
Risk of Tuberculosis Caused by Fluticasone Propionate versus Budesonide in Chronic Obstructive Pulmonary Disease: A Nationwide Population-Based Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Design
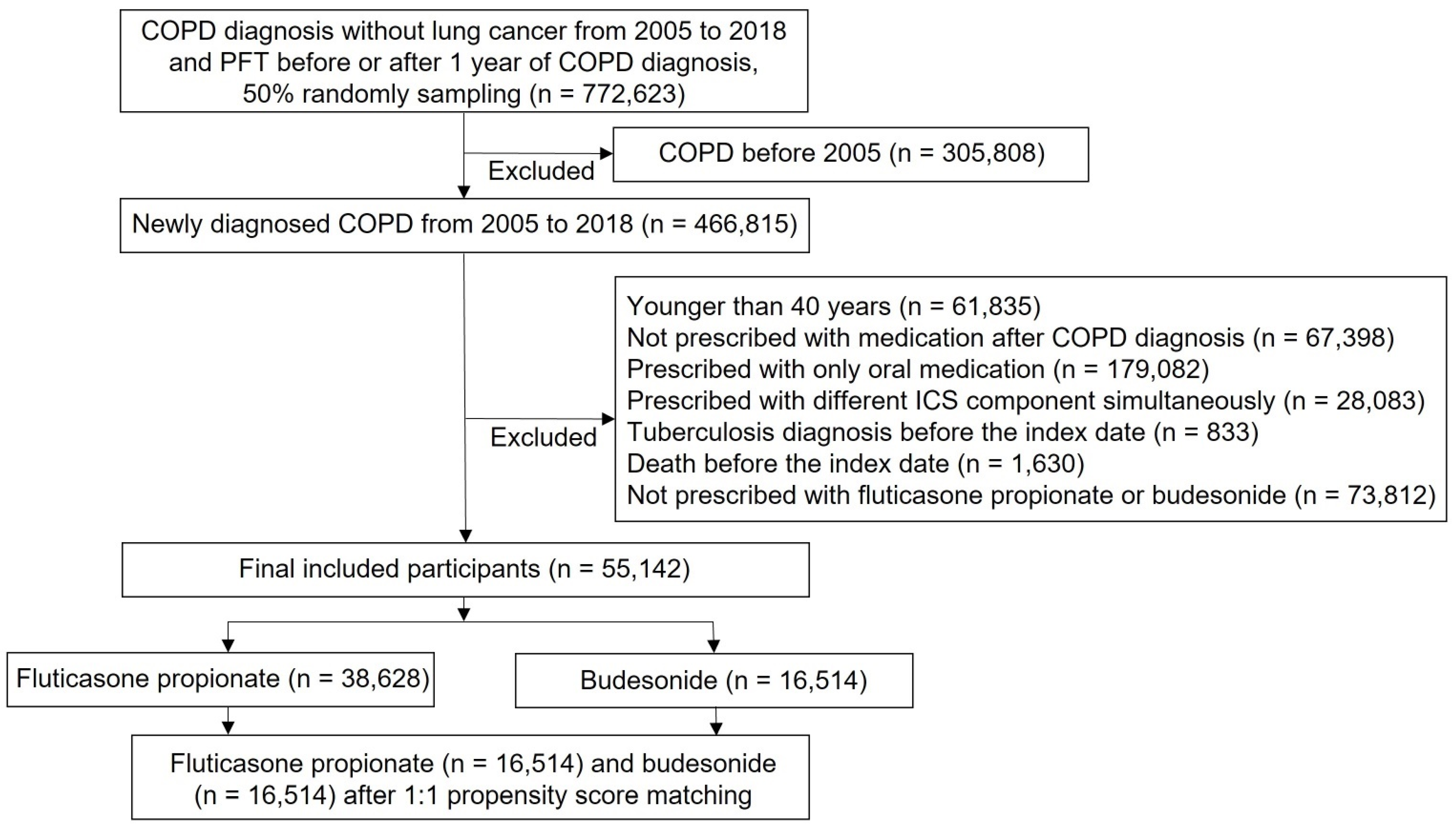
2.3. Study Participants
2.4. Study Outcomes
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Incidence of Tuberculosis
3.3. Risk of Tuberculosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Varmaghani, M.; Dehghani, M.; Heidari, E.; Sharifi, F.; Moghaddam, S.S.; Farzadfar, F. Global prevalence of chronic obstructive pulmonary disease: Systematic review and meta-analysis. East Mediterr. Health J. 2019, 25, 47–57. [Google Scholar] [CrossRef]
- Lee, S.H.; Rhee, C.K.; Yoo, K.; Park, J.W.; Yong, S.J.; Kim, J.; Lee, T.; Lim, S.Y.; Lee, J.-H.; Park, H.Y.; et al. Direct switch from tiotropium to indacaterol/glycopyrronium in chronic obstructive pulmonary disease patients in Korea. Tuberc. Respir. Dis. 2021, 84, 96–104. [Google Scholar] [CrossRef]
- Singh, D. Blood eosinophil counts in chronic obstructive pulmonary disease: A biomarker of inhaled corticosteroid effects. Tuberc. Respir. Dis. 2020, 83, 185–194. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Kostikas, K.; Fang, J.; Tian, H.; Jones, B.; Morgan, C.L.; Fogel, R.; Gutzwiller, F.S.; Cao, H. Evaluation of exacerbations and blood eosinophils in UK and US COPD populations. Respir. Res. 2019, 20, 178. [Google Scholar] [CrossRef]
- Falk, J.; Dik, N.; Bugden, S. An evaluation of early medication use for COPD: A population-based cohort study. Int. J. Chron. Obstr. Pulm. Dis. 2016, 11, 3101–3108. [Google Scholar] [CrossRef] [Green Version]
- Griffith, M.F.; Feemster, L.C.; Zeliadt, S.B.; Donovan, L.M.; Spece, L.J.; Udris, E.M.; Au, D.H. Overuse and misuse of inhaled corticosteroids among veterans with COPD: A cross-sectional study evaluating targets for de-implementation. J. Gen. Intern. Med. 2020, 35, 679–686. [Google Scholar] [CrossRef]
- Festic, E.; Bansal, V.; Gupta, E.; Scanlon, P.D. Association of inhaled corticosteroids with incident pneumonia and mortality in COPD patients; systematic review and meta-analysis. COPD 2016, 13, 312–326. [Google Scholar] [CrossRef]
- Lodise, T.P.; Li, J.; Gandhi, H.N.; O’Brien, G.; Sethi, S. Intraclass difference in pneumonia risk with fluticasone and budesonide in COPD: A systematic review of evidence from direct-comparison studies. Int. J. Chron. Obstr. Pulm. Dis. 2020, 15, 2889–2900. [Google Scholar] [CrossRef]
- Avdeev, S.; Aisanov, Z.; Arkhipov, V.; Belevskiy, A.; Leshchenko, I.; Ovcharenko, S.; Shmelev, E.; Miravitlles, M. Withdrawal of inhaled corticosteroids in COPD patients: Rationale and algorithms. Int. J. Chron. Obstr. Pulm. Dis. 2019, 14, 1267–1280. [Google Scholar] [CrossRef] [Green Version]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S.; et al. Data resource profile: The national health information database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef] [Green Version]
- Rhee, C.K. Chronic obstructive pulmonary disease research by using big data. Clin. Respir. J. 2021, 15, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Janson, C.; Stratelis, G.; Miller-Larsson, A.; Harrison, T.W.; Larsson, K. Scientific rationale for the possible inhaled corticosteroid intraclass difference in the risk of pneumonia in COPD. Int. J. Chron. Obstr. Pulm. Dis. 2017, 12, 3055–3064. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.H.; Kim, K.; Hyun, M.K.; Jang, E.J.; Lee, N.R.; Yim, J.J. Use of inhaled corticosteroids and the risk of tuberculosis. Thorax 2013, 68, 1105–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marzoratti, L.; Iannella, H.A.; Waterer, G.W. Inhaled corticosteroids and the increased risk of pneumonia. Ther. Adv. Respir. Dis. 2013, 7, 225–234. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.H.; Chang, C.H.; Wu, F.L.; Shen, L.J.; Calverley, P.M.A.; Löfdahl, C.G.; Lai, M.S.; Mahler, D.A. Use of inhaled corticosteroids in patients with COPD and the risk of TB and influenza: A systematic review and meta-analysis of randomized controlled trials. Chest 2014, 145, 1286–1297. [Google Scholar] [CrossRef]
- Brassard, P.; Suissa, S.; Kezouh, A.; Ernst, P. Inhaled corticosteroids and risk of tuberculosis in patients with respiratory diseases. Am. J. Respir. Crit. Care Med. 2011, 183, 675–678. [Google Scholar] [CrossRef]
- Wu, M.F.; Jian, Z.H.; Huang, J.Y.; Jan, C.F.; Nfor, O.N.; Jhang, K.M.; Ku, W.Y.; Ho, C.C.; Lung, C.C.; Pan, H.H.; et al. Post-inhaled corticosteroid pulmonary tuberculosis and pneumonia increases lung cancer in patients with COPD. BMC Cancer 2016, 16, 778. [Google Scholar] [CrossRef] [Green Version]
- Castellana, G.; Castellana, M.; Castellana, C.; Castellana, G.; Resta, E.; Carone, M.; Resta, O. Inhaled corticosteroids and risk of tuberculosis in patients with obstructive lung diseases: A systematic review and meta-analysis of non-randomized studies. Int. J. Chron. Obstr. Pulm. Dis. 2019, 14, 2219–2227. [Google Scholar] [CrossRef] [Green Version]
- Agusti, A.; Fabbri, L.M.; Singh, D.; Vestbo, J.; Celli, B.; Franssen, F.M.E.; Rabe, K.F.; Papi, A. Inhaled corticosteroids in COPD: Friend or foe? Eur. Respir. J. 2018, 52, 1801219. [Google Scholar] [CrossRef]
- Zhang, Q.; Li, S.; Zhou, W.; Yang, X.; Li, J.; Cao, J. Risk of pneumonia with different inhaled corticosteroids in COPD patients: A meta-analysis. COPD 2020, 17, 462–469. [Google Scholar] [CrossRef]
- Brode, S.K.; Campitelli, M.A.; Kwong, J.C.; Lu, H.; Marchand-Austin, A.; Gershon, A.S.; Jamieson, F.B.; Marras, T.K. The risk of mycobacterial infections associated with inhaled corticosteroid use. Eur. Respir. J. 2017, 50, 1700037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.M.; Kuo, K.C.; Wang, Y.H.; Wang, C.Y.; Lai, C.C.; Wang, H.C.; Chen, L.; Yu, C.J. Risk of active tuberculosis among COPD patients treated with fixed combinations of long-acting beta2 agonists and inhaled corticosteroids. BMC Infect. Dis. 2020, 20, 706. [Google Scholar] [CrossRef] [PubMed]
- Chalmers, J.D.; Laska, I.F.; Franssen, F.M.E.; Janssens, W.; Pavord, I.; Rigau, D.; McDonnell, M.J.; Roche, N.; Sin, D.D.; Stolz, D.; et al. Withdrawal of inhaled corticosteroids in COPD: A European Respiratory Society guideline. Eur. Respir. J. 2020, 55, 2000351. [Google Scholar] [CrossRef] [PubMed]
- Edsbäcker, S.; Wollmer, P.; Selroos, O.; Borgström, L.; Olsson, B.; Ingelf, J. Do airway clearance mechanisms influence the local and systemic effects of inhaled corticosteroids? Pulm. Pharmacol. Ther. 2008, 21, 247–258. [Google Scholar] [CrossRef] [PubMed]
- Tashkin, D.P.; Strange, C. Inhaled corticosteroids for chronic obstructive pulmonary disease: What is their role in therapy? Int. J. Chron. Obstr. Pulm. Dis. 2018, 13, 2587–2601. [Google Scholar] [CrossRef] [Green Version]
- Ek, A.; Larsson, K.; Siljerud, S.; Palmberg, L. Fluticasone and budesonide inhibit cytokine release in human lung epithelial cells and alveolar macrophages. Allergy 1999, 54, 691–699. [Google Scholar] [CrossRef]
- Atsuta, J.; Plitt, J.; Bochner, B.S.; Schleimer, R.P. Inhibition of VCAM-1 expression in human bronchial epithelial cells by glucocorticoids. Am. J. Respir. Cell Mol. Biol. 1999, 20, 643–650. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Fluticasone Propionate (n = 16,514) | Budesonide (n = 16,514) | p-Value | |||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age (years) | |||||
| Mean (SD) | 62.39 (11.68) | 62.47 (11.54) | 0.5205 | ||
| 40–49 | 2728 | 16.52 | 2590 | 15.68 | 0.2795 |
| 50–59 | 4188 | 25.36 | 4174 | 25.28 | |
| 60–69 | 4754 | 28.79 | 4854 | 29.39 | |
| 70–79 | 3660 | 22.16 | 3716 | 22.50 | |
| ≥80 | 1184 | 7.17 | 1180 | 7.15 | |
| Sex | |||||
| Male | 9413 | 57.00 | 9364 | 56.70 | 0.5862 |
| Female | 7101 | 43.00 | 7150 | 43.30 | |
| Comorbidity | |||||
| Bronchiectasis | 1436 | 4.92 | 1452 | 4.92 | 0.7553 |
| Diabetes | 5132 | 17.60 | 5215 | 17.66 | 0.3248 |
| Hypertension | 9346 | 32.05 | 9445 | 31.99 | 0.2713 |
| Heart failure | 3217 | 11.03 | 3260 | 11.04 | 0.5512 |
| Stroke | 3530 | 12.11 | 3569 | 12.09 | 0.6014 |
| Chronic kidney disease | 825 | 2.83 | 861 | 2.92 | 0.3681 |
| Chronic liver disease | 5674 | 19.46 | 5720 | 19.38 | 0.5944 |
| CCI | |||||
| Mean (SD) | 3.05 (2.11) | 3.01 (2.08) | 0.0615 | ||
| <2 | 4542 | 27.50 | 4586 | 27.77 | 0.5882 |
| ≥2 | 11,972 | 72.50 | 11,928 | 72.23 | |
| Bronchodilator | |||||
| SABA | 327 | 1.98 | 1035 | 6.27 | <0.0001 |
| LAMA | 2186 | 13.24 | 2231 | 13.51 | 0.4669 |
| LABA | 12,866 | 77.91 | 12,134 | 73.48 | <0.0001 |
| LAMA/LABA | 1135 | 6.87 | 1114 | 6.75 | 0.6464 |
| OCS prescription | |||||
| Yes | 13,613 | 84.72 | 13,602 | 84.65 | 0.8467 |
| No | 2456 | 15.28 | 2467 | 15.35 | |
| OCS prescription day | |||||
| Mean (SD) | 11.07 (17.37) | 10.98 (17.56) | 0.6521 | ||
| Interval from COPD diagnosis to index date | |||||
| Mean (SD) | 446.2 (830.7) | 467.7 (905.8) | 0.0245 | ||
| Fluticasone Propionate (n = 16,514) | Budesonide (n = 16,514) | |||
|---|---|---|---|---|
| n | % | n | % | |
| ICS cumulative dose (μg) | ||||
| Mean (SD) | 185,521 (551,181) | 138,827 (314,267) | ||
| 0–15,000 (Q1) | 5691 | 34.46 | 5958 | 36.08 |
| 15,001–60,000 (Q2) | 2700 | 16.35 | 3271 | 19.81 |
| 60,001–225,000 (Q3) | 4019 | 24.34 | 3507 | 21.24 |
| >225,000 (Q4) | 4104 | 24.85 | 3778 | 22.88 |
| Fluticasone Propionate | Budesonide | |||||
|---|---|---|---|---|---|---|
| Variables | Person -Years | Tuberculosis Cases | Incidence (per 100,000) | Person- Years | Tuberculosis Cases | Incidence (per 100,000) |
| Total | 84,810.47 | 233 | 274.73 | 85,907.51 | 184 | 214.18 |
| ICS cumulative dose (μg) | ||||||
| 0–15,000 | 27,033.70 | 63 | 233.04 | 28,415.55 | 67 | 235.79 |
| 15,001–60,000 | 13,161.30 | 39 | 296.32 | 15,916.96 | 40 | 251.30 |
| 60,001–225,000 | 20,137.46 | 48 | 238.36 | 17,043.64 | 32 | 187.75 |
| >225,000 | 24,478.01 | 83 | 339.08 | 24,521.94 | 45 | 183.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, I.; Park, S.; Hong, S.H.; Chang, M.-S.; Lee, S.J.; Yong, S.J.; Lee, W.-Y.; Kim, S.-H.; Lee, J.-H. Risk of Tuberculosis Caused by Fluticasone Propionate versus Budesonide in Chronic Obstructive Pulmonary Disease: A Nationwide Population-Based Study. J. Pers. Med. 2022, 12, 1189. https://doi.org/10.3390/jpm12071189
Yu I, Park S, Hong SH, Chang M-S, Lee SJ, Yong SJ, Lee W-Y, Kim S-H, Lee J-H. Risk of Tuberculosis Caused by Fluticasone Propionate versus Budesonide in Chronic Obstructive Pulmonary Disease: A Nationwide Population-Based Study. Journal of Personalized Medicine. 2022; 12(7):1189. https://doi.org/10.3390/jpm12071189
Chicago/Turabian StyleYu, Iseul, Sunmin Park, Se Hwa Hong, Min-Seok Chang, Seok Jeong Lee, Suk Joong Yong, Won-Yeon Lee, Sang-Ha Kim, and Ji-Ho Lee. 2022. "Risk of Tuberculosis Caused by Fluticasone Propionate versus Budesonide in Chronic Obstructive Pulmonary Disease: A Nationwide Population-Based Study" Journal of Personalized Medicine 12, no. 7: 1189. https://doi.org/10.3390/jpm12071189
APA StyleYu, I., Park, S., Hong, S. H., Chang, M.-S., Lee, S. J., Yong, S. J., Lee, W.-Y., Kim, S.-H., & Lee, J.-H. (2022). Risk of Tuberculosis Caused by Fluticasone Propionate versus Budesonide in Chronic Obstructive Pulmonary Disease: A Nationwide Population-Based Study. Journal of Personalized Medicine, 12(7), 1189. https://doi.org/10.3390/jpm12071189