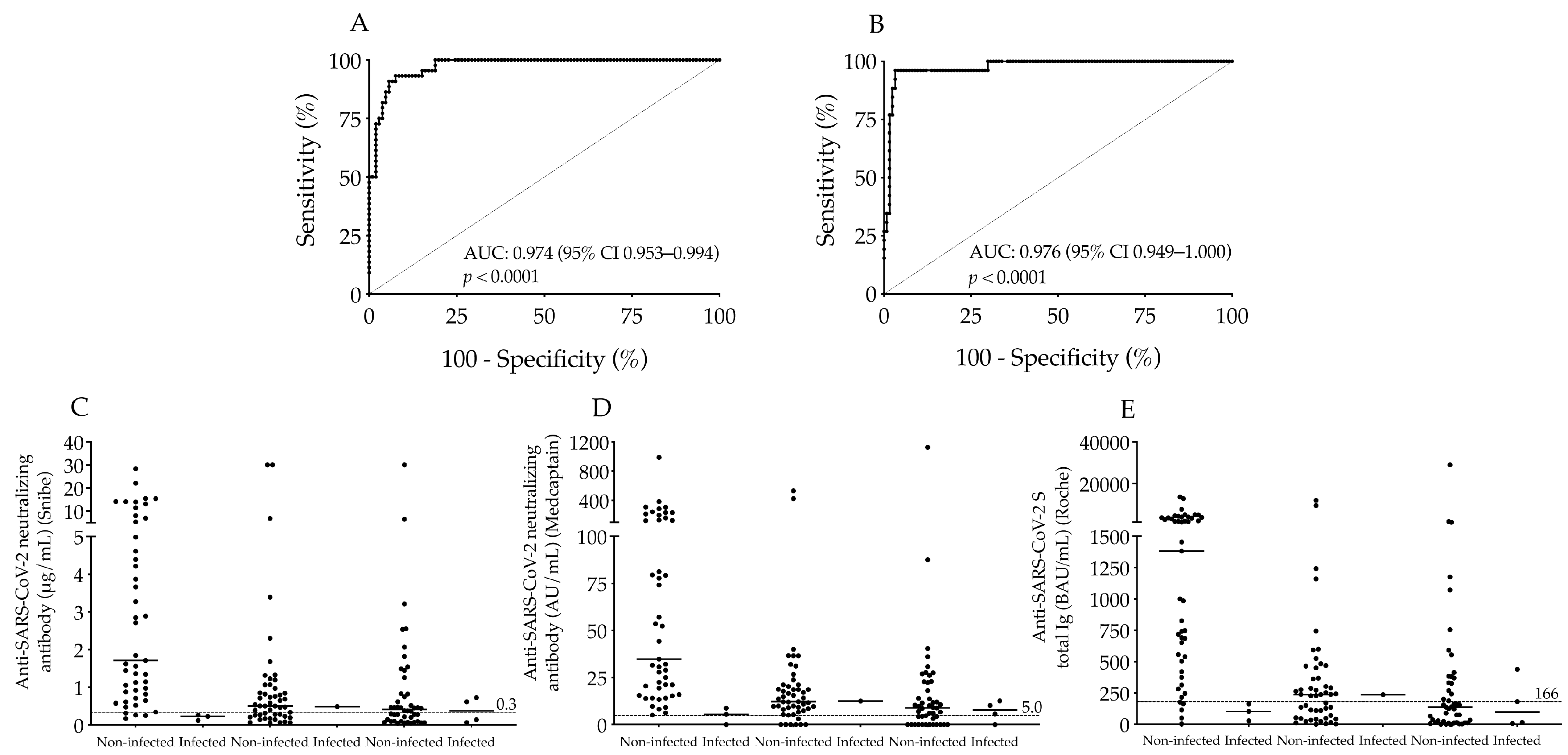
3.4. Analysis of Concordance among Serological Tests to Detect Seropositivity after Three Types of COVID-19 Vaccines
3.5. Follow-Up of Vaccinated Subjects for the Risk of SARS-CoV-2 Infection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valyi-Nagy, I.; Matula, Z.; Gonczi, M.; Tasnady, S.; Beko, G.; Reti, M.; Ajzner, E.; Uher, F. Comparison of antibody and T cell responses elicited by BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) vaccines against SARS-CoV-2 in healthy adult humans. Geroscience 2021, 43, 2321–2331. [Google Scholar] [CrossRef] [PubMed]
- Bonelli, M.; Mrak, D.; Tobudic, S.; Sieghart, D.; Mandl, P.; Kornek, B.; Simader, E.; Koblischke, M.; Radner, H.; Perkmann, T.; et al. Additional Heterologous versus Homologous Booster Vaccination in Immunosuppressed Patients Without SARS-CoV-2 Antibody Seroconversion After Primary mRNA Vaccination: A Randomized Controlled Trial. Arthritis Rheumatol. 2021, 73, 4125–4126. [Google Scholar] [CrossRef] [PubMed]
- Matula, Z.; Gonczi, M.; Beko, G.; Kadar, B.; Ajzner, E.; Uher, F.; Valyi-Nagy, I. Antibody and T Cell Responses against SARS-CoV-2 Elicited by the Third Dose of BBIBP-CorV (Sinopharm) and BNT162b2 (Pfizer-BioNTech) Vaccines Using a Homologous or Heterologous Booster Vaccination Strategy. Vaccines 2022, 10, 539. [Google Scholar] [CrossRef] [PubMed]
- Rakoczi, E.; Magocs, G.; Kovacs, S.; Nagy, B., Jr.; Szucs, G.; Szekanecz, Z. Evaluation of the Efficacy of BBIBP-CorV Inactivated Vaccine Combined with BNT62b2 mRNA Booster Vaccine. Diagnostics 2023, 13, 556. [Google Scholar] [CrossRef]
- Mrak, D.; Sieghart, D.; Simader, E.; Tobudic, S.; Radner, H.; Mandl, P.; Goschl, L.; Koblischke, M.; Hommer, N.; Wagner, A.; et al. Heterologous vector versus homologous mRNA COVID-19 booster vaccination in non-seroconverted immunosuppressed patients: A randomized controlled trial. Nat. Commun. 2022, 13, 5362. [Google Scholar] [CrossRef]
- Hou, X.; Zaks, T.; Langer, R.; Dong, Y. Lipid nanoparticles for mRNA delivery. Nat. Reviews. Mater. 2021, 6, 1078–1094. [Google Scholar] [CrossRef]
- Mendonca, S.A.; Lorincz, R.; Boucher, P.; Curiel, D.T. Adenoviral vector vaccine platforms in the SARS-CoV-2 pandemic. NPJ Vaccines 2021, 6, 97. [Google Scholar] [CrossRef]
- Ndwandwe, D.; Wiysonge, C.S. COVID-19 vaccines. Curr. Opin. Immunol. 2021, 71, 111–116. [Google Scholar] [CrossRef]
- Moncunill, G.; Aguilar, R.; Ribes, M.; Ortega, N.; Rubio, R.; Salmeron, G.; Molina, M.J.; Vidal, M.; Barrios, D.; Mitchell, R.A.; et al. Determinants of early antibody responses to COVID-19 mRNA vaccines in a cohort of exposed and naive healthcare workers. EBioMedicine 2022, 75, 103805. [Google Scholar] [CrossRef]
- Broseta, J.J.; Rodriguez-Espinosa, D.; Rodriguez, N.; Mosquera, M.D.M.; Marcos, M.A.; Egri, N.; Pascal, M.; Soruco, E.; Bedini, J.L.; Bayes, B.; et al. Humoral and Cellular Responses to mRNA-1273 and BNT162b2 SARS-CoV-2 Vaccines Administered to Hemodialysis Patients. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2021, 78, 571–581. [Google Scholar] [CrossRef]
- Pham, M.N.; Murugesan, K.; Banaei, N.; Pinsky, B.A.; Tang, M.; Hoyte, E.; Lewis, D.B.; Gernez, Y. Immunogenicity and tolerability of COVID-19 messenger RNA vaccines in primary immunodeficiency patients with functional B-cell defects. J. Allergy Clin. Immunol. 2022, 149, 907–911.e903. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Mendizabal, M.; Ducasa, N.; Benencio, P.; Anders, M.; Cairo, F.; Barbero, M.; Etcheves, P.; Alter, A.; Scarton, G.; Abraldes, J.G.; et al. Heterologous adenovirus-vector/messenger RNA regimen is associated with improved severe acute respiratory syndrome coronavirus 2 humoral response in liver transplant recipients. Hepatol. Commun. 2022, 6, 2850–2859. [Google Scholar] [CrossRef]
- Rearte, A.; Castelli, J.M.; Rearte, R.; Fuentes, N.; Pennini, V.; Pesce, M.; Barbeira, P.B.; Iummato, L.E.; Laurora, M.; Bartolomeu, M.L.; et al. Effectiveness of rAd26-rAd5, ChAdOx1 nCoV-19, and BBIBP-CorV vaccines for risk of infection with SARS-CoV-2 and death due to COVID-19 in people older than 60 years in Argentina: A test-negative, case-control, and retrospective longitudinal study. Lancet 2022, 399, 1254–1264. [Google Scholar] [CrossRef]
- Pascuale, C.A.; Varese, A.; Ojeda, D.S.; Pasinovich, M.E.; Lopez, L.; Rossi, A.H.; Rodriguez, P.E.; Miglietta, E.A.; Mazzitelli, I.; Di Diego Garcia, F.; et al. Immunogenicity and reactogenicity of heterologous immunization against SARS CoV-2 using Sputnik V, ChAdOx1-S, BBIBP-CorV, Ad5-nCoV, and mRNA-1273. Cell Rep. Med. 2022, 3, 100706. [Google Scholar] [CrossRef]
- Sarker, P.; Akhtar, E.; Kuddusi, R.U.; Alam, M.M.; Haq, M.A.; Hosen, M.B.; Chanda, B.C.; Haque, F.; Alam, M.; Razzaque, A.; et al. Comparison of the Immune Responses to COVID-19 Vaccines in Bangladeshi Population. Vaccines 2022, 10, 1498. [Google Scholar] [CrossRef]
- Dashdorj, N.J.; Wirz, O.F.; Roltgen, K.; Haraguchi, E.; Buzzanco, A.S., 3rd; Sibai, M.; Wang, H.; Miller, J.A.; Solis, D.; Sahoo, M.K.; et al. Direct comparison of antibody responses to four SARS-CoV-2 vaccines in Mongolia. Cell Host Microbe 2021, 29, 1738–1743.e1734. [Google Scholar] [CrossRef]
- Al Qahtani, M.; Du, X.; Bhattacharyya, S.; Alawadi, A.; Al Mahmeed, H.; Al Sayed, J.; Justman, J.; El-Sadr, W.M.; Hidary, J.; Mukherjee, S. Post-vaccination outcomes in association with four COVID-19 vaccines in the Kingdom of Bahrain. Sci. Rep. 2022, 12, 9236. [Google Scholar] [CrossRef]
- Jeewandara, C.; Aberathna, I.S.; Danasekara, S.; Gomes, L.; Fernando, S.; Guruge, D.; Ranasinghe, T.; Gunasekera, B.; Kamaladasa, A.; Kuruppu, H.; et al. Comparison of the immunogenicity of five COVID-19 vaccines in Sri Lanka. Immunology 2022, 167, 263–274. [Google Scholar] [CrossRef]
- Adjobimey, T.; Meyer, J.; Sollberg, L.; Bawolt, M.; Berens, C.; Kovacevic, P.; Trudic, A.; Parcina, M.; Hoerauf, A. Comparison of IgA, IgG, and Neutralizing Antibody Responses Following Immunization With Moderna, BioNTech, AstraZeneca, Sputnik-V, Johnson and Johnson, and Sinopharm’s COVID-19 Vaccines. Front. Immunol. 2022, 13, 917905. [Google Scholar] [CrossRef]
- Lau, C.S.; Phua, S.K.; Liang, Y.L.; Oh, M.L.H.; Aw, T.C. SARS-CoV-2 Spike and Neutralizing Antibody Kinetics 90 Days after Three Doses of BNT162b2 mRNA COVID-19 Vaccine in Singapore. Vaccines 2022, 10, 331. [Google Scholar] [CrossRef] [PubMed]
- Lau, C.S.; Thundyil, J.; Oh, M.L.H.; Phua, S.K.; Liang, Y.L.; Li, Y.; Huo, J.; Huang, Y.; Zhang, B.; Xu, S.; et al. Neutralizing and Total/IgG Spike Antibody Responses Following Homologous CoronaVac vs. BNT162b2 Vaccination Up to 90 Days Post-Booster. Antibodies 2022, 11, 70. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Su, X.; Yu, G.; Yang, S.; Wang, F.; Huang, T.; Zhou, L.; Hui, Z.; Liao, Y.; Qiu, Y.; et al. An automated chemiluminescent immunoassay (CLIA) detects SARS-CoV-2 neutralizing antibody levels in COVID-19 patients and vaccinees. Int. J. Infect. Dis. IJID Off. Publ. Int. Soc. Infect. Dis. 2022, 115, 116–125. [Google Scholar] [CrossRef] [PubMed]
- Voko, Z.; Kiss, Z.; Surjan, G.; Surjan, O.; Barcza, Z.; Palyi, B.; Formanek-Balku, E.; Molnar, G.A.; Herczeg, R.; Gyenesei, A.; et al. Nationwide effectiveness of five SARS-CoV-2 vaccines in Hungary-the HUN-VE study. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2022, 28, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Shrotri, M.; Navaratnam, A.M.D.; Nguyen, V.; Byrne, T.; Geismar, C.; Fragaszy, E.; Beale, S.; Fong, W.L.E.; Patel, P.; Kovar, J.; et al. Spike-antibody waning after second dose of BNT162b2 or ChAdOx1. Lancet 2021, 398, 385–387. [Google Scholar] [CrossRef]
- Petrovic, V.; Vukovic, V.; Patic, A.; Markovic, M.; Ristic, M. Immunogenicity of BNT162b2, BBIBP-CorV and Gam-COVID-Vac vaccines and immunity after natural SARS-CoV-2 infection-A comparative study from Novi Sad, Serbia. PLoS ONE 2022, 17, e0263468. [Google Scholar] [CrossRef]
- Seija, M.; Rammauro, F.; Santiago, J.; Orihuela, N.; Zulberti, C.; Machado, D.; Recalde, C.; Noboa, J.; Frantchez, V.; Astesiano, R.; et al. Comparison of antibody response to SARS-CoV-2 after two doses of inactivated virus and BNT162b2 mRNA vaccines in kidney transplant. Clin. Kidney J. 2022, 15, 527–533. [Google Scholar] [CrossRef]
- Ciampi, E.; Uribe-San-Martin, R.; Soler, B.; Garcia, L.; Guzman, J.; Pelayo, C.; Jurgensen, L.; Guzman, I.; Vera, F.; Galleguillos, L.; et al. Safety and humoral response rate of inactivated and mRNA vaccines against SARS-CoV-2 in patients with Multiple Sclerosis. Mult. Scler. Relat. Disord. 2022, 59, 103690. [Google Scholar] [CrossRef]
- Salvagno, G.L.; Henry, B.M.; di Piazza, G.; Pighi, L.; de Nitto, S.; Bragantini, D.; Gianfilippi, G.L.; Lippi, G. Anti-spike S1 IgA, anti-spike trimeric IgG, and anti-spike RBD IgG response after BNT162b2 COVID-19 mRNA vaccination in healthcare workers. J. Med. Biochem. 2021, 40, 327–334. [Google Scholar] [CrossRef]
- Padoan, A.; Cosma, C.; Bonfante, F.; Rocca, F.D.; Barbaro, F.; Santarossa, C.; Dall’Olmo, L.; Pagliari, M.; Bortolami, A.; Cattelan, A.; et al. SARS-CoV-2 neutralizing antibodies after one or two doses of Comirnaty (BNT162b2, BioNTech/Pfizer): Kinetics and comparison with chemiluminescent assays. Clin. Chim. Acta Int. J. Clin. Chem. 2021, 523, 446–453. [Google Scholar] [CrossRef]
- Malipiero, G.; D’Agaro, P.; Segat, L.; Moratto, A.; Villalta, D. Long-term decay of anti-RBD IgG titers after BNT162b2 vaccination is not mirrored by loss of neutralizing bioactivity against SARS-CoV-2. Clin. Chim. Acta Int. J. Clin. Chem. 2022, 524, 11–17. [Google Scholar] [CrossRef]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Cromer, D.; Steain, M.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Kent, S.J.; Triccas, J.A.; Khoury, D.S.; Davenport, M.P. Neutralising antibody titres as predictors of protection against SARS-CoV-2 variants and the impact of boosting: A meta-analysis. Lancet. Microbe 2022, 3, e52–e61. [Google Scholar] [CrossRef]
- Pieri, M.; Infantino, M.; Manfredi, M.; Nuccetelli, M.; Grossi, V.; Lari, B.; Tomassetti, F.; Sarubbi, S.; Russo, E.; Amedei, A.; et al. Performance evaluation of four surrogate Virus Neutralization Tests (sVNTs) in comparison to the in vivo gold standard test. Front. Biosci. Landmark 2022, 27, 74. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | mRNA Vaccines (n = 50) | Adenoviral Vector Vaccines (n = 50) | Inactivated Whole-Virus Vaccine (n = 50) |
|---|---|---|---|
| Age (years), median (IQR) | 61.1 (48.9–70.3) | 53.6 (47.8–62.4) | 63.6 (46.7–66.5) |
| Sex (female/male), n/n | 35/15 | 26/24 | 30/20 |
| Elapsed time between 2nd dose and serology (days), median (IQR) | 36 (22–62) | 36 (25–53) | 47 (21–67) |
| Hypertension, n | 24 | 24 | 29 |
| Cardiovascular disease, n | 6 | 5 | 4 |
| Diabetes mellitus, n | 6 | 6 | 9 |
| Chronic renal disorder, n | 5 | 7 | 6 |
| Autoimmune disease, n | 4 | 4 | 3 |
| Lung disease, n | 1 | 1 | 2 |
| Thyroid disorder, n | 2 | 3 | 2 |
| Comparisons | Agreement | Cohen’s Kappa [95% CI] | p Value |
|---|---|---|---|
| Snibe-Roche (all vaccination groups) | 87.3% | 0.722 [0.566–0.878] | <0.0001 |
| Snibe-Roche (mRNA) | 94.0% | 0.735 [0.458–1.000] | <0.0001 |
| Snibe-Roche (adenoviral vector) | 88.0% | 0.749 [0.481–1.000] | <0.0001 |
| Snibe-Roche (inactivated whole-virus) | 80.0% | 0.609 [0.346–0.872] | <0.0001 |
| Medcaptain-Roche (all vaccination groups) | 76.7% | 0.458 [0.320–0.595] | <0.0001 |
| Medcaptain-Roche (mRNA) | 88.0% | 0.229 [0.048–0.397] | 0.0061 |
| Medcaptain-Roche (adenoviral vector) | 70.0% | 0.343 [0.134–0.552] | 0.0006 |
| Medcaptain-Roche (inactivated whole-virus) | 72.0% | 0.469 [0.222–0.716] | 0.0001 |
| Snibe-Medcaptain (all vaccination groups) | 86.7% | 0.635 [0.483–0.785] | <0.0001 |
| Snibe-Medcaptain (mRNA) | 90.0% | 0.261 [0.073–0.447] | 0.0031 |
| Snibe-Medcaptain (adenoviral vector) | 82.0% | 0.514 [0.271–0.756] | <0.0001 |
| Snibe-Medcaptain (inactivated whole-virus) | 88.0% | 0.752 [0.478–1.000] | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Csoma, E.; Nagy Koroknai, Á.; Sütő, R.; Szakács Szilágyi, E.; Pócsi, M.; Nagy, A.; Bíró, K.; Kappelmayer, J.; Nagy, B., Jr. Evaluation of the Diagnostic Performance of Two Automated SARS-CoV-2 Neutralization Immunoassays following Two Doses of mRNA, Adenoviral Vector, and Inactivated Whole-Virus Vaccinations in COVID-19 Naïve Subjects. Microorganisms 2023, 11, 1187. https://doi.org/10.3390/microorganisms11051187
Csoma E, Nagy Koroknai Á, Sütő R, Szakács Szilágyi E, Pócsi M, Nagy A, Bíró K, Kappelmayer J, Nagy B Jr. Evaluation of the Diagnostic Performance of Two Automated SARS-CoV-2 Neutralization Immunoassays following Two Doses of mRNA, Adenoviral Vector, and Inactivated Whole-Virus Vaccinations in COVID-19 Naïve Subjects. Microorganisms. 2023; 11(5):1187. https://doi.org/10.3390/microorganisms11051187
Chicago/Turabian StyleCsoma, Eszter, Ágnes Nagy Koroknai, Renáta Sütő, Erika Szakács Szilágyi, Marianna Pócsi, Attila Nagy, Klára Bíró, János Kappelmayer, and Béla Nagy, Jr. 2023. "Evaluation of the Diagnostic Performance of Two Automated SARS-CoV-2 Neutralization Immunoassays following Two Doses of mRNA, Adenoviral Vector, and Inactivated Whole-Virus Vaccinations in COVID-19 Naïve Subjects" Microorganisms 11, no. 5: 1187. https://doi.org/10.3390/microorganisms11051187
APA StyleCsoma, E., Nagy Koroknai, Á., Sütő, R., Szakács Szilágyi, E., Pócsi, M., Nagy, A., Bíró, K., Kappelmayer, J., & Nagy, B., Jr. (2023). Evaluation of the Diagnostic Performance of Two Automated SARS-CoV-2 Neutralization Immunoassays following Two Doses of mRNA, Adenoviral Vector, and Inactivated Whole-Virus Vaccinations in COVID-19 Naïve Subjects. Microorganisms, 11(5), 1187. https://doi.org/10.3390/microorganisms11051187