

Immunohistochemical Profiling of PD-1, PD-L1, CD8, MSI, and p53 and Prognostic Implications in Advanced Serous Ovarian Carcinoma: A Retrospective Study

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. Histological Analysis
2.3. Immunohistochemical Tests
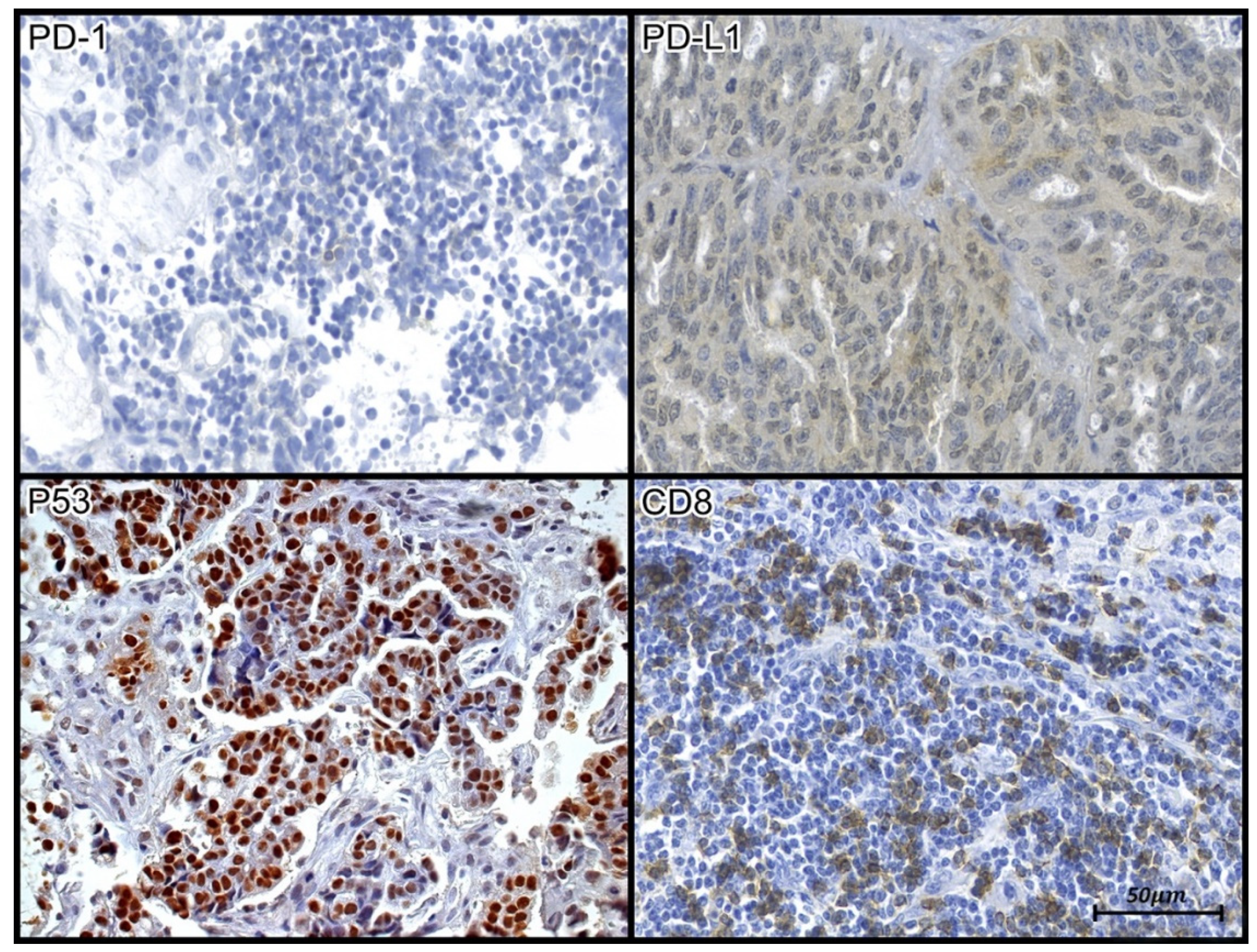
2.4. PD-1, PD-L1, CD8, and p53
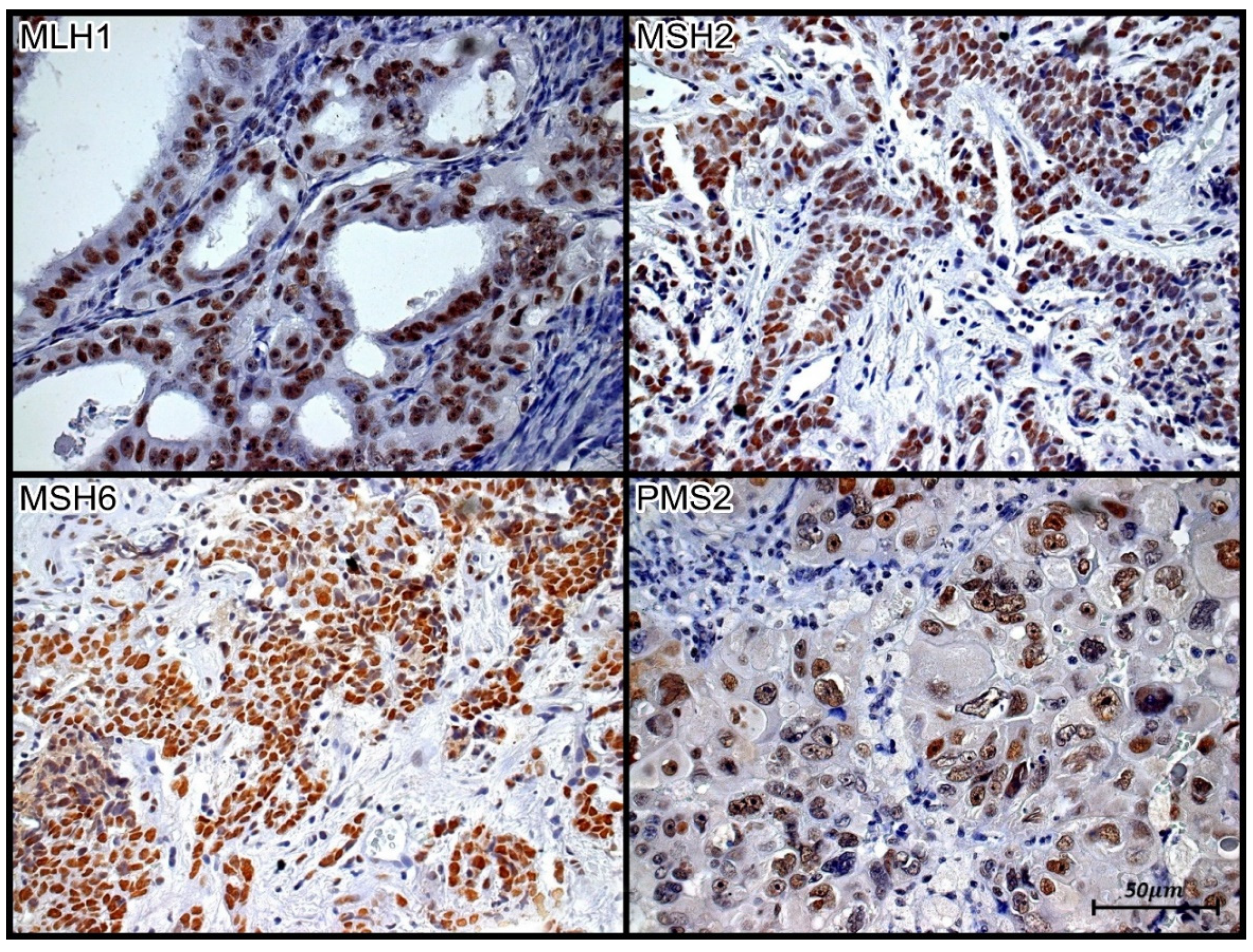
2.5. MLH1, MSH2, MSH6 and PMS2
2.6. Tissue Immunoexpression Analysis
2.6.1. PD-L1
2.6.2. CD8 and PD-1
2.6.3. MLH1, MSH2, MSH6, and PMS2
2.6.4. p53
2.7. Statistical Analysis
3. Results


{kind=link}
{kind=link}
{kind=link}
| Marker | Status of MSI | n 1 | Median (Min–Max) | IQR 2 | p * |
|---|---|---|---|---|---|
| PD-1 | stable | 23 | 16.0 (1.0–62.0) | 29.0 | 0.272 |
| unstable | 4 | 6.0 (3.0–17.0) | 9.0 | ||
| CD8/PD-1 | stable | 23 | 12.5 (0.1–77.0) | 37.1 | 0.049 |
| unstable | 4 | 1.8 (0.7–7.6) | 4.5 | ||
| PD-L1 | stable | 22 | 9.8 (0.5–72.4) | 11.5 | 0.471 |
| unstable | 4 | 5.0 (0.8–51.3) | 27.6 |
| Variable | n 1 | Relapse | p * | |
|---|---|---|---|---|
| n (%) | ||||
| p53 | overexpressed | 22 | 12 (54.5) | 0.496 |
| wild type | 4 | 2 (50.0) | ||
| MSI | stable | 23 | 10 (43.5) | 0.031 |
| unstable | 4 | 4 (100.0) | ||
| Clinical stage | III | 19 | 9 (47.4) | 0.948 |
| IV | 8 | 6 (75.0) | ||
| Grade of serous carcinoma | high | 21 | 13 (61.9) | 0.862 |
| low | 7 | 2 (28.6) | ||
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Globocan. The Global Cancer Observatory. 2020. Available online: https://gco.iarc.fr/ (accessed on 8 March 2021).
- INCA—Instituto Nacional do Câncer. 2020. Available online: www.inca.gov.br (accessed on 8 March 2021).
- Burger, R.A.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Monk, B.J.; Huang, H.; Mannel, R.S.; Homesley, H.D.; Fowler, J.; Greer, B.E.; et al. Incorporation of bevacizumab in the primary treatment of ovarian cancer. N. Engl. J. Med. 2011, 365, 2473–2483. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance olaparib in patients with newly diagnosed advanced ovarian cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef]
- Coleman, R.L.; Fleming, G.F.; Brady, M.F.; Swisher, E.M.; Steffensen, K.D.; Friedlander, M.; Okamoto, A.; Moore, K.N.; Efrat Ben-Baruch, N.; Werner, T.L.; et al. Veliparib with first-line chemotherapy and as maintenance therapy in ovarian cancer. N. Engl. J. Med. 2019, 381, 2403–2415. [Google Scholar] [CrossRef] [PubMed]
- González-Martín, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in patients with newly diagnosed advanced ovarian cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef]
- Openshaw, M.R.; Fotopoulou, C.; Blagden, S.; Gabra, H. The next steps in improving the outcomes of advanced ovarian cancer. Womens Health 2015, 11, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Mouw, K.W.; Goldberg, M.S.; Konstantinopoulos, P.A.; D’Andrea, A.D. DNA damage and repair biomarkers of immuno-therapy response. Cancer Discov. 2017, 7, 675–693. [Google Scholar] [CrossRef]
- Pawlowska, A.; Suszczyk, D.; Okla, K.; Barczyński, B.; Kotarski, J.; Wertel, I. Immunotherapies based on PD-1/PD-L1 pathway inhibitors in ovarian cancer treatment. Clin. Exp. Immunol. 2019, 195, 334–344. [Google Scholar] [CrossRef]
- Holloway, R.W.; Gupta, S.; Stavitzski, N.M.; Zhu, X.; Takimoto, E.L.; Gubbi, A.; Bigsby, G.E.; Brudie, L.A.; Kendrick, J.E.; Ahmad, S. Sentinel Lymph Node Mapping with Staging Lymphadenectomy for Patients with Endometrial Cancer Increases the Detection of Metastasis. Gynecol. Oncol. 2016, 141, 206–210. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1-Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. [Google Scholar] [CrossRef]
- Weber, J.; Mandala, M.; Del Vecchio, M.; Gogas, H.J.; Arance, A.M.; Cowey, C.L.; Dalle, S.M.; Schenker, M.; Chiarion-Sileni, V.; Marquez-Rodas, I.; et al. Adjuvant Nivolumab versus ipilimumab in Resected Stage III or IV Melanoma. N. Engl. J. Med. 2017, 377, 1824–1835. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.-A.; Shaw Wright, G. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef] [PubMed]
- André, T.; Shiu, K.K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia- Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability-High Advanced Colorectal Cancer. N. Engl. J. Med. 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Hamanishi, J.; Mandai, M.; Ikeda, T.; Minami, M.; Kawaguchi, A.; Murayama, T.; Kanai, M.; Mori, Y.; Matsumoto, S.; Chikuma, S.; et al. Safety and antitumor activity of anti-PD-1 antibody, nivolumab, in patients with platinum-resistant ovarian cancer. J. Clin. Oncol. 2015, 33, 4015–4022. [Google Scholar] [CrossRef]
- Zhu, X.; Lang, J. Programmed death-1 pathway blockade produces a synergistic antitumor effect: Combined application in ovarian cancer. J. Gynecol. Oncol. 2017, 28, e64. [Google Scholar] [CrossRef]
- Pietzner, K.; Nasser, S.; Alavi, S.; Darb-Esfahani, S.; Passler, M.; Muallem, M.Z.; Sehouli, J. Checkpoint-inhibition in ovarian cancer: Rising star or just a dream? J. Gynecol. Oncol. 2018, 29, e93. [Google Scholar] [CrossRef]
- Gatalica, Z.; Vranic, S.; Xiu, J.; Swensen, J.; Reddy, S. High microsatellite instability (MSI-H) colorectal carcinoma: A brief review of predictive biomarkers in the era of personalized medicine. Fam. Cancer 2016, 15, 405–412. [Google Scholar] [CrossRef]
- Marabelle, A.; Le, D.T.; Ascierto, P.A.; Di Giacomo, A.M.; De Jesus-Acosta, A.; Delord, J.P.; Geva, R.; Gottfried, M.; Penel, N.; Hansen, A.R.; et al. Efficacy of pembrolizumab in patients with noncolorectal high microsatellite instability/mismatch re-pair-deficient cancer: Results from the Phase II KEYNOTE-158 study. J. Clin. Oncol. 2020, 38, 1–10. [Google Scholar] [CrossRef]
- Sehgal, R.; Sheahan, K.; O’Connell, P.R.; Hanly, A.M.; Martin, S.T.; Winter, D.C. Lynch syndrome: An updated review. Genes 2014, 5, 497–507. [Google Scholar] [CrossRef]
- Richman, S. Deficient mismatch repair: Read all about it (Review). Int. J. Oncol. 2015, 47, 1189–1202. [Google Scholar] [CrossRef]
- Blank, C.; Mackensen, A. Contribution of the PD-L1/PD-1 pathway to T-cell exhaustion: An update on implications for chronic infections and tumor evasion. Cancer Immunol. Immunother. 2007, 56, 739–745. [Google Scholar] [CrossRef] [PubMed]
- Popat, S.; Hubner, R.; Houlston, R.S. Systematic review of microsatellite instability and colorectal cancer prognosis. J. Clin. Oncol. 2005, 23, 609–618. [Google Scholar] [CrossRef]
- Colle, R.; Cohen, R.; Cochereau, D.; Duval, A.; Lascols, O.; Lopez-Trabada, D.; Afchain, P.; Trouilloud, I.; Parc, Y.; Lefevre, J.H.; et al. Immunotherapy and patients treated for cancer with microsatellite instability. Bull. Cancer. 2017, 104, 42–51. [Google Scholar] [CrossRef]
- Chang, L.; Chang, M.; Chang, H.M.; Chang, F. Microsatellite Instability: A Predictive Biomarker for Cancer Immunotherapy. Appl. Immunohistochem. Mol. Morphol. 2018, 26, e15–e21. [Google Scholar] [CrossRef]
- Skilling, J.S.; Sood, A.; Niemann, T.; Lager, D.J.; Buller, R.E. An abundance of p53 null mutations in ovarian carcinoma. Oncogene 1996, 13, 117–123. [Google Scholar] [PubMed]
- Chiesa-Vottero, A.G.; Malpica, A.; Deavers, M.T.; Broaddus, R.; Nuovo, G.J.; Silva, E.G. Immunohistochemical overexpression of p16 and p53 in uterine serous carcinoma and ovarian high-grade serous carcinoma. Int. J. Gynecol. Pathol. 2007, 26, 328–333. [Google Scholar] [CrossRef]
- Ahmed, A.A.; Etemadmoghadam, D.; Temple, J.; Lynch, A.G.; Riad, M.; Sharma, R.; Stewart, C.; Fereday, S.; Caldas, C.; Defazio, A.; et al. Driver mutations in TP53 are ubiquitous in high-grade serous carcinoma of the ovary. J. Pathol. 2010, 221, 49–56. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef] [PubMed]
- American Joint Committee on Cancer AJCC. 2021. Available online: www.uicc.org (accessed on 27 November 2021).
- Drakes, M.L.; Mehrotra, S.; Aldulescu, M.; Potkul, R.K.; Liu, Y.; Grisoli, A.; Joyce, C.; O’Brien, T.E.; Stack, M.S.; Stiff, P.J. Stratification of ovarian tumor pathology by expression of programmed cell death-1 (PD-1) and PD-ligand-1 (PD-L1) in ovarian cancer. J. Ovarian Res. 2018, 11, 43. [Google Scholar] [CrossRef]
- Cortez, A.J.; Tudrej, P.; Kujawa, K.A.; Lisowska, K.M. Advances in ovarian cancer therapy. Cancer Chemother. Pharmacol. 2018, 81, 17–38. [Google Scholar] [CrossRef]
- Reles, A.; Wen, W.H.; Schmider, A.; Gee, C.; Runnebaum, I.B.; Kilian, U.; Jones, L.A.; El-Naggar, A.; Minguillon, C.; Schönborn, I.; et al. Correlation of p53 mutations with resistance to platinum-based chemotherapy and shortened survival in ovarian cancer. Clin. Cancer Res. 2001, 7, 2984–2997. [Google Scholar]
- Geisler, J.P.; Geisler, H.E.; Wiemann, M.C.; Givens, S.S.; Zhou, Z.; Miller, G.A. Quantification of p53 in epithelial ovarian cancer. Gynecol. Oncol. 1997, 66, 435–438. [Google Scholar] [CrossRef] [PubMed]
- Rambau, P.F.; Duggan, M.A.; Ghatage, P.; Warfa, K.; Steed, H.; Perrier, R.; Kelemen, L.E.; Köbel, M. Significant frequency of MSH2/MSH6 abnormality in ovarian endometrioid carcinoma supports histotype-specific Lynch syndrome screening in ovarian carcinomas. Histopathology 2016, 69, 288–297. [Google Scholar] [CrossRef] [PubMed]
- Aysal, A.; Karnezis, A.; Medhi, I.; Grenert, J.P.; Zaloudek, C.J.; Rabban, J.T. Ovarian endometrioid adenocarcinoma: Incidence and clinical significance of the morphologic and immunohistochemical markers of mismatch repair protein defects and tumor microsatellite instability. Am. J. Surg. Pathol. 2012, 36, 163–172. [Google Scholar] [CrossRef]
- Jensen, K.C.; Mariappan, M.R.; Putcha, G.V.; Husain, A.; Chun, N.; Ford, J.M.; Schrijver, I.; Longacre, T.A. Microsatellite instability and mismatch repair protein defects in ovarian epithelial neoplasms in patients 50 years of age and younger. Am. J. Surg. Pathol. 2008, 32, 1029–1037. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, H.; Nakayama, K.; Ishikawa, M.; Ishibashi, T.; Nakamura, K.; Sawada, K.; Yoshimura, Y.; Tatsumi, N.; Kurose, S.; Minamoto, T.; et al. Relationship between microsatellite instability, immune cells infiltration, and expression of immune checkpoint Molecules in ovarian carcinoma: Immunotherapeutic strategies for the future. Int. J. Mol. Sci. 2019, 20, 5129. [Google Scholar] [CrossRef] [PubMed]
- Mandai, M.; Hamanishi, J.; Abiko, K.; Matsumura, N.; Baba, T.; Konishi, I. Anti-PD-L1/PD-1 immune therapies in ovarian cancer: Basic mechanism and future clinical application. Int. J. Clin. Oncol. 2016, 21, 456–461. [Google Scholar] [CrossRef]
- Patel, S.J.; Sanjana, N.E.; Kishton, R.J.; Eidizadeh, A.; Vodnala, S.K.; Cam, M.; Gartner, J.J.; Jia, L.; Steinberg, S.M.; Yamamoto, T.N.; et al. Identification of essential genes for cancer immunotherapy. Nature 2017, 548, 537–542. [Google Scholar] [CrossRef]
- Zhang, L.; Conejo-Garcia, J.R.; Katsaros, D.; Gimotty, P.A.; Massobrio, M.; Regnani, G.; Makrigiannakis, A.; Gray, H.; Schlienger, K.; Liebman, M.N.; et al. Intratumoral T cells, recurrence, and Survivalin Epithelial Ovarian Cancer. N. Engl. J. Med. 2003, 348, 203–213. [Google Scholar] [CrossRef]
- Hwang, W.T.; Adams, S.F.; Tahirovic, E.; Hagemann, I.S.; Coukos, G. Prognostic significance of tumor-infiltrating T cells in ovarian cancer: A meta-analysis. Gynecol. Oncol. 2012, 124, 192–198. [Google Scholar] [CrossRef]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.; Rustin, G.; Scott, C.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer. N. Engl. J. Med. 2012, 366, 1382–1392. [Google Scholar] [CrossRef] [PubMed]


| Variable | n 1 | Average ± SD | Median (Min–Max) | IQR |
|---|---|---|---|---|
| Age at diagnosis (years) | 28 | 61.3 ± 14.0 | 60.0 (34.0–90.0) | 18.0 |
| BMI | 26 | 25.9 ± 5.8 | 25.2 (18.6–41.3) | 6.3 |
| Variable | n 1 | % | |
|---|---|---|---|
| Diagnosis 2 | high grade | 21 | 75.0 |
| low grade | 7 | 25.0 | |
| Size of the tumor | T3 | 24 | 96.0 |
| Compromise of lymph nodes | no | 11 | 42.3 |
| yes | 15 | 57.7 | |
| Metastasis | no | 18 | 69.2 |
| yes | 8 | 30.8 | |
| Clinical stage | III | 19 | 70.4 |
| IV | 8 | 29.6 | |
| History of cancer | no | 13 | 65.0 |
| yes | 7 | 35.0 | |
| BRCA1 mutation | no | 11 | 61.1 |
| yes | 7 | 38.9 | |
| BRCA2 mutation | no | 12 | 66.7 |
| yes | 6 | 33.3 | |
| BRCA mutation type | germline | 7 | 70.0 |
| tumor | 3 | 30.0 | |
| Comorbidity | no | 10 | 38.5 |
| yes | 16 | 61.5 | |
| Platinum sensitivity | no | 2 | 8.0 |
| yes | 23 | 92.0 | |
| Relapse | no | 13 | 46.4 |
| yes | 15 | 53.6 | |
| Outcome | dead | 6 | 21.4 |
| alive | 18 | 64.3 | |
| segment loss | 4 | 14.3 | |
| Marker | n 1 | Result |
|---|---|---|
| PD-1 | 28 | 18.8 ± 17.2 |
| CD8 | 28 | 346.6 ± 469.2 |
| PD-L1 | 26 | 15.2 ± 18.1 |
| MLH1 | 5 | Negative |
| 23 | Positive | |
| MSH2 | 2 | Negative |
| 26 | Positive | |
| MSH6 | 1 | Negative |
| 27 | Positive | |
| PMS2 | 3 | Negative |
| 25 | Positive | |
| p53 | 6 | wild type |
| 22 | overexpressed | |
| status MSI | 23 | stable |
| 4 | unstable |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dergham, A.P.; Vaz de Paula, C.B.; Nagashima, S.; Olandoski, M.; de Noronha, L.; Sotomaior, V.S. Immunohistochemical Profiling of PD-1, PD-L1, CD8, MSI, and p53 and Prognostic Implications in Advanced Serous Ovarian Carcinoma: A Retrospective Study. J. Pers. Med. 2023, 13, 1045. https://doi.org/10.3390/jpm13071045
Dergham AP, Vaz de Paula CB, Nagashima S, Olandoski M, de Noronha L, Sotomaior VS. Immunohistochemical Profiling of PD-1, PD-L1, CD8, MSI, and p53 and Prognostic Implications in Advanced Serous Ovarian Carcinoma: A Retrospective Study. Journal of Personalized Medicine. 2023; 13(7):1045. https://doi.org/10.3390/jpm13071045
Chicago/Turabian StyleDergham, Ana Paula, Caroline Busatta Vaz de Paula, Seigo Nagashima, Márcia Olandoski, Lucia de Noronha, and Vanessa Santos Sotomaior. 2023. "Immunohistochemical Profiling of PD-1, PD-L1, CD8, MSI, and p53 and Prognostic Implications in Advanced Serous Ovarian Carcinoma: A Retrospective Study" Journal of Personalized Medicine 13, no. 7: 1045. https://doi.org/10.3390/jpm13071045
APA StyleDergham, A. P., Vaz de Paula, C. B., Nagashima, S., Olandoski, M., de Noronha, L., & Sotomaior, V. S. (2023). Immunohistochemical Profiling of PD-1, PD-L1, CD8, MSI, and p53 and Prognostic Implications in Advanced Serous Ovarian Carcinoma: A Retrospective Study. Journal of Personalized Medicine, 13(7), 1045. https://doi.org/10.3390/jpm13071045