
Impact of Race and Ethnicity on Presentation and Surgical Outcomes of Idiopathic Macular Holes

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Cohort Data
3.2. Preoperative Status
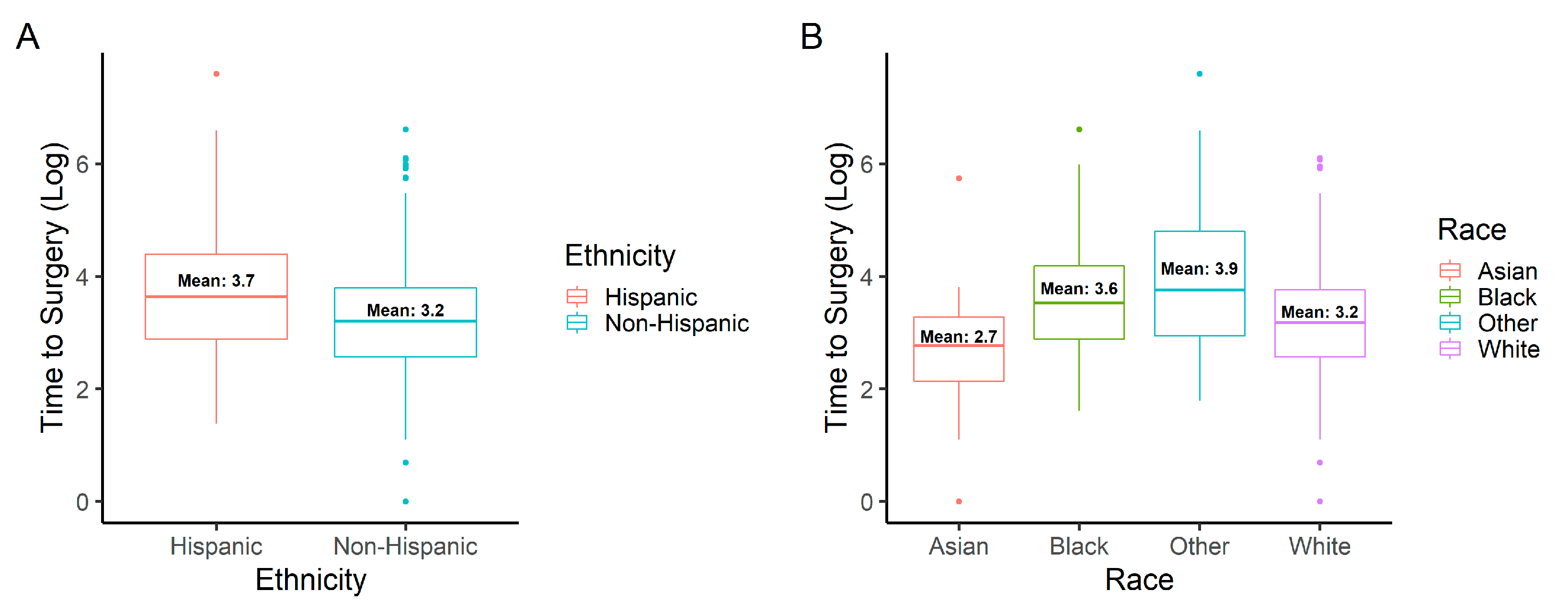
3.2.1. Time to Surgery
3.2.2. Preoperative Vision
3.3. Postoperative Status
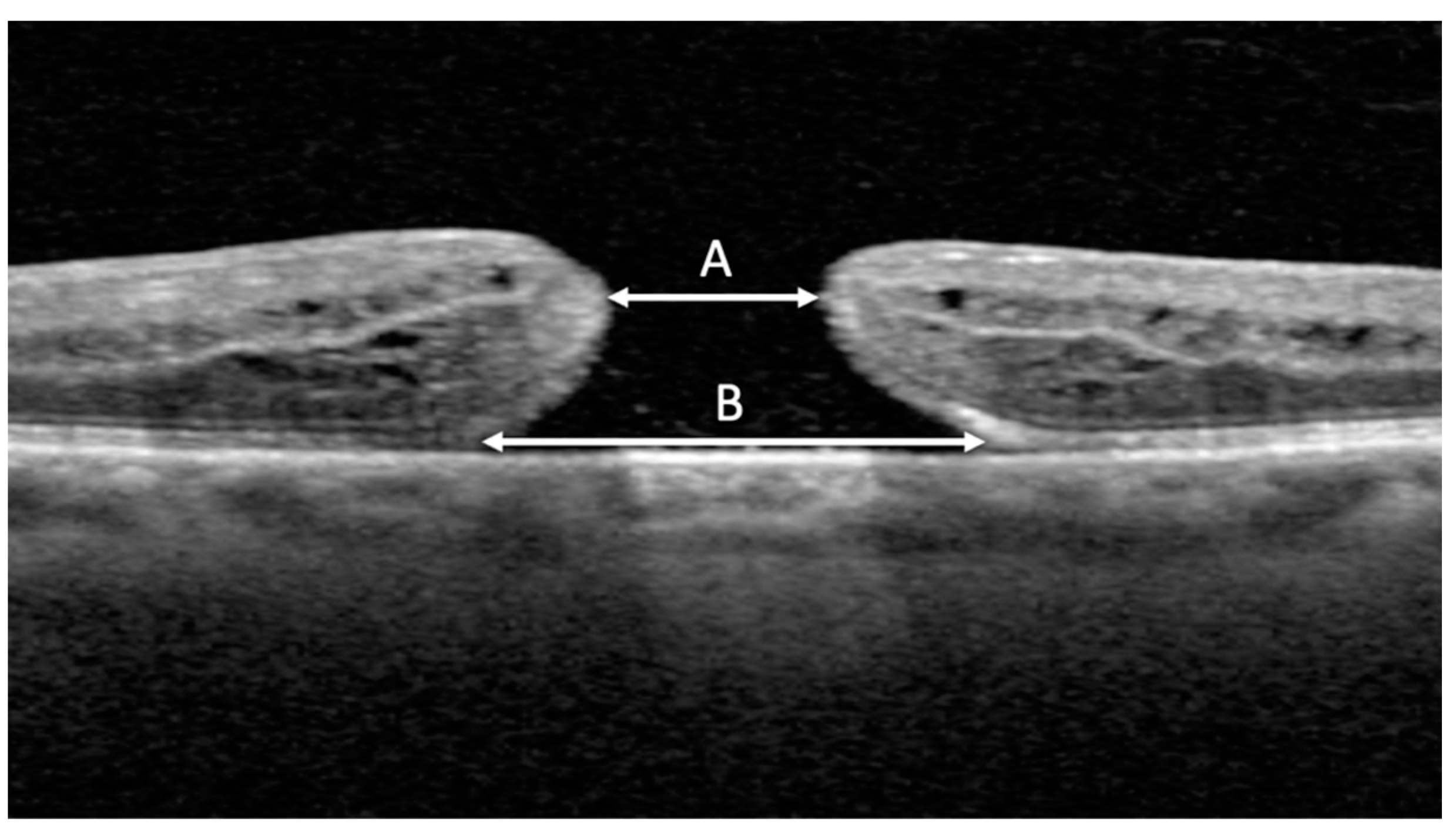
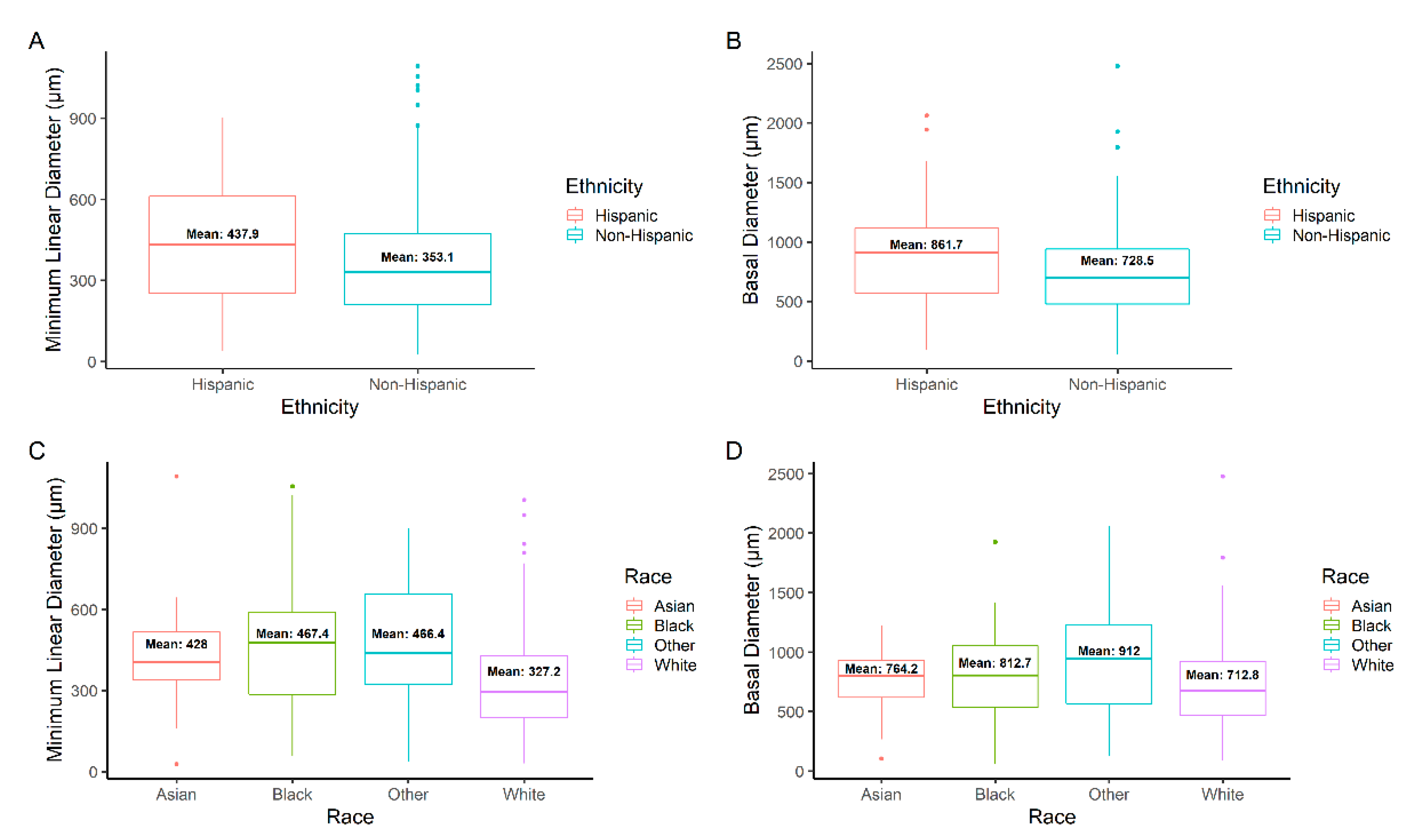
3.3.1. IMH Measurements
3.3.2. Surgical Outcomes
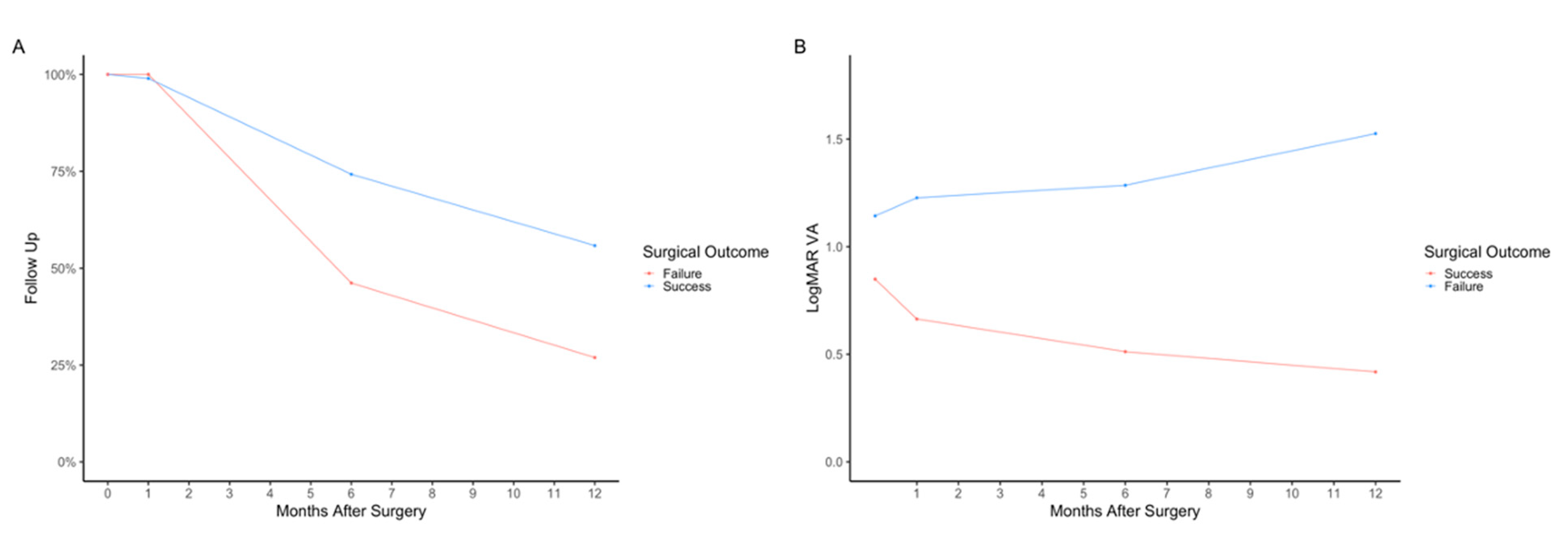
3.3.3. Follow-Up Data
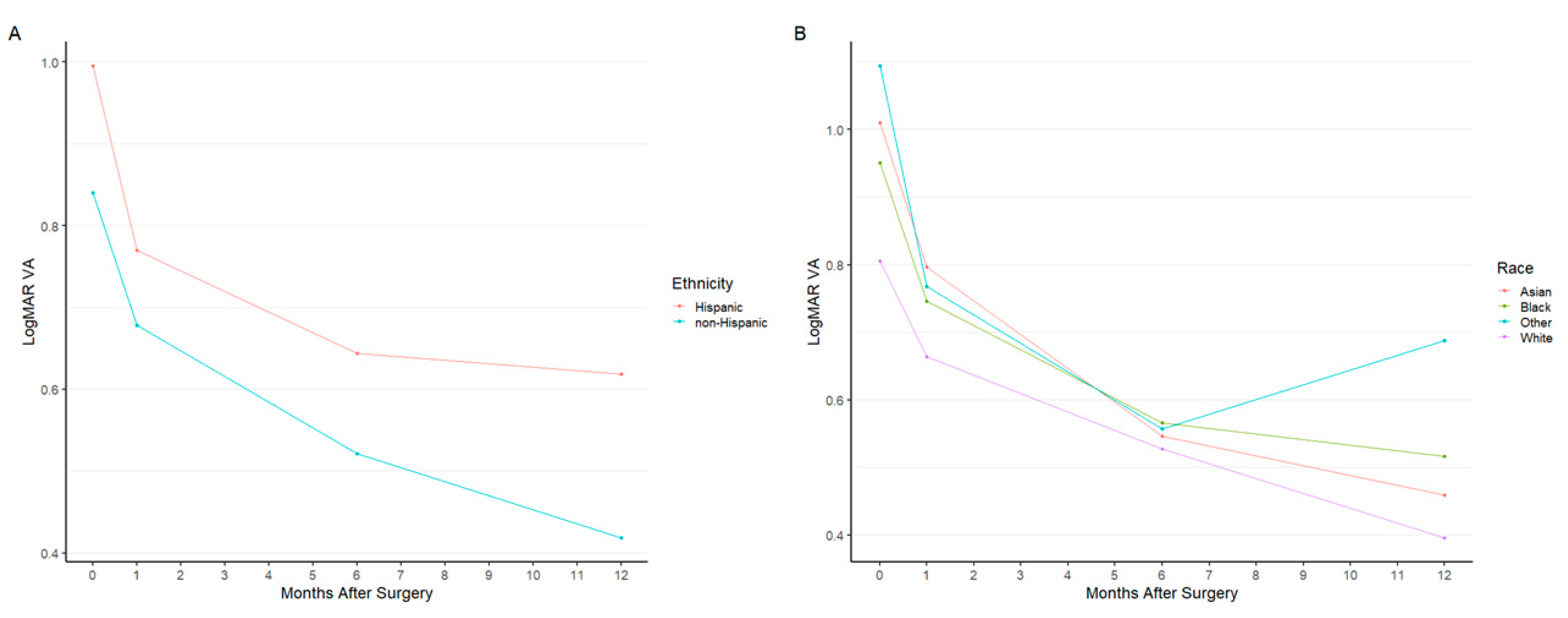
3.3.4. Visual Outcomes
4. Discussion
4.1. Association between Variance in MLD and BD, Time to Surgery, and Surgical Outcomes
4.2. Effect of Language
4.3. Diabetes in the Hispanic Population and FTMH
4.4. Visual Acuity Analysis
4.5. Age and Sex
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Majumdar, S.; Tripathy, K. Macular Hole. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: http://www.ncbi.nlm.nih.gov/books/NBK559200/ (accessed on 25 June 2022).
- Stec, L.A.; Ross, R.D.; Williams, G.A.; Trese, M.T.; Margherio, R.R.; Cox, M.S. Vitrectomy for chronic macular holes. Retina 2004, 24, 341–347. [Google Scholar] [CrossRef]
- Willis, A.W.; Garcia-Cosio, J.F. Macular hole surgery. Comparison of longstanding versus recent macular holes. Ophthalmology 1996, 103, 1811–1814. [Google Scholar] [CrossRef]
- Chandra, A.; Lai, M.; Mitry, D.; Banerjee, P.J.; Flayeh, H.; Negretti, G.; Kumar, N.; Wickham, L. Ethnic variation in primary idiopathic macular hole surgery. Eye 2017, 31, 708–712. [Google Scholar] [CrossRef]
- Velissaris, S.; Papavasileiou, E.; Garnavou-Xirou, C.; Theodorou, O.; Zakir, R.; Duguid, G.; Sandinha, T.; Steel, D.; Jackson, T. Characteristics, socioeconomic status and ethnic variations of primary idiopathic macular hole repair in vitreoretinal centers in the United Kingdom. Acta Ophthalmol. 2017, 95. [Google Scholar] [CrossRef]
- Valentim, C.C.S.; Iyer, A.I.; Xu, C.; Muste, J.C.; Li, A.; Singh, R.P. Influence of Race, Ethnicity, and Socioeconomic Factors in Idiopathic Macular Hole Presentation and Surgical Outcomes. Ophthalmic Surg. Lasers Imaging Retin. 2022, 53, 333–344. [Google Scholar] [CrossRef]
- Bureau, U.C. 2020 Census Illuminates Racial and Ethnic Composition of the Country. Census.gov. Available online: https://www.census.gov/library/stories/2021/08/improved-race-ethnicity-measures-reveal-united-states-population-much-more-multiracial.html (accessed on 6 August 2022).
- Mozdbar, S.T.; Deakins, J.; Terrell, J.; Johnson, L.A.; Clark, A.F. Community-Based Eye Health Screening Study in the Elderly Hispanic Population in North Texas. Tex. Public Health J. 2020, 72, 19–21. [Google Scholar]
- Varma, R.; Mohanty, S.A.; Deneen, J.; Wu, J.; Azen, S.P. Burden and Predictors of Undetected Eye Disease in Mexican-Americans. Med. Care 2008, 46, 497–506. [Google Scholar] [CrossRef]
- Ford, M.E.; Kelly, P.A. Conceptualizing and Categorizing Race and Ethnicity in Health Services Research. Health Serv Res. 2005, 40 Pt 2, 1658–1675. [Google Scholar] [CrossRef]
- Flanagin, A.; Frey, T.; Christiansen, S.L. AMA Manual of Style Committee Updated Guidance on the Reporting of Race and Ethnicity in Medical and Science Journals. JAMA 2021, 326, 621–627. [Google Scholar] [CrossRef]
- Steel, D.H.; A Madi, H.; Masri, I. Optimal management of idiopathic macular holes. Clin. Ophthalmol. 2016, 10, 97–116. [Google Scholar] [CrossRef]
- Duker, J.S.; Kaiser, P.K.; Binder, S.; de Smet, M.D.; Gaudric, A.; Reichel, E.; Sadda, S.R.; Sebag, J.; Spaide, R.F.; Stalmans, P. The International Vitreomacular Traction Study Group Classification of Vitreomacular Adhesion, Traction, and Macular Hole. Ophthalmology 2013, 120, 2611–2619. [Google Scholar] [CrossRef] [PubMed]
- Berton, M.; Robins, J.; Frigo, A.C.; Wong, R. Rate of progression of idiopathic full-thickness macular holes before surgery. Eye 2019, 34, 1386–1391. [Google Scholar] [CrossRef]
- Nelson, A. Unequal treatment: Confronting racial and ethnic disparities in health care. J. Natl. Med. Assoc. 2002, 94, 666–668. [Google Scholar]
- Zhang, X.; Cotch, M.F.; Ryskulova, A.; Primo, S.A.; Nair, P.; Chou, C.-F.; Geiss, L.S.; Barker, L.E.; Elliott, A.F.; Crews, J.E.; et al. Vision Health Disparities in the United States by Race/Ethnicity, Education, and Economic Status: Findings From Two Nationally Representative Surveys. Am. J. Ophthalmol. 2012, 154 (Suppl 6), S53–S62.e1. [Google Scholar] [CrossRef]
- Aguwa, U.T.; Srikumaran, D.; Brown, N.; Woreta, F. Improving Racial Diversity in the Ophthalmology Workforce: A Call to Action for Leaders in Ophthalmology. Am. J. Ophthalmol. 2020, 223, 306–307. [Google Scholar] [CrossRef]
- Rasendran, C.; Tye, G.; Knusel, K.; Singh, R.P. Demographic and Socioeconomic Differences in Outpatient Ophthalmology Utilization in the United States. Am. J. Ophthalmol. 2020, 218, 156–163. [Google Scholar] [CrossRef]
- Riley, W.J. Health disparities: Gaps in access, quality and affordability of medical care. Trans. Am. Clin. Clim. Assoc. 2012, 123, 167–174. [Google Scholar]
- Ruiz-Moreno, J.M.; Staicu, C.; Pinero, D.P.; Montero, J.; Lugo, F.; Amat, P. Optical coherence tomography predictive factors for macular hole surgery outcome. Br. J. Ophthalmol. 2008, 92, 640–644. [Google Scholar] [CrossRef]
- Ip, M.S.; Baker, B.J.; Duker, J.S.; Reichel, E.; Baumal, C.R.; Gangnon, R.; Puliafito, C.A. Anatomical Outcomes of Surgery for Idiopathic Macular Hole as Determined by Optical Coherence Tomography. Arch. Ophthalmol. 2002, 120, 29–35. [Google Scholar] [CrossRef]
- Liang, X.; Wang, Y.; Liu, L.; Gao, M.; Yu, Y.; Wang, Z.; Chen, J.; Liu, X.; Liu, W. Relationship Between Metamorphopsia and Macular Parameters Before and After Idiopathic Macular Hole Surgery. Ophthalmic Surg. Lasers Imaging Retin. 2018, 49, 595–602. [Google Scholar] [CrossRef]
- Al Shamsi, H.; Almutairi, A.G.; Al Mashrafi, S.; Al Kalbani, T. Implications of Language Barriers for Healthcare: A Systematic Review. Oman Med. J. 2020, 35, e122. [Google Scholar] [CrossRef] [PubMed]
- Meuter, R.F.I.; Gallois, C.; Segalowitz, N.S.; Ryder, A.G.; Hocking, J. Overcoming language barriers in healthcare: A protocol for investigating safe and effective communication when patients or clinicians use a second language. BMC Health Serv. Res. 2015, 15, 371. [Google Scholar] [CrossRef]
- Steinberg, E.M.; Valenzuela-Araujo, D.; Zickafoose, J.S.; Kieffer, E.; DeCamp, L.R. The “Battle” of Managing Language Barriers in Health Care. Clin. Pediatrics 2016, 55, 1318–1327. [Google Scholar] [CrossRef] [PubMed]
- Aguayo-Mazzucato, C.; Diaque, P.; Hernandez, S.; Rosas, S.; Kostic, A.; Caballero, A.E. Understanding the growing epidemic of type 2 diabetes in the Hispanic population living in the United States. Diabetes/Metab. Res. Rev. 2018, 35, e3097. [Google Scholar] [CrossRef] [PubMed]
- Haw, J.S.; Shah, M.; Turbow, S.; Egeolu, M.; Umpierrez, G. Diabetes Complications in Racial and Ethnic Minority Populations in the USA. Curr. Diabetes Rep. 2021, 21, 1–8. [Google Scholar] [CrossRef]
- Mazhar, K.; Varma, R.; Choudhury, F.; McKean-Cowdin, R.; Shtir, C.J.; Azen, S.P. Severity of Diabetic Retinopathy and Health-Related Quality of Life: The Los Angeles Latino Eye Study. Ophthalmology 2011, 118, 649–655. [Google Scholar] [CrossRef]
- Cartwright, K. Social determinants of the Latinx diabetes health disparity: A Oaxaca-Blinder decomposition analysis. SSM-Popul. Health 2021, 15, 100869. [Google Scholar] [CrossRef]
- Lai, C.-T.; Yang, C.-M. Development of macular holes in diabetic retinopathy with fibrovascular proliferation: Report of four cases. Taiwan J. Ophthalmol. 2015, 5, 85–89. [Google Scholar] [CrossRef]
- Cubuk, M.O.; Unsal, E.; Ciftci, F. Preoperative prognostic factors for macular hole surgery: Which is better? Oman J. Ophthalmol. 2019, 12, 20–24. [Google Scholar] [CrossRef]
- Feng, H.; Adelman, R. Cataract formation following vitreoretinal procedures. Clin. Ophthalmol. 2014, 8, 1957–1965. [Google Scholar] [CrossRef]
- Cheng, L.; Azen, S.P.; El-Bradey, M.H.; Scholz, B.M.; Chaidhawangul, S.; Toyoguchi, M.; Freeman, W.R. Duration of vitrectomy and postoperative cataract in the vitrectomy for macular hole study. Am. J. Ophthalmol. 2001, 132, 881–887. [Google Scholar] [CrossRef]
- McCannel, C.A.; Ensminger, J.L.; Diehl, N.N.; Hodge, D.N. Population-based Incidence of Macular Holes. Ophthalmology 2009, 116, 1366–1369. [Google Scholar] [CrossRef]
- Ali, F.S.; Stein, J.D.; Blachley, T.S.; Ackley, S.; Stewart, J.M. Incidence of and Risk Factors for Developing Idiopathic Macular Hole Among a Diverse Group of Patients Throughout the United States. JAMA Ophthalmol. 2017, 135, 299–305. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data | |
|---|---|
| Number of Participants | 488 |
| Number of Eyes | 515 |
| OD: n (%) | 252 (48.9) |
| OS: n (%) | 263 (51.1) |
| Male: n (%) | 145 (28.2) |
| Female: n (%) | 370 (71.8) |
| Age: mean (SD) | 66.3 (7.5) |
| Pseudophakic: n (%) | 164 (31.8) |
| FE FTMH: n (%) | 55 (10.7) |
| FE LMH: n (%) | 23 (5.5) |
| Population by Ethnicity | n (%) |
| Hispanic | 79 (15.3) |
| Non-Hispanic | 436 (84.7) |
| Population by Race | n (%) |
| Asian | 23 (4.5) |
| Black | 79 (15.3) |
| White | 365 (70.9) |
| Other | 48 (9.3) |
| Ethnicity | Mean Age (SD) |
| Hispanic | 64.0 (9.5) |
| Non-Hispanic | 66.7 (7.0) |
| p-Value | 0.016 * |
| Race | Mean Age (SD) |
| Asian | 61.8 (7.5) |
| Black | 63.7 (7.3) |
| White | 63.0 (6.6) |
| Other | 67.6 (10.4) |
| p-Value | <0.001 * |
| Language | n (%) |
| English | 475 (92.2) |
| Spanish | 33 (6.4) |
| Other | 7 (1.4) |
| Diabetes | n (%) |
| Type I | 2 (0.4) |
| Type II | 78 (15.1) |
| Covariate | Mean Time to Surgery (SD), days | p-Value | |||
|---|---|---|---|---|---|
| Ethnicity | Hispanic | Non-Hispanic | |||
| 99.7 (245.8) | 43.2 (68.4) | 0.046 * | |||
| Race | Asian | Black | White | Other | |
| 30.6 (62.5) | 64.2 (101.8) | 39.5 (56.2) | 135.9 (309.5) | <0.001 * | |
| Preferred Language | English | Non-English | |||
| 50.0 (115.2) | 73.9 (129.0) | 0.263 | |||
| Spanish | Non-Spanish | ||||
| 92.9 (139.2) | 50.7 (114.5) | 0.127 | |||
| Diabetes | Diabetic | Non-Diabetic | |||
| 48.3 (94.6) | 52.5 (120.1) | 0.723 | |||
| Covariate | Mean Preoperative LogMAR Visual Acuity (SD) | p-Value | |||
|---|---|---|---|---|---|
| Ethnicity | Hispanic | Non-Hispanic | |||
| 1.00 (0.48) | 0.84 (0.40) | 0.008 * | |||
| Race | Asian | Black | White | Other | |
| 1.01 (0.45) | 0.95 (0.43) | 0.81 (0.38) | 1.10 (0.51) | <0.001 * | |
| IMH Status ** | Closed | Open | |||
| 0.85 (0.41) | 1.14 (0.45) | 0.003 * | |||
| Covariate | Mean Measurement (SD), μm | p-Value | |||
|---|---|---|---|---|---|
| Sex | Female | Male | |||
| (n = 370) | (n = 145) | ||||
| MLD | 389.3 (200.5) | 307.0 (175.7) | <0.001 * | ||
| BD | 756.9 (349.2) | 728.8 (358.3) | 0.420 | ||
| Ethnicity | Hispanic (n = 79) | Non-Hispanic (n = 436) | |||
| MLD | 437.9 (219.0) | 353.2 (190.1) | 0.002 * | ||
| BD | 861.7 (417.2) | 728.5 (334.9) | 0.009 * | ||
| Race | Asian (n = 23) | Black (n = 79) | White (n = 365) | Other (n = 365) | |
| MLD | 428.0 (208.9) | 467.4 (220.1) | 327.2 (172.9) | 466.4 (227.3) | <0.001 * |
| BD | 764.2 (300.1) | 812.7 (352.2) | 712.8 (331.7) | 912.0 (456.1) | <0.001 * |
| Preferred Language | English (n = 451) | Non-English (n = 37) | |||
| MLD | 357.5 (190.6) | 469.0 (242.9) | 0.007 * | ||
| BD | 742.1 (344.8) | 830.5 (421.4) | 0.204 | ||
| Spanish (n = 30) | Non-Spanish (n = 458) | ||||
| MLD | 482.0 (224.5) | 357.6 (193.1) | 0.007 * | ||
| BD | 873.2 (428.7) | 742.2 (344.9) | 0.121 | ||
| Diabetes | Diabetic (n = 78) | Non-Diabetic (n = 435) | |||
| MLD, Overall | 359.3 (177.2) | 367.4 (200.8) | 0.713 | ||
| MLD, Non-Hispanic | 326.4 (169.2) | 357.9 (193.5) | 0.176 | ||
| MLD, Hispanic | 514.2 (128.2) | 421.5 (232.6) | 0.046 * | ||
| BD, Overall | 747.4 (385.9) | 749.3 (345.5) | 0.968 | ||
| BD, Non-Hispanic | 684.5 (376.9) | 736.4 (326.8) | 0.296 | ||
| BD, Hispanic | 1044.1 (282.4) | 822.4 (432.6) | 0.024 * | ||
| Size of IMH | Number of Study Eyes | |
|---|---|---|
| Ethnicity | Hispanic (n = 79) | Non-Hispanic (n = 436) |
| MLD | ||
| Small | 20 | 147 |
| Medium | 14 | 134 |
| Large | 45 | 155 |
| p-value | <0.001 * | 0.462 |
| BD | ||
| Small | 21 | 153 |
| Medium | 17 | 152 |
| Large | 41 | 131 |
| p-value | 0.002 * | 0.346 |
| Size of IMH | Number of Study Eyes | |||
|---|---|---|---|---|
| Race | Asian (n = 23) | Black (n = 79) | White (n = 365) | Other (n = 48) |
| MLD | ||||
| Small | 4 | 13 | 140 | 10 |
| Medium | 7 | 20 | 113 | 8 |
| Large | 12 | 46 | 112 | 30 |
| p-value | 0.119 | <0.001 * | 0.126 | <0.001 * |
| BD | ||||
| Small | 6 | 23 | 132 | 13 |
| Medium | 8 | 22 | 131 | 8 |
| Large | 9 | 34 | 102 | 27 |
| p-value | 0.738 | 0.186 | 0.092 | 0.002 * |
| Covariant | Macular Hole Closure | p-Value | |
|---|---|---|---|
| Ethnicity | 0.399 | ||
| Race | 0.418 | ||
| Language | |||
| English vs. non-English | 0.718 | ||
| Spanish vs. non-Spanish | 0.470 | ||
| FE FTMH | 0.267 | ||
| MLD Size | <0.001 * | ||
| BD Size | <0.001 * | ||
| Diabetes | 0.759 | ||
| MLD | Open [mean (SD), μm] | Closed [mean (SD), μm] | |
| 607.3 (188.6) | 353.3 (189.4) | <0.001 * | |
| BD | Open [mean (SD), μm] | Closed [mean (SD), μm] | |
| 1119.7 (327.7) | 729.3 (342.1) | <0.001 * | |
| TTS | Open [mean (SD), days] | Closed [mean (SD), days] | |
| 55.7 (83.4) | 51.7 (118.0) | 0.815 | |
| Covariate | Mean Postoperative LogMAR Visual Acuity (SD) | p-Value | |||
|---|---|---|---|---|---|
| Ethnicity | Hispanic | Non-Hispanic | |||
| POM1 | 0.77 (0.51) | 0.68 (0.47) | 0.144 | ||
| POM6 | 0.64 (0.50) | 0.52 (0.42) | 0.115 | ||
| POM12 | 0.62 (0.51) | 0.42 (0.40) | 0.026 * | ||
| Race | Asian | Black | White | Other | |
| POM1 | 0.80 (0.38) | 0.75 (0.48) | 0.66 (0.49) | 0.768 (0.46) | 0.210 |
| POM6 | 0.55 (0.27) | 0.57 (0.42) | 0.53 (0.44) | 0.557 (0.47) | 0.922 |
| POM12 | 0.46 (0.30) | 0.52 (0.45) | 0.40 (0.39) | 0.69 (0.55) | 0.005 * |
| IMH Status ** | Closed | Open | |||
| POM1 | 0.66 (0.46) | 1.23 (0.51) | <0.001 * | ||
| POM6 | 0.51 (0.41) | 1.29 (0.54) | <0.001 * | ||
| POM12 | 0.42 (0.38) | 1.53 (0.41) | <0.001 * | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parvus, M.N.; Louis, A.M.; Trejo Corona, S.; Wong, T.P.; Major, J.C.; Patel, S.B.; Wykoff, C.C. Impact of Race and Ethnicity on Presentation and Surgical Outcomes of Idiopathic Macular Holes. J. Pers. Med. 2022, 12, 1518. https://doi.org/10.3390/jpm12091518
Parvus MN, Louis AM, Trejo Corona S, Wong TP, Major JC, Patel SB, Wykoff CC. Impact of Race and Ethnicity on Presentation and Surgical Outcomes of Idiopathic Macular Holes. Journal of Personalized Medicine. 2022; 12(9):1518. https://doi.org/10.3390/jpm12091518
Chicago/Turabian StyleParvus, Matthew N., Abigail M. Louis, Stephanie Trejo Corona, Tien P. Wong, James C. Major, Sagar B. Patel, and Charles C. Wykoff. 2022. "Impact of Race and Ethnicity on Presentation and Surgical Outcomes of Idiopathic Macular Holes" Journal of Personalized Medicine 12, no. 9: 1518. https://doi.org/10.3390/jpm12091518
APA StyleParvus, M. N., Louis, A. M., Trejo Corona, S., Wong, T. P., Major, J. C., Patel, S. B., & Wykoff, C. C. (2022). Impact of Race and Ethnicity on Presentation and Surgical Outcomes of Idiopathic Macular Holes. Journal of Personalized Medicine, 12(9), 1518. https://doi.org/10.3390/jpm12091518