Social support networks provide health and survival benefits to old adults by maintaining social integration and strengthening coping under the adverse life events. Numerous studies have demonstrated that older adults with more supportive and integrated networks have better mental health and a lower risk of morbidity and mortality (
Berkman and Syme 1979;
Cohen 1985,
2004;
House et al. 1988;
Kaplan et al. 1977;
Uchino et al. 2018). Despite the use of diverse definitions and measurements in previous research, there is a general agreement that social support is a multidimensional concept consisting of structural (e.g., size or interaction frequency), functional (e.g., types of support), and relationship (e.g., source of supports) dimensions (
Cohen 1985;
House et al. 1988;
Thoits 1982,
1985;
Wellman and Wortley 1990). Empirical studies have carefully interpreted the different mechanisms between social support networks and health according to the different dimensions of social support networks. For example, the functions of social support (e.g., emotional aid and instrumental aid) are often linked to a stress-buffering mechanism in which the negative effects of adverse life events on mental health are mitigated by social support. The effects of the support networks’ structural aspects (e.g., size and contact frequency) on health, on the other hand, have been interpreted as the positive consequence of normative health-related regulations and social integration (
Berkman et al. 2000;
Kawachi and Berkman 2001).
Yet, despite its importance, the multidimensionality of social support is often conceptualized and operationalized only at the network level, without considering the multifaceted characteristics of dyadic support ties. A dyadic social relationship has several attributes such as interaction frequency, intimacy, and types of support. Given the fact that dyadic ties have multiple attributes, it is not surprising that each social tie takes its own relationship form (
Adams et al. 1998;
Allan 1998;
Pahl 2000;
Spencer and Pahl 2006). For example, a close friend who gives emotional and instrumental help is quite different from a more distant friend who only gives instrumental help, even though both people are friends or provide instrumental help. Defining the complexity of dyadic relationships and the systemic assessment of the multiple forms of dyadic social relationships is necessary for understanding the potential importance of diverse, supportive social relationships in individual lives.
In this article, I extend previous research by examining the role of multiple forms of core social ties in buffering the effects of stress on depression symptoms. Specifically, this study examines core discussion partner networks, a relationship term widely used in social support network studies (
Bookwala 2017;
Brown and Harris 1978;
Burt 1987;
Cornwell 2012;
Murphy 1982;
Shiovitz-Ezra and Litwin 2012). Although core discussion partners are believed to be most supportive social relationships (
Burt 1984;
Marsden 1987;
McPherson et al. 2006), recent studies have shown that discussion partner relationships vary greatly by the subject of discussion, individual circumstances, and relationship contexts (
Bearman and Parigi 2004;
Small 2013,
2017). Different core discussion partners provide different types of support (
Brashears 2014). This study aims to classify multiple forms of discussion partner ties empirically and to examine what types of core discussion partner are most important in the stress-buffering role of social networks.
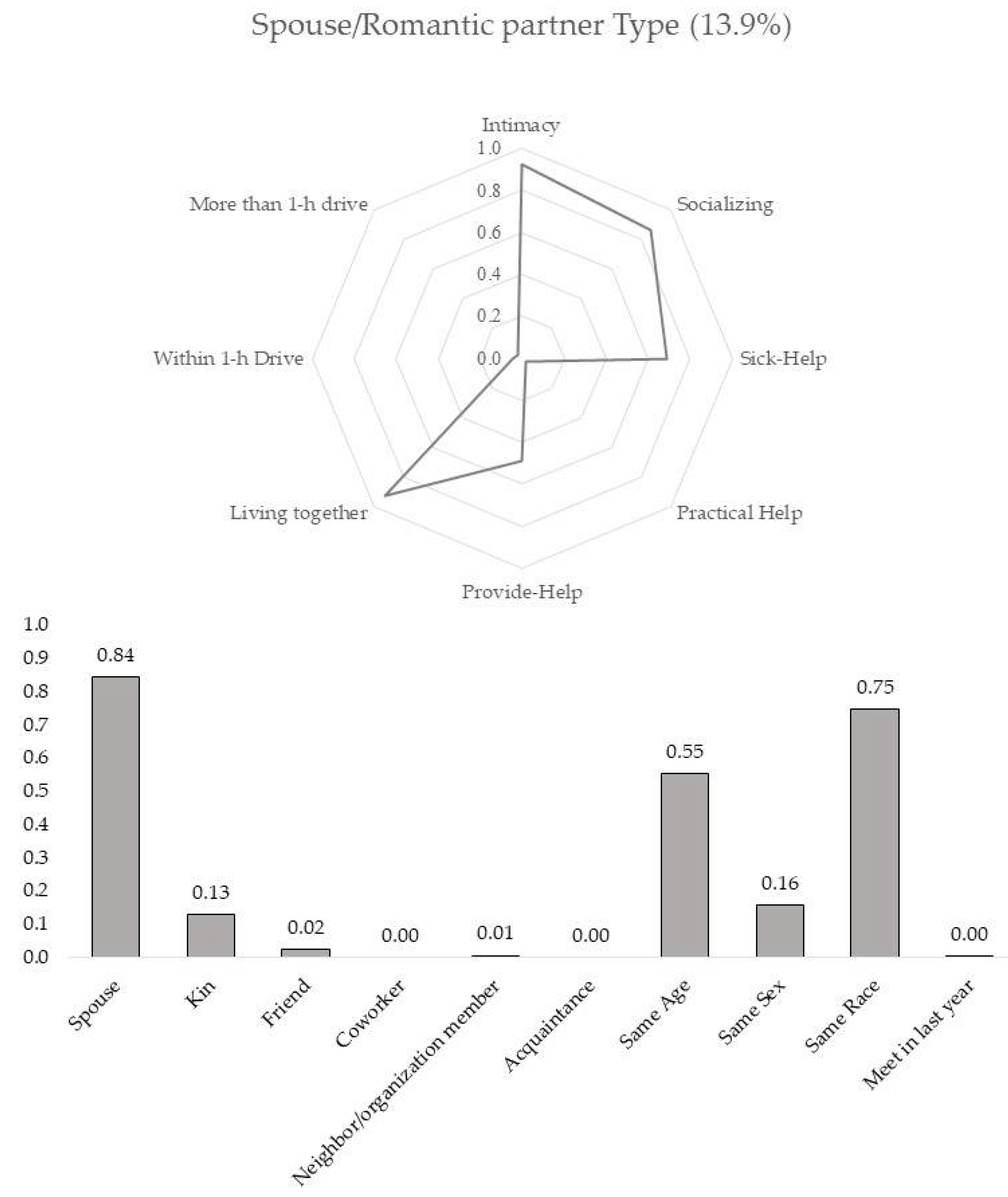
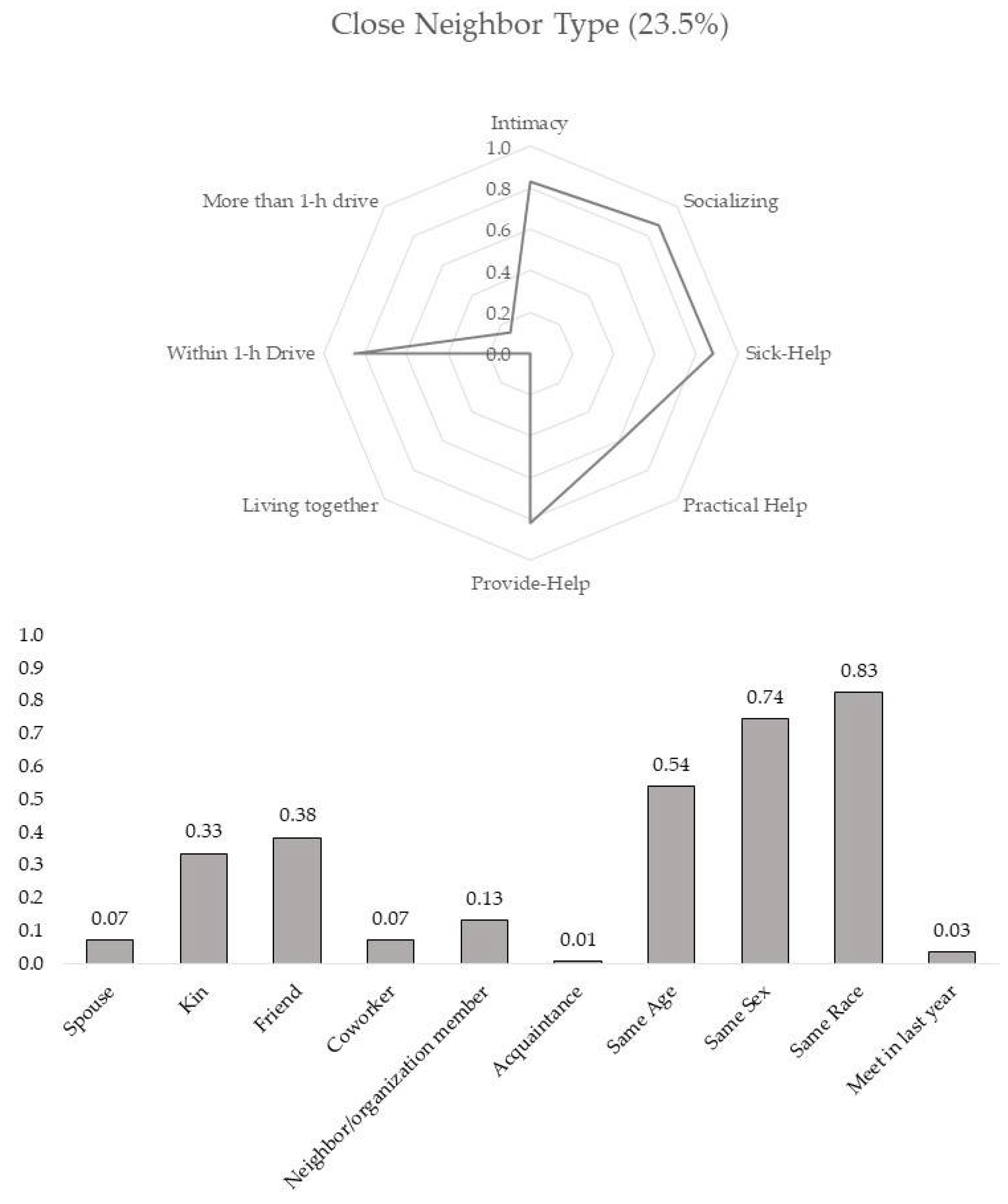
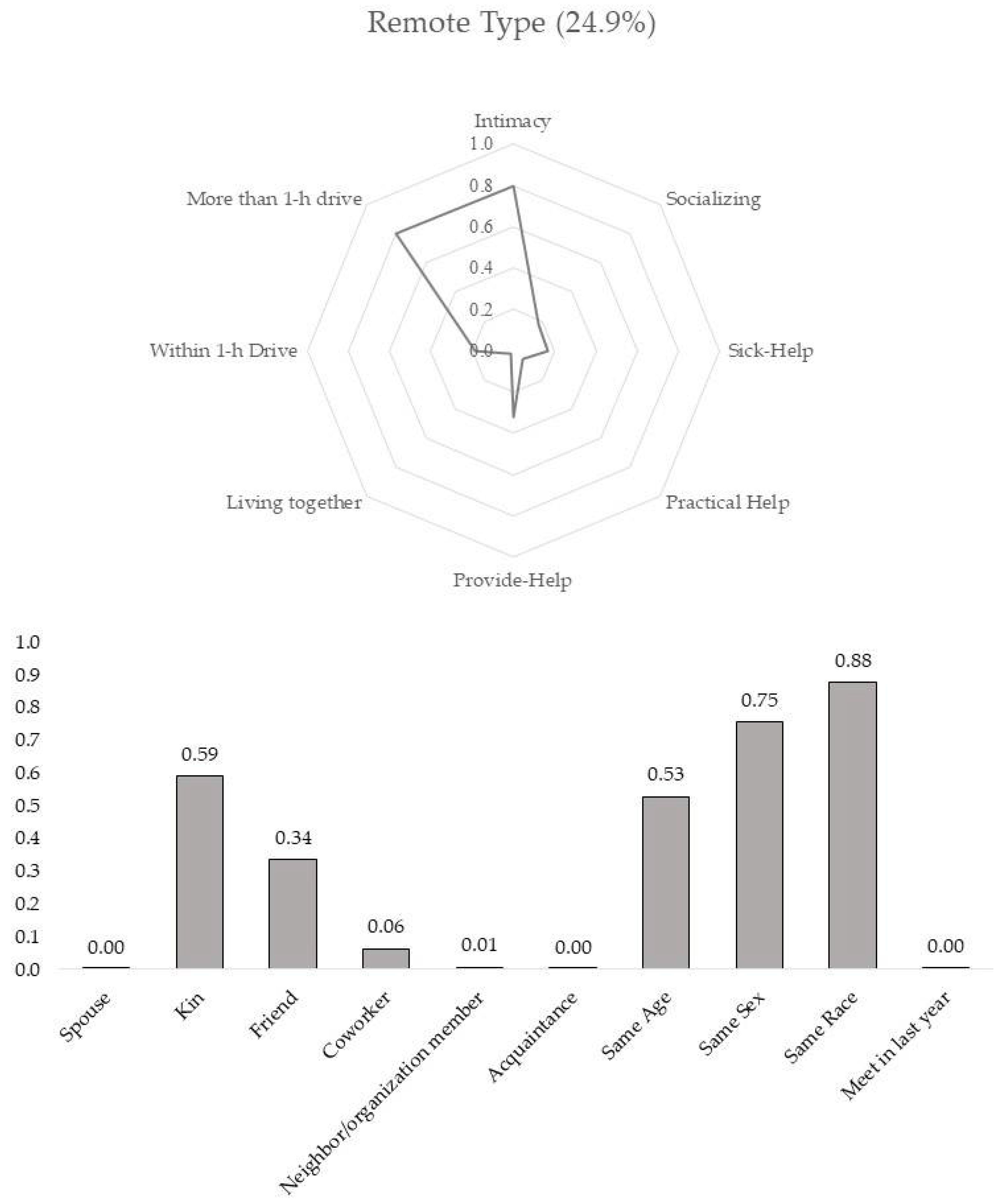
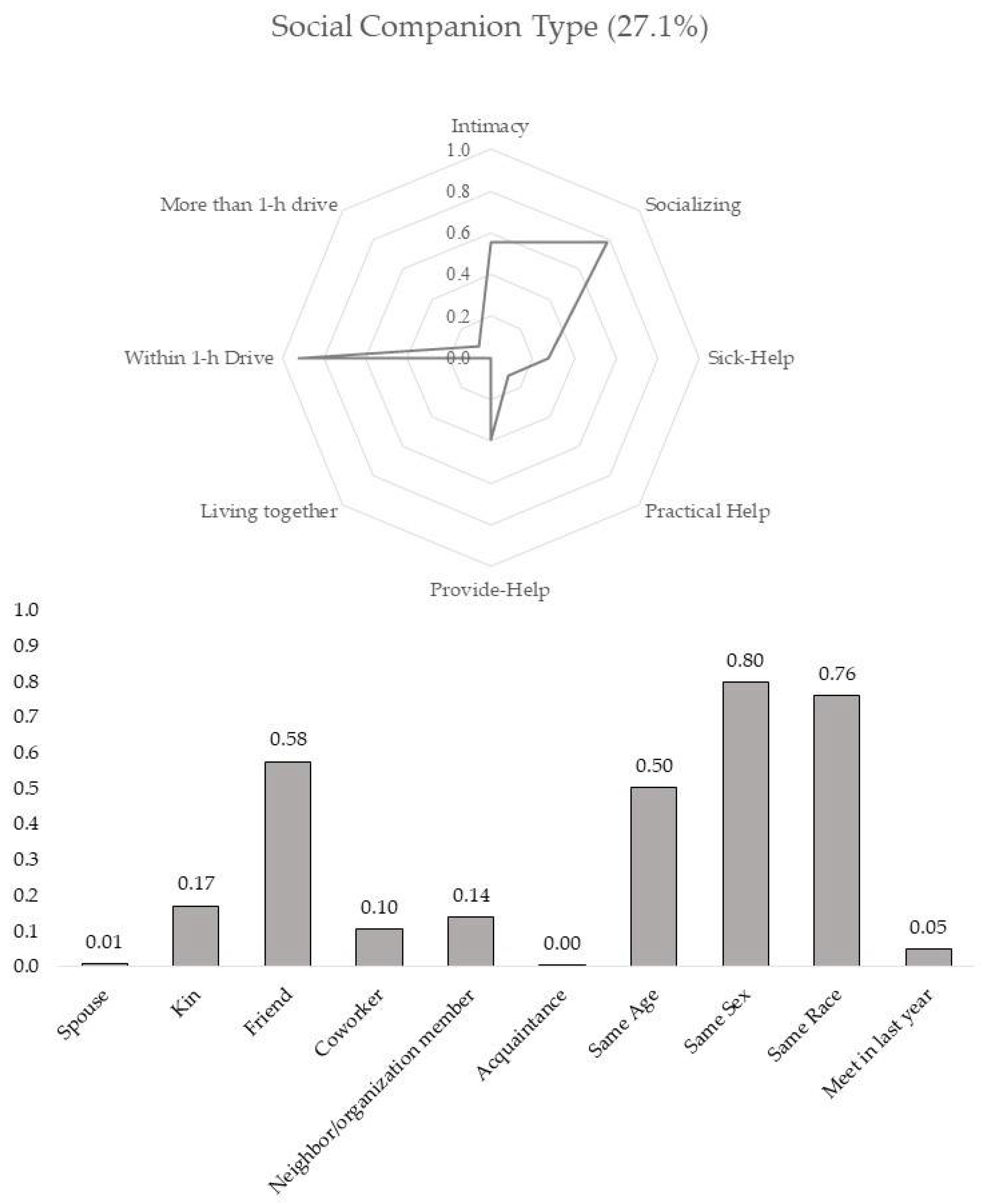
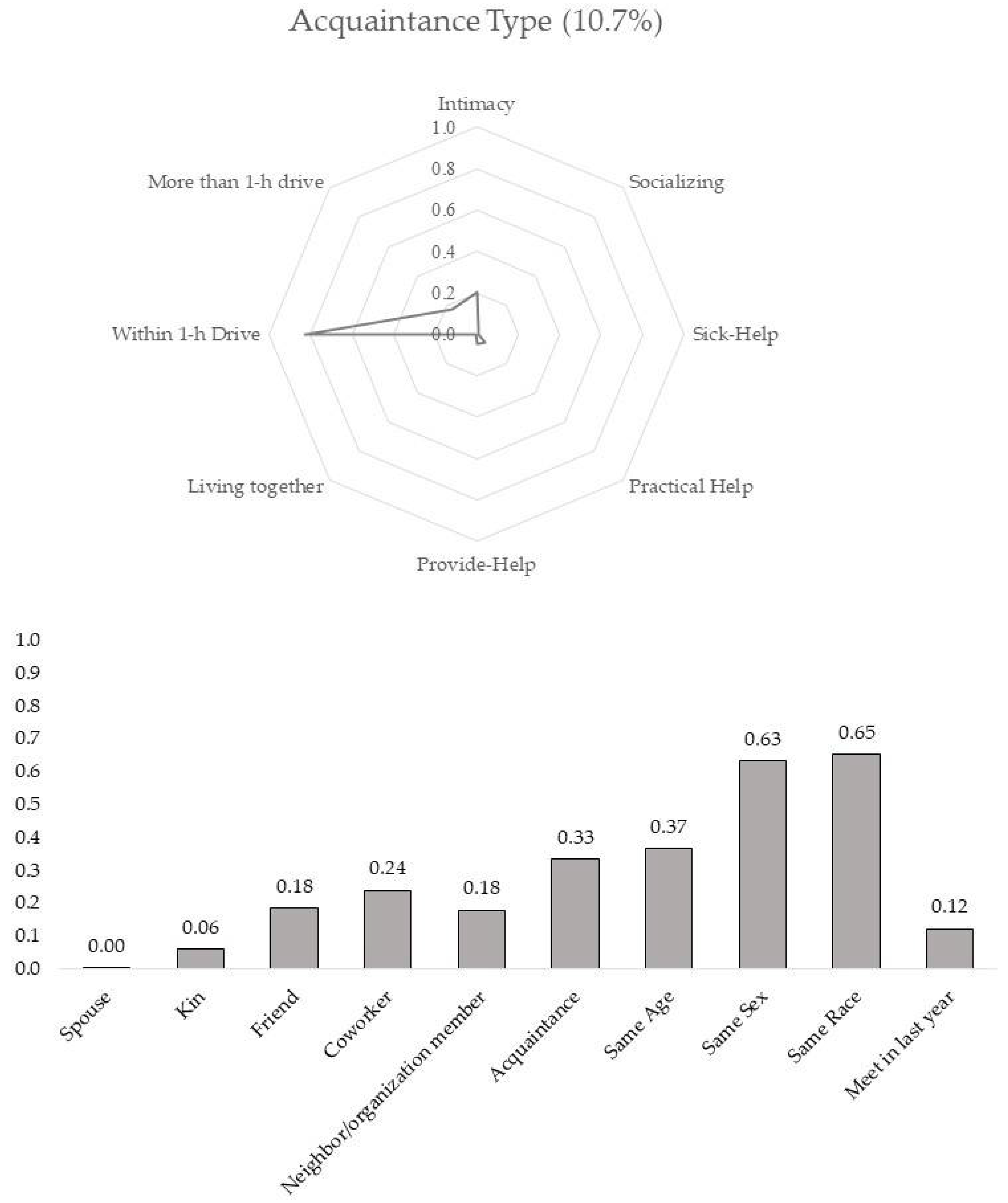
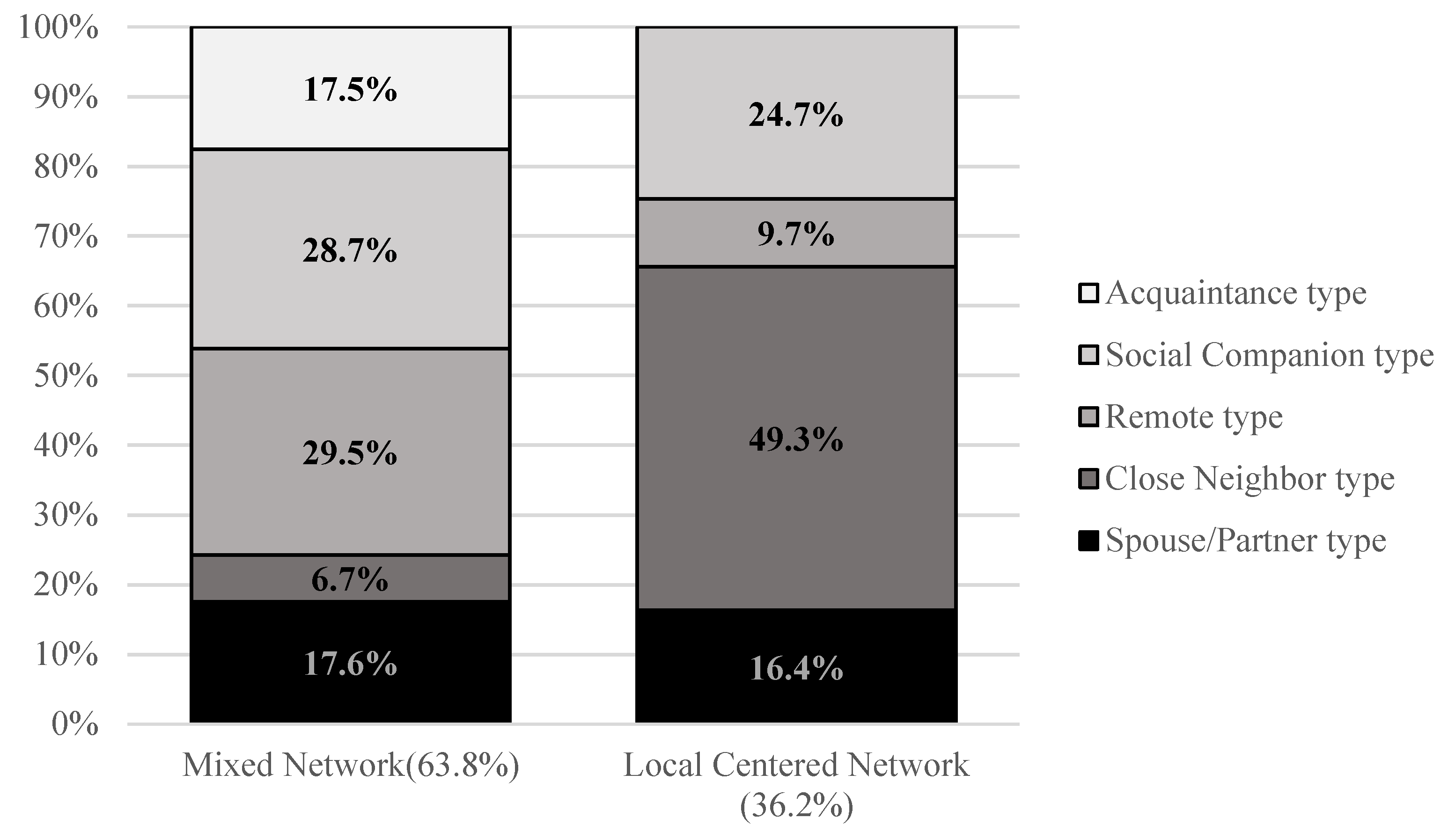
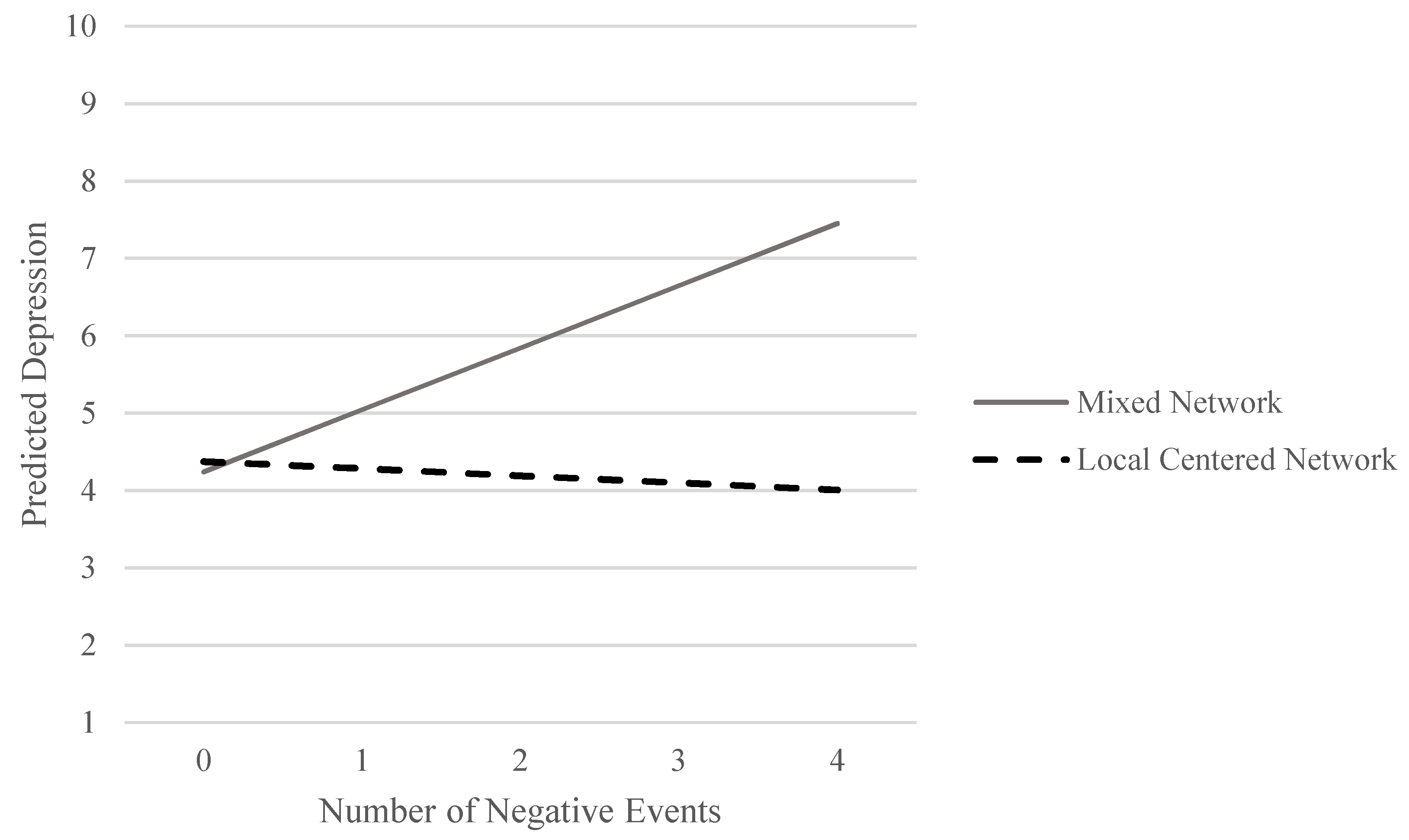
This study used rich personal network survey data collected from the San Francisco-Oakland area in 2015. The analysis is conducted in three steps to (1) classify the various forms of discussion partner ties based on multiple tie-level characteristics; (2) cluster the discussion partner networks at network level based on the multiple types of ties; then (3) examine interaction effects between adverse life events and discussion network typology on depression. The results of this study demonstrate five different types of discussion partner ties. They also show that close neighbor discussion partners seem to be crucial for buffering the negative effects of adverse life events on depression.
1.1. Multidimensionality of Social Support Networks
Although diverse definitions have been suggested, a social support network is generally understood to be a set of members of a personal network who provide emotional aid, instrumental aid, and informational aid (
House et al. 1988;
Kaplan et al. 1977;
Thoits 1982). Numerous studies have shown the significant effects of social support upon psychological well-being, physical morbidity, and mortality (
Berkman and Syme 1979;
Cohen 1985;
Seeman 2000). Belonging to stable social networks directly promotes positive psychological states, such as feelings of self-worth and social integration. Normative regulation of health-related behaviors exercised by social network members can reduce the likelihood of poor health behaviors (
Berkman and Kawachi 2000;
House et al. 1988;
Kawachi and Berkman 2001;
Umberson 1987). Network members’ support buffers the negative impacts of stressful adverse conditions on mental health status. Discussing problems with network members helps redefine the importance of the issues and prevents maladaptive reactions to stressful events. In addition, the mobilized support may directly help individuals resolve the difficulties (
Cobb 1976;
Cohen 1985;
Lin et al. 1985).
Though the operationalization of social support in empirical studies varies by survey instruments and research interests, a common way of measuring social support is to sum up the characteristics of social relationships. For example, the size of the network is a sum of the existing social ties. Emotional support is often measured by counting the total number of social network members who provide this support. Although aggregate measures are informative, additive measures rely on the crude assumption that the observed supports may be equally important. For example, when a study finds that having more emotional support significantly reduces depression, the association between emotional support and depression assumes that adding each emotional support reduces depression to the same degree as that which was achieved from adding the first emotional support. This symmetric linear association is possible only when every emotional support has an equally important effect against depression. However, as Thoits notes (
Thoits 1982, p. 147), “not all sources or types of social support are equally effective in reducing depression.” The types of support people get from alters vary by the relationship (
Brashears 2014;
Wellman and Wortley 1990), and the effects of social support on psychological status depend on the characteristics of the relationship (
Dean et al. 1990). For example, support from kin or adult children may exert weak effects on mental health because obligation strains independence and autonomy (
Dean et al. 1990;
Silverstein et al. 1996). Further, the social networks’ benefits may be attributed mainly to supports from alters who have specific knowledge related to the ego’s stressful situation (
Perry and Pescosolido 2015). There is substantial evidence that the multidimensional aspects of social support and relationships are associated with the effects of social support on health outcomes.
The multidimensionality of social support networks has received considerable attention in social network and health studies. The literature has conceptualized three different dimensions of social support: the structures (e.g., size and density of networks), functions (e.g., types of support and social influence), and sources of social support (e.g., role relationships) (
House et al. 1988;
Kaplan et al. 1977;
Thoits 1982;
Baruch-Feldman et al. 2002;
Dean et al. 1990;
House et al. 1988;
Thoits 1982;
Wellman and Wortley 1990). Empirical studies often developed support measurements and interpreted the benefits of social support by distinguishing the specific dimensions of social support. For example, structural aspects of support networks often link to the social influence explanation, whereas the types of support people receive from their networks are interpreted as buffering factors that reduce the adverse effects of stress (
Kawachi and Berkman 2001).
Instead of separating social support dimensions, network typology studies have suggested an alternative approach that identifies different types of support networks through complex combinations of structures, functions, and source of social support (
Agneessens et al. 2006;
Fiori et al. 2006;
Litwin 1998;
Litwin and Stoeckel 2014;
Shiovitz-Ezra and Litwin 2012;
Youm et al. 2018). The network typology research demonstrates that there are a countable number of social network types (usually between four and six), which differ from each other in terms of the proportion of support types (e.g., emotional support and instrumental aids), average size, and interaction frequencies, and distribution of role relationships.
Despite their contributions, studies taking multidimensionality into account have limited their attention to the complexity of support networks. The theoretical claim about multidimensionality can apply not only to the multidimensional aspects of support networks but also to the complexity of dyadic support relationships. For example, one observed dyadic support relationship can be described by applying the structural, functional, and relationship attributes of social support, such as a frequently interacting friend who provides emotional and instrumental aids. Although the concepts and operational strategy for the network-level multidimensionality have been well established, more conceptual and operational measures are needed to capture the tie-level complexity.
This study suggests conceptualizing the dyadic social tie as a multifaceted composite. Specifically, I argue that interactions of multiple attributes, including functions, structures, and other relationship-level characteristics, constitute the form of a dyadic social relationship. According to the pattern of associations among various attributes, diverse social ties take distinctive forms of relationships. The social support network in this study is redefined as a set of social relationships that takes multiple forms of relationship according to the configuration of its functional, structural, and other attributes. Examining the effects of social support on health by assessing the multiple forms of dyadic social ties is particularly beneficial to the asymmetric problem of the aggregated social support measures. As I discussed above, not every support or alter is equally important. Instead, the effect of one additional support (or alter) would depend on the types, functions, and importance of the relationship. Having a close friend who provides various types of support may not have an equal effect on health as having a more distant friend who only offers informational aid. By assessing the multiple forms of social ties, this study examines what forms of social relationships are essential for understanding the stress-buffering role of social support networks.
1.2. Diversity of Discussion Partners
In assessing the buffering effect of multiple forms of a dyadic social relationship on depression, this study examines core discussion networks, which have been widely used in social network and health research. The social network members that people rely on for discussing important matters are thought to be the closest social relationships (
Burt 1984;
Marsden 1987;
McPherson et al. 2006). Accordingly, having a small number of core discussion partners has been treated as a proxy of social isolation, weak social support, and difficulty of support mobilization, which in turn results in negative individual-level outcomes such as lower happiness (
Burt 1987), bad self-rated health (
Cornwell and Waite 2009), alcohol abuse, and physical inactivity (
Shiovitz-Ezra and Litwin 2012).
However, recent studies on core discussion networks have shown that the discussion partners are neither homogenously close nor provide similar supports. People choose discussion partners from various social relationships based on discussion topics (
Bearman and Parigi 2004), availability, and individual contexts (
Small 2013,
2017).
Bearman and Parigi (
2004) found that particular discussion subjects are likely to be matched with particular role relationships. For example, a spouse is likely to be approached for economic and house-related issues, whereas friends would be partners for discussing community or ideological issues. Indeed, people sometimes discuss their important matters with newly encountered people in their current institutional contexts. For example,
Small (
2017) demonstrated that a substantial portion of graduate students’ old and close discussion partners was replaced by newly encountered people such as roommates or administrators in their new institutional environment. Regardless of the emotional attachment, people disclose their personal matters to newly formed relations or acquaintances when they perceive that they have relevant knowledge and are available at the time of need (
Small 2009,
2013,
2017). The support provided by discussion partners also differs depending on the role relationship and characteristics of alters. Using nationally representative data,
Brashears (
2014) showed that discussion topics, role relationships, and expected support are all significantly associated. For example, a spouse with whom one discusses economic issues is more likely than friends to provide monetary support (
Brashears 2014).
The diversity of discussion partners implies that the social networks’ buffering function varies according to what kind of discussion partners constitute the core discussion networks. One discussion network may be better for reducing stress under adverse circumstances than other networks, if the former network was more accessible, more knowledgeable, or had more supportive alters than the latter. Strong social relationships may successfully lessen the adverse effects of negative life events. People are likely to meet their basic psychological needs such as approval, esteem, or affirmation through the interaction with primary network members (
Antonucci and Akiyama 1987;
Kaplan et al. 1977;
Thoits 2011). For example, having a confiding relationship with a marital partner may be the most effective factor in mitigating the adverse psychological impact of stressful life events (
Brown and Harris 1978;
Dean et al. 1990).
By contrast, some studies emphasize the role of secondary or weak ties in protecting mental health. Secondary social relationships may contribute to buffering stressors by suggesting fresh perspectives and information. For example,
Perry and Pescosolido (
2015) demonstrate that it is not total network size but the number of discussion partners people “talk to about health problems when they come up” that significantly improves individuals’ mental health and health-related service satisfaction. While people tend to form close and supportive relations with others who they perceive to be similar to them (
McPherson et al. 2001), the heterogeneous social relations in terms of gender, race/ethnicity, and aging also can offer benefits to protecting mental health. For example, cross-sex relationships in older adults provide a buffer against loneliness (
O’Connor 1993). Network typology studies also show that a social network with diverse role relationships is more beneficial for reducing depression than networks dominated by kin ties (
Fiori et al. 2006;
Fiori and Jager 2012;
Litwin 1998;
Litwin and Stoeckel 2014;
Shiovitz-Ezra and Litwin 2012).
In sum, relationships with core discussion partners take heterogeneous forms according to relationship dimensions, including intimacy, accessibility, types of support, and role relationship. Accordingly, the core discussion network includes various forms of social relationships. In this case, the association between mental health and core discussion networks is not merely attributable to the amount of help and resources provided by close social relationships. Instead, the discussion networks’ buffering effect on depression varies according to what forms of discussion partner relations compose the discussion network. Based on this discussion, I hypothesize that at the tie-level, there will be diverse discussant ties who take different forms of relationship in terms of intimacy, accessibility, and support provision. At the network level, the core discussion networks will be differently configured according to the distribution of multiple forms of discussants. Finally, I expect that the buffering effects of the core discussion networks on depression will vary according to the network configuration.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






