
Lessons Learned from the Pilot Phase of a Population-Wide Genomic Screening Program: Building the Base to Reach a Diverse Cohort of 100,000 Participants

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Setting and Sample
2.2. Design and Data Collection
2.3. Data Analysis
3. Results
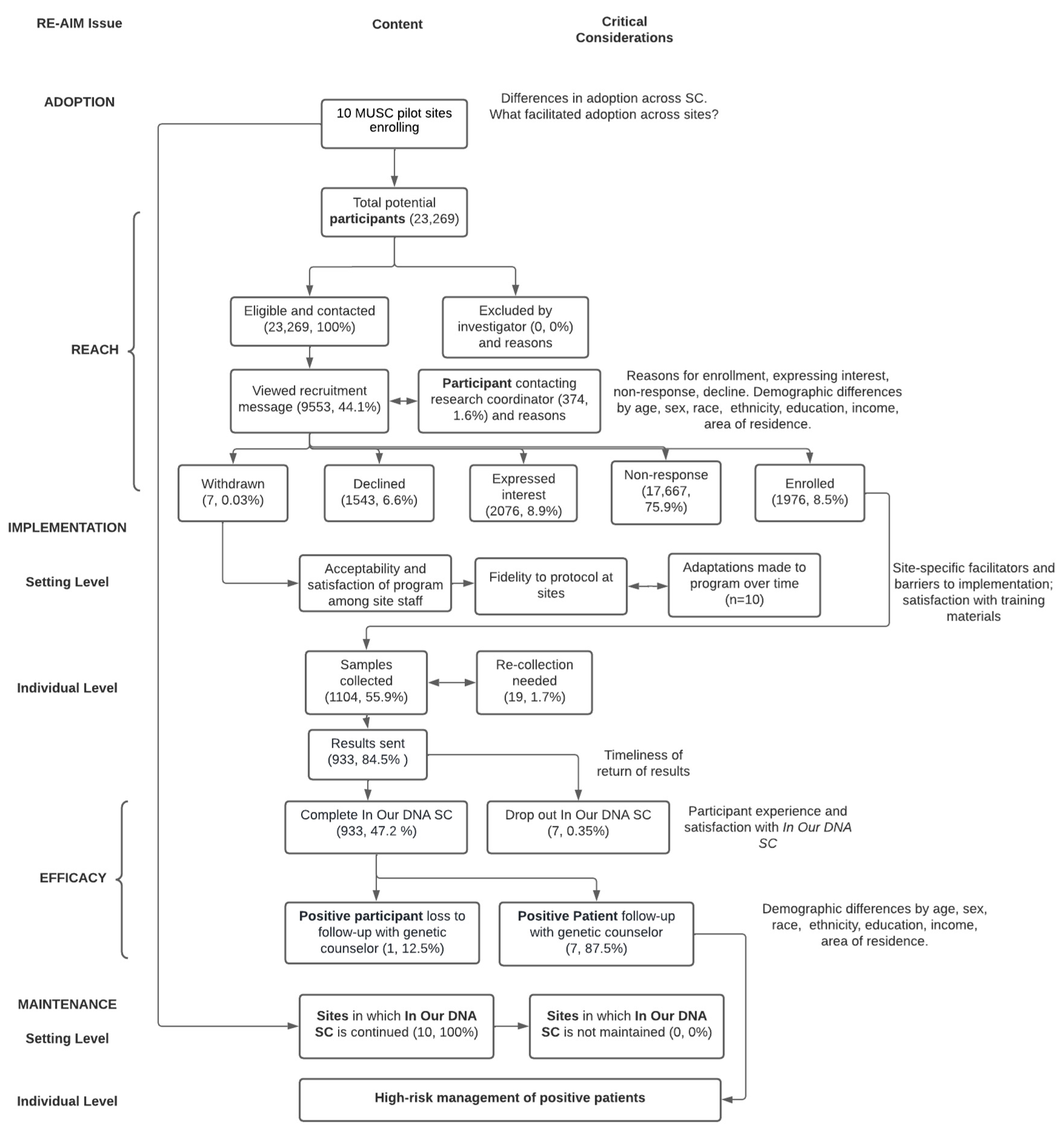
3.1. Assessing Reach of In Our DNA SC
3.2. Implementation of In Our DNA SC
3.3. Effectiveness of In Our DNA SC
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khoury, M.J.; Bowen, M.S.; Clyne, M.; Dotson, W.D.; Gwinn, M.L.; Green, R.F.; Kolor, K.; Rodriguez, J.L.; Wulf, A.; Yu, W. From public health genomics to precision public health: A 20-year journey. Genet. Med. Off. J. Am. Coll. Med. Genet. 2018, 20, 574–582. [Google Scholar] [CrossRef] [Green Version]
- Smith, C.E.; Fullerton, S.M.; Dookeran, K.A.; Hampel, H.; Tin, A.; Maruthur, N.M.; Schisler, J.C.; Henderson, J.A.; Tucker, K.L.; Ordovás, J.M. Using Genetic Technologies To Reduce, Rather Than Widen, Health Disparities. Health Aff. 2016, 35, 1367–1373. [Google Scholar] [CrossRef] [PubMed]
- Buchanan, A.H.; Rahm, A.K.; Williams, J.L. Alternate Service Delivery Models in Cancer Genetic Counseling: A Mini-Review. Front. Oncol. 2016, 6, 120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buchanan, A.H.; Lester Kirchner, H.; Schwartz, M.L.B.; Kelly, M.A.; Schmidlen, T.; Jones, L.K.; Hallquist, M.L.; Rocha, H.; Betts, M.; Schwiter, R.; et al. Clinical outcomes of a genomic screening program for actionable genetic conditions. Genet. Med. Off. J. Am. Coll. Med. Genet. 2020, 22, 1874–1882. [Google Scholar] [CrossRef]
- Murray, M.F.; Evans, J.P.; Angrist, M.; Uhlmann, W.R.; Lochner Doyle, D.; Fullerton, S.M.; Ganiats, T.G.; Hagenkord, J.; Imhof, S.; Rim, S.H.; et al. A Proposed Approach for Implementing Genomics-Based Screening Programs for Healthy Adults. NAM Perspect. 2018. [Google Scholar] [CrossRef]
- Foss, K.S.; O’Daniel, J.M.; Berg, J.S.; Powell, S.N.; Cadigan, R.J.; Kuczynski, K.J.; Milko, L.V.; Saylor, K.W.; Roberts, M.; Weck, K.; et al. The Rise of Population Genomic Screening: Characteristics of Current Programs and the Need for Evidence Regarding Optimal Implementation. J. Pers. Med. 2022, 12, 692. [Google Scholar] [CrossRef]
- Shen, E.C.; Srinivasan, S.; Passero, L.E.; Allen, C.G.; Dixon, M.; Foss, K.; Halliburton, B.; Milko, L.V.; Smit, A.K.; Carlson, R.; et al. Barriers and facilitators for population genetic screening in healthy populations: A systematic review. Front. Genet. 2022, 13, 865384. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.G.; Judge, D.P.; Levin, E.; Sterba, K.; Hunt, K.; Ramos, P.S.; Melvin, C.; Wager, K.; Catchpole, K.; Clinton, C.; et al. A pragmatic implementation research study for in our DNA SC: A protocol to identify multi-level factors that support the implementation of a population-wide genomic screening initiative in diverse populations. Implement. Sci. Commun. 2022, 3, 48. [Google Scholar] [CrossRef] [PubMed]
- Glasgow, R.E.; Estabrooks, P.E. Pragmatic Applications of RE-AIM for Health Care Initiatives in Community and Clinical Settings. Prev. Chronic Dis. 2018, 15, E02. [Google Scholar] [CrossRef] [PubMed]
- Landry, L.G.; Ali, N.; Williams, D.R.; Rehm, H.L.; Bonham, V.L. Lack Of Diversity In Genomic Databases Is A Barrier to Translating Precision Medicine Research Into Practice. Health Aff. 2018, 37, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Popejoy, A.B.; Fullerton, S.M. Genomics is failing on diversity. Nature 2016, 538, 161–164. [Google Scholar] [CrossRef] [Green Version]
- Sirugo, G.; Williams, S.M.; Tishkoff, S.A. The Missing Diversity in Human Genetic Studies. Cell 2019, 177, 26–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manrai, A.K.; Funke, B.H.; Rehm, H.L.; Olesen, M.S.; Maron, B.A.; Szolovits, P.; Margulies, D.M.; Loscalzo, J.; Kohane, I.S. Genetic Misdiagnoses and the Potential for Health Disparities. N. Engl. J. Med. 2016, 375, 655–665. [Google Scholar] [CrossRef] [PubMed]
- Meulenkamp, T.M.; Gevers, S.K.; Bovenberg, J.A.; Koppelman, G.H.; van Hylckama Vlieg, A.; Smets, E.M. Communication of biobanks’ research results: What do (potential) participants want? Am. J. Med. Genet. Part A 2010, 152, 2482–2492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterling, R.; Henderson, G.E.; Corbie-Smith, G. Public willingness to participate in and public opinions about genetic variation research: A review of the literature. Am. J. Public Health 2006, 96, 1971–1978. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, D.J.; Murphy-Bollinger, J.; Scott, J.; Hudson, K.L. Public opinion about the importance of privacy in biobank research. Am. J. Hum. Genet. 2009, 85, 643–654. [Google Scholar] [CrossRef] [Green Version]
- Suthers, G.K.; Armstrong, J.; McCormack, J.; Trott, D. Letting the family know: Balancing ethics and effectiveness when notifying relatives about genetic testing for a familial disorder. J. Med. Genet. 2006, 43, 665–670. [Google Scholar] [CrossRef] [PubMed]
- Compadre, A.J.; Simonson, M.E.; Gray, K.; Runnells, G.; Kadlubar, S.; Zorn, K.K. Challenges in recruiting African-American women for a breast cancer genetics study. Hered. Cancer Clin. Pract. 2018, 16, 8. [Google Scholar] [CrossRef] [PubMed]
- Halbert, C.H.; Kessler, L.; Collier, A.; Weathers, B.; Stopfer, J.; Domchek, S.; McDonald, J.A. Low rates of African American participation in genetic counseling and testing for BRCA1/2 mutations: Racial disparities or just a difference? J. Genet. Couns. 2012, 21, 676–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Senier, L.; McBride, C.M.; Ramsey, A.T.; Bonham, V.L.; Chambers, D.A. Blending Insights from Implementation Science and the Social Sciences to Mitigate Inequities in Screening for Hereditary Cancer Syndromes. Int. J. Environ. Res. Public Health 2019, 16, 3899. [Google Scholar] [CrossRef] [Green Version]
- National Academies of Sciences E, and Medicine. Action Collaboratives: Genomics and Population Health Action Collaborative 2018. Available online: http://www.nationalacademies.org/hmd/Activities/Research/GenomicBasedResearch/InnovationCollaboratives/Genomics-andPopulation-Health.aspx (accessed on 1 May 2022).
- Hughes, C.; Peterson, S.K.; Ramirez, A.; Gallion, K.J.; McDonald, P.G.; Skinner, C.S.; Bowen, D. Minority recruitment in hereditary breast cancer research. Cancer Epidemiol. Biomark. Prev. A Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2004, 13, 1146–1155. [Google Scholar] [CrossRef]
- McDonald, J.A.; Barg, F.K.; Weathers, B.; Guerra, C.E.; Troxel, A.B.; Domchek, S.; Bowen, D.; Shea, J.A.; Halbert, C.H. Understanding participation by African Americans in cancer genetics research. J. Natl. Med. Assoc. 2012, 104, 324–330. [Google Scholar] [CrossRef] [Green Version]
- Ewing, A.; Thompson, N.; Ricks-Santi, L. Strategies for enrollment of African Americans into cancer genetic studies. J. Cancer Educ. Off. J. Am. Assoc. Cancer Educ. 2015, 30, 108–115. [Google Scholar] [CrossRef] [Green Version]
- Sanderson, S.C.; Diefenbach, M.A.; Zinberg, R.; Horowitz, C.R.; Smirnoff, M.; Zweig, M.; Streicher, S.; Jabs, E.W.; Richardson, L.D. Willingness to participate in genomics research and desire for personal results among underrepresented minority patients: A structured interview study. J. Community Genet. 2013, 4, 469–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horowitz, C.R.; Brenner, B.L.; Lachapelle, S.; Amara, D.A.; Arniella, G. Effective recruitment of minority populations through community-led strategies. Am. J. Prev. Med. 2009, 37 (Suppl. 1), S195–S200. [Google Scholar] [CrossRef] [Green Version]
- Obeid, J.S.; Shoaibi, A.; Oates, J.C.; Habrat, M.L.; Hughes-Halbert, C.; Lenert, L.A. Research participation preferences as expressed through a patient portal: Implications of demographic characteristics. JAMIA Open. 2018, 1, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otte-Trojel, T.; de Bont, A.; Rundall, T.G.; van de Klundert, J. What do we know about developing patient portals? a systematic literature review. J. Am. Med. Inform. Assoc. JAMIA 2016, 23, e162–e168. [Google Scholar] [CrossRef] [PubMed]
- Graetz, I.; Gordon, N.; Fung, V.; Hamity, C.; Reed, M.E. The Digital Divide and Patient Portals: Internet Access Explained Differences in Patient Portal Use for Secure Messaging by Age, Race, and Income. Med. Care 2016, 54, 772–779. [Google Scholar] [CrossRef] [PubMed]
- Irizarry, T.; Shoemake, J.; Nilsen, M.L.; Czaja, S.; Beach, S.; DeVito Dabbs, A. Patient Portals as a Tool for Health Care Engagement: A Mixed-Method Study of Older Adults With Varying Levels of Health Literacy and Prior Patient Portal Use. J. Med. Internet Res. 2017, 19, e99. [Google Scholar] [CrossRef] [PubMed]
- Kikut, A.I.; O’Brien, J.M. A Collaborative Community Model for Including Minorities in Genetic Research. JAMA Ophthalmol. 2018, 136, 313–314. [Google Scholar] [CrossRef]
- Scherr, C.L.; Ramesh, S.; Marshall-Fricker, C.; Perera, M.A. A Review of African Americans’ Beliefs and Attitudes About Genomic Studies: Opportunities for Message Design. Front. Genet. 2019, 10, 548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fisher, E.R.; Pratt, R.; Esch, R.; Kocher, M.; Wilson, K.; Lee, W.; Zierhut, H.A. The role of race and ethnicity in views toward and participation in genetic studies and precision medicine research in the United States: A systematic review of qualitative and quantitative studies. Mol. Genet. Genom. Med. 2020, 8, e1099. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.S.; Zhao, S.; Stelzig, D.; Dhar, S.U.; Eble, T.; Yeh, Y.C.; Kwok, O.M. Development and evaluation of a genomics training program for community health workers in Texas. Genet. Med. Off. J. Am. Coll. Med. Genet. 2018, 20, 1030–1037. [Google Scholar] [CrossRef] [Green Version]
- Allen, C.G.; Bethea, B.J.; McKinney, L.P.; Escoffery, C.; Akintobi, T.H.; McCray, G.G.; McBride, C.M. Exploring the Role of Community Health Workers in Improving the Collection of Family Health History: A Pilot Study. Health Promot. Pract. 2021, 15248399211019980. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Kim, M. Needs Assessment in Genomic Education: A Survey of Health Educators in the United States. Health Promot. Pract. 2014, 15, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Dendere, R.; Slade, C.; Burton-Jones, A.; Sullivan, C.; Staib, A.; Janda, M. Patient Portals Facilitating Engagement With Inpatient Electronic Medical Records: A Systematic Review. J. Med. Internet Res. 2019, 21, e12779. [Google Scholar] [CrossRef]
- Tomlinson, T.; De Vries, R.; Ryan, K.; Kim, H.M.; Lehpamer, N.; Kim, S.Y.H. Moral Concerns and the Willingness to Donate to a Research Biobank. JAMA 2015, 313, 417–419. [Google Scholar] [CrossRef]
- Milne, R.; Morley, K.I.; Howard, H.; Niemiec, E.; Nicol, D.; Critchley, C.; Prainsack, B.; Vears, D.; Smith, J.; Steed, C.; et al. Trust in genomic data sharing among members of the general public in the UK, USA, Canada and Australia. Hum. Genet. 2019, 138, 1237–1246. [Google Scholar] [CrossRef] [Green Version]
- Williams, M.S. Population Screening in Health Systems. Annu. Rev. Genom. Hum. Genet. 2022, 23. [Google Scholar] [CrossRef]


{kind=link}
| Total n (%) (n = 23,269) | Enrolled n (%) (n = 1976) | Sample n (%) (n = 1104) | |
|---|---|---|---|
| Gender | |||
| Female | 16,548 (71.12) | 1475 (74.65) | 804 (72.83) |
| Male | 6721 (28.88) | 501 (25.35) | 300 (27.17) |
| Race | |||
| Black | 6454 (27.74) | 223 (11.29) | 102 (9.24) |
| White | 15,880 (68.25) | 1670 (84.51) | 960 (86.96) |
| Asian | 287 (1.23) | 25 (1.27) | 15 (1.36) |
| Other | 547 (2.35) | 54 (2.68) | 25 (2.26) |
| Missing | 101 (0.43) | 5 (0.25) | 2 (0.18) |
| Ethnicity | |||
| Hispanic/Latino | 454 (1.95) | 53 (2.68) | 19 (1.72) |
| non-Hispanic/Lat | 22,477 (96.60) | 1902 (96.26) | 1078 (97.64) |
| Missing | 338 (1.45) | 21 (1.06) | 7 (0.63) |
| Age | |||
| 18–29 years | 3631 (15.60) | 250 (12.65) | 111 (10.05) |
| 30–39 years | 4111 (17.67) | 403 (20.39) | 213 (19.29) |
| 40–49 years | 3217 (13.83) | 332 (16.80) | 174 (15.76) |
| 50–59 years | 3411 (14.66) | 320 (16.19) | 192 (17.39) |
| 60–69 years | 4056 (17.43) | 333 (16.85) | 193 (17.48) |
| 70–79 years | 3522 (15.14) | 284 (14.37) | 188 (17.03) |
| 80–89 years | 1153 (4.96) | 50 (2.53) | 30 (2.72) |
| 90+ years | 168 (0.72) | 4 (0.20) | 3 (0.27) |
| Mutually Exclusive Categories out of All Patients Sent Recruitment Messages 1 | Viewed Invitation 2 (n = 9553) | Sample Collected 3 (n = 1104) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Enrolled (n = 1976) | Interested (n = 2076) | Declined (n = 1543) | Non-Response (n = 17,667) | ||||||||||
| n | % | p-Value | % | p-Value | % | p-Value | % | p-Value | % | p-Value | % | p-Value | |
| Total | 23,269 | 8.49 | - | 8.92 | - | 6.63 | - | 75.9 | 41.1 | 4.74 | |||
| Gender | 0.0003 | <0.0001 | 0.2776 | <0.0001 | <0.0001 | 0.1990 | |||||||
| Female | 16,548 | 8.91 | 9.55 | 6.74 | 74.8 | 42.7 | 4.86 | ||||||
| Male | 6721 | 7.45 | 7.38 | 6.35 | 78.8 | 37.0 | 4.46 | ||||||
| Race | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | <0.0001 | |||||||
| Black | 6454 | 3.46 | 6.21 | 5.22 | 85.1 | 28.9 | 1.58 | ||||||
| White | 15,880 | 10.5 | 10.0 | 7.29 | 72.1 | 46.2 | 6.05 | ||||||
| Asian | 287 | 8.71 | 8.36 | 5.57 | 77.4 | 42.5 | 5.23 | ||||||
| Other | 547 | 9.69 | 8.41 | 5.12 | 76.8 | 34.9 | 4.57 | ||||||
| Missing | 101 | 4.95 | 13.9 | 4.95 | 76.2 | 43.6 | 1.98 | ||||||
| Ethnicity | 0.0166 | 0.2135 | 0.0695 | 0.1270 | 0.5471 | 0.0552 | |||||||
| Hispanic/Latino | 454 | 11.7 | 11.0 | 3.96 | 73.4 | 40.8 | 4.19 | ||||||
| non-Hispanic/Lat | 22,477 | 8.46 | 8.90 | 6.69 | 75.9 | 41.1 | 4.80 | ||||||
| Missing | 338 | 6.21 | 7.69 | 6.51 | 79.6 | 38.2 | 2.07 | ||||||
| Age | <0.0001 | <0.0001 | 0.0018 | <0.0001 | <0.0001 | <0.0001 | |||||||
| 18–29 years | 3631 | 6.89 | 7.22 | 5.23 | 80.7 | 38.2 | 3.06 | ||||||
| 30–39 years | 4111 | 9.80 | 8.29 | 7.15 | 74.8 | 44.4 | 5.18 | ||||||
| 40–49 years | 3217 | 10.3 | 10.2 | 6.12 | 73.3 | 43.5 | 5.41 | ||||||
| 50–59 years | 3411 | 9.38 | 10.1 | 6.45 | 74.1 | 41.7 | 5.63 | ||||||
| 60–69 years | 4056 | 8.21 | 9.81 | 6.95 | 74.9 | 42.2 | 4.76 | ||||||
| 70–79 years | 3522 | 8.06 | 9.48 | 7.58 | 74.8 | 40.5 | 5.34 | ||||||
| 80–89 years | 1153 | 4.34 | 5.55 | 6.68 | 83.4 | 29.2 | 2.60 | ||||||
| 90+ years | 168 | 2.38 | 2.98 | 9.52 | 85.1 | 24.4 | 1.79 | ||||||
| Theme | Quotes | Demographics |
|---|---|---|
| REACH: Barriers to Participation and Resulting in Reduced Reach | ||
| Concern about privacy and security of data | I mean is it just you know I just… With all the DNA stuff going on now I just kind of wonder | African American, 55 years old, male, interested |
| The security of any specific findings associated with my medical I don’t know individual medical circumstances. What entities would have access to it and when and what purposes and this kind of thing | White, 53 years old, male, interested | |
| I just don’t want my genetic information out there […] I think you probably have a wonderful computer program within your institution but if somebody was to hack into it then you know that could come back to you later on and say oh we know you’ve got this this and this and I’m just like I don’t I would not be comfortable with just having that out there | White, 68 years old, male, declined | |
| Impact of participation on health or life insurance | Well, I wouldn’t be real thrilled with insurance companies having free range or goes through my medical records but I mean the opportunity for studies and for additional research I don’t care who makes the buck off of it as long as it’s helpful. | White, 53 years old, male, interested |
| Well like I said the questions I had about whether the insurance companies get access to this information particularly since it’s a state function that would concern me that my insurance rates might be adjusted up because of a marker that they found in the DNA that was my concern when I you know I sat there and thought about it for a few minutes first as I don’t know okay but I said you know it’s feasible that might happen Don’t know that it would but do I really want to go through all that so I said probably not and that’s what I had declined. | White, 68 years old, male, declined | |
| No, I mean I’m interested in it. Literally. The only reason I’m not participating, it’s because of the fact that it’s part of my medical record and I’m trying to get life insurance. That’s really the only reason. | White, 40 years old, female, interested | |
| Who will have access to my information? Specifically, I wouldn’t want an insurance company to have access and deny me insurance because I may be a high-risk person to insure if something shows in my test. | Research coordinator tracking log | |
| I wanted to participate in this study, but the risks are too high. I can’t afford to pay a higher health insurance premium. I live on social security. If you can’t protect my data so it can’t be traced back to me by an insurance company, I have to refuse. | Research coordinator tracking log | |
| Do not want to know results | Yeah, very well surprising but again my dad had it two or three of his brothers and sisters in both of his grandparents so you know that’s a real touchy subject with me so that’s another part of the reason I don’t want that information going out there. I’ve never had a test to see if I have the gene or whatever it is and to be honest with you at my age, I don’t know I particularly want to know that information that’s probably a worst-case scenario for any health issue that I have and I really don’t want to. You know, I think I would be more depressed by finding out the results than anything else and I don’t really need that kind of negativity in my life I’ve already has no health problems as it were. | White, 68 years old, male, declined |
| Well, I think it would be scary to find out the results. I mean if people are anxious and get the results, how will they? I guess what I would want to know is what do I do with this information and who can help me navigate that? | White, 68 years old, female, interested | |
| Unaware of consent | That’s a hard one, because my chart and getting those messages is actually really effective. I really don’t remember seeing a message about any of the consent form in my regular email, which I do normally get for and I get noticed notifications in my chart. | White, 34 years old, female, interested |
| Well actually I am one of those that kind of just glances over things and so it probably was there the whole time. | White, 43 years old, female, enrolled | |
| Not that I could think of. I mean the biggest problem I don’t check… I don’t go into my chart that much you know unless my kids tells me I got a message or something and then I could think that’s how I saw it. I saw it when I first logged into it, it said I had a message. | African American, 55 years old, male, interested | |
| REACH: Facilitators to Participation Resulting in Increased Reach | ||
| Family history of a condition | Yes, because of a couple things that they’re that you’re looking at. And because I am a breast cancer survivor and my mother was died of breast cancer and my father died of colon cancer, so those things are near and dear to me. And if there’s something that I need to know or need to tell my biological son, you know that I think it’s important that he has information. | White, 68 years old, female, interested |
| Well, we have in my family there’s colon cancer is a big thing there’s been five of my family members that have had it I’ve not. I get tested every five years of all my doctors are at MUSC. | White, 68 years old, male, declined | |
| The first reason is I don’t know a lot of my family history. I mean I know my mom, my dad, but I didn’t know a lot of my Grandparents so Some of my medical history. Some of the things that I go through might be because it’s just a genetic thing, you know. | African American, 60 years old, female, interested | |
| Involvement in prior genetic testing or personal history | I don’t know what’s too much to share in this, so apologies if I ramble. But I suppose I have a lot of you know, history with cancer and my family, and I think that was kind of one of the big things that you know. I’m also a cancer survivor, so those things kind of were the benchmarks for me. So, if something came up came up that was related to that. For example, I would probably be more moderately interested then genetics, but I’m also still interested in this. You know, until something else were to arise. | White, 34 years old, female, interested |
| I don’t recall having any questions about it or concerns because of the fact that I have already done DNA testing previously, so it didn’t. It didn’t bother me. I mean, maybe some other people might be concerned about privacy. | White, 60 years old, female, enrolled | |
| Interested in results for self | I think for personal reasons I’d like to know if there’s like a potential issue that I could avert. | White, 40 years old, female, interested |
| For the greater good | Well, you’re DNA is already out there. Whether you wanted to or not, I opted to share it because I wanted it. The more they learn, the more accurate they can get. The more that you get to know. | White, 33 years old, female, enrolled |
| And like I said it, if it can help somebody else, maybe down the road, then I think that’s a good thing. | African American, 60 years old, female, interested | |
| No, you had mentioned about different research opportunities. I just click yes, that I’d be interested in entertaining things that come through my chart. Um, I’m not going out and looking to make a living on doing research studies like you know, I, but to the extent that it’s, you know, a couple times or something like that because I’m so close to the university, I do feel like, you know, it’s easy enough to be helpful. | White, 58 years old, female, interested | |
| And it, and it seemed it seemed to me like that’s kind of the future of where this kind of thing is going, where you can actually use someone’s DNA to maybe give them a chance at knowing what their future could be. | White, 47 years old, male, enrolled | |
| IMPLEMENTATION: Barriers to Adherence to Protocols/Fidelity to Protocol at Individual or Clinical Level | ||
| Modifications made to appointment associated with sample collection | It could happen whenever I go into the clinic. That’s what I thought, but I don’t go into. I usually do the virtual visits if I can, unless it’s for some reason I need to be face to face with my doctor. | African American, 29 years old, female, enrolled |
| What can I do to get tested now that the clinic failed to test me? | N/A | |
| Hey there, my provider had to cancel my scheduled appointment tomorrow morning. I will be rescheduling with her at a later date. Is there a way to reschedule when I provide the sample for the research study? | N/A | |
| Distance to provide sample | If possible, it just depends on what it would be worth my while because I would have to drive to Charleston depending on what day it was. And you know if I could drive from work, work is closer to Charleston but still 45 min there and back […] so it just depends on whether it was worth it for me. | African American, 49 years old, female, declined |
| Does participating in this survey require regular trips to MUSC? I live about 2 h away and regular trips are needed; I cannot participate. | N/A | |
| Is there anywhere in the upstate where this saliva submission can be done? Driving to Charleston is about 3 h. Also, from the list of locations provided, would need to know which is the most “northern” so I don’t have so far to drive if I have to. | N/A | |
| IMPLEMENTATION: Facilitators to Adherence to Protocols/Fidelity to Protocol at Individual or Clinical Level | ||
| Efficient collection process | Yeah, I was provided a plastic, I guess vial with the top and it was explained that I need to get my saliva to a certain line and then close up the vile and go back. | White, 34 years old, female, interested |
| They did all my normal office visit stuff. You know, blood pressure or temperature. All that kind of stuff. And wow, ‘cause I actually had two people in the room so one was doing the blood pressure and everything and typing stuff in the chart. The other one said okay, we understand, you know was there and said we have this too. When you’re done filling out all your paperwork. ‘cause I mean my visit was fast. I got there for my appointment. Barely sat down less than five minutes. I was called in the back to get. Now my other stuff walked in the room and it’s like boom boom boom boom you know very quick getting all the free stuff done before the doctor came in and then it’s like okay um the doctor will be in in just a second while you’re waiting for her go ahead and spit in the tube and here’s a pamphlet. Two if you need further information so. | White, 60 years old, female, enrolled | |
| Staff enthusiasm and relationships | No, I will give you a comment on my doctor’s office. In particularly the nurse that was taking my information and getting the saliva sample seemed very excited about it and actually commented that it was a great thing to do, and she was glad to see people do it. | White, 47 years old, male, enrolled |
| EFFECTIVENESS: Facilitators to Effectiveness of Completing Public Health Goal of Identifying High-risk Individuals | ||
| Need to simplify and shorten consent | So, it’s okay, but it’s kind of like if somebody sat me down and you know gave me a synopsis of what it was and answered any questions that I may have and discussed What’s the downside might be versus the upsides. | White, 59 years old, female, interested |
| No, I think it was I mean it was several pages long the whole thing but I think it was fairly straight forward that my only questions had to do with security or I guess it’s best said security of the medical of any kind of findings you know where they’d be released where they wouldn’t be and it appears it’s going to be pretty secure so I was comfortable signing it. | White, 53 years old, male, interested | |
| Uhm, maybe a little more explanation. I, I know legally you have to put a lot of information about what could possibly happen if someone gets your DNA results or in the future, which is kind of scary. So maybe just a little verbiage to kind of make people feel better. That may be on the fence. | White, 47 years old, male, enrolled | |
| And because of that, yes, that’s good. It takes 20 min to go through. I just think you’re going to lose a lot of people because people don’t have the attention span. Understand what it means. It’s intimidating and just you’re going to lose people. But if you say, here’s the gist of it and throughout it have hyperlinks to click on it, then it’s more digestible. Or not as intimidating. | White, 58 years old, female, interested | |
| Better understanding of program | I guess how quickly I’m going to get results. What kind of stuff you are actually going to be sending me with my DNA and then what you all are using our DNA to study like why you’re collecting it? | White, 43 years old, female, enrolled |
| I really value kind of the full story, almost I would almost be more inclined to have the information up front at the beginning to say hey. You know this is this is the purpose and like why this is important, and then at the end if it was possible to kind of have that information to say this is kind of what you’re participation led us to find and what we were able to discover in general with the program. Like you know, kind of a findings summary for me, so it’s sort of like that. I don’t need to necessarily know all the method and what happened like how it was conducted in the process. I think just more of the purpose and then the results are more what I’m most would be most interested in. | White, 34 years old, female, interested | |
| Yes, because okay. So, I did all this, and I did this helpful research to the state of South Carolina. But what does this mean for me? How do I navigate it and am I going to do anything with it? I mean, that’s a personal choice, but how do I get that information? | White, 68 years old, female, interested | |
| Enrolled | Sample Collected | ||
|---|---|---|---|
| n | Percent (n) | p-Value | |
| Total | 1976 | 55.9 (1104) | ---- |
| Gender | 0.0364 | ||
| Female | 1475 | 54.5 (804) | |
| Male | 501 | 59.9 (300) | |
| Race | 0.0096 | ||
| Black | 223 | 45.7 (102) | |
| White | 1670 | 57.5 (960) | |
| Asian | 25 | 60.0 (15) | |
| Other | 53 | 47.2 (25) | |
| Missing | 5 | 40.0 (2) | |
| Ethnicity | 0.0012 | ||
| Hispanic/Latino | 53 | 35.9 (19) | |
| non-Hispanic/Lat | 1902 | 56.7 (1078) | |
| Missing | 21 | 33.3 (7) | |
| Age | <0.0001 | ||
| 18–29 years | 250 | 44.4 (111) | |
| 30–39 years | 403 | 52.9 (213) | |
| 40–49 years | 332 | 52.4 (174) | |
| 50–59 years | 320 | 60.0 (192) | |
| 60–69 years | 333 | 58.0 (193) | |
| 70–79 years | 284 | 66.2 (188) | |
| 80–89 years | 50 | 60.0 (30) | |
| 90+ years | 4 | 75.0 (3) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allen, C.G.; Lenert, L.; Hunt, K.; Jackson, A.; Levin, E.; Clinton, C.; Clark, J.T.; Garrison, K.; Gallegos, S.; Wager, K.; et al. Lessons Learned from the Pilot Phase of a Population-Wide Genomic Screening Program: Building the Base to Reach a Diverse Cohort of 100,000 Participants. J. Pers. Med. 2022, 12, 1228. https://doi.org/10.3390/jpm12081228
Allen CG, Lenert L, Hunt K, Jackson A, Levin E, Clinton C, Clark JT, Garrison K, Gallegos S, Wager K, et al. Lessons Learned from the Pilot Phase of a Population-Wide Genomic Screening Program: Building the Base to Reach a Diverse Cohort of 100,000 Participants. Journal of Personalized Medicine. 2022; 12(8):1228. https://doi.org/10.3390/jpm12081228
Chicago/Turabian StyleAllen, Caitlin G., Leslie Lenert, Kelly Hunt, Amy Jackson, Elissa Levin, Catherine Clinton, John T. Clark, Kelli Garrison, Sam Gallegos, Karen Wager, and et al. 2022. "Lessons Learned from the Pilot Phase of a Population-Wide Genomic Screening Program: Building the Base to Reach a Diverse Cohort of 100,000 Participants" Journal of Personalized Medicine 12, no. 8: 1228. https://doi.org/10.3390/jpm12081228
APA StyleAllen, C. G., Lenert, L., Hunt, K., Jackson, A., Levin, E., Clinton, C., Clark, J. T., Garrison, K., Gallegos, S., Wager, K., He, W., Sterba, K., Ramos, P. S., Melvin, C., Ford, M., Catchpole, K., McMahon, L., & Judge, D. P. (2022). Lessons Learned from the Pilot Phase of a Population-Wide Genomic Screening Program: Building the Base to Reach a Diverse Cohort of 100,000 Participants. Journal of Personalized Medicine, 12(8), 1228. https://doi.org/10.3390/jpm12081228