

Factors Associated with Carriage of Enteropathogenic and Non-Enteropathogenic Viruses: A Reanalysis of Matched Case-Control Data from the AFRIBIOTA Site in Antananarivo, Madagascar

 , , , , , ,
, , , , , ,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design/Recruitment of Participants
2.2. Data Collection
2.3. Sample Collection
2.4. Extraction of Nucleic Acids
2.5. Real-Time PCR and RT-PCR (qPCR and RTqPCR)
2.6. Statistical Analysis
3. Results
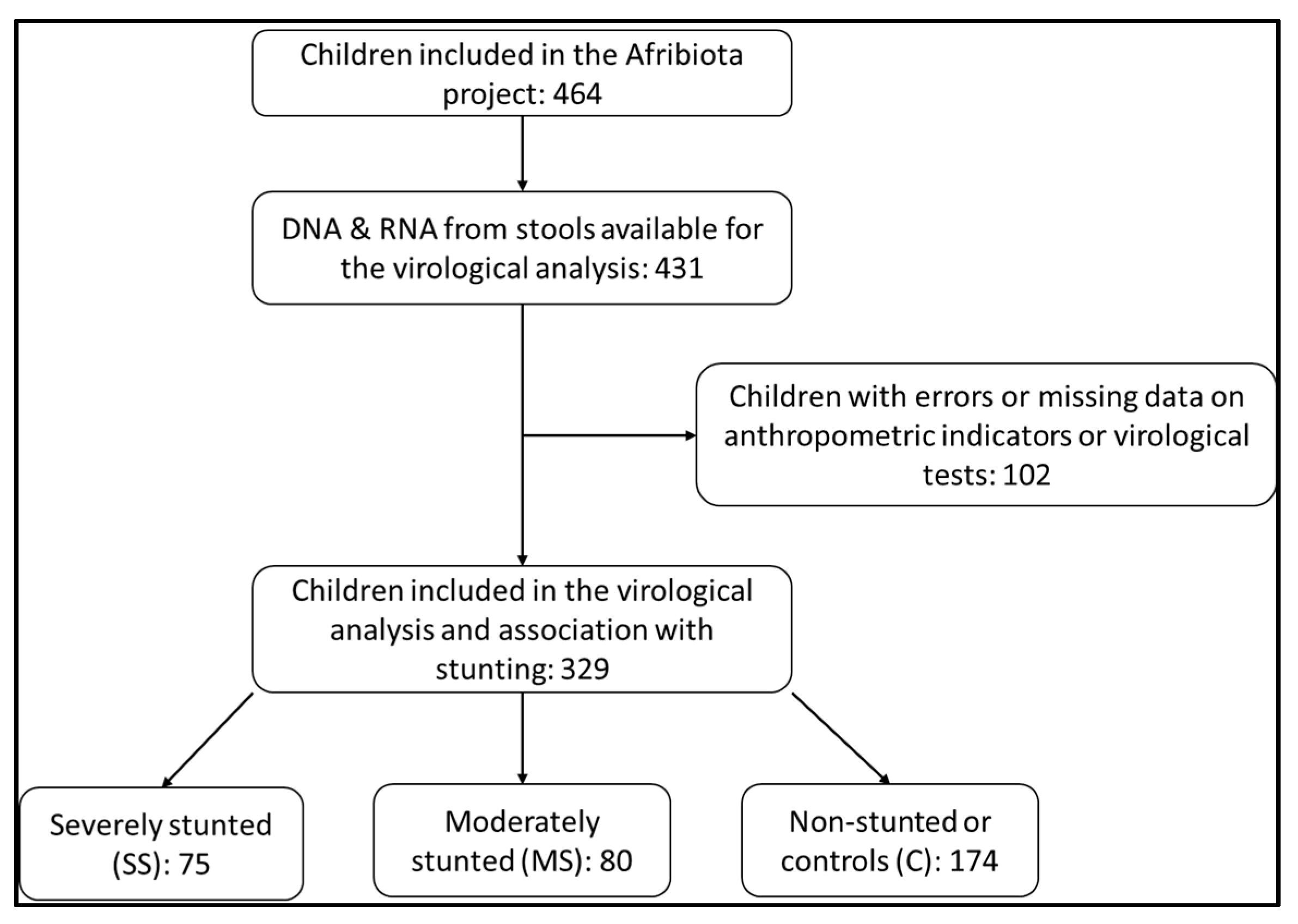
3.1. Description of the Study Population
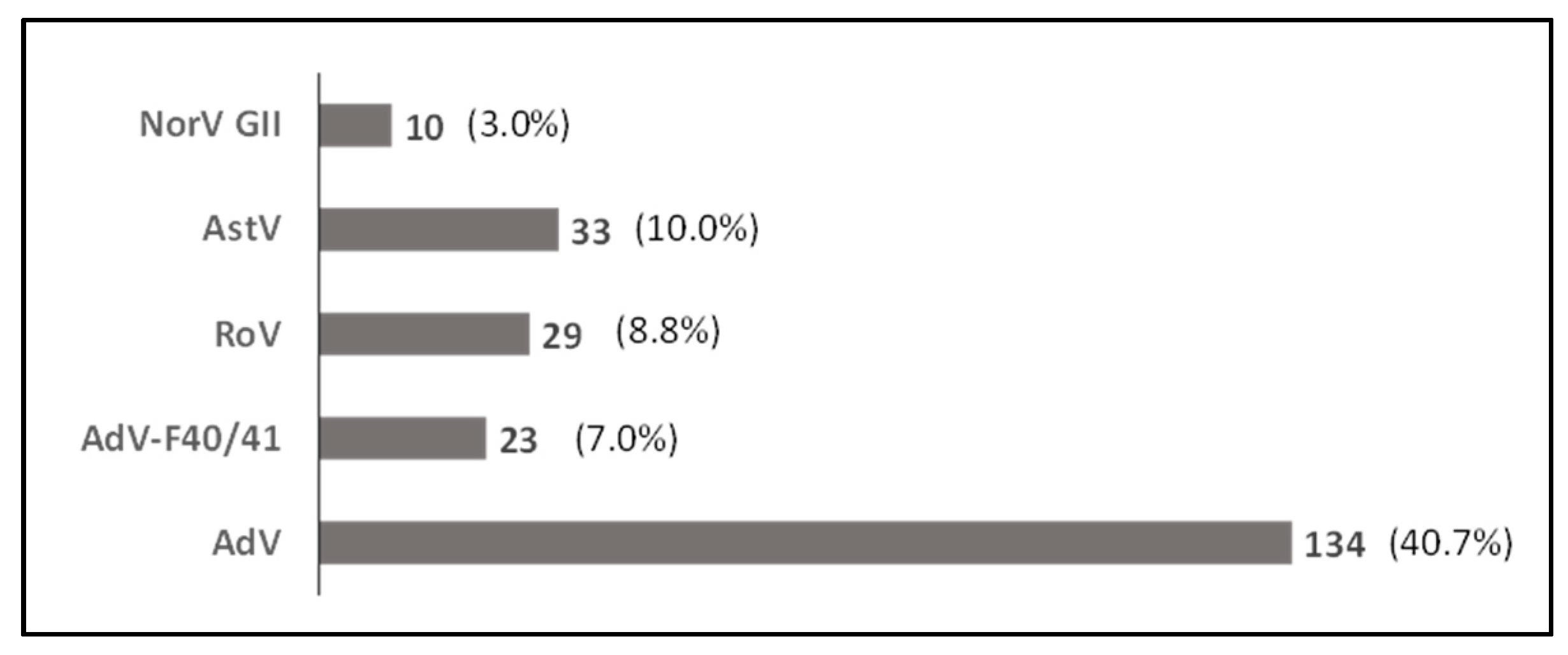
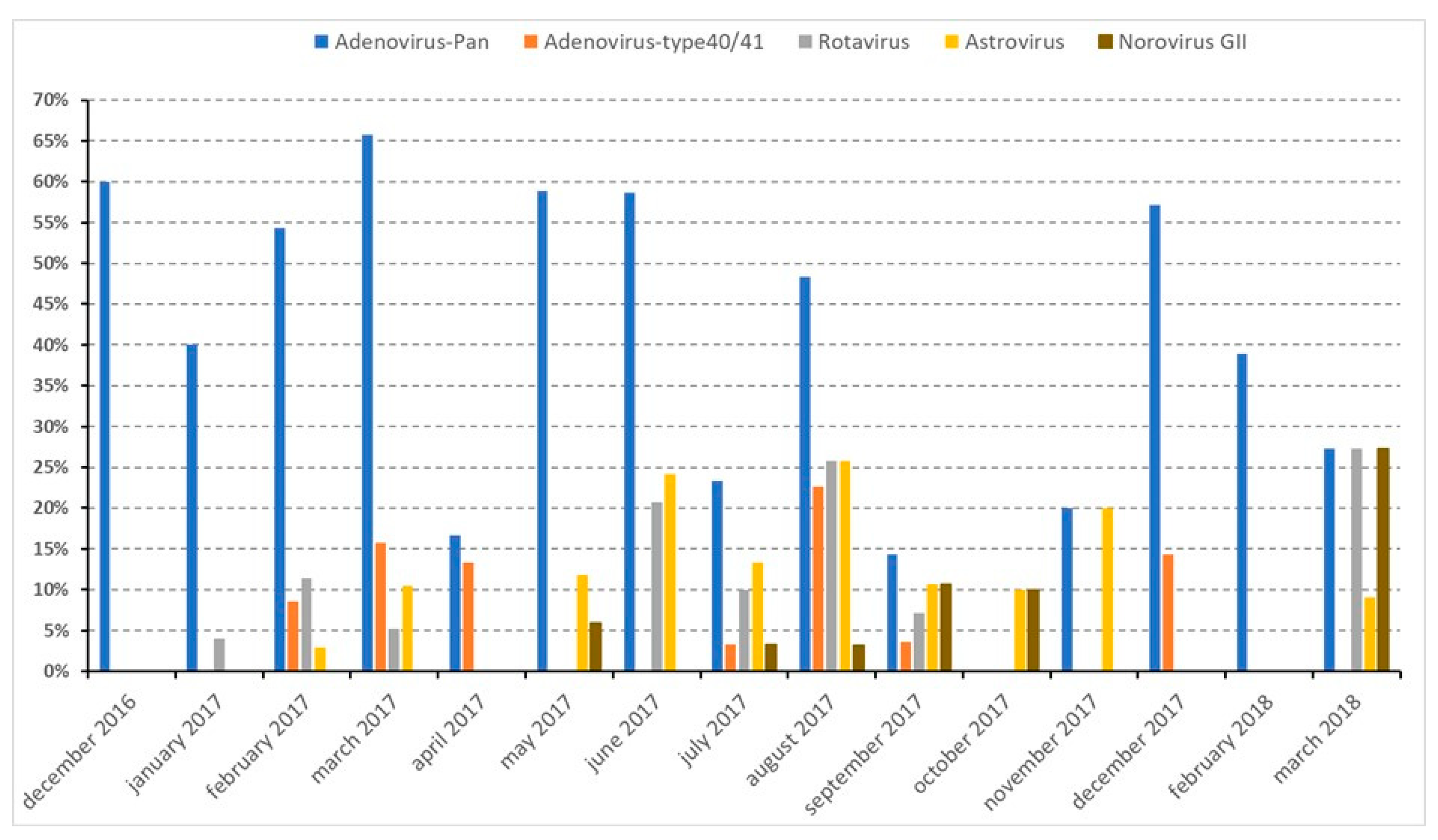
3.2. Detection of Viruses in the Study Population
3.3. Characteristics of the Study Population Associated with Viral Infection
3.4. Characteristics of the Household Environment of the Study Population and Viral Infection
3.5. Risk Factors and Protective Factors Associated with Viral Infection
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- The World Bank. World Bank Approves Second Phase of Nutrition Program to Reduce Child Stunting in Madagascar. Available online: https://www.worldbank.org/en/news/press-release/2022/07/13/world-bank-approves-second-phase-of-nutrition-program-to-reduce-child-stunting-in-madagascar (accessed on 17 April 2023).
- McKay, S.; Gaudier, E.; Campbell, D.I.; Prentice, A.M.; Albers, R. Environmental Enteropathy: New Targets for Nutritional Interventions. Int. Health 2010, 2, 172–180. [Google Scholar] [CrossRef] [PubMed]
- The World Bank. Reducing Child Stunting in Madagascar. 7 July 2021. Available online: https://www.worldbank.org/en/news/feature/2021/07/07/reducing-child-stunting-in-madagascar (accessed on 28 June 2023).
- Watanabe, K.; Petri, W.A., Jr. Environmental Enteropathy: Elusive but Significant Subclinical Abnormalities in Developing Countries. EBioMedicine 2016, 10, 25–32. [Google Scholar] [CrossRef]
- Tickell, K.D.; Atlas, H.E.; Walson, J.L. Environmental Enteric Dysfunction: A Review of Potential Mechanisms, Consequences and Management Strategies. BMC Med. 2019, 17, 181. [Google Scholar] [CrossRef] [PubMed]
- Collard, J.M.; Andrianonimiadana, L.; Habib, A.; Rakotondrainipiana, M.; Andriantsalama, P.; Randriamparany, R.; Rabenandrasana, M.A.N.; Weill, F.X.; Sauvonnet, N.; Randremanana, R.V.; et al. High Prevalence of Small Intestine Bacteria Overgrowth and Asymptomatic Carriage of Enteric Pathogens in Stunted Children in Antananarivo, Madagascar. PLoS Negl. Trop. Dis. 2022, 16, e0009849. [Google Scholar] [CrossRef]
- Agus, S.G.; Dolin, R.; Wyatt, R.G.; Tousimis, A.J.; Northrup, R.S. Acute Infectious Nonbacterial Gastroenteritis: Intestinal Histopathology Histologic and Enzymatic Alterations During Illness Produced by the Norwalk Agent in Man. Ann. Intern. Med. 1973, 79, 18–25. [Google Scholar] [CrossRef]
- Crane, R.J.; Jones, K.D.J.; Trust, K.-W.; Programme, R.; Kilifi, K.; Berkley, J.A. Environmental Enteric Dysfunction: An Overview. Food Nutr. Bull. 2015, 36 (Suppl. S1), S76–S87. [Google Scholar] [CrossRef]
- Rodríguez-Lázaro, D.; Cook, N.; Ruggeri, F.M.; Sellwood, J.; Nasser, A.; Nascimento, M.S.J.; D’Agostino, M.; Santos, R.; Saiz, J.C.; Rzezutka, A.; et al. Virus Hazards from Food, Water and Other Contaminated Environments. FEMS Microbiol. Rev. 2012, 36, 786–814. [Google Scholar] [CrossRef] [PubMed]
- Vonaesch, P.; Randremanana, R.; Gody, J.C.; Collard, J.M.; Giles-Vernick, T.; Doria, M.; Vigan-Womas, I.; Rubbo, P.A.; Etienne, A.; Andriatahirintsoa, E.J.; et al. Identifying the Etiology and Pathophysiology Underlying Stunting and Environmental Enteropathy: Study Protocol of the AFRIBIOTA Project. BMC Pediatr. 2018, 18, 236. [Google Scholar] [CrossRef]
- Vonaesch, P.; Morien, E.; Andrianonimiadana, L.; Sanke, H.; Mbecko, J.R.; Huus, K.E.; Naharimanananirina, T.; Gondje, B.P.; Nigatoloum, S.N.; Vondo, S.S.; et al. Stunted Childhood Growth Is Associated with Decompartmentalization of the Gastrointestinal Tract and Overgrowth of Oropharyngeal Taxa. Proc. Natl. Acad. Sci. USA 2018, 115, E8489–E8498. [Google Scholar] [CrossRef]
- Vonaesch, P.; Djorie, S.G.; Kandou, K.J.E.; Rakotondrainipiana, M.; Schaeffer, L.; Andriatsalama, P.V.; Randriamparany, R.; Gondje, B.P.; Nigatoloum, S.; Vondo, S.S.; et al. Factors Associated with Stunted Growth in Children Under Five Years in Antananarivo, Madagascar and Bangui, Central African Republic. Matern. Child Health J. 2021, 25, 1626–1637. [Google Scholar] [CrossRef]
- Habib, A.; Andrianonimiadana, L.; Rakotondrainipiana, M.; Andriantsalama, P.; Randriamparany, R.; Randremanana, R.V.; Rakotoarison, R.; Vigan-Womas, I.; Rafalimanantsoa, A.; Vonaesch, P.; et al. High Prevalence of Intestinal Parasite Infestations among Stunted and Control Children Aged 2 to 5 Years Old in Two Neighborhoods of Antananarivo, Madagascar. PLoS Negl. Trop. Dis. 2021, 15, e0009333. [Google Scholar] [CrossRef] [PubMed]
- Andersson, M.E.; Elfving, K.; Shakely, D.; Nilsson, S.; Msellem, M.; Trollfors, B.; Mårtensson, A.; Björkman, A.; Lindh, M. Rapid Clearance and Frequent Reinfection with Enteric Pathogens among Children with Acute Diarrhea in Zanzibar. Clin. Infect. Dis. 2017, 65, 1371–1377. [Google Scholar] [CrossRef] [PubMed]
- Okitsu, S.; Khamrin, P.; Takanashi, S.; Thongprachum, A.; Hoque, S.A.; Takeuchi, H.; Khan, M.A.; Hasan, S.M.T.; Iwata, T.; Shimizu, H.; et al. Molecular Detection of Enteric Viruses in the Stool Samples of Children without Diarrhea in Bangladesh. Infect. Genet. Evol. 2020, 77, 104055. [Google Scholar] [CrossRef] [PubMed]
- Karst, S.M. Viral Safeguard: The Enteric Virome Protects against Gut Inflammation. Immunity 2016, 44, 715–718. [Google Scholar] [CrossRef]
- Rogawski, E.T.; Liu, J.; Platts-Mills, J.A.; Kabir, F.; Lertsethtakarn, P.; Siguas, M.; Khan, S.S.; Praharaj, I.; Murei, A.; Nshama, R.; et al. Use of Quantitative Molecular Diagnostic Methods to Investigate the Effect of Enteropathogen Infections on Linear Growth in Children in Low-Resource Settings: Longitudinal Analysis of Results from the MAL-ED Cohort Study. Lancet Glob. Health 2018, 6, e1319–e1328. [Google Scholar] [CrossRef]
- Praharaj, I.; Revathy, R.; Bandyopadhyay, R.; Benny, B.; Ko, M.A.; Liu, J.; Houpt, E.R.; Kang, G. Enteropathogens and Gut Inflammation in Asymptomatic Infants and Children in Different Environments in Southern India. Am. J. Trop. Med. Hyg. 2018, 98, 576–580. [Google Scholar] [CrossRef]
- Lee, B.; Damon, C.F.; Platts-Mills, J.A. Pediatric Acute Gastroenteritis Associated with Adenovirus 40/41 in Low-Income and Middle-Income Countries. Curr. Opin. Infect. Dis. 2020, 33, 398–403. [Google Scholar] [CrossRef]
- Alsved, M.; Fraenkel, C.J.; Bohgard, M.; Widell, A.; Söderlund-Strand, A.; Lanbeck, P.; Holmdahl, T.; Isaxon, C.; Gudmundsson, A.; Medstrand, P.; et al. Sources of Airborne Norovirus in Hospital Outbreaks. Clin. Infect. Dis. 2020, 70, 2023–2028. [Google Scholar] [CrossRef]
- Blyn, L.B.; Hall, T.A.; Libby, B.; Ranken, R.; Sampath, R.; Rudnick, K.; Moradi, E.; Desai, A.; Metzgar, D.; Russell, K.L.; et al. Rapid Detection and Molecular Serotyping of Adenovirus by Use of PCR Followed by Electrospray Ionization Mass Spectrometry. J. Clin. Microbiol. 2008, 46, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Razafindratsimandresy, R.; Heraud, J.M.; Ramarokoto, C.E.; Rabemanantsoa, S.; Randremanana, R.; Andriamamonjy, N.S.; Richard, V.; Reynes, J.M. Rotavirus Genotypes in Children in the Community with Diarrhea in Madagascar. J. Med. Virol. 2013, 85, 1652–1660. [Google Scholar] [CrossRef]
- Papaventsis, D.C.; Dove, W.; Cunliffe, N.A.; Nakagomi, O.; Combe, P.; Grosjean, P.; Hart, C.A. Norovirus infection in children with acute gastroenteritis, Madagascar, 2004–2005. Emerg. Infect. Dis. 2007, 13, 908–911. [Google Scholar] [CrossRef]
- Papaventsis, D.C.; Dove, W.; Cunliffe, N.A.; Nakagomi, O.; Combe, P.; Grosjean, P.; Hart, C.A. Human Astrovirus gastroenteritis in children, Madagascar, 2004–2005. Emerg. Infect. Dis. 2007, 14, 844–846. [Google Scholar] [CrossRef] [PubMed]
- Randremanana, R.V.; Razafindratsimandresy, R.; Andriatahina, T.; Randriamanantena, A.; Ravelomanana, L.; Randrianirina, F.; Richard, V. Etiologies, Risk Factors and Impact of Severe Diarrhea in the under-Fives in Moramanga and Antananarivo, Madagascar. PLoS ONE 2016, 11, e0158862. [Google Scholar] [CrossRef] [PubMed]
- Randrianarisoa, M.M.; Rakotondrainipiana, M.; Randriamparany, R.; Andriantsalama, P.V.; Randrianarijaona, A.; Habib, A.; Robinson, A.; Raharimalala, L.; Hunald, F.A.; Etienne, A.; et al. Factors associated with anaemia among preschool- age children in underprivileged neighbourhoods in Antananarivo, Madagascar. BMC Public Health 2022, 22, 1320. [Google Scholar] [CrossRef] [PubMed]
- WHO Multicentre growth reference study group. WHO Child Growth Standards based on length/height, weight and age. Acta Paediatr. Int. J. Paediatr. 2006, 95 (Suppl. S450), 76–85. [Google Scholar]
- Prendergast, A.J.; Kelly, P. Interactions between Intestinal Pathogens, Enteropathy and Malnutrition in Developing Countries. Curr. Opin. Infect. Dis. 2016, 29, 229–236. [Google Scholar] [CrossRef]
- The MAL-ED Network Investigators; Acosta, A.M.; Chavez, C.B.; Flores, J.T.; Olotegui, M.P.; Pinedo, S.R.; Trigoso, D.R.; Vasquez, A.O.; Ahmed, I.; Alam, D.; et al. The MAL-ED Study: A Multinational and Multidisciplinary Approach to Understand the Relationship between Enteric Pathogens, Malnutrition, Gut Physiology, Physical Growth, Cognitive Development, and Immune Responses in Infants and Children up to 2 Years of Age in Resource-Poor Environments. Clin. Infect. Dis. 2014, 59, S193–S206. [Google Scholar] [CrossRef]
- Verkerke, H.; Sobuz, S.; Ma, J.Z.; Petri, S.E.; Reichman, D.; Qadri, F.; Rahman, M.; Haque, R.; Petri, W.A. Malnutrition Is Associated with Protection from Rotavirus Diarrhea: Evidence from a Longitudinal Birth Cohort Study in Bangladesh. J. Clin. Microbiol. 2016, 54, 2568–2574. [Google Scholar] [CrossRef]
- George, C.M.; Oldja, L.; Biswas, S.; Perin, J.; Lee, G.O.; Kosek, M.; Sack, R.B.; Ahmed, S.; Haque, R.; Parvin, T.; et al. Geophagy Is Associated with Environmental Enteropathy and Stunting in Children in Rural Bangladesh. Am. J. Tropl. Med. Hyg. 2015, 92, 1117–1124. [Google Scholar] [CrossRef]
- Shivoga, W.A.; Moturi, W.N. Geophagia as a Risk Factor for Diarrhoea. J. Infect. Dev. Ctries. 2009, 3, 94–98. [Google Scholar]
- Jhanji, V.; Chan, T.C.Y.; Li, E.Y.M.; Agarwal, K.; Vajpayee, R.B. Adenoviral Keratoconjunctivitis. Surv. Ophthalmol. 2015, 60, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Midha, A.; Ebner, F.; Schlosser-Brandenburg, J.; Rausch, S.; Hartmann, S. Trilateral Relationship: Ascaris, Microbiota, and Host Cells. Trends Parasitol. 2021, 37, 251–262. [Google Scholar] [CrossRef]
- Desai, P.; Diamond, M.S.; Thackray, L.B. Helminth—virus interactions: Determinants of coinfection outcomes. Gut Microbes 2021, 13, e1961202. [Google Scholar] [CrossRef]
- Osborne, L.C.; Monticelli, L.A.; Nice, T.J.; Sutherland, T.E.; Siracusa, M.C.; Hepworth, M.R.; Tomov, V.T.; Kobuley, D.; Tran, S.S.; Bittinger, K.; et al. Virus-helminth co-infection reveals a microbiota-independent mechanism of immune-modulation. Science 2014, 345, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Afrad, M.H.; Avzun, T.; Haque, J.; Haque, W.; Hossain, M.E.; Rahman, A.R.; Ahmed, S.; Faruque, A.S.G.; Rahman, M.Z.; Rahman, M. Detection of enteric- and non-enteric adenoviruses in gastroenteritis patients, Bangladesh, 2012–2015. J. Med. Virol. 2018, 90, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Kumthip, K.; Khamrin, P.; Ushijima, H.; Maneekarn, N. Enteric and non-enteric adenoviruses associated with acute gastroenteritis in pediatric patients in Thailand, 2011 to 2017. PLoS ONE 2019, 14, e0220263. [Google Scholar] [CrossRef]
- De Francesco, M.A.; Lorenzin, G.; Meini, A.; Schumacher, R.F.; Caruso, A. Non-enteric Adenoviruses Associated with Gastroenteritis in Hospitalized Children. Microbiol. Spectr. 2021, 9, e0030021. [Google Scholar] [CrossRef] [PubMed]
- Razanajatovo, N.H.; Richard, V.; Hoffmann, J.; Reynes, J.M.; Razafitrimo, G.M.; Randremanana, R.V.; Heraud, J.M. Viral Etiology of Influenza-like Illnesses in Antananarivo, Madagascar, July 2008 to June 2009. PLoS ONE 2011, 6, e17579. [Google Scholar] [CrossRef]
- Razafindratsimandresy, R.; Joffret, M.L.; Andriamandimby, S.F.; Andriamamonjy, S.; Rabemanantsoa, S.; Richard, V.; Delpeyroux, F.; Heraud, J.M.; Bessaud, M. Enterovirus Detection in Different Regions of Madagascar Reveals a Higher Abundance of Enteroviruses of Species C in Areas Where Several Outbreaks of Vaccine-Derived Polioviruses Occurred. BMC Infect. Dis. 2022, 22, 821. [Google Scholar] [CrossRef]
- Rakotonirainy, N.H.; Razafindratovo, V.; Remonja, C.R.; Rasoloarijaona, R.; Piola, P. Dietary diversity of 6- to 59-month-old children in rural areas of Moramanga and Morondava districts, Madagascar. PLoS ONE 2018, 13, e0200235. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Virus 1 | NS 2 N1 (%) | MS 2 N2 (%) | SS 2 N3 (%) | Total N = 329 | p-Value 3 |
|---|---|---|---|---|---|
| AdV | 75 (43.1) | 27 (33.7) | 32 (42.7) | 134 (40.7) | 0.344 |
| AdV type F40/41 | 15 (8.6) | 4 (5) | 4 (5.3) | 23 (7) | 0.551 |
| AstV | 14 (8) | 10 (12.5) | 9 (12) | 33 (10) | 0.444 |
| RoV | 14 (8) | 4 (5) | 11 (14.7) | 29 (8.8) | 0.115 |
| NorV GII | 5 (2.9) | 1 (1.25) | 4 (5.3) | 10 (3) | 0.350 |
| Variable | Viral Detection | Total (N = 329) | p-Value | |
|---|---|---|---|---|
| No (N = 159) | Yes (N = 170) | |||
| n (%)/Median [IQR] | n (%)/Median [IQR] | n/Median [IQR] | ||
| Sex | 0.362 1 | |||
| Female | 79 (45.9%) | 93 (54.1%) | 172 | |
| Male | 80 (51.0%) | 77 (49.0%) | 157 | |
| Age (months) | 44.28 [34.8–53.1] | 42.131 [33.0–52.2] | 43.232 [33.7–53.0] | 0.256 2 |
| Weight at birth | 0.085 3 | |||
| Mean (SD) | 3.167 (0.668) | 3.356 (0.681) | 3.269 (0.680) | |
| Standard deviation | 1.750–5.000 | 1.900–4.900 | 1.750–5.000 | |
| Food diversity score (child) | 0.035 1 | |||
| Inadequacy/insufficiency | 53 (41.1%) | 76 (58.9%) | 129 | |
| Acceptable | 106 (53.0%) | 94 (47.0%) | 200 | |
| Growth status | 0.352 1 | |||
| Moderately stunted | 44 (55.0%) | 36 (45.0%) | 80 | |
| Severely stunted | 33 (44.0%) | 42 (56.0%) | 75 | |
| Non-stunted | 82 (47.1%) | 92 (52.9%) | 174 | |
| Chronic malnutrition | 0.941 1 | |||
| Moderate chronic malnutrition | 47 (49.5%) | 48 (50.5%) | 95 | |
| Acute chronic malnutrition | 37 (46.8%) | 42 (53.2%) | 79 | |
| Normal nutrition | 75 (48.4%) | 80 (51.6%) | 155 | |
| History of acute malnutrition | 1.000 4 | |||
| Yes | 5 (50.0%) | 5 (50.0%) | 10 | |
| No | 154 (48.3%) | 165 (51.7%) | 319 | |
| Diarrhea | 0.323 4 | |||
| Yes | 6 (66.7%) | 3 (33.3%) | 9 | |
| No | 153 (47.8%) | 167 (52.2%) | 320 | |
| History of diarrhea | 0.685 1 | |||
| Yes | 7 (53.8%) | 6 (46.2%) | 13 | |
| No | 152 (48.1%) | 164 (51.9%) | 316 | |
| Respiratory infection history | 0.176 4 | |||
| Yes | 2 (22.2%) | 7 (77.8%) | 9 | |
| No | 157 (49.1%) | 163 (50.9%) | 320 | |
| History of fever | 0.389 1 | |||
| Yes | 101 (46.3%) | 117 (53.7%) | 218 | |
| No | 56 (51.4%) | 53 (48.6%) | 109 | |
| Rotavirus vaccination | 0.354 1 | |||
| At least one dose | 149 (47.8%) | 163 (52.2%) | 312 | |
| Zero dose | 9 (60.0%) | 6 (40.0%) | 15 | |
| Stuffy nose | 0.608 1 | |||
| Yes | 84 (49.7%) | 85 (50.3%) | 169 | |
| No | 75 (46.9%) | 85 (53.1%) | 160 | |
| Rhinorrhea | 0.2141 | |||
| Yes | 105 (51.0%) | 101 (49.0%) | 206 | |
| No | 54 (43.9%) | 69 (56.1%) | 123 | |
| Cough | 0.301 1 | |||
| Yes | 63 (52.1%) | 58 (47.9%) | 121 | |
| No | 96 (46.2%) | 112 (53.8%) | 208 | |
| Number of children under 5-years old in the household | 1.0 [1.0–2.0] | 1.0 [1.0–2.0] | 1.0 [1.0–2.0] | 0.627 1 |
| Nutritional status of the mother | 0.006 2 | |||
| Normal | 106 (54.1%) | 90 (45.9%) | 196 | |
| Undernourished | 24 (51.1%) | 23 (48.9%) | 47 | |
| Overnourished | 24 (32.4%) | 50 (67.6%) | 74 | |
| Education level of the mother | 0.258 3 | |||
| No schooling | 3 (33.3%) | 6 (66.7%) | 9 | |
| Elementary school | 84 (53.8%) | 72 (46.2%) | 156 | |
| Secondary School | 58 (43.6%) | 75 (56.4%) | 133 | |
| High School or above | 12 (44.4%) | 15 (55.6%) | 27 | |
| Weaning age | 0.388 2 | |||
| ≤12 months | 19 (52.8%) | 17 (47.2%) | 36 | |
| 12–24 months | 28 (41.2%) | 40 (58.8%) | 68 | |
| ≥24 months | 97 (50.0%) | 97 (50.0%) | 194 | |
| Age at the introduction of first solid foods | 0.458 2 | |||
| <6 months | 43 (45.3%) | 52 (54.7%) | 95 | |
| ≥6 months | 115 (49.8%) | 116 (50.2%) | 231 | |
| Running water in the house | 0.695 2 | |||
| Yes | 21 (45.7%) | 25 (54.3%) | 46 | |
| No | 138 (48.8%) | 145 (51.2%) | 283 | |
| Water used for child hygiene | 1.000 3 | |||
| Running water and other water sources | 4 (50.0%) | 4 (50.0%) | 8 | |
| Running water only | 155 (48.4%) | 165 (51.6%) | 320 | |
| Water used for the child during the last 2 weeks | 1.000 3 | |||
| Running water | 157 (48.6%) | 166 (51.4%) | 323 | |
| Other water sources | 2 (40.0%) | 3 (60.0%) | 5 | |
| Drinking water treatment | 0.107 2 | |||
| No | 109 (45.6%) | 130 (54.4%) | 239 | |
| Yes | 50 (55.6%) | 40 (44.4%) | 90 | |
| Using soap in the household | 0.674 3 | |||
| Yes | 83 (50.3%) | 82 (49.7%) | 165 | |
| Sometimes | 73 (46.8%) | 83 (53.2%) | 156 | |
| No | 3 (37.5%) | 5 (62.5%) | 8 | |
| Washing the hands of the child | 0.527 3 | |||
| No hand washing | 0 (0.0%) | 2 (100.0%) | 2 | |
| Only with cold/hot water | 53 (48.2%) | 57 (51.8%) | 110 | |
| Sometimes with water and soap | 90 (50.3%) | 89 (49.7%) | 179 | |
| Always with water and soap | 16 (42.1%) | 22 (57.9%) | 38 | |
| Water used for child hygiene | 1.000 3 | |||
| Running water and other water sources | 4 (50.0%) | 4 (50.0%) | 8 | |
| Running water only | 155 (48.4%) | 165 (51.6%) | 320 | |
| Water used for the child during the last 2 weeks | 1.000 3 | |||
| Running water | 157 (48.6%) | 166 (51.4%) | 323 | |
| Other water sources | 2 (40.0%) | 3 (60.0%) | 5 | |
| Drinking water treatment | 0.107 2 | |||
| No | 109 (45.6%) | 130 (54.4%) | 239 | |
| Yes | 50 (55.6%) | 40 (44.4%) | 90 | |
| Using soap in the household | 0.674 3 | |||
| Yes | 83 (50.3%) | 82 (49.7%) | 165 | |
| Sometimes | 73 (46.8%) | 83 (53.2%) | 156 | |
| No | 3 (37.5%) | 5 (62.5%) | 8 | |
| Washing the hands of the child | 0.527 3 | |||
| No hand washing | 0 (0.0%) | 2 (100.0%) | 2 | |
| Only with cold/hot water | 53 (48.2%) | 57 (51.8%) | 110 | |
| Sometimes with water and soap | 90 (50.3%) | 89 (49.7%) | 179 | |
| Always with water and soap | 16 (42.1%) | 22 (57.9%) | 38 | |
| Guardian’s hand washing | 1.000 3 | |||
| No hand washing | 2 (40.0%) | 3 (60.0%) | 5 | |
| Only with cold and/or hot water | 92 (48.7%) | 97 (51.3%) | 189 | |
| With water and soap | 64 (48.5%) | 68 (51.5%) | 132 | |
| Number of handwashing of the guardian per day | 0.770 2 | |||
| 1–2 times | 12 (42.9%) | 16 (57.1%) | 28 | |
| 3–4 times | 73 (50.0%) | 73 (50.0%) | 146 | |
| ≥5 times | 73 (47.7%) | 80 (52.3%) | 153 | |
| Type of kitchen | 0.213 2 | |||
| Indoor kitchen in specific room | 20 (55.6%) | 16 (44.4%) | 36 | |
| Indoor kitchen no specific room | 85 (52.1%) | 78 (47.9%) | 163 | |
| Outdoor kitchen in specific room | 13 (43.3%) | 17 (56.7%) | 30 | |
| Outdoor kitchen no specific room | 40 (40.4%) | 59 (59.6%) | 99 | |
| Child has a personal plate | 0.285 3 | |||
| Yes | 18 (39.1%) | 28 (60.9%) | 46 | |
| No | 141 (49.8%) | 142 (50.2%) | 283 | |
| Sewage disposal | 0.572 2 | |||
| Adapted | 132 (47.7%) | 145 (52.3%) | 277 | |
| Unsuitable | 27 (51.9%) | 25 (48.1%) | 52 | |
| Household waste disposal | 1.000 3 | |||
| Adapted | 127 (48.3%) | 136 (51.7%) | 263 | |
| Unsuitable | 27 (48.2%) | 29 (51.8%) | 56 | |
| Unknown | 5 (50.0%) | 5 (50.0%) | 10 | |
| Guardian’s hand washing | 1.000 3 | |||
| No hand washing | 2 (40.0%) | 3 (60.0%) | 5 | |
| Only with cold and/or hot water | 92 (48.7%) | 97 (51.3%) | 189 | |
| With water and soap | 64 (48.5%) | 68 (51.5%) | 132 | |
| Number of handwashing of the guardian per day | 0.770 2 | |||
| 1–2 times | 12 (42.9%) | 16 (57.1%) | 28 | |
| 3–4 times | 73 (50.0%) | 73 (50.0%) | 146 | |
| ≥5 times | 73 (47.7%) | 80 (52.3%) | 153 | |
| Type of kitchen | 0.213 2 | |||
| Indoor kitchen in specific room | 20 (55.6%) | 16 (44.4%) | 36 | |
| Indoor kitchen no specific room | 85 (52.1%) | 78 (47.9%) | 163 | |
| Outdoor kitchen in specific room | 13 (43.3%) | 17 (56.7%) | 30 | |
| Outdoor kitchen no specific room | 40 (40.4%) | 59 (59.6%) | 99 | |
| Child has a personal plate | 0.285 3 | |||
| Yes | 18 (39.1%) | 28 (60.9%) | 46 | |
| No | 141 (49.8%) | 142 (50.2%) | 283 | |
| Sewage disposal | 0.572 2 | |||
| Adapted | 132 (47.7%) | 145 (52.3%) | 277 | |
| Unsuitable | 27 (51.9%) | 25 (48.1%) | 52 | |
| Household waste disposal | 1.000 3 | |||
| Adapted | 127 (48.3%) | 136 (51.7%) | 263 | |
| Unsuitable | 27 (48.2%) | 29 (51.8%) | 56 | |
| Unknown | 5 (50.0%) | 5 (50.0%) | 10 | |
| Viral Detection | Total (N = 329) | p-Value | ||
|---|---|---|---|---|
| No (N = 159) | Yes (N = 170) | |||
| n (%) | n (%) | n (%) | ||
| Presence of at least one parasite | 0.370 1 | |||
| Yes | 124 (50.0%) | 124 (50.0%) | 248 (75.4%) | |
| No | 34 (44.2%) | 43 (55.8%) | 77 (23.4%) | |
| Giardia intestinalis | 0.873 1 | |||
| Yes | 40 (49.4%) | 41 (50.6%) | 81 (24.6%) | |
| No | 118 (48.4%) | 126 (51.6%) | 244 (74.2%) | |
| Ascaris lumbricoides | 0.013 1 | |||
| Yes | 90 (55.6%) | 72 (44.4%) | 162 (49.2%) | |
| No | 68 (41.7%) | 95 (58.3%) | 163 (49.5%) | |
| Trichuris trichiura | 0.637 1 | |||
| Yes | 103 (47.7%) | 113 (52.3%) | 216 (65.6%) | |
| No | 55 (50.5%) | 54 (49.5%) | 109 (33.1%) | |
| Enterobius vermicularis | 0.614 2 | |||
| Yes | 2 (66.7%) | 1 (33.3%) | 3 (0.9%) | |
| No | 156 (48.4%) | 166 (51.6%) | 322 (97.9%) | |
| Viral Detection | Crude OR (CI 95%) * | Adjusted OR ** (CI 95%) * | p-Value | ||
|---|---|---|---|---|---|
| No (N = 149) | Yes (N = 155) | ||||
| Child’s food diversity score | 0.03 | ||||
| Unsuitable | 49 (32.9%) | 70 (45.2%) | ref. | ref. | |
| Adequate | 100 (67.1%) | 85 (54.8%) | 0.59 (0.37–0.95) | 0.58 (0.35–0.94) | |
| Nutritional status of the mother | |||||
| Normal | 102 (68.5%) | 86 (55.5%) | ref. | ref. | |
| Undernourished | 23 (15.4%) | 20 (12.9%) | 1.03 (0.53–2) | 1.07 (0.54–2.11) | 0.791 |
| Overnourished | 24 (16.1%) | 49 (31.6%) | 2.42 (1.37–4.27) | 2.45 (1.38–4.42) | 0.003 |
| A. lumbricoides carriage | 0.021 | ||||
| Yes | 87 (58.4%) | 69 (44.5%) | ref. | ref. | |
| No | 62 (41.6%) | 86 (55.5%) | 1.75 (1.11,2.75) | 1.75 (1.09–2.83) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razanajatovo, I.M.; Andrianomiadana, L.; Habib, A.; Randrianarisoa, M.M.; Razafimanjato, H.; Rakotondrainipiana, M.; Andriantsalama, P.; Randriamparany, R.; Andriamandimby, S.F.; Vonaesch, P.; et al. Factors Associated with Carriage of Enteropathogenic and Non-Enteropathogenic Viruses: A Reanalysis of Matched Case-Control Data from the AFRIBIOTA Site in Antananarivo, Madagascar. Pathogens 2023, 12, 1009. https://doi.org/10.3390/pathogens12081009
Razanajatovo IM, Andrianomiadana L, Habib A, Randrianarisoa MM, Razafimanjato H, Rakotondrainipiana M, Andriantsalama P, Randriamparany R, Andriamandimby SF, Vonaesch P, et al. Factors Associated with Carriage of Enteropathogenic and Non-Enteropathogenic Viruses: A Reanalysis of Matched Case-Control Data from the AFRIBIOTA Site in Antananarivo, Madagascar. Pathogens. 2023; 12(8):1009. https://doi.org/10.3390/pathogens12081009
Chicago/Turabian StyleRazanajatovo, Iony Manitra, Lova Andrianomiadana, Azimdine Habib, Mirella Malala Randrianarisoa, Helisoa Razafimanjato, Maheninasy Rakotondrainipiana, Prisca Andriantsalama, Ravaka Randriamparany, Soa Fy Andriamandimby, Pascale Vonaesch, and et al. 2023. "Factors Associated with Carriage of Enteropathogenic and Non-Enteropathogenic Viruses: A Reanalysis of Matched Case-Control Data from the AFRIBIOTA Site in Antananarivo, Madagascar" Pathogens 12, no. 8: 1009. https://doi.org/10.3390/pathogens12081009
APA StyleRazanajatovo, I. M., Andrianomiadana, L., Habib, A., Randrianarisoa, M. M., Razafimanjato, H., Rakotondrainipiana, M., Andriantsalama, P., Randriamparany, R., Andriamandimby, S. F., Vonaesch, P., Sansonetti, P. J., Lacoste, V., Randremanana, R. V., Collard, J.-M., Heraud, J.-M., & on behalf of the Afribiota Investigators. (2023). Factors Associated with Carriage of Enteropathogenic and Non-Enteropathogenic Viruses: A Reanalysis of Matched Case-Control Data from the AFRIBIOTA Site in Antananarivo, Madagascar. Pathogens, 12(8), 1009. https://doi.org/10.3390/pathogens12081009