
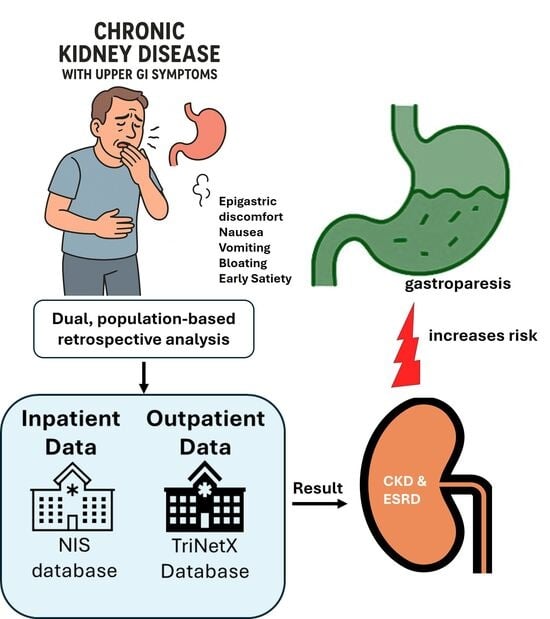
The Hidden Burden of Gastroparesis in Chronic Kidney Disease: Evidence from Inpatient and Outpatient Cohorts for Personalized Care

 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Database
2.2. Data Collection and Outcomes
2.3. Statistical Analysis
3. Results

4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| Abbreviation | Full Term |
| CKD | Chronic Kidney Disease |
| GI | Gastrointestinal |
| NIS | National Inpatient Sample |
| HCUP | Healthcare Cost and Utilization Project |
| TriNetX | TriNetX Research Network |
| EHR | Electronic Health Record |
| ICD-10-CM | International Classification of Diseases, 10th Revision, Clinical Modification |
| T2DM | Type 2 Diabetes Mellitus |
| HTN | Hypertension |
| PUD | Peptic Ulcer Disease |
| FD | Functional Dyspepsia |
| EE | Eosinophilic Esophagitis |
| GERD | Gastroesophageal Reflux Disease |
| URM | Uremic Retention Molecules |
| BMI | Body Mass Index |
| ESRD | End-Stage Renal Disease |
| GLP-1 | Glucagon-Like Peptide-1 |
| OR | Odds Ratio |
| CI | Confidence Interval |
| SIBO | Small Intestinal Bacterial Overgrowth |
| nNOS | Neuronal Nitric Oxide Synthase |
| NO | Nitric Oxide |
| LES | Lower Esophageal Sphincter |
| WT | Wild Type |
| MMC | Migrating Motor Complex |
| IMC | Interdigestive Myoelectric Complex |
| ADMA | Asymmetric Dimethylarginine |
| HD | Hemodialysis |
| EGD | Esophagogastroduodenoscopy |
References
- Johansen, K.L.; Gilbertson, D.T.; Li, S.; Li, S.; Liu, J.; Roetker, N.S.; Hart, A.; Knapp, C.D.; Ku, E.; Powe, N.R.; et al. US Renal Data System 2024 Annual Data Report: Epidemiology of Kidney Disease in the United States. Am. J. Kidney Dis. 2025, 85, A8–A11. [Google Scholar] [CrossRef]
- Karahan, D.; Şahin, İ. Comparison of gastrointestinal symptoms and findings in renal replacement therapy modalities. BMC Nephrol. 2022, 23, 261. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.J.; Harrison, L.E.; Hoad, C.L.; Marciani, L.; Gowland, P.A.; McIntyre, C.W. Patients with Chronic Kidney Disease Have Abnormal Upper Gastro-Intestinal Tract Digestive Function: A Study of Uremic Enteropathy. J. Gastroenterol. Hepatol. 2017, 32, 372–377. [Google Scholar] [CrossRef] [PubMed]
- Lew, S.Q.; Radhakrishnan, J. Chapter 25—Chronic Kidney Disease and Gastrointestinal Disorders. In Chronic Renal Disease; Kimmel, P.L., Rosenberg, M.E., Eds.; Academic Press: San Diego, CA, USA, 2015; pp. 298–309. [Google Scholar]
- Sandoval Terra Campos Guelli, M.; Correa, T.; Silva, I.; Zampier, D.; Costa, L.; Dias, L.; Guidoreni, A. Mo558: Chronic Kidney Disease and Gastroparesis: What Is the Association? Nephrol. Dial. Transplant. 2022, 37 (Suppl. 3), gfac074-003. [Google Scholar] [CrossRef]
- De Schoenmakere, G.; Vanholder, R.; Rottey, S.; Duym, P.; Lameire, N. Relationship between Gastric Emptying and Clinical and Biochemical Factors in Chronic Haemodialysis Patients. Nephrol. Dial. Transplant. 2001, 16, 1850–1855. [Google Scholar] [CrossRef]
- Strid, H.; Simrén, M.; Stotzer, P.O.; Abrahamsson, H.; Björnsson, E.S. Delay in Gastric Emptying in Patients with Chronic Renal Failure. Scand. J. Gastroenterol. 2004, 39, 516–520. [Google Scholar] [CrossRef]
- Camilleri, M.; Kuo, B.; Nguyen, L.; Vaughn, V.M.; Petrey, J.; Greer, K.; Yadlapati, R.; Abell, T.L. Acg Clinical Guideline: Gastroparesis. Am. J. Gastroenterol. 2022, 117, 1197–1220. [Google Scholar] [CrossRef] [PubMed]
- Choung, R.S.; Locke, G.R., 3rd; Schleck, C.D.; Zinsmeister, A.R.; Melton, L.J., 3rd; Talley, N.J. Risk of Gastroparesis in Subjects with Type 1 and 2 Diabetes in the General Population. Am. J. Gastroenterol. 2012, 107, 82–88. [Google Scholar] [CrossRef]
- Jung, H.K.; Choung, R.S.; Locke, G.R., 3rd; Schleck, C.D.; Zinsmeister, A.R.; Szarka, L.A.; Mullan, B.; Talley, N.J. The Incidence, Prevalence, and Outcomes of Patients with Gastroparesis in Olmsted County, Minnesota, from 1996 to 2006. Gastroenterology 2009, 136, 1225–1233. [Google Scholar] [CrossRef]
- Shen, S.; Xu, J.; Lamm, V.; Vachaparambil, C.T.; Chen, H.; Cai, Q. Diabetic Gastroparesis and Nondiabetic Gastroparesis. Gastrointest. Endosc. Clin. N. Am. 2019, 29, 15–25. [Google Scholar] [CrossRef]
- Young, C.F.; Moussa, M.; Shubrook, J.H. Diabetic Gastroparesis: A Review. Diabetes Spectr. 2020, 33, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Singh, I.; Baker, C.; Underkofler, C.; Rasouli, N. Diabetic Gastroparesis: An Overview of Pathogenesis, Clinical Presentation and Novel Therapies, with a Focus on Ghrelin Receptor Agonists. J. Diabetes its Complicat. 2021, 35, 107733. [Google Scholar] [CrossRef] [PubMed]
- Almogbel, R.A.; Alhussan, F.A.; Alnasser, S.A.; Algeffari, M.A. Prevalence and Risk Factors of Gastroparesis-Related Symptoms among Patients with Type 2 Diabetes. Int. J. Health Sci. 2016, 10, 379–386. [Google Scholar] [CrossRef]
- Eguchi, E. Dietary modifications achieved successful resolution of symptoms of gastroparesis diagnosed by demonstrating gastric food retention after overnight fasting in diabetic dialysis patients: Two case reports with literature review. Ren. Replace. Ther. 2020, 6, 62. [Google Scholar] [CrossRef]
- Ives, D.; Brown, S.; Phillips, S. Gastroparesis in the Chronic Kidney Disease Patient: Clinical Management and Implications for Practice. J. Ren. Nutr. 2023, 33, e1–e3. [Google Scholar] [CrossRef]
- Tuttle, K.R.; Agarwal, R.; Alpers, C.E.; Bakris, G.L.; Brosius, F.C.; Kolkhof, P.; Uribarri, J. Molecular Mechanisms and Therapeutic Targets for Diabetic Kidney Disease. Kidney Int. 2022, 102, 248–260. [Google Scholar] [CrossRef]
- Cheng, H.T.; Xu, X.; Lim, P.S.; Hung, K.Y. Worldwide Epidemiology of Diabetes-Related End-Stage Renal Disease, 2000–2015. Diabetes Care 2021, 44, 89–97. [Google Scholar] [CrossRef]
- Schol, J.; Wauters, L.; Dickman, R.; Drug, V.; Mulak, A.; Serra, J.; Enck, P.; Tack, J. United European Gastroenterology (Ueg) and European Society for Neurogastroenterology and Motility (Esnm) Consensus on Gastroparesis. United Eur. Gastroenterol. J. 2021, 9, 287–306. [Google Scholar] [CrossRef]
- Camilleri, M.; Sanders, K.M. Gastroparesis. Gastroenterology 2022, 162, 68–87.e1. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Kudva, Y.; Basu, A.; Camilleri, M.; Low, P.A.; Vella, A.; Zinsmeister, A.R. Relationship between Glycemic Control and Gastric Emptying in Poorly Controlled Type 2 Diabetes. Clin. Gastroenterol. Hepatol. 2015, 13, 466–476.e1. [Google Scholar] [CrossRef]
- Camilleri, M.; Zheng, T.; Vosoughi, K.; Lupianez-Merly, C.; Eckert, D.; Busciglio, I.; Burton, D.; Dilmaghani, S. Optimal Measurement of Gastric Emptying of Solids in Gastroparesis or Functional Dyspepsia: Evidence to Establish Standard Test. Gut 2023, 72, 2241–2249. [Google Scholar] [CrossRef]
- Syed, A.R.; Wolfe, M.M.; Calles-Escandon, J. Epidemiology and Diagnosis of Gastroparesis in the United States: A Population-based Study. J. Clin. Gastroenterol. 2020, 54, 50–54. [Google Scholar] [CrossRef]
- Huang, I.H.; Schol, J.; Carbone, F.; Chen, Y.J.; Van den Houte, K.; Balsiger, L.M.; Broeders, B.; Vanuytsel, T.; Tack, J. Prevalence of Delayed Gastric Emptying in Patients with Gastroparesis-Like Symptoms. Aliment. Pharmacol. Ther. 2023, 57, 773–782. [Google Scholar] [CrossRef]
- Richter, J.E.; Rubenstein, J.H. Presentation and Epidemiology of Gastroesophageal Reflux Disease. Gastroenterology 2018, 154, 267–276. [Google Scholar] [CrossRef]
- Wang, X.; Wright, Z.; Patton-Tackett, E.D.; Song, G. The Relationship between Gastroesophageal Reflux Disease and Chronic Kidney Disease. J. Pers. Med. 2023, 13, 827. [Google Scholar] [CrossRef]
- Wang, X.; Wright, Z.; Wang, J.; Frandah, W.M.; Song, G. Chronic Kidney Disease Linked to Higher Incidence of Gastric Diseases. Gastrointest. Disord. 2023, 5, 329–339. [Google Scholar] [CrossRef]
- Rey, E.; Choung, R.S.; Schleck, C.D.; Zinsmeister, A.R.; Talley, N.J.; Locke, G.R., 3rd. Prevalence of Hidden Gastroparesis in the Community: The Gastroparesis "Iceberg". J. Neurogastroenterol. Motil. 2012, 18, 34–42. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.R.; Fisher, R.S.; Parkman, H.P. Gastroparesis-related hospitalizations in the United States: Trends, characteristics, and outcomes, 1995–2004. Am. J. Gastroenterol. 2008, 103, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, P.; Agarwal, R.; Chan, J.C.N.; Levin, A.; Kalyesubula, R.; Karam, S.; Nangaku, M.; Rodríguez-Iturbe, B.; Anders, H.-J. Chronic Kidney Disease. Nat. Rev. Dis. Primers 2025, 11, 8. [Google Scholar] [CrossRef]
- Kovesdy, C.P. Epidemiology of chronic kidney disease: An update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar]
- Webster, A.C.; Nagler, E.V.; Morton, R.L.; Masson, P. Chronic Kidney Disease. Lancet 2017, 389, 1238–1252. [Google Scholar] [CrossRef]
- Thomas, M.C.; Brownlee, M.; Susztak, K.; Sharma, K.; Jandeleit-Dahm, K.A.; Zoungas, S.; Rossing, P.; Groop, P.H.; Cooper, M.E. Diabetic Kidney Disease. Nat. Rev. Dis. Primers 2015, 1, 15018. [Google Scholar] [CrossRef]
- Bharucha, A.E.; Kudva, Y.C.; Prichard, D.O. Diabetic Gastroparesis. Endocr. Rev. 2019, 40, 1318–1352. [Google Scholar] [CrossRef]
- Van Vlem, B.; Schoonjans, R.; Vanholder, R.; Vandamme, W.; De Vos, M.; Lameire, N. Dyspepsia and Gastric Emptying in Chronic Renal Failure Patients. Clin. Nephrol. 2001, 56, 302–307. [Google Scholar]
- Hirako, M.; Kamiya, T.; Misu, N.; Kobayashi, Y.; Adachi, H.; Shikano, M.; Matsuhisa, E.; Kimura, G. Impaired Gastric Motility and Its Relationship to Gastrointestinal Symptoms in Patients with Chronic Renal Failure. J. Gastroenterol. 2005, 40, 1116–1122. [Google Scholar] [CrossRef]
- Zoccali, C.; Mallamaci, F.; Kanbay, M.; Tuttle, K.R.; Kotanko, P.; De Caterina, R.; Grassi, G.; Mancia, G. The Autonomic Nervous System and Inflammation in Chronic Kidney Disease. Nephrol. Dial. Transplant. 2025, 40, 1470–1482. [Google Scholar] [CrossRef] [PubMed]
- Allison, S.J. Study reveals link between autonomic imbalance and kidney disease. Nat. Rev. Nephrol. 2010, 6, 631. [Google Scholar] [CrossRef]
- Fu, R.-G.; Wang, Y.; Yuan, H.-Z.; Zhou, J.-P.; Wang, L.; Liu, X.-D.; Ma, F.; Zhang, J. Effects of Chronic Renal Failure on Gastrointestinal Motility: A Study on the Changes of Gastric Emptying, Small Intestinal Transit, Interdigestive Myoelectric Complex, and Fecal Water Content. Ren. Fail. 2011, 33, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Fouque, D.; Pelletier, S.; Mafra, D.; Chauveau, P. Nutrition and Chronic Kidney Disease. Kidney Int. 2011, 80, 348–357. [Google Scholar] [CrossRef]
- Stotzer, P.-O.; Björnsson, E.S.; Abrahamsson, H. Interdigestive and postprandial motility in small-intestinal bacterial overgrowth. Scand. J. Gastroenterol. 1996, 31, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Vantrappen, G.; Janssens, J.; Hellemans, J.; Ghoos, Y. The Interdigestive Motor Complex of Normal Subjects and Patients with Bacterial Overgrowth of the Small Intestine. J. Clin. Investig. 1977, 59, 1158–1166. [Google Scholar] [CrossRef]
- Evenepoel, P.; Meijers, B.K.; Bammens, B.R.; Verbeke, K. Uremic Toxins Originating from Colonic Microbial Metabolism. Kidney Int. 2009, 76, S12–S19. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, M.; Bonazzi, P.; Scarpellini, E.; Bendia, E.; Lauritano, E.C.; Fasano, A.; Ceravolo, M.G.; Capecci, M.; Bentivoglio, A.R.; Provinciali, L.; et al. Prevalence of small intestinal bacterial overgrowth in Parkinson’s disease. Mov. Disord. 2011, 26, 889–892. [Google Scholar] [CrossRef] [PubMed]
- Bures, J.; Cyrany, J.; Kohoutova, D.; Förstl, M.; Rejchrt, S.; Kvetina, J.; Vorisek, V.; Kopacova, M. Small Intestinal Bacterial Overgrowth Syndrome. World J. Gastroenterol. 2010, 16, 2978–2990. [Google Scholar] [CrossRef]
- Wu, Y.; Xie, N.; Yu, Y.; Li, B. Baiwen Pathogenesis and Endoscopic Treatment of Gastroparesis. Gastroenterol. Endosc. 2023, 1, 110–117. [Google Scholar] [CrossRef]
- Pasricha, P.J.; Grover, M.; Yates, K.P.; Abell, T.L.; Koch, K.L.; McCallum, R.W.; Sarosiek, I.; Bernard, C.E.; Kuo, B.; Bulat, R.; et al. Progress in Gastroparesis—A Narrative Review of the Work of the Gastroparesis Clinical Research Consortium. Clin. Gastroenterol. Hepatol. 2022, 20, 2684–2695.e3. [Google Scholar] [CrossRef]
- Cairns, B.R.; Jevans, B.; Chanpong, A.; Moulding, D.; McCann, C.J. Automated Computational Analysis Reveals Structural Changes in the Enteric Nervous System of Nnos Deficient Mice. Sci. Rep. 2021, 11, 17189. [Google Scholar] [CrossRef]
- Hoibian, E.; Florens, N.; Koppe, L.; Vidal, H.; Soulage, C.O. Distal Colon Motor Dysfunction in Mice with Chronic Kidney Disease: Putative Role of Uremic Toxins. Toxins 2018, 10, 204. [Google Scholar] [CrossRef]
- Mashimo, H.; Kjellin, A.; Goyal, R.K. Gastric stasis in neuronal nitric oxide synthase-deficient knockout mice. Gastroenterology 2000, 119, 766–773. [Google Scholar] [CrossRef]
- Baylis, C. Nitric oxide deficiency in chronic kidney disease. Am. J. Physiol.-Ren. Physiol. 2008, 294, F1–F9. [Google Scholar] [CrossRef]
- Erdely, A.; Wagner, L.; Muller, V.; Szabo, A.; Baylis, C. Protection of Wistar Furth Rats from Chronic Renal Disease Is Associated with Maintained Renal Nitric Oxide Synthase. J. Am. Soc. Nephrol. 2003, 14, 2526–2533. [Google Scholar] [CrossRef][Green Version]
- Muller, V.; Tain, Y.-L.; Croker, B.; Baylis, C. Chronic Nitric Oxide Deficiency and Progression of Kidney Disease after Renal Mass Reduction in the C57bl6 Mouse. Am. J. Nephrol. 2010, 32, 575–580. [Google Scholar] [CrossRef] [PubMed]
- Salera, D.; Merkel, N.; Bellasi, A.; de Borst, M.H. Pathophysiology of Chronic Kidney Disease–Mineral Bone Disorder (Ckd-Mbd): From Adaptive to Maladaptive Mineral Homeostasis. Clin. Kidney J. 2025, 18, i3–i14. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.J.; Yokota, S.; Tracy, T.S.; Sorkin, M.I.; Baylis, C. Nitric Oxide Production Is Low in End-Stage Renal Disease Patients on Peritoneal Dialysis. Am. J. Physiol. 1999, 276, F794–F797. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Inpatient CKD | Inpatient Non-CKD | Outpatient CKD | Outpatient Non-CKD | Outpatient CKD | Outpatient Non-CKD | |
|---|---|---|---|---|---|---|
| Pre-Propensity matching | Post- Propensity matching | |||||
| Total number of patients | 502,770 | 3,076,602 | 422,238 | 5,841,013 | 404,359 | 404,359 |
| Age | ||||||
| 62.4 ± 0.1 | 47.5 ± 0.1 | 68.6 ± 17.6 * | 37.3 ± 22.8 * | 68.0 ± 17.7 | 68.1 ± 17.6 | |
| Gender | ||||||
| Female | 234,733 (53.3%) | 1,783,893 (63.4%) | 229,787(54.5%) * | 3,496,771 (60.6%) * | 223,309 (55.2%) | 222,943 (55.1%) |
| Male | 268,037 (46.7%) | 1,292,709 (36.6%) | 174,517 (41.4%) * | 2,122,644 (36.8%) * | 164,201 (40.6%) | 164,556 (40.7%) |
| Race | ||||||
| White | 311,646 (53.8%) | 1,900,025 (62.4%) | 260,541 (61.7%) * | 3,545,903 (61.5%) * | 252,584 (62.5%) | 254,048 (62.8%) |
| Black | 101,463 (27.1%) | 423,511 (17.1%) | 81,801 (19.4%) * | 882,360 (15.3%) * | 75,752 (18.7%) | 74,776 (18.5%) |
| Hispanic | 47,439 (11.4%) | 380,646 (11.3%) | 37,771 (9.0%) * | 869,601 (15.1%) * | 36,787 (9.1%) | 37,226 (9.2%) |
| Asian | 13,230 (2.3%) | 93,619 (2.2%) | 17,020 (4.0%) | 232,557 (4.0%) | 16,268 (4.0%) | 16,037 (4.0%) |
| Risk factors | ||||||
| T2DM | 25,053 (34.3%) | 309,459 (24.9%) | 186,899 (44.3%) * | 353,951 (6.1%) * | 169,490 (41.9%) | 169,854 (42.0%) |
| Smoking | 49,639 (11.0%) | 422,314 (16.1%) | 33,950 (8.0%) * | 235,692 (4.1%) * | 32,301 (8.0%) | 32,608 (8.1%) |
| Hypertension | 254,375 (46.6%) | 1,001,862 (39.9%) | 336,850 (79.8%) * | 864,007 (15.0%) * | 319,280 (79.0%) | 319,253 (79.0%) |
| Hyperlipidemia | 234,552 (52.2%) | 640,711 (24.6%) | 221,849 (52.6%) * | 517,893 (9.0%) * | 205,477 (50.8%) | 203,178 (50.2%) |
| GLP-1A | N/A | N/A | 24,728 (5.9%) * | 67,283 (1.2%) * | 23,259 (5.8%) | 21,588 (5.3%) |
| Gastroparesis | |||||
|---|---|---|---|---|---|
| Case | Prevalence | p Value | Adjusted OR (CI) | p Value | |
| non-CKD | 34,600 | 0.57% | |||
| CKD | 18,953 | 1.88% | <0.01 | 4.287 (4.119–4.377) | <0.01 |
| CKD stage 1 | 106 | 1.98% | <0.01 | 3.541 (2.914–4.302) | <0.01 |
| CKD stage 2 | 655 | 1.34% | <0.01 | 2.386 (2.204–2.583) | <0.01 |
| CKD stage 3 | 5035 | 1.26% | <0.01 | 2.299 (2.226–2.373) | <0.01 |
| CKD stage 4 | 1926 | 1.76% | <0.01 | 3.048 (2.905–3.198) | <0.01 |
| CKD stage 5 | 308 | 2.11% | <0.01 | 3.791 (3.381–4.250) | <0.01 |
| ESRD | 8305 | 4.06% | <0.01 | 8.079 (7.874–8.289) | <0.01 |
| Gastroparesis | |||||||
|---|---|---|---|---|---|---|---|
| Census | Propensity Matching | Number of Outcomes | ARD | Odds Ratio | 95% CI | p Value | |
| CKD | 422,238 | 404,359 | 14,550 | 1.80% | 2.15 | (2.089, 2.214) * | <0.001 |
| Non-CKD | 5,841,013 | 404,359 | 6899 | ||||
| CKD-Stage 1 | 5921 | 5920 | 159 | 1.20% | 1.895 | (1.452, 2.472) * | <0.001 |
| Non-CKD | 5,656,007 | 5920 | 85 | ||||
| CKD-Stage 2 | 24,391 | 24,214 | 658 | 1.20% | 1.825 | (1.604, 2.077) * | <0.001 |
| Non-CKD | 5,841,013 | 24,214 | 365 | ||||
| CKD-Stage 3 | 88,479 | 88,478 | 1409 | 0.10% | 1.043 | (0.967, 1.124) | 0.274 |
| Non-CKD | 5,841,013 | 88,478 | 1352 | ||||
| CKD-Stage 4 | 4125 | 4124 | 52 | −0.20% | 0.865 | (0.595, 1.257) | 0.447 |
| Non-CKD | 5,841,013 | 4124 | 60 | ||||
| CKD-Stage 5 | 629 | 629 | 14 | −0.30% | 0.872 | (0.422, 1.802) | 0.712 |
| Non-CKD | 5,577,009 | 629 | 16 | ||||
| ESRD | 12,117 | 12,116 | 605 | 3% | 2.753 | (2.358, 3.213) * | <0.001 |
| Non-CKD | 5,466,574 | 12,116 | 227 | ||||
| HD-CKD | 30,414 | 30,413 | 2192 | 1.60% | 1.304 | (1.221, 1.392) * | <0.001 |
| HD | 387,236 | 30,413 | 1710 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, X.; Almetwali, O.; Marino-Melendez, A.; Tan, D.; Wang, J.; Song, G. The Hidden Burden of Gastroparesis in Chronic Kidney Disease: Evidence from Inpatient and Outpatient Cohorts for Personalized Care. J. Pers. Med. 2025, 15, 600. https://doi.org/10.3390/jpm15120600
Wang X, Almetwali O, Marino-Melendez A, Tan D, Wang J, Song G. The Hidden Burden of Gastroparesis in Chronic Kidney Disease: Evidence from Inpatient and Outpatient Cohorts for Personalized Care. Journal of Personalized Medicine. 2025; 15(12):600. https://doi.org/10.3390/jpm15120600
Chicago/Turabian StyleWang, Xiaoliang, Omar Almetwali, Armando Marino-Melendez, Darwin Tan, Jiayan Wang, and Gengqing Song. 2025. "The Hidden Burden of Gastroparesis in Chronic Kidney Disease: Evidence from Inpatient and Outpatient Cohorts for Personalized Care" Journal of Personalized Medicine 15, no. 12: 600. https://doi.org/10.3390/jpm15120600
APA StyleWang, X., Almetwali, O., Marino-Melendez, A., Tan, D., Wang, J., & Song, G. (2025). The Hidden Burden of Gastroparesis in Chronic Kidney Disease: Evidence from Inpatient and Outpatient Cohorts for Personalized Care. Journal of Personalized Medicine, 15(12), 600. https://doi.org/10.3390/jpm15120600