
Strategic Biophilic Residential Design Based on Seniors’ Health Profiles: A HRQoL-Driven Approach



Abstract
1. Introduction
1.1. Background
1.2. Research Aim and Research Questions
- RQ1. How do senior individuals’ HRQoL profiles influence their preferences for biophilic residential design elements?
- RQ2. How can biophilic design elements be functionally categorized and matched to residential spatial needs according to each senior HRQoL profile?
- RQ3. What are effective strategic design interventions that reflect seniors’ HRQoL and BRD needs?
2. Literature Review
2.1. Seniors’ HRQoL and Residential Environment
2.2. Biophilia and Biophilic Design
2.2.1. Biophilia: Preference for Nature
2.2.2. Theoretical Frameworks of Biophilic Design
2.3. Biophilic Design Experience for Seniors
3. Methodology
3.1. Survey Procedure and Participants
3.2. Measurements
3.3. Data Analysis
- (1)
- Descriptive statistics were first computed for all variables to assess the overall distribution of HRQoL levels and BRD preferences among senior participants;
- (2)
- A principal component analysis (PCA) with Varimax rotation was conducted on the HRQoL items to identify the underlying factor structure. Factors were extracted based on eigenvalues greater than 1.0, with a minimum factor loading threshold of 0.5;
- (3)
- Using the factor scores derived from the PCA, a two-step cluster analysis was performed. An initial hierarchical clustering approach was applied to determine the optimal number of clusters, followed by K-means clustering to clearly segment HRQoL profiles. Each cluster was then labeled based on the dominant characteristics of its factor composition;
- (4)
- Finally, a one-way ANOVA was conducted to examine differences in BRD preferences across the HRQoL-based clusters. All statistical tests were performed with a 95% confidence level, and the significance threshold was set at α = 0.05.
4. Results
4.1. Descriptive Statistics
4.2. Factor Structure of HRQoL
4.3. Identification of the HRQoL-Based Senior Cluster
4.4. Analysis of BRD Preference Differences: ANOVA
5. Strategic BRD Framework
5.1. Summary of Residential Spatial Needs by Cluster
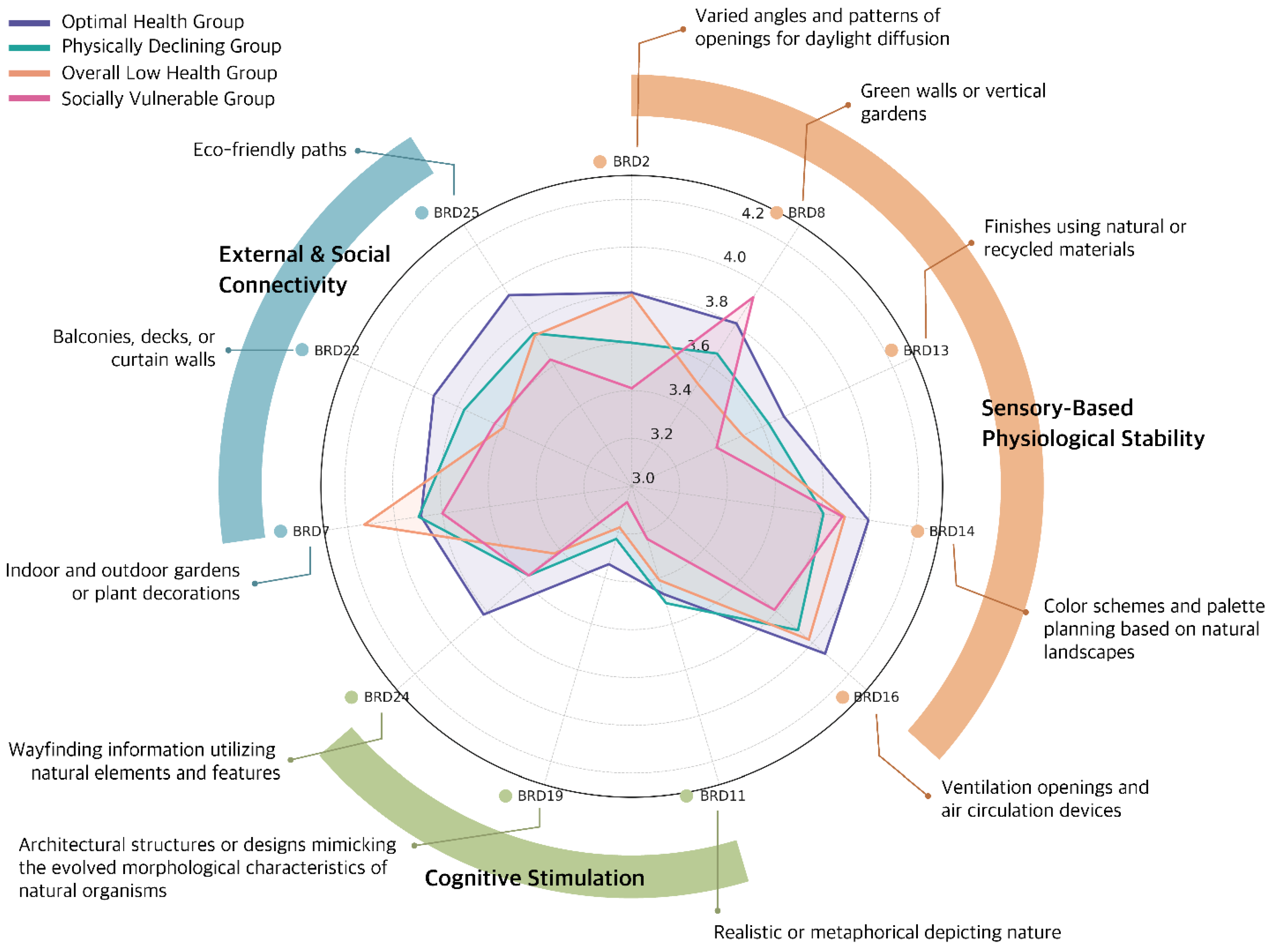
5.2. Functional Typology of BRD Preference
- (1)
- Sensory-Based Physiological Stability
- (2)
- Cognitive Stimulation
- (3)
- External and Social Connectivity
5.3. Strategic Recommendations for Cluster-Based BRD
- (1)
- Optimal Health Group
- (2)
- Physically Declining Group
- (3)
- Overall Low Health Group
- (4)
- Socially Vulnerable Group
6. Conclusions
6.1. Summary of the Study
- (1)
- Regarding RQ1, statistically significant differences were identified in 11 BRD elements across clusters, indicating that seniors’ spatial expectations and receptivity to design features vary meaningfully depending on their health status;
- (2)
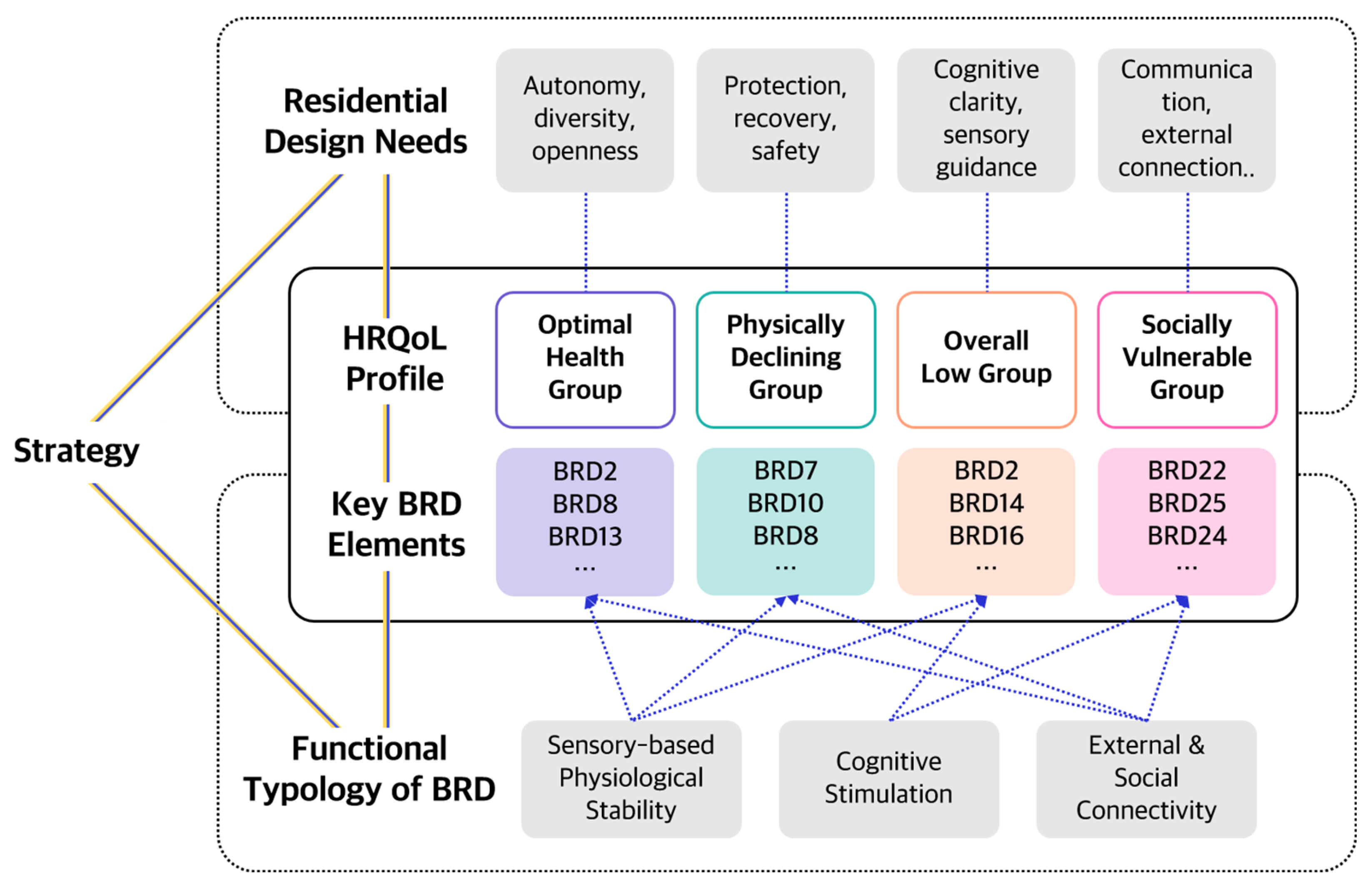
- For RQ2, BRD elements were reclassified into three functional categories—sensory stability, cognitive stimulation, and social connection—and mapped onto the specific spatial needs of each cluster. This mapping demonstrated the feasibility of translating health characteristics into design logic;
- (3)
- In addressing RQ3, a strategic design matrix was developed, integrating HRQoL profiles, spatial demands, and BRD functionality. This matrix offers a structured health-responsive model that supports user-centered residential planning based on differentiated needs.
6.2. Contributions and Implications
- It presents the feasibility of HRQoL-based user profiling for senior-centered residential planning;
- It enhances the applicability of BRD elements by reorganizing them into functional categories tailored to the needs of HRQoL clusters;
- It establishes a strategic foundation for policy-driven design guidelines through differentiated spatial strategies for each user cluster.
6.3. Limitations and Future Research Directions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Available online: https://www.who.int/health-topics/ageing#tab=tab_1 (accessed on 7 January 2020).
- Wang, L.; Muxin, G.; Nishida, H.; Shirakawa, C.; Sato, S.; Konishi, T. Psychological stress-induced oxidative stress as a model of sub-healthy condition and the effect of TCM. Evid. -Based Complement. Altern. Med. 2007, 4, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.; Pabst, A.; Weyerer, S.; Werle, J.; Maier, W.; Heilmann, K.; Scherer, M.; Stark, A.; Kaduszkiewicz, H.; Wiese, B. The assessment of met and unmet care needs in the oldest old with and without depression using the Camberwell Assessment of Need for the Elderly (CANE): Results of the AgeMooDe study. J. Affect. Disord. 2016, 193, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Balfour, J.L.; Kaplan, G.A. Neighborhood environment and loss of physical function in older adults: Evidence from the Alameda County Study. Am. J. Epidemiol. 2002, 155, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Yin, J.; Arfaei, N.; MacNaughton, P.; Catalano, P.J.; Allen, J.G.; Spengler, J.D. Effects of biophilic interventions in office on stress reaction and cognitive function: A randomized crossover study in virtual reality. Indoor Air 2019, 29, 1028–1039. [Google Scholar] [CrossRef]
- Brown, D.K.; Barton, J.L.; Gladwell, V.F. Viewing nature scenes positively affects recovery of autonomic function following acute-mental stress. Environ. Sci. Technol. 2013, 47, 5562–5569. [Google Scholar] [CrossRef]
- Kondo, M.C.; Jacoby, S.F.; South, E.C. Does spending time outdoors reduce stress? A review of real-time stress response to outdoor environments. Health Place 2018, 51, 136–150. [Google Scholar] [CrossRef]
- Bratman, G.N.; Daily, G.C.; Levy, B.J.; Gross, J.J. The benefits of nature experience: Improved affect and cognition. Landsc. Urban Plan. 2015, 138, 41–50. [Google Scholar] [CrossRef]
- Berto, R. Exposure to restorative environments helps restore attentional capacity. J. Environ. Psychol. 2005, 25, 249–259. [Google Scholar] [CrossRef]
- Bratman, G.N.; Hamilton, J.P.; Daily, G.C. The impacts of nature experience on human cognitive function and mental health. Ann. N. Y. Acad. Sci. 2012, 1249, 118–136. [Google Scholar] [CrossRef]
- Oh, B.; Lee, K.J.; Zaslawski, C.; Yeung, A.; Rosenthal, D.; Larkey, L.; Back, M. Health and well-being benefits of spending time in forests: Systematic review. Environ. Health Prev. Med. 2017, 22, 1–11. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Simons, R.F.; Losito, B.D.; Fiorito, E.; Miles, M.A.; Zelson, M. Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 1991, 11, 201–230. [Google Scholar] [CrossRef]
- Kaplan, R.; Kaplan, S. The Experience of Nature: A Psychological Perspective; Cambridge University Press: Cambridge, NY, USA, 1989. [Google Scholar]
- Kellert, S.; Heerwagen, J.; Mador, P. Biophilic Design: The Theory, Science, and Practice of Bringing Buildings to Life; John Wiley & Sons: Hoboken, NJ, USA, 2008. [Google Scholar]
- Van den Berg, A.E.; Hartig, T.; Staats, H. Preference for nature in urbanized societies: Stress, restoration, and the pursuit of sustainability. J. Soc. Issues 2007, 63, 79–96. [Google Scholar] [CrossRef]
- Lei, Q.; Lau, S.; Yuan, C.; Qi, Y. Post-occupancy evaluation of the biophilic design in the workplace for health and wellbeing. Buildings 2022, 12, 417. [Google Scholar] [CrossRef]
- Meidenbauer, K.L.; Stenfors, C.U.; Bratman, G.N.; Gross, J.J.; Schertz, K.E.; Choe, K.W.; Berman, M.G. The affective benefits of nature exposure: What’s nature got to do with it? J. Environ. Psychol. 2020, 72, 101498. [Google Scholar] [CrossRef]
- Russell, R.; Guerry, A.D.; Balvanera, P.; Gould, R.K.; Basurto, X.; Chan, K.M.; Klain, S.; Levine, J.; Tam, J. Humans and nature: How knowing and experiencing nature affect well-being. Annu. Rev. Environ. Resour. 2013, 38, 473–502. [Google Scholar] [CrossRef]
- Lee, E.-J.; Park, S.-J.; Choi, J.-H. Effect of a Virtual Biophilic Residential Environment on the Perception and Responses of Seniors. Appl. Sci. 2024, 14, 11431. [Google Scholar] [CrossRef]
- Peters, T.; Verderber, S. Biophilic Design Strategies in Long-Term Residential Care Environments for Persons with Dementia. J. Aging Environ. 2022, 36, 227–255. [Google Scholar] [CrossRef]
- Hartig, T.; Mitchell, R.; De Vries, S.; Frumkin, H. Nature and health. Annu. Rev. Public Health 2014, 35, 207–228. [Google Scholar] [CrossRef]
- Yin, S.; Njai, R.; Barker, L.; Siegel, P.Z.; Liao, Y. Summarizing health-related quality of life (HRQOL): Development and testing of a one-factor model. Popul. Health Metr. 2016, 14, 22. [Google Scholar] [CrossRef]
- Maunder, R.G.; Cohen, Z.; McLeod, R.S.; Greenberg, G.R. Effect of intervention in inflammatory bowel disease on health-related quality of life: A critical review. Dis. Colon Rectum 1995, 38, 1147–1161. [Google Scholar] [CrossRef]
- Diener, E.; Emmons, R.A.; Larsen, R.J.; Griffin, S. The satisfaction with life scale. J. Personal. Assess. 1985, 49, 71–75. [Google Scholar] [CrossRef] [PubMed]
- Han, C.-W.; Lee, E.-J.; Iwaya, T.; Kataoka, H.; Kohzuki, M. Development of the Korean version of Short-Form 36-Item Health Survey: Health related QOL of healthy elderly people and elderly patients in Korea. Tohoku J. Exp. Med. 2004, 203, 189–194. [Google Scholar] [CrossRef] [PubMed]
- WHO. Development of the World Health Organization WHOQOL-BREF quality of life assessment. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Group, T.E. EuroQol-a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-ltem short-form health survey (SF-36): I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Perneger, T.V.; Courvoisier, D.S. Exploration of health dimensions to be included in multi-attribute health-utility assessment. Int. J. Qual. Health Care 2011, 23, 52–59. [Google Scholar] [CrossRef]
- Krabbe, P.F.; Stouthard, M.E.; Essink-Bot, M.-L.; Bonsel, G.J. The effect of adding a cognitive dimension to the EuroQol multiattribute health-status classification system. J. Clin. Epidemiol. 1999, 52, 293–301. [Google Scholar] [CrossRef]
- Jo, M.-W.; Kim, S.-H.; Son, W.-S.; Ock, M.; Kim, S.-G. Exploratory Study for Korean Preference-Based Health Related Quality of Life Instrument; Ministry of Health & Welfare: Ulsan, Republic of Korea, 2012. [Google Scholar]
- Ock, M.; Jo, M.; Lee, S. Measuring health related quality of life using EQ-5D in South Korea. Health Technol. Assess. 2013, 1, 103–111. [Google Scholar]
- Yang, Y.; Brazier, J.; Tsuchiya, A. Effect of adding a sleep dimension to the EQ-5D descriptive system: A “bolt-on” experiment. Med. Decis. Mak. 2014, 34, 42–53. [Google Scholar] [CrossRef]
- Stuck, A.E.; Walthert, J.M.; Nikolaus, T.; Büla, C.J.; Hohmann, C.; Beck, J.C. Risk factors for functional status decline in community-living elderly people: A systematic literature review. Soc. Sci. Med. 1999, 48, 445–469. [Google Scholar] [CrossRef]
- Perkins, B.; Kliment, S.A.; Hoglund, J.D.; King, D.; Cohen, E. Building Type Basics for Senior Living; John Wiley & Sons: Hoboken, NJ, USA, 2004; Volume 7. [Google Scholar]
- Clarke, P.J.; Weuve, J.; Barnes, L.; Evans, D.A.; de Leon, C.F.M. Cognitive decline and the neighborhood environment. Ann. Epidemiol. 2015, 25, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Christenson, M.A. Enhancing independence in the home setting. Phys. Occup. Ther. Geriatr. 1990, 8, 49–65. [Google Scholar] [CrossRef]
- Abidin, N.Z.; Abdullah, M.I.; Basrah, N.; Alias, M.N. Residential satisfaction: Literature review and a conceptual framework. IOP Conf. Ser. Earth Environ. Sci. 2019, 385, 012040. [Google Scholar] [CrossRef]
- Butzer, K.W. Environment, Culture, and Human Evolution: Hominids first evolved in mosaic environments, but stone toolmaking accelerated the emergence of Homo, and both culture and environment subsequently served as catalysts for evolution. Am. Sci. 1977, 65, 572–584. [Google Scholar]
- Orians, G.H. Habitat selection: General theory and applications to human behavior. In The Evolution of Human Social Behavior; Lockard, J.S., Ed.; Elsevier: New York, NY, USA, 1980; pp. 49–63. [Google Scholar]
- Appleton, J. The Experience of Landscape; Wiley Chichester: New York, NY, USA, 1996. [Google Scholar]
- Wilson, E.O. Biophilia; Harvard University Press: Cambridge, MA, USA, 1984. [Google Scholar]
- Kellert, S.R.; Wilson, E.O. The Biophilia Hypothesis; Island Press: Washington, DC, USA, 1993. [Google Scholar]
- Lee, E.J. Developing Hybrid Residential Model for the Elderly’s Biophilic Experience. Ph.D. Thesis, Keimyung University, Daegu, Republic of Korea, 2022. [Google Scholar]
- Lee, E.J.; Park, S.J. A Framework of Smart-Home Service for Elderly’s Biophilic Experience. Sustainability 2020, 12, 8572. [Google Scholar] [CrossRef]
- Hartig, T.; Evans, G.W.; Jamner, L.D.; Davis, D.S.; Gärling, T. Tracking restoration in natural and urban field settings. J. Environ. Psychol. 2003, 23, 109–123. [Google Scholar] [CrossRef]
- Berto, R. The role of nature in coping with psycho-physiological stress: A literature review on restorativeness. Behav. Sci. 2014, 4, 394–409. [Google Scholar] [CrossRef]
- Kellert, S.R. Dimensions, elements, and attributes of biophilic design. In Biophilic Design: The Theory, Science, and Practice of Bringing Buildings to Life; John Wiley and Sons: Hoboken, NJ, USA, 2008; pp. 3–19. [Google Scholar]
- Goldhagen, S.W. Welcome to Your World; HarperCollins: New York, NY, USA, 2017. [Google Scholar]
- Cramer, J.S.; Browning, W.D. Transforming building practices through biophilic design. In Biophilic Design: The Theory, Science and Practice of Bringing Buildings to Life; Wiley: Hoboken, NJ, USA, 2008; pp. 335–346. [Google Scholar]
- Browning, W.D.; Ryan, C.O.; Clancy, J.O. 14 Patterns of Biophilic Design: Improving Health & Well-Being in the Built Environment; Terrapin Bright Green, LLC: New York, NY, USA, 2014. [Google Scholar]
- Browning, W.D.; Ryan, C.O. Nature Inside: A Biophilic Design Guide; RIBA Publishing: London, UK, 2020; pp. 1–9. [Google Scholar]
- Xue, F.; Lau, S.S.; Gou, Z.; Song, Y.; Jiang, B. Incorporating biophilia into green building rating tools for promoting health and wellbeing. Environ. Impact Assess. Rev. 2019, 76, 98–112. [Google Scholar] [CrossRef]
- Zhong, W.; Schröder, T.; Bekkering, J. Biophilic design in architecture and its contributions to health, well-being, and sustainability: A critical review. Front. Archit. Res. 2022, 11, 114–141. [Google Scholar] [CrossRef]
- Kellert, S.R. Nature by Design: The Practice of Biophilic Design; Yale University Press: New Haven, CT, USA; London, UK, 2018. [Google Scholar]
- Agarwal, N.; Meena, C.S.; Raj, B.P.; Saini, L.; Kumar, A.; Gopalakrishnan, N.; Kumar, A.; Balam, N.B.; Alam, T.; Kapoor, N.R. Indoor air quality improvement in COVID-19 pandemic. Sustain. Cities Soc. 2021, 70, 102942. [Google Scholar] [CrossRef]
- Mata, T.M.; Felgueiras, F.; Martins, A.A.; Monteiro, H.; Ferraz, M.P.; Oliveira, G.M.; Gabriel, M.F.; Silva, G.V. Indoor air quality in elderly centers: Pollutants emission and health effects. Environments 2022, 9, 86. [Google Scholar] [CrossRef]
- Lee, E.-J.; Park, S.-J. Biophilic Experience-Based Residential Hybrid Framework. Int. J. Environ. Res. Public Health 2022, 19, 8512. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Park, S.J. The Application of Bio-philic Design Pattern in Housing for Cure of Mental Health-Focused on the Elderly and Baby-boomer. JAIK Plan. Des. 2018, 34, 13–21. [Google Scholar] [CrossRef]
- Hunter, P.R.; MacDonald, A.M.; Carter, R.C. Water supply and health. PLoS Med. 2010, 7, e1000361. [Google Scholar] [CrossRef]
- El-Darwish, I.I. Fractal design in streetscape: Rethinking the visual aesthetics of building elevation composition. Alex. Eng. J. 2019, 58, 957–966. [Google Scholar] [CrossRef]
- Hildebrand, G. The Wright Space: Pattern & Meaning in Frank Lloyd Wright’s Houses; University of Washington: Seattle, WA, USA, 1991. [Google Scholar]
- Boffi, M.; Pola, L.; Fumagalli, N.; Fermani, E.; Senes, G.; Inghilleri, P. Nature experiences of older people for active ageing: An interdisciplinary approach to the co-design of community gardens. Front. Psychol. 2021, 12, 702525. [Google Scholar] [CrossRef]
- Kearney, A.R.; Winterbottom, D. Nearby nature and long-term care facility residents: Benefits and design recommendations. J. Hous. Elder. 2006, 19, 7–28. [Google Scholar] [CrossRef]
- Chaudhury, H.; Cooke, H.A.; Cowie, H.; Razaghi, L. The influence of the physical environment on residents with dementia in long-term care settings: A review of the empirical literature. Gerontologist 2018, 58, e325–e337. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| HRQoL Assessment Items | Details |
|---|---|
| Functional mobility | Limitations in physical movements such as standing up, sitting down, or climbing stairs. |
| Ability to perform daily activities | Restrictions in daily activities such as work, studying, or housework. |
| Pain and discomfort | Limitations caused by physical pain, discomfort, or heartburn. |
| Sensory function | Limitations due to impaired sensory functions such as vision and hearing. |
| Anxiety and depression | Restrictions due to feelings of depression and anxiety. |
| Quality of sleep | Limitations due to insufficient sleep duration and poor sleep quality. |
| Cognitive function and memory | Limitations in recognizing objects and people or recalling familiar information. |
| Hobbies and leisure activities | Restrictions on engaging in hobbies, leisure activities, or travel. |
| Social relationships | Level of physical and emotional closeness with family and peers. |
| Productive activities | Limitations related to productive activities or economic circumstances. |
| Demographic Information | Frequency (n) | % | |
|---|---|---|---|
| Gender | Male | 212 | 50.0 |
| Female | 212 | 50.0 | |
| Age (years) | 50–55 | 91 | 21.5 |
| 56–60 | 86 | 20.3 | |
| 61–65 | 63 | 14.9 | |
| 66–70 | 123 | 29.0 | |
| 71 and above | 61 | 14.4 | |
| Housing type | Apartment | 299 | 70.5 |
| Townhouse | 69 | 16.3 | |
| Detached house | 51 | 12.0 | |
| One-room unit | 5 | 1.1 | |
| Residential floor area (m2) | Less than 33 | 8 | 1.9 |
| 33–66 | 44 | 10.4 | |
| 69–99 | 127 | 30.1 | |
| 102–132 | 172 | 40.6 | |
| More than 133 | 73 | 17.2 | |
| Survey Construct | Number of Items | Likert Scale | Cronbach’s α | |
|---|---|---|---|---|
| HRQoL self-assessment | 10 | 1 = Strongly agree, 5 = Strongly disagree | 0.876 | |
| BRD preferences | Direct experience of nature | 10 | 1 = Not at all preferred, 5 = Strongly preferred | 0.894 |
| Indirect experience of nature | 9 | |||
| Experience of space and place | 9 | |||
| Survey Construct | Items | Item Description | M | SD | |
|---|---|---|---|---|---|
| HRQoL self-assessment | Functional mobility | HQ1 | I sometimes struggle to stand up, sit down, or climb stairs. | 3.25 | 1.04 |
| Ability to perform daily activities | HQ2 | I experience difficulties in personal tasks such as work, housework, or academic activities. | 3.78 | 0.92 | |
| Pain and discomfort | HQ3 | I feel physical pain, discomfort, or heartburn. | 3.60 | 1.05 | |
| Sensory function | HQ4 | I feel discomfort due to dull senses, impaired vision, or reduced hearing. | 3.32 | 1.02 | |
| Anxiety and depression | HQ5 | I have been feeling depressed or anxious lately, and sometimes feel a tightness in my chest. | 3.46 | 1.04 | |
| Quality of sleep | HQ6 | I often become sensitive, feel fatigued, or have difficulty sleeping. | 3.43 | 0.96 | |
| Cognitive function and memory | HQ7 | I struggle to recall familiar words, recognize objects, or identify people. | 3.25 | 1.00 | |
| Hobbies and leisure activities | HQ8 | I feel fearful or hesitant about engaging in hobbies, leisure activities, or travel, and often avoid such activities. | 3.68 | 0.96 | |
| Social relationships | HQ9 | I feel physically or emotionally distant from my peers, family, or friends. | 3.70 | 0.92 | |
| Productive activities | HQ10 | I feel dissatisfied with my level of productive activities or economic situation. | 3.11 | 1.07 | |
| BRD preferences | Direct experience of nature | BRD1 | Lightwell or courtyard | 3.89 | 0.85 |
| BRD2 | Varied angles and patterns of openings for daylight diffusion | 3.68 | 0.91 | ||
| BRD3 | Architectural openings and spatial structures facilitating natural ventilation | 3.85 | 0.84 | ||
| BRD4 | Water features and ornaments (waterways, fountains, wall fountains, cascading water decorations, etc.) | 4.13 | 0.73 | ||
| BRD5 | Skylights or atriums to see the sky | 3.65 | 0.92 | ||
| BRD6 | Large windows providing views of natural environments (trees, sea, mountains, etc.) | 4.10 | 0.79 | ||
| BRD7 | Indoor and outdoor gardens or plant decorations | 3.91 | 0.82 | ||
| BRD8 | Green walls or vertical gardens | 3.75 | 0.96 | ||
| BRD9 | Habitat environments for native species (aquariums, ponds, rooftop gardens, etc.) | 3.28 | 0.95 | ||
| BRD10 | Air-purifying vegetation and shading greenery | 3.54 | 0.95 | ||
| Indirect experience of nature | BRD11 | Realistic or metaphorical depictions of nature (paintings, photographs, videos, etc.) | 3.43 | 0.87 | |
| BRD12 | Murals or decorations depicting nature | 3.42 | 0.83 | ||
| BRD13 | Finishes using natural or recycled materials (stone walls, architectural and interior finishes, handles, etc.) | 3.60 | 0.94 | ||
| BRD14 | Color schemes and palette planning based on natural landscapes | 3.91 | 0.72 | ||
| BRD15 | Architectural elements utilizing organic forms (columns, supports, walls, facades, etc.) | 3.43 | 0.95 | ||
| BRD16 | Ventilation openings and air circulation devices | 3.96 | 0.76 | ||
| BRD17 | Indirect and diffused lighting | 3.97 | 0.74 | ||
| BRD18 | Artificial natural lighting and warm-tone lighting | 3.93 | 1.06 | ||
| BRD19 | Architectural structures or designs mimicking the evolved morphological characteristics of natural organisms | 3.24 | 0.91 | ||
| Experience of space and place | BRD20 | Visually open small-scale resting spaces | 4.19 | 0.72 | |
| BRD21 | Pavilions, shelters, or seating designs that provide a sense of protection | 3.75 | 0.91 | ||
| BRD22 | Balconies, decks, or curtain walls | 3.77 | 0.88 | ||
| BRD23 | Harmonized application of natural materials, textures, and patterns | 3.36 | 0.97 | ||
| BRD24 | Wayfinding information utilizing natural elements and features | 3.65 | 0.87 | ||
| BRD25 | Eco-friendly circulation paths (permeable pavements, parklets, etc.) | 3.81 | 0.83 | ||
| BRD26 | Community gardens and edible landscaping | 3.70 | 0.91 | ||
| BRD27 | Architectural elements reflecting local or regional characteristics (landscape colors, building heights, etc.) | 3.60 | 0.90 | ||
| BRD28 | Informational signage on biophilic applications and effects | 3.47 | 0.91 | ||
| HRQoL Factor M ± SD | Items | Factor Loadings | Eigenvalues | Dispersion Ratio (%) | Cronbach’s α | ||
|---|---|---|---|---|---|---|---|
| 1 | Social-economic QoL: 3.49 ± 0.78 | HQ9 | Social relationships | 0.808 | 4.747 | 47.48 | 0.710 |
| HQ8 | Hobbies and leisure activities | 0.690 | |||||
| HQ10 | Productive activities | 0.561 | |||||
| 2 | Mental-sensory QoL: 3.39 ± 0.79 | HQ4 | Sensory function | 0.780 | 1.191 | 59.41 | 0.752 |
| HQ5 | Anxiety and depression | 0.689 | |||||
| HQ7 | Cognitive function and memory | 0.594 | |||||
| 3 | Physical QoL: 3.5 ± 0.77 | HQ3 | Pain and discomfort | 0.788 | 1.098 | 70.34 | 0.777 |
| HQ2 | Ability to perform daily activities | 0.646 | |||||
| HQ6 | Quality of sleep | 0.625 | |||||
| HQ1 | Functional mobility | 0.613 | |||||
| Cluster | CL1 | CL2 | CL3 | CL4 | F | |
| Name | Optimal Health Group | Physically Declining Group | Overall Low Health Group | Socially Vulnerable Group | ||
| N (%) | 169 (39.8) | 124 (29.2) | 61 (14.4) | 70 (16.5) | ||
| HRQoL factor M ± SD | Physical QoL | 4.10 ± 0.71 | 2.92 ± 0.72 | 2.23 ± 0.74 | 3.26 ± 0.81 | 325.400 *** |
| Mental-sensory QoL | 4.23 ± 0.75 | 3.43 ± 0.74 | 2.41 ± 0.82 | 3.19 ± 0.92 | 242.906 *** | |
| Social-economic QoL | 4.10 ± 0.74 | 3.54 ± 0.71 | 2.75 ± 0.89 | 2.60 ± 0.83 | 200.586 *** | |
| Items | Optimal Health Group | Physically Declining Group | Overall Low Health Group | Socially Vulnerable Group | F | η2 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |||
| BRD1 | 3.91 | 0.89 | 3.77 | 0.77 | 4.02 | 0.85 | 3.93 | 0.87 | 1.302 | - |
| BRD2 | 3.81 | 0.94 | 3.60 | 0.75 | 3.80 | 1.01 | 3.41 | 0.94 | 3.953 ** | 0.027 |
| BRD3 | 3.85 | 0.94 | 3.91 | 0.75 | 3.89 | 0.9 | 3.73 | 0.71 | 0.437 | - |
| BRD4 | 4.15 | 0.75 | 4.10 | 0.70 | 4.20 | 0.79 | 4.07 | 0.67 | 0.733 | - |
| BRD5 | 3.69 | 0.96 | 3.57 | 0.80 | 3.79 | 1.07 | 3.54 | 0.88 | 1.175 | - |
| BRD6 | 4.09 | 0.82 | 4.14 | 0.71 | 4.05 | 0.78 | 4.10 | 0.87 | 0.186 | - |
| BRD7 | 3.89 | 0.85 | 3.90 | 0.82 | 4.13 | 0.72 | 3.80 | 0.83 | 2.347 * | 0.016 |
| BRD8 | 3.81 | 0.99 | 3.66 | 0.91 | 3.51 | 0.99 | 3.94 | 0.93 | 2.823 * | 0.021 |
| BRD9 | 3.64 | 0.98 | 3.65 | 0.75 | 3.70 | 0.88 | 3.59 | 0.91 | 0.197 | - |
| BRD10 | 3.67 | 0.94 | 3.53 | 0.95 | 3.38 | 1.00 | 3.37 | 0.87 | 2.508 | - |
| BRD11 | 3.47 | 0.91 | 3.51 | 0.77 | 3.41 | 0.99 | 3.23 | 0.82 | 1.741 * | 0.012 |
| BRD12 | 3.46 | 0.84 | 3.39 | 0.83 | 3.34 | 0.91 | 3.44 | 0.73 | 0.353 | - |
| BRD13 | 3.70 | 0.94 | 3.63 | 0.84 | 3.51 | 0.99 | 3.39 | 1.04 | 2.616 * | 0.018 |
| BRD14 | 4.00 | 0.72 | 3.81 | 0.74 | 3.90 | 0.72 | 3.89 | 0.69 | 2.576 * | 0.018 |
| BRD15 | 3.51 | 0.96 | 3.48 | 0.88 | 3.20 | 1.14 | 3.37 | 0.80 | 1.887 | - |
| BRD16 | 4.07 | 0.83 | 3.92 | 0.65 | 3.98 | 0.67 | 3.79 | 0.80 | 2.481 * | 0.017 |
| BRD17 | 4.02 | 0.79 | 3.98 | 0.66 | 3.89 | 0.73 | 3.93 | 0.73 | 0.590 | - |
| BRD18 | 4.02 | 1.03 | 3.79 | 1.14 | 4.10 | 0.98 | 3.83 | 1.01 | 1.907 | - |
| BRD19 | 3.34 | 0.95 | 3.23 | 0.84 | 3.18 | 0.87 | 3.07 | 0.92 | 2.623 * | 0.018 |
| BRD20 | 4.22 | 0.71 | 4.15 | 0.71 | 4.15 | 0.79 | 4.19 | 0.73 | 0.302 | - |
| BRD21 | 3.86 | 0.86 | 3.72 | 0.93 | 3.70 | 0.99 | 3.61 | 0.91 | 1.414 | - |
| BRD22 | 3.91 | 0.82 | 3.77 | 0.87 | 3.59 | 0.97 | 3.63 | 0.92 | 2.830 * | 0.021 |
| BRD23 | 3.46 | 0.99 | 3.34 | 0.86 | 3.15 | 1.09 | 3.34 | 0.98 | 1.628 | - |
| BRD24 | 3.82 | 0.88 | 3.57 | 0.82 | 3.43 | 0.90 | 3.57 | 0.84 | 4.031 *** | 0.028 |
| BRD25 | 3.95 | 0.79 | 3.76 | 0.78 | 3.75 | 0.98 | 3.63 | 0.82 | 2.963 * | 0.021 |
| BRD26 | 3.80 | 0.94 | 3.65 | 0.83 | 3.70 | 0.95 | 3.53 | 0.91 | 1.622 | - |
| BRD27 | 3.59 | 0.95 | 3.66 | 0.78 | 3.57 | 1.01 | 3.54 | 0.88 | 0.314 | - |
| BRD28 | 3.59 | 0.95 | 3.44 | 0.76 | 3.26 | 1.11 | 3.39 | 0.84 | 2.327 | - |
| Total | 3.82 | 0.53 | 3.71 | 0.63 | 3.69 | 0.71 | 3.64 | 0.84 | - | - |
| Cluster | HRQoL Profile | Key Design Needs | Keywords |
|---|---|---|---|
| Optimal Health Group | High across physical, cognitive, and social dimensions | Open and flexible layouts allowing active engagement; multi-sensory stimulation; strong visual and physical connections with nature | Autonomy, diversity, openness |
| Physically Declining Group | Decline in physical functions, moderate in others | Short-distance movement; quiet, restorative green areas; sheltered and ventilated environments for comfort | Protection, recovery, safety |
| Overall Low Health Group | Overall low, particularly in cognitive and emotional functions | Clear zoning and orientation cues; sensory safety through material and color familiarity; simplified circulation | Cognitive clarity, sensory guidance |
| Socially Vulnerable Group | Low in social connection and emotional stability | Shared green spaces; nature-linked communal zones; visual openness toward outdoors to reduce isolation | Communication, external connection, visual openness |
| HRQoL-Based Cluster | Profile Summary | * Key BRD Elements | Design Strategies | Example Application Spaces |
|---|---|---|---|---|
| Optimal Health Group |
| BRD2, BRD8, BRD13, BRD14, BRD16 BRD25, BRD22 |
| Living rooms, balconies, home offices, flexible open-plan spaces |
| Physically Declining Group |
| BRD7, BRD10, BRD8, BRD14, BRD16 BRD25 |
| Indoor courtyards, indoor gardens, bench seating, corridors |
| Overall Low Health Group |
| BRD2, BRD13, BRD14, BRD16 BRD11, BRD24 |
| Bedrooms, entryways, corridors, personal rest areas, communal zones |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, E.-J.; Park, S.-J. Strategic Biophilic Residential Design Based on Seniors’ Health Profiles: A HRQoL-Driven Approach. Buildings 2025, 15, 1792. https://doi.org/10.3390/buildings15111792
Lee E-J, Park S-J. Strategic Biophilic Residential Design Based on Seniors’ Health Profiles: A HRQoL-Driven Approach. Buildings. 2025; 15(11):1792. https://doi.org/10.3390/buildings15111792
Chicago/Turabian StyleLee, Eun-Ji, and Sung-Jun Park. 2025. "Strategic Biophilic Residential Design Based on Seniors’ Health Profiles: A HRQoL-Driven Approach" Buildings 15, no. 11: 1792. https://doi.org/10.3390/buildings15111792
APA StyleLee, E.-J., & Park, S.-J. (2025). Strategic Biophilic Residential Design Based on Seniors’ Health Profiles: A HRQoL-Driven Approach. Buildings, 15(11), 1792. https://doi.org/10.3390/buildings15111792