
The Detrimental Clinical Associations of Anxiety and Depression with Difficult Asthma Outcomes

 , , , ,
, , , ,  , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
Analysis
- We used enrolment data to characterise WATCH patients with anxiety alone against patients with no clinical diagnosis of anxiety or depression (controls). This was repeated for depression alone and for dual anxiety and depression;
- In patients with the associated psychological comorbidity, the HADS-A (anxiety) and -D (depression) scores were utilised to stratify and characterise patients based on their self-reported severity of psychological distress [17]. The HADS cut-offs used were normal (0–7), mild (8–10), moderate (11–14) and severe (≥15) [17];
- To further elucidate the association of psychological distress severity with difficult asthma outcomes, we compared patients at polar opposites, i.e., those with ‘severe’ anxiety and/or depression (defined as a clinical diagnosis of anxiety and/or depression and ‘severe’ HADS-A or HADS-D scores) against those who had no anxiety and/or depression (defined as no anxiety, no depression and ‘normal’ HADS-A and HADS-D scores).
3. Results
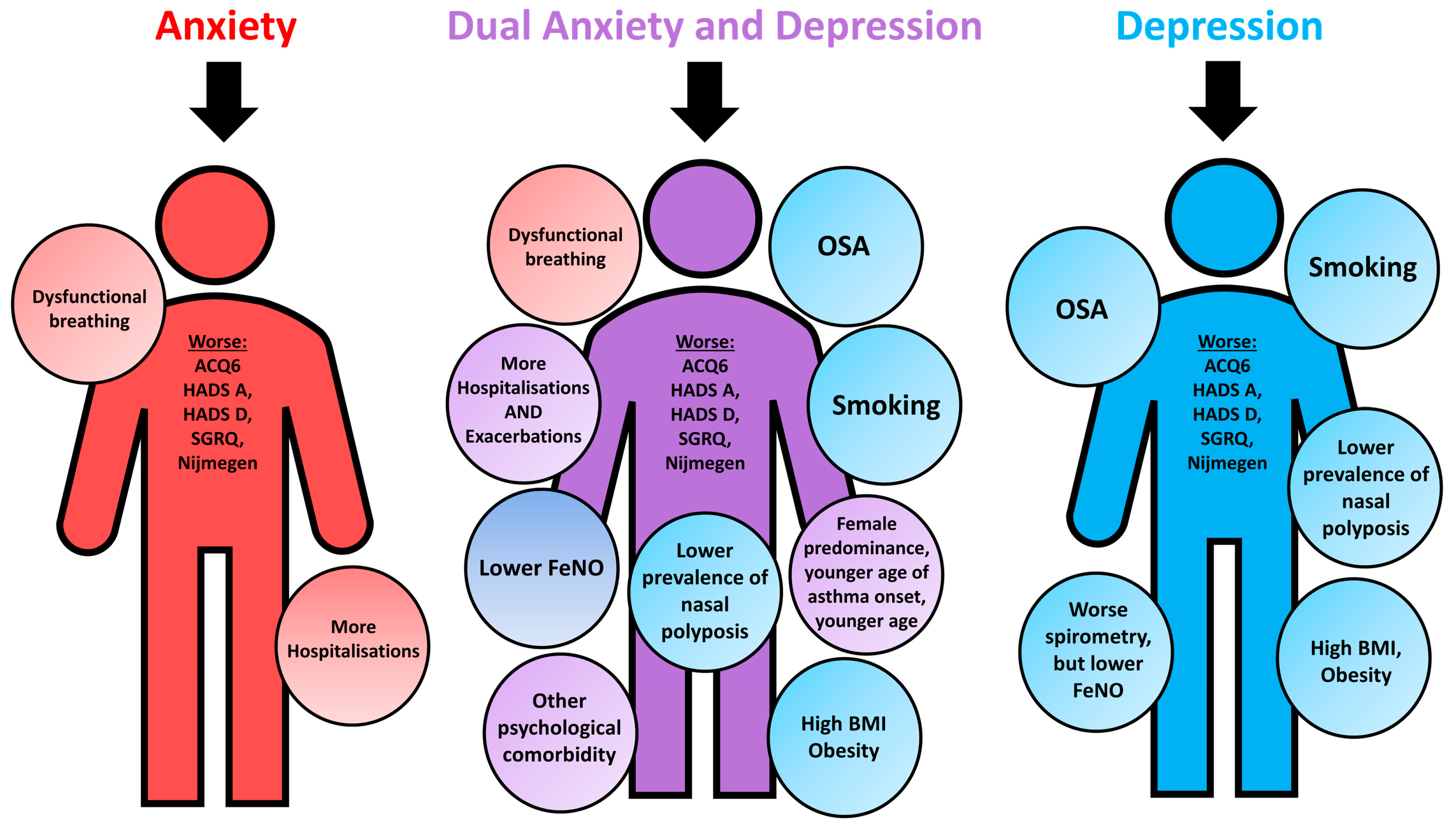
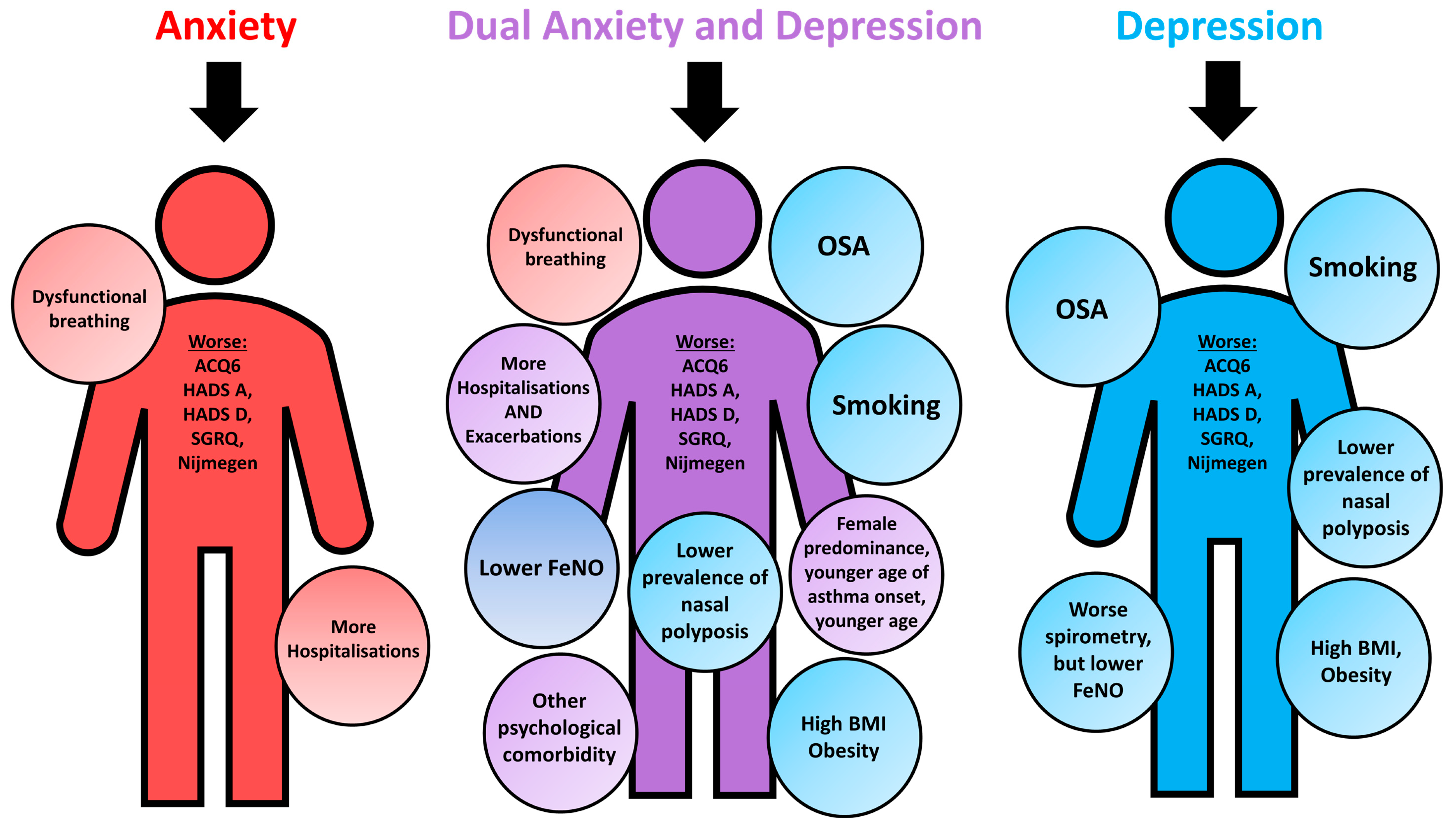
3.1. Anxiety Alone in Difficult Asthma
3.2. Depression Alone in Difficult Asthma
3.3. Dual Anxiety and Depression in Difficult Asthma
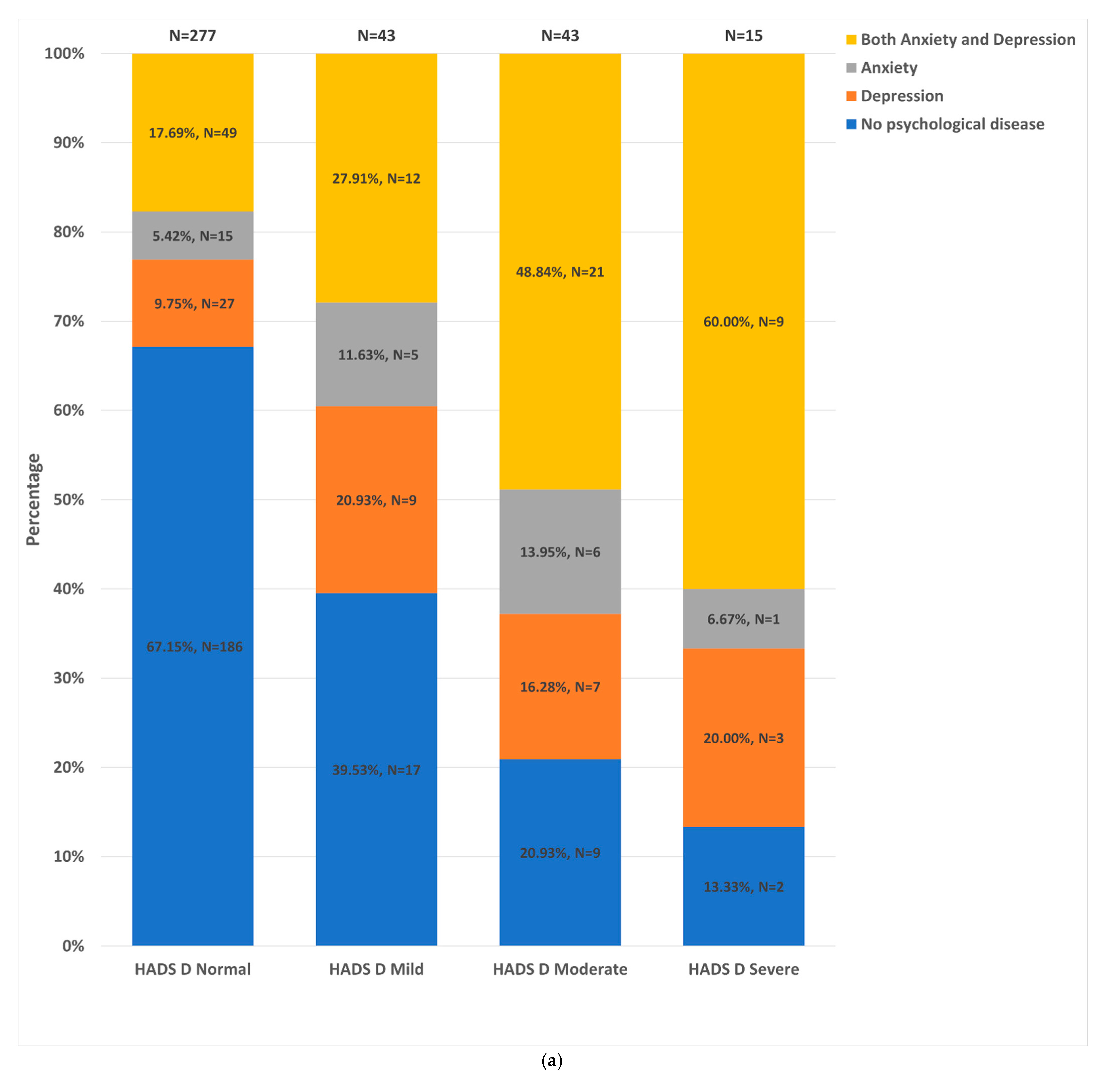
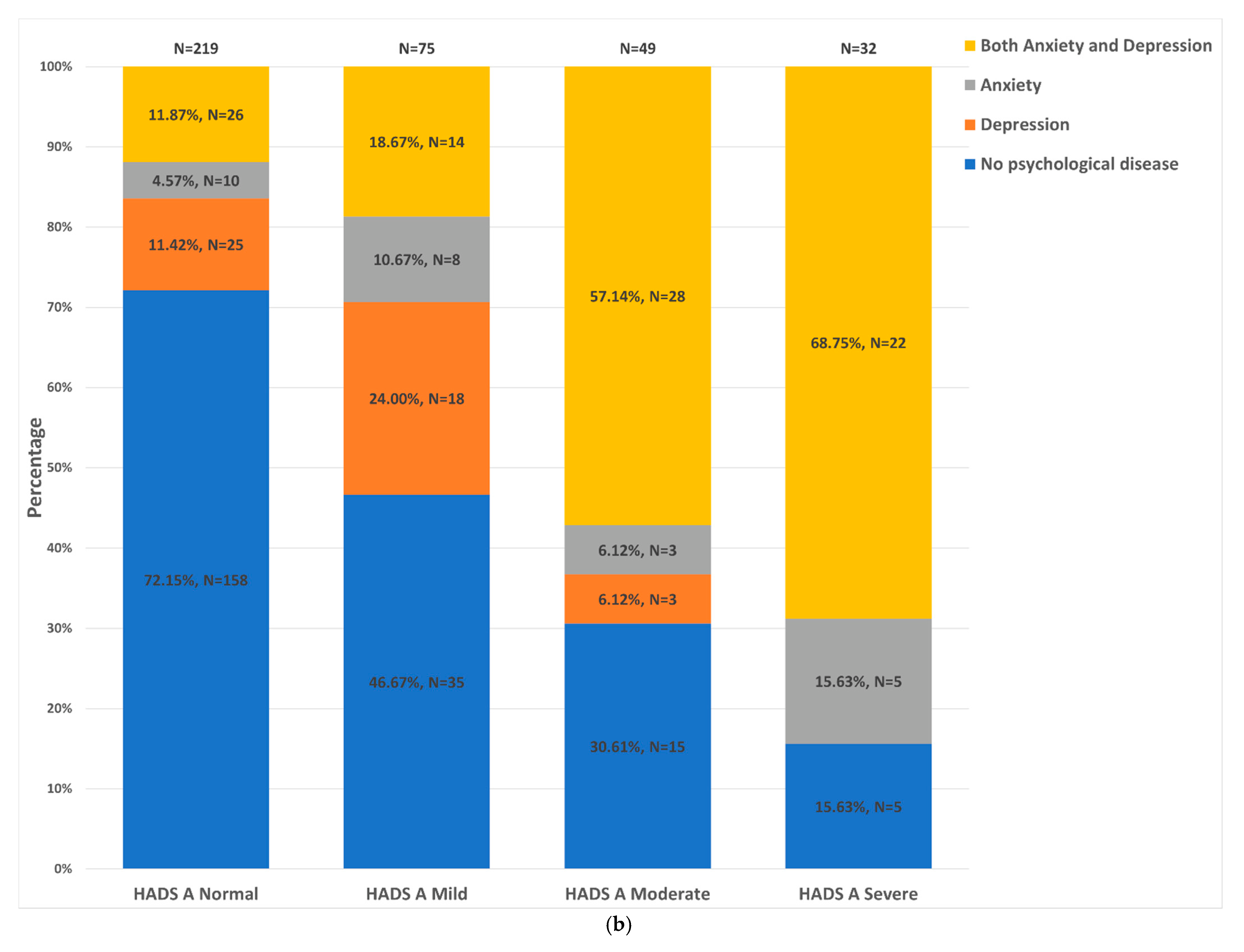
3.4. Distribution of HADS-A and -D Strata
3.5. Clinical Outcomes by Stratification with HADS Scores
3.6. Severe Psychological Comorbidity Is Associated with Worse Asthma Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Dharmage, S.C.; Perret, J.L.; Custovic, A. Epidemiology of Asthma in Children and Adults. Front. Pediatr. 2019, 18, 246. [Google Scholar] [CrossRef]
- Katon, W.; Lozano, P.; Russo, J.; McCauley, E.; Richardson, L.; Bush, T. The prevalence of DSM-IV anxiety and depressive disorders in youth with asthma compared with controls. J. Adolesc. Health 2007, 41, 455–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marco, F.D.; Santus, P.; Centanni, S. Anxiety and depression in asthma. Curr. Opin. Pulm. Med. 2011, 17, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Stanescu, S.; Kirby, S.E.; Thomas, M.; Yardley, L.; Ainsworth, B. A systematic review of psychological, physical health factors, and quality of life in adult asthma. NPJ Prim. Care Respir. Med. 2019, 29, 37. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, X.; Zheng, J.; Wang, L.; Zhang, H.-P.; Wang, L.; Gang, W. Co-morbid psychological dysfunction is associated with a higher risk of asthma exacerbations: A systematic review and meta-analysis. J. Thorac. Dis. 2016, 8, 1257–1268. [Google Scholar] [CrossRef] [Green Version]
- Mahdavian, M.; Power, B.H.; Asghari, S.; Pike, J.C. Effects of Comorbidities on Asthma Hospitalization and Mortality Rates: A Systematic Review. Can. Respir. J. 2018, 2018, 6460379. [Google Scholar] [CrossRef] [Green Version]
- Lavoie, K.L.; Bacon, S.L.; Barone, S.; Cartier, A.; Ditto, B.; Labrecque, M. What Is Worse for Asthma Control and Quality of Life: Depressive Disorders, Anxiety Disorders, or Both? Chest 2006, 130, 1039–1047. [Google Scholar] [CrossRef]
- Zhang, Y.; Cheng, J.; Li, Y.; He, R.; Choudhry, A.A.; Jiang, J.; Pan, P.; Su, X.; Hun, C. Suicidality among patients with asthma: A systematic review and meta-analysis. J. Affect. Disord. 2019, 256, 594–603. [Google Scholar] [CrossRef]
- Shams, M.R.; Bruce, A.C.; Fitzpatrick, A.M. Anxiety Contributes to Poorer Asthma Outcomes in Inner-City Black Adolescents. J. Allergy Clin. Immunol. Pract. 2018, 6, 227–235. [Google Scholar] [CrossRef]
- Tay, T.R.; Hew, M. Comorbid “treatable traits” in difficult asthma: Current evidence and clinical evaluation. Allergy 2018, 73, 1369–1382. [Google Scholar] [CrossRef]
- Tay, T.R.; Radhakrishna, N.; Hore-Lacy, F.; Smith, C.; Hoy, R.; Dabscheck, E.; Hew, M. Comorbidities in difficult asthma are independent risk factors for frequent exacerbations, poor control and diminished quality of life. Respirology 2016, 21, 1384–1390. [Google Scholar] [CrossRef]
- González-Freire, B.; Vázquez, I.; Pértega-Díaz, S. The Relationship of Psychological Factors and Asthma Control to Health-Related Quality of Life. J. Allergy Clin. Immunol. Pract. 2020, 8, 197–207. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental Health and the COVID-19 Pandemic. New Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Azim, A.; Mistry, H.; Freeman, A.; Barber, C.; Newell, C.; Gove, K.; Thirlwall, Y.; Harvey, M.; Bentley, K.; Knight, D.; et al. Protocol for the Wessex AsThma CoHort of difficult asthma (WATCH): A pragmatic real-life longitudinal study of difficult asthma in the clinic. BMC Pulm. Med. 2019, 19, 99. [Google Scholar] [CrossRef]
- Asthma; British Thoracic Society. Better Lung Health for All. Available online: https://www.brit-thoracic.org.uk/quality-improvement/guidelines/asthma/ (accessed on 29 December 2020).
- GINA Severe Asthma. Pocket Guide. Available online: https://ginasthma.org/wp-content/uploads/2019/04/GINA-Severe-asthma-Pocket-Guide-v2.0-wms-1.pdf (accessed on 14 April 2021).
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Rothman, K.J. No Adjustments Are Needed for Multiple Comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Vargas, P.A. Spreading the Word: Comorbidity of Asthma and Depression Is Not Just the Product of a Vulnerable Personality. J. Allergy Clin. Immunol. Practice 2020, 8, 208–209. [Google Scholar] [CrossRef]
- Azim, A.; Freeman, A.; Lavenu, A.; Mistry, H.; Haitchi, H.M.; Newell, C.; Cheng, Y.; Thirlwall, Y.; Harvey, M.; Barber, C.; et al. New Perspectives on Difficult Asthma; Sex and Age of Asthma-Onset Based Phenotypes. J. Allergy Clin. Immunol. Pract. 2020, 8, 3396–3406. [Google Scholar] [CrossRef]
- Wit, L.D.; Luppino, F.; Straten, A.V.; Penninx, B.; Zitman, F.; Cuijpers, P. Depression and obesity: A meta-analysis of community-based studies. Psychiatry Res. 2010, 178, 230–235. [Google Scholar] [CrossRef]
- Mathew, J.L.; Narang, I. Sleeping too Close Together: Obesity and Obstructive Sleep Apnea in Childhood and Adolescence. Paediatr. Respir. Rev. 2014, 15, 211–218. [Google Scholar] [CrossRef]
- Clair, C.; Chiolero, A.; Faeh, D.; Cornuz, J.; Marques-Vidal, P.; Paccaud, F.; Mooser, V.; Waeber, G.; Vollenweider, P. Dose-dependent positive association between cigarette smoking, abdominal obesity and body fat: Cross-sectional data from a population-based survey. BMC Public Health 2011, 11, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor, G.M.J.; Munafò, M.R. Does smoking cause poor mental health? Lancet Psychiatry 2019, 6, 2–3. [Google Scholar] [CrossRef]
- Agache, I.; Ciobanu, C.; Paul, G.; Rogozea, L. Dysfunctional breathing phenotype in adults with asthma—Incidence and risk factors. Clin. Transl. Allergy 2012, 2, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, V.M.; Clark, V.L.; Cordova-Rivera, L.; Wark, P.A.B.; Baines, K.J.; Gibson, P.G. Targeting treatable traits in severe asthma: A randomised controlled trial. Eur. Respir. J. 2020, 55, 1901509. [Google Scholar] [CrossRef]
- Bardin, P.G.; Rangaswamy, J.; Yo, S.W. Managing comorbid conditions in severe asthma. Med. J. Aust. 2018, 209, S11–S17. [Google Scholar] [CrossRef]
- Burke, H.; Davis, J.; Evans, S.; Flower, L.; Tan, A.; Kurukulaaratchy, R.J. A multidisciplinary team case management approach reduces the burden of frequent asthma admissions. ERJ Open Res. 2016, 2, 00039–2016. [Google Scholar] [CrossRef] [Green Version]
- Sastre, J.; Crespo, A.; Fernandez-Sanchez, A.; Rial, M.; Plaza, V. Anxiety, Depression, and Asthma Control: Changes After Standardized Treatment. J. Allergy Clin. Immunol. Pract. 2018, 6, 1953–1959. [Google Scholar] [CrossRef]
- Przybyszowski, M.; Pilinski, R.; Sliwka, A.; Polczyk, R.; Nowobilski, R.; Sladek, K.; Bochenek, G. The impact of clinical and psychological factors on asthma control: The experience of a single asthma center in Poland. J. Asthma 2022, 59, 407–417. [Google Scholar] [CrossRef]
- Deshmukh, V.M.; Toelle, B.G.; Usherwood, T.; O’Grady, B.; Jenkins, C.R. The association of comorbid anxiety and depression with asthma-related quality of life and symptom perception in adults. Respirology 2008, 13, 695–702. [Google Scholar] [CrossRef]
- Pezzulo, G.; Maisto, D.; Barca, L.; Bergh, O.V.D. Symptom Perception From a Predictive Processing Perspective. Clin. Psychol. Eur. 2019, 1, e35952. [Google Scholar] [CrossRef] [Green Version]
- Grenard, J.L.; Munjas, B.A.; Adams, J.L.; Suttorp, M.; Maglione, M.; McGlynn, E.A.; Gellad, W.F. Depression and medication adherence in the treatment of chronic diseases in the United States: A meta-analysis. J. Gen. Intern. Med. 2011, 26, 1175–1182. [Google Scholar] [CrossRef] [Green Version]
- Jiang, M.; Qin, P.; Yang, X. Comorbidity between depression and asthma via immune-inflammatory pathways: A meta-analysis. J. Affect. Disord. 2014, 166, 22–29. [Google Scholar] [CrossRef]
- Isono, S. Obesity and obstructive sleep apnoea: Mechanisms for increased collapsibility of the passive pharyngeal airway. Respirology 2012, 17, 32–42. [Google Scholar] [CrossRef]
- Ahovuo-Saloranta, A.; Csonka, P.; Lehtimäki, L. Basic characteristics and clinical value of FeNO in smoking asthmatics—A systematic review. J. Breath Res. 2019, 13, 034003. [Google Scholar] [CrossRef]
- Gibeon, D.; Batuwita, K.; Osmond, M.; Heaney, L.G.; Brightling, C.E.; Niven, R.; Mansur, A.; Chaudhuri, R.; Bucknall, C.E.; Rowe, A.; et al. Obesity-Associated Severe Asthma Represents a Distinct Clinical Phenotype: Analysis of the British Thoracic Society Difficult Asthma Registry Patient Cohort According to BMI. Chest 2013, 143, 406–414. [Google Scholar] [CrossRef]
- Fellows, J.L.; Flower, L.; Blakey, J.; Kurukulaaratchy, R.; Howard, R.; Mansur, A. Case series: The application of “third wave” cognitive behavioural therapies in difficult to treat asthma. J. Asthma 2015, 52, 905–912. [Google Scholar] [CrossRef]
- Ainsworth, B.; Patel, A.; Eyles, C.; Davies, G.E.; Kurukulaaratchy, R.; Thomas, M. Feasibility and Acceptability of a Group Mindfulness Intervention in a Difficult Asthma Clinic. Mindfulness 2020, 11, 1734–1746. [Google Scholar] [CrossRef]
- Wu, Z.; Fang, Y. Comorbidity of depressive and anxiety disorders: Challenges in diagnosis and assessment. Shanghai Arch. Psychiatry 2014, 26, 227–231. [Google Scholar]
- Hodes, G.E.; Epperson, C.N. Sex Differences in Vulnerability and Resilience to Stress Across the Life Span. Biol. Psychiatry 2019, 86, 421–432. [Google Scholar] [CrossRef]
- Fong, W.C.G.; Azim, A.; Knight, D.; Mistry, H.; Freeman, A.; Felongco, M.; Kyyaly, A.; Harvey, M.; Dennison, P.; Zhang, H.; et al. Real-world Omalizumab and Mepolizumab treated Difficult Asthma Phenotypes and their Clinical Outcomes. Clin. Exp. Allergy 2021, 51, 1019–1032. [Google Scholar] [CrossRef]
- Gaynes, B.N.; Magruder, K.M.; Burns, B.J.; Wagner, H.R.; Yarnall, K.S.H.; Broadhead, W.E. Does a coexisting anxiety disorder predict persistence of depressive illness in primary care patients with major depression? Gen. Hosp. Psychiatry 1999, 21, 158–167. [Google Scholar] [CrossRef]
- Hecht, H.; Zerssen, D.V.; Wittchen, H.-U. Anxiety and depression in a community sample: The influence of comorbidity on social functioning. J. Affect. Disord. 1990, 18, 137–144. [Google Scholar] [CrossRef]
- Wells, K.B.; Golding, J.M.; Burnam, M.A. Psychiatric disorder in a sample of the general population with and without chronic medical conditions. Am. J. Psychiatry 1988, 145, 976–981. [Google Scholar] [PubMed] [Green Version]
- Foster, J.M.; McDonald, V.M.; Guo, M.; Reddel, H.K. “I have lost in every facet of my life”: The hidden burden of severe asthma. Eur. Respir. J. 2017, 50, 1700765. [Google Scholar] [CrossRef] [Green Version]
- Ciprandi, G.; Schiavetti, I.; Rindone, E.; Ricciardolo, F.L.M. The impact of anxiety and depression on outpatients with asthma. Ann. Allergy Asthma Immunol. 2015, 115, 408–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogelzangs, N.; Jonge, P.D.; Smit, J.H.; Bahn, S.; Penninx, B.W. Cytokine production capacity in depression and anxiety. Transl. Psychiatry 2016, 6, e825. [Google Scholar] [CrossRef] [PubMed]
- Brown, E.S.; Sayed, N.; Enkevort, E.V.; Kulikova, A.; Nakamura, A.; Khan, D.A.; Ivleva, E.I.; Sunderajan, P.; Bender, B.G.; Holmes, T. A Randomized, Double-Blind, Placebo-Controlled Trial of Escitalopram in Patients with Asthma and Major Depressive Disorder. J. Allergy Clin. Immunol. Pract. 2018, 6, 1604–1612. [Google Scholar] [CrossRef] [PubMed]
- Braido, F.; Tiotiu, A.; Kowal, K.; Mihaicuta, S.; Novakova, P.; Oguzulgen, I.K. Phenotypes/endotypes-driven treatment in asthma. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 184–189. [Google Scholar] [CrossRef]
- Dean, K.; Niven, R. Asthma Phenotypes and Endotypes: Implications for Personalised Therapy. BioDrugs 2017, 31, 393–408. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Anxiety Alone (N = 35, 6.99%) | Depression Alone (N = 51, 10.7%) | Dual Anxiety and Depression (N = 104, 20.8%) | Control (N = 251, 50.1%) | |||||
|---|---|---|---|---|---|---|---|---|
| Median (IQR) | Missing | Median (IQR) | Missing | Median (IQR) | Missing | Median (IQR) | Missing | |
| Age of asthma onset—y | 28.5 (37.0) | 3 | 20.5 (37.0) | 1 | 11.0 ** (24.0) | 5 | 24.0 (39.0) | 11 |
| Duration of asthma at enrolment—y | 23 (19.5) | 3 | 25 (34.75) | 1 | 26.0 (17) | 5 | 24.0 (29) | 11 |
| Current age—y | 57.0 (17.0) | 0 | 52.0 (20.0) | 0 | 48.0 ** (22.0) | 0 | 58.0 (22.0) | 0 |
| Body mass index—kgm−2 | 30.6 (6.50) | 0 | 32.4 ** (13.5) | 0 | 31.1 ** (10.0) | 3 | 28.3 (8.50) | 2 |
| Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | |
| Sex, male | 34.3% (12) | 0 | 29.4% (15) | 0 | 21.2% ** (22) | 0 | 41.8% (105) | 0 |
| Obesity (body mass index ≥ 30), ever | 54.3% (19) | 0 | 70.6% ** (36) | 0 | 60.4% ** (61) | 3 | 41.4% (103) | 2 |
| Smoked, ever | 54.3% (19) | 0 | 64.7% ** (33) | 0 | 53.8% ** (56) | 0 | 39.6% (99) | 1 |
| Rhinitis, ever | 64.7% (22) | 1 | 54.3% (25) | 5 | 66.0% (66) | 4 | 67.6% (161) | 13 |
| GORD, ever | 71.4% (25) | 0 | 56.0% (28) | 1 | 73.1% (76) | 0 | 59.4% (148) | 2 |
| Eczema, ever | 25.7% (9) | 0 | 21.6% (11) | 0 | 27.9% (29) | 0 | 26.9% (67) | 2 |
| Urticaria/angioedema, ever | 5.88% (2) | 1 | 3.92% (2) | 0 | 12.5% (13) | 0 | 8.80% (22) | 1 |
| Dysfunctional breathing, ever | 61.8% * (21) | 1 | 45.1% (23) | 0 | 65.7% ** (67) | 2 | 37.0% (90) | 8 |
| Intermittent laryngeal obstruction, ever | 16.1% (5) | 4 | 12.0% (6) | 1 | 20.4% (20) | 6 | 11.6% (27) | 18 |
| Obstructive sleep apnoea, ever | 5.88% (2) | 1 | 11.8% ** (6) | 0 | 13.5% ** (14) | 0 | 4.03% (10) | 3 |
| COPD, ever | 17.6% (6) | 1 | 7.84% (4) | 0 | 9.62% (10) | 0 | 9.60% (24) | 1 |
| Bronchiectasis, ever | 9.09% (3) | 2 | 11.8% (6) | 0 | 9.62% (10) | 0 | 16.7% (42) | 0 |
| Positive for aeroallergen SPT, ever | 61.3% (19) | 4 | 68.6% (24) | 16 | 73.8% (59) | 24 | 67.2% (131) | 56 |
| Sulphite sensitivity, ever | 2.94% (1) | 1 | 3.92% (2) | 0 | 10.7% (11) | 1 | 8.00% (20) | 1 |
| Salicylates sensitivity, ever | 20.6% (7) | 1 | 21.6% (11) | 0 | 30.8% (32) | 0 | 24.0% (60) | 1 |
| Nasal polyposis, ever | 16.1% (5) | 4 | 8% (4) ** | 1 | 16.2% (16) * | 5 | 30.2% (71) | 16 |
| Anxiety Alone (N = 35, 6.99%) | Depression Alone (N = 51, 10.7%) | Dual Anxiety and Depression (N = 104, 20.8%) | Control (N = 251, 50.1%) | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD)/ Median (IQR) | Missing | Mean (SD)/ Median (IQR) | Missing | Mean (SD)/ Median (IQR) | Missing | Mean (SD)/ Median (IQR) | Missing | |
| ACQ6 at enrolment, median (IQR) | 3.00 * (2.20) | 4 | 3.20 * (1.30) | 2 | 2.80 ** (1.60) | 9 | 2.20 (1.80) | 14 |
| HADS-A at enrolment, median (IQR) | 10.0 ** (5.00) | 9 | 7.00 * (5.00) | 5 | 11.0 ** (8.00) | 14 | 4.00 (6.00) | 38 |
| HADS-D at enrolment, median (IQR) | 5.00 * (9.00) | 8 | 6.50 ** (7.00) | 5 | 7.00 ** (8.00) | 13 | 4.00 (5.00) | 37 |
| SGRQ score (Symptoms) at enrolment, mean (SD) | 68.60 (24.05) | 3 | 67.07 (20.52) | 9 | 70.69 ** (18.32) | 20 | 60.23 (23.65) | 44 |
| SGRQ score (Activity) at enrolment, mean (SD) | 70.03 * (28) | 6 | 74.93 ** (19.05) | 10 | 72.28 ** (21.94) | 23 | 55.48 (25.85) | 60 |
| SGRQ score (Impacts) at enrolment, mean (SD) | 44.96 * (23.68) | 5 | 44.95 ** (19.59) | 10 | 50.10 ** (20.02) | 22 | 34.76 (20.73) | 54 |
| SGRQ score (Total) at enrolment, mean (SD) | 57.12 ** (22.92) | 6 | 57.28 ** (17.34) | 11 | 60.29 ** (17.81) | 24 | 45.35 (20.05) | 65 |
| Nijmegen score at enrolment, median (IQR) | 28.0 ** (16.0) | 9 | 22.0 * (18.0) | 14 | 30.0 ** (17.0) | 26 | 17.0 (15.0) | 64 |
| Anxiety Alone (N = 35, 6.99%) | Depression Alone (N = 51, 10.7%) | Dual Anxiety and Depression (N = 104, 20.8%) | Control (N = 251, 50.1%) | |||||
|---|---|---|---|---|---|---|---|---|
| Median (IQR) | Missing | Median (IQR) | Missing | Median (IQR) | Missing | Median (IQR) | Missing | |
| Number of asthma exacerbations in the prior 12 months | 4.00 (5.00) | 3 | 4.00 (5.00) | 4 | 3.00 * (5.00) | 8 | 3.00 (3.00) | 25 |
| Number of asthma hospitalisations in the prior 12 months | 0.00 * (2.00) | 1 | 0.0 (1.00) | 1 | 0.00 * (1.00) | 0 | 0.00 (0.00) | 1 |
| Number of days taken off work/education in the prior 12 months due to asthma | 7.00 (20.0) | 14 | 13.0 (61.0) | 30 | 7.00 (30.0) | 51 | 4.00 (14.0) | 108 |
| Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | |
| On maintenance OCS at enrolment, yes | 31.3% (10) | 3 | 32.0% (16) | 1 | 30.9% (30) | 7 | 32.0% (77) | 10 |
| ICU admissions for asthma, ever | 28.6% (10) | 0 | 23.5% (12) | 0 | 29.8% (31) | 0 | 25.1% (63) | 0 |
| Intubation for asthma, ever | 17.1% (6) | 0 | 12.0% (6) | 1 | 11.5% (12) | 0 | 12.4% (31) | 1 |
| On asthma biologics at enrolment, yes | 8.6% (3) | 0 | 7.8% (4) | 0 | 15.4% (16) | 0 | 19.1% (48) | 0 |
| Model Name | Cases Included | Variables Included | Final Variables | p-Value | OR; 95 CI |
|---|---|---|---|---|---|
| Dual anxiety and depression vs. controls | 230/355 64.8% | Sex; Age; Age at asthma diagnosis; Smoking, ever; OSA; Nasal polyposis; Dysfunctional breathing; BMI; Duration of asthma at enrolment; Other psychiatric comorbidities; ACQ6; Exacerbations; Hospitalisations | Sex | 0.001 | 0.23 (0.09−0.56) |
| Age | 0.004 | 0.97 (0.94−0.99) | |||
| Smoking, ever | 0.011 | 2.48 (1.23−5.00) | |||
| OSA | 0.021 | 4.08 (1.23−13.46) | |||
| Duration of asthma at enrolment | 0.023 | 1.03 (1.00−1.05) | |||
| Nasal polyposis | 0.058 | 0.42 (0.17−1.03) | |||
| Other psychiatric comorbidities | 0.038 | 3.17 (1.07−9.41) | |||
| ACQ6 | 0.068 | 1.28 (0.98−1.67) | |||
| Severe anxiety and/or depression vs. no anxiety and/or depression | 118/185 63.8% | Sex; Age; Age at asthma diagnosis; Smoking, ever; Brochiectasis; Nasal polyposis; Eczema; OSA; Dysfunctional breathing; BMI GORD; Other psychiatric comorbidities; Exacerbations; ACQ6 | Sex | 0.019 | 0.13 (0.02−0.71) |
| Smoking, ever | 0.067 | 3.54 (0.91−13.68) | |||
| ACQ6 | <0.001 | 3.66 (1.99−6.73) |
| HADS-D Normal (0–7) N = 79, 54.1% | HADS-D Mild (8–10) N = 25, 17.1% | HADS-D Moderate (11–14) N = 30, 20.5% | HADS-D Severe (≥15) N = 12, 8.2% | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD)/ Median (IQR) | Missing | Mean (SD)/ Median (IQR) | Missing | Mean (SD)/ Median (IQR) | Missing | Mean (SD)/ Median (IQR) | Missing | ||
| Number of exacerbations in the prior 12 months, median (IQR) | 2.5 (5) | 5 | 3 (4) | 2 | 4 (6) | 2 | 4.5 (4.25) | 2 | 0.099 |
| Number of days lost from work/education in the prior 12 months, median (IQR) | 5 (28) | 34 | 14 (80) | 16 | 7.5 (45) | 16 | 29 (NA) | 10 | 0.464 |
| Number of hospitalisations the prior 12 months, median (IQR) | 0 (1) | 0 | 0 (1) | 1 | 0 (1) | 0 | 1 (2) | 0 | 0.293 |
| ACQ6 at enrolment, median (IQR) | 2.7 (1.8) | 1 | 3.4 (1.3) | 1 | 3.2 (1.45) | 1 | 4.7 (1.4) | 1 | <0.001 |
| SGRQ score (Symptoms) at enrolment, mean (SD) | 64.51 (18.60) | 9 | 73.11 (13.81) | 3 | 72.63 (21.67) | 1 | 79.69 (11.86) | 4 | 0.031 |
| SGRQ score (Activity) at enrolment, mean (SD) | 64.43 (22.91) | 11 | 83.84 (13.70) | 4 | 78.58 (13.46) | 3 | 92.82 (18.03) | 4 | <0.001 |
| SGRQ score (Impacts) at enrolment, mean (SD) | 39.78 (17.52) | 10 | 53.72 (17.45) | 3 | 54.65 (17.08) | 3 | 73.36 (18.65) | 4 | <0.001 |
| SGRQ score (Total) at enrolment, mean (SD) | 51.02 (16.20) | 12 | 66.43 (13.85) | 4 | 64.65 (13.95) | 3 | 80.43 (14.47) | 4 | <0.001 |
| Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | p-value | |
| ICU admissions for asthma, ever | 21.5% (17) | 0 | 20% (5) | 0 | 60% (18) | 0 | 25% (3) | 0 | 0.001 |
| Intubation for asthma, ever | 7.6% (6) | 0 | 4% (1) | 0 | 23.3% (7) | 0 | 16.7% (2) | 0 | 0.064 |
| On maintenance OCS at enrolment, yes | 27.4% (20) | 6 | 12.5% (3) | 1 | 46.7% (14) | 0 | 81.8% (9) | 1 | <0.001 |
| HADS-D Normal (0–7) N = 49, 53.8% | HADS-D Mild (8–10) N = 12, 13.2% | HADS-D Moderate (11–14) N = 21, 23.1% | HADS-D Severe (≥15) N = 9, 9.9% | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| Mean (SD)/Median (IQR) | Missing | Mean (SD)/Median (IQR) | Missing | Mean (SD) Median (IQR) | Missing | Mean (SD)/Median (IQR) | Missing | ||
| Number of exacerbations in the prior 12 months, Median (IQR) | 2 (4) | 4 | 2 (4) | 1 | 5 (6.5) | 0 | 4 (4.5) | 1 | 0.016 |
| Number of days lost from work/education in the prior 12 months, Median (IQR) | 6 (28.5) | 19 | 3.5 (138.25) | 8 | 5 (30) | 10 | 29 (NA) | 7 | 0.596 |
| Number of hospitalisations the prior 12 months, median (IQR) | 0 (1) | 0 | 0.5 (1) | 0 | 0 (1) | 0 | 1 (1.5) | 0 | 0.626 |
| ACQ6 at enrolment, median (IQR) | 2.7 (1.75) | 1 | 2.9 (1.3) | 0 | 3.25 (1.3) | 1 | 4.5 (1.43) | 1 | 0.001 |
| SGRQ score (Symptoms) at enrolment, mean (SD) | 66.02 (18.61) | 5 | 70.81 (11.46) | 0 | 78.43 (15.70) | 1 | 84.54 (10.30) | 4 | 0.015 |
| SGRQ score (Activity) at enrolment, mean (SD) | 65.44 (22.14) | 5 | 78.66 (13.84) | 1 | 82.91 (13.32) | 3 | 89.70 (23.03) | 4 | 0.002 |
| SGRQ score (Impacts) at enrolment, mean (SD) | 41.72 (17.23) | 5 | 52.09 (18.02) | 0 | 60.59 (12.65) | 3 | 80.28 (16.49) | 4 | <0.001 |
| SGRQ score (Total) at enrolment, mean (SD) | 52.92 (15.68) | 6 | 63.79 (14.03) | 1 | 70.06 (10.27) | 3 | 83.87 (16.16) | 4 | <0.001 |
| Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | Percentage (frequency) | Missing | p-value | |
| ICU admissions for asthma, ever | 20.4% (10) | 0 | 16.7% (2) | 0 | 57.1% (12) | 0 | 33.3% (3) | 0 | 0.014 |
| Intubation for asthma, ever | 2% (1) | 0 | 0% (0) | 0 | 28.6% (6) | 6 | 22.2% (2) | 0 | 0.002 |
| On maintenance OCS at enrolment, yes | 25% (11) | 5 | 9.1% (1) | 1 | 47.6% (10) | 0 | 87.5% (7) | 1 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fong, W.C.G.; Rafiq, I.; Harvey, M.; Stanescu, S.; Ainsworth, B.; Varkonyi-Sepp, J.; Mistry, H.; Kyyaly, M.A.; Barber, C.; Freeman, A.; et al. The Detrimental Clinical Associations of Anxiety and Depression with Difficult Asthma Outcomes. J. Pers. Med. 2022, 12, 686. https://doi.org/10.3390/jpm12050686
Fong WCG, Rafiq I, Harvey M, Stanescu S, Ainsworth B, Varkonyi-Sepp J, Mistry H, Kyyaly MA, Barber C, Freeman A, et al. The Detrimental Clinical Associations of Anxiety and Depression with Difficult Asthma Outcomes. Journal of Personalized Medicine. 2022; 12(5):686. https://doi.org/10.3390/jpm12050686
Chicago/Turabian StyleFong, Wei Chern Gavin, Ishmail Rafiq, Matthew Harvey, Sabina Stanescu, Ben Ainsworth, Judit Varkonyi-Sepp, Heena Mistry, Mohammed Aref Kyyaly, Clair Barber, Anna Freeman, and et al. 2022. "The Detrimental Clinical Associations of Anxiety and Depression with Difficult Asthma Outcomes" Journal of Personalized Medicine 12, no. 5: 686. https://doi.org/10.3390/jpm12050686
APA StyleFong, W. C. G., Rafiq, I., Harvey, M., Stanescu, S., Ainsworth, B., Varkonyi-Sepp, J., Mistry, H., Kyyaly, M. A., Barber, C., Freeman, A., Wilkinson, T., Djukanovic, R., Dennison, P., Haitchi, H. M., & Kurukulaaratchy, R. J. (2022). The Detrimental Clinical Associations of Anxiety and Depression with Difficult Asthma Outcomes. Journal of Personalized Medicine, 12(5), 686. https://doi.org/10.3390/jpm12050686