
Endotypes of Prematurity and Phenotypes of Bronchopulmonary Dysplasia: Toward Personalized Neonatology

 , ,
, , 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
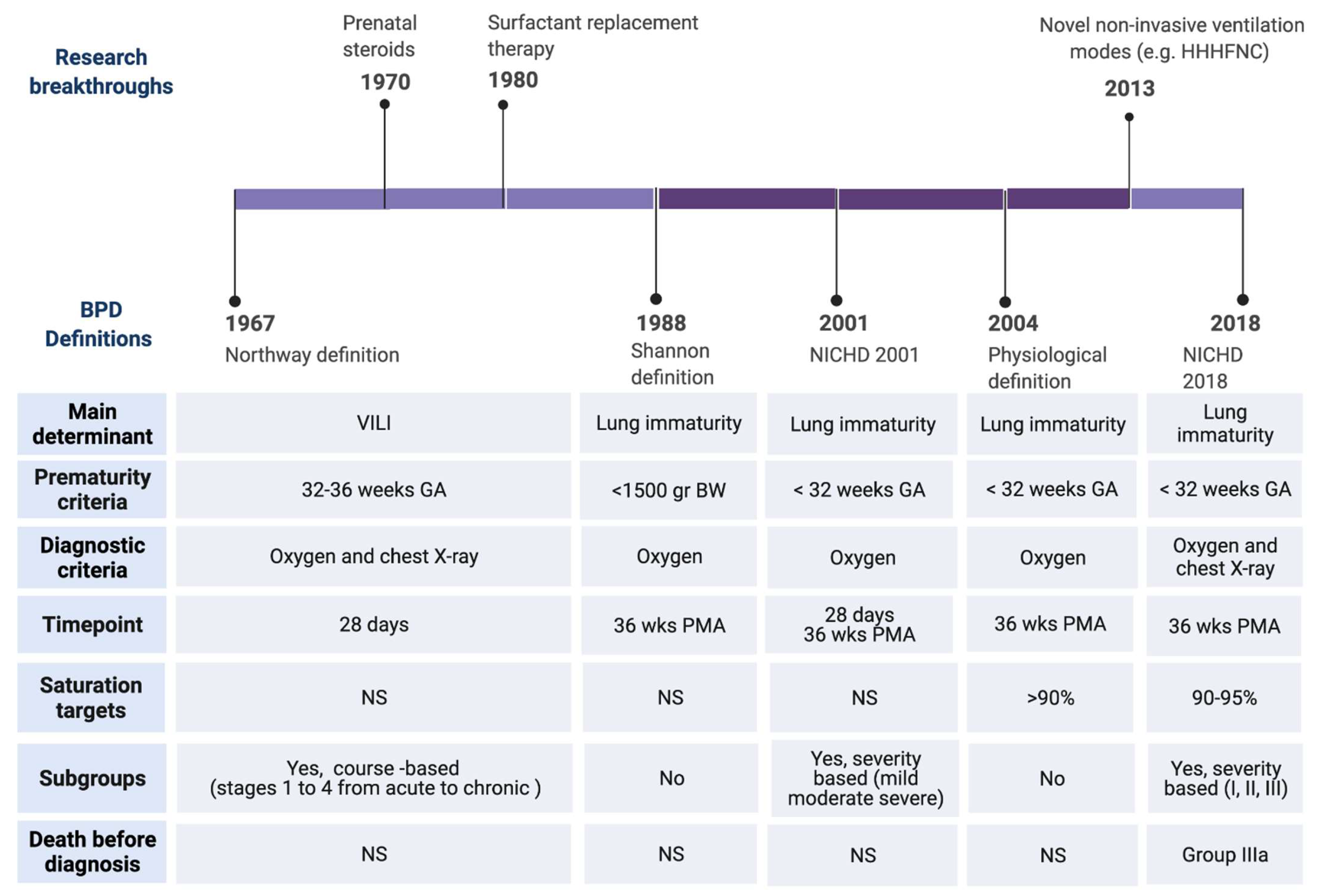
2. Historical Perspectives of BPD Pathogenesis and Diagnostic Criteria
3. Current Definitions of BPD: Downsides and Pitfalls
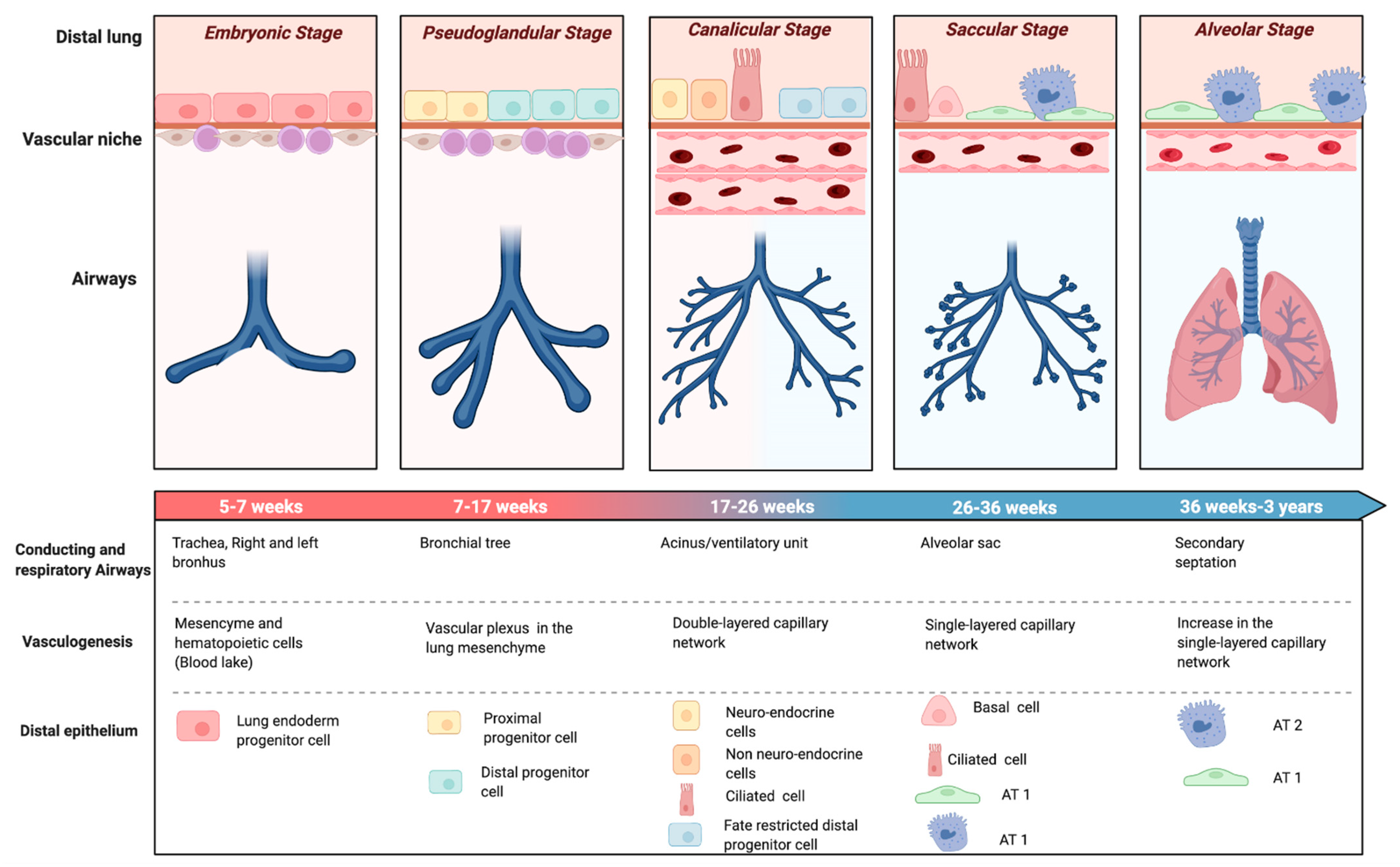
4. Endotypes of Very and Extremely Preterm Birth: Definition and Impact on Fetal Lung Development
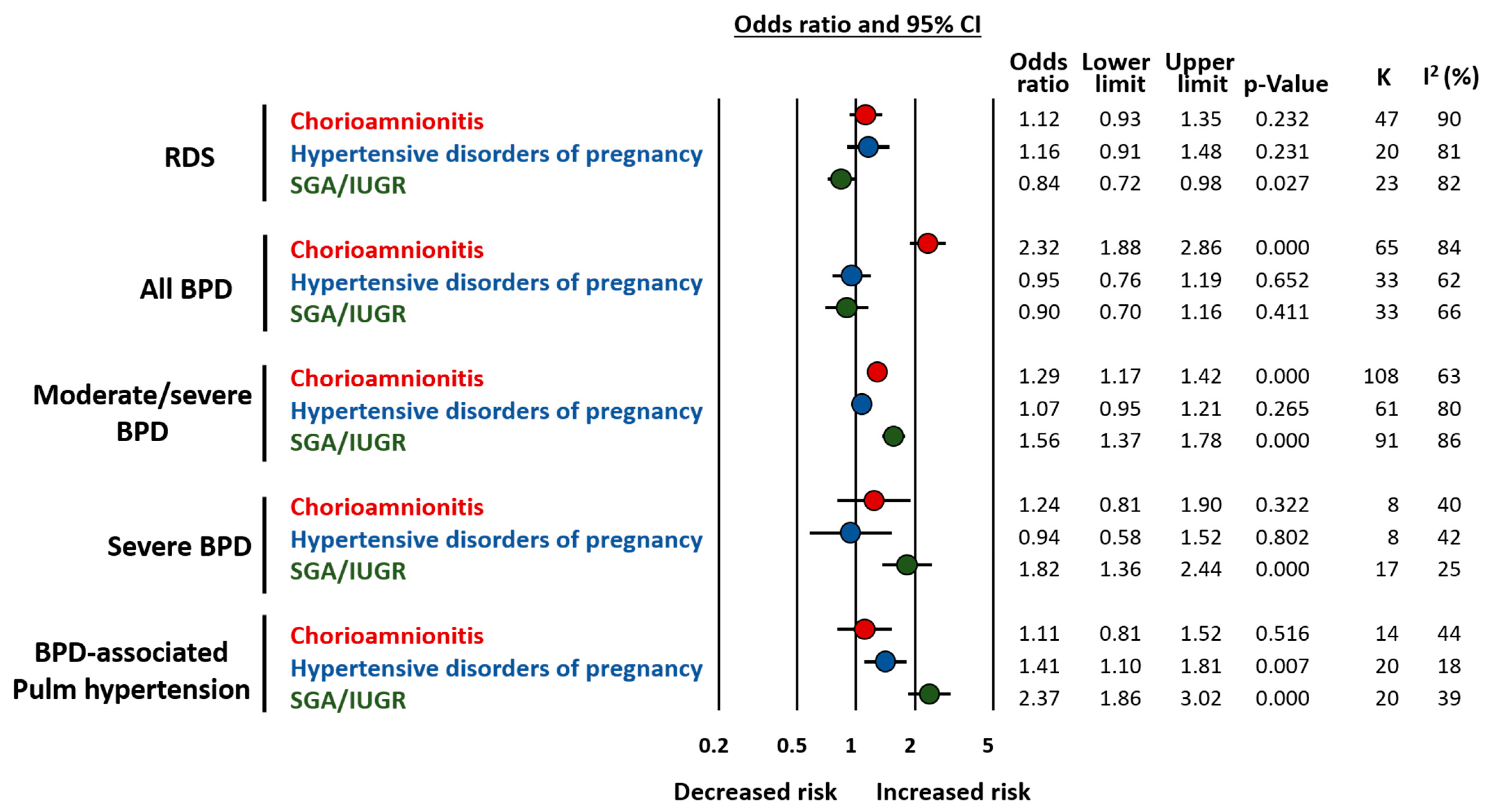
5. Endotypes of Prematurity and Respiratory Outcome
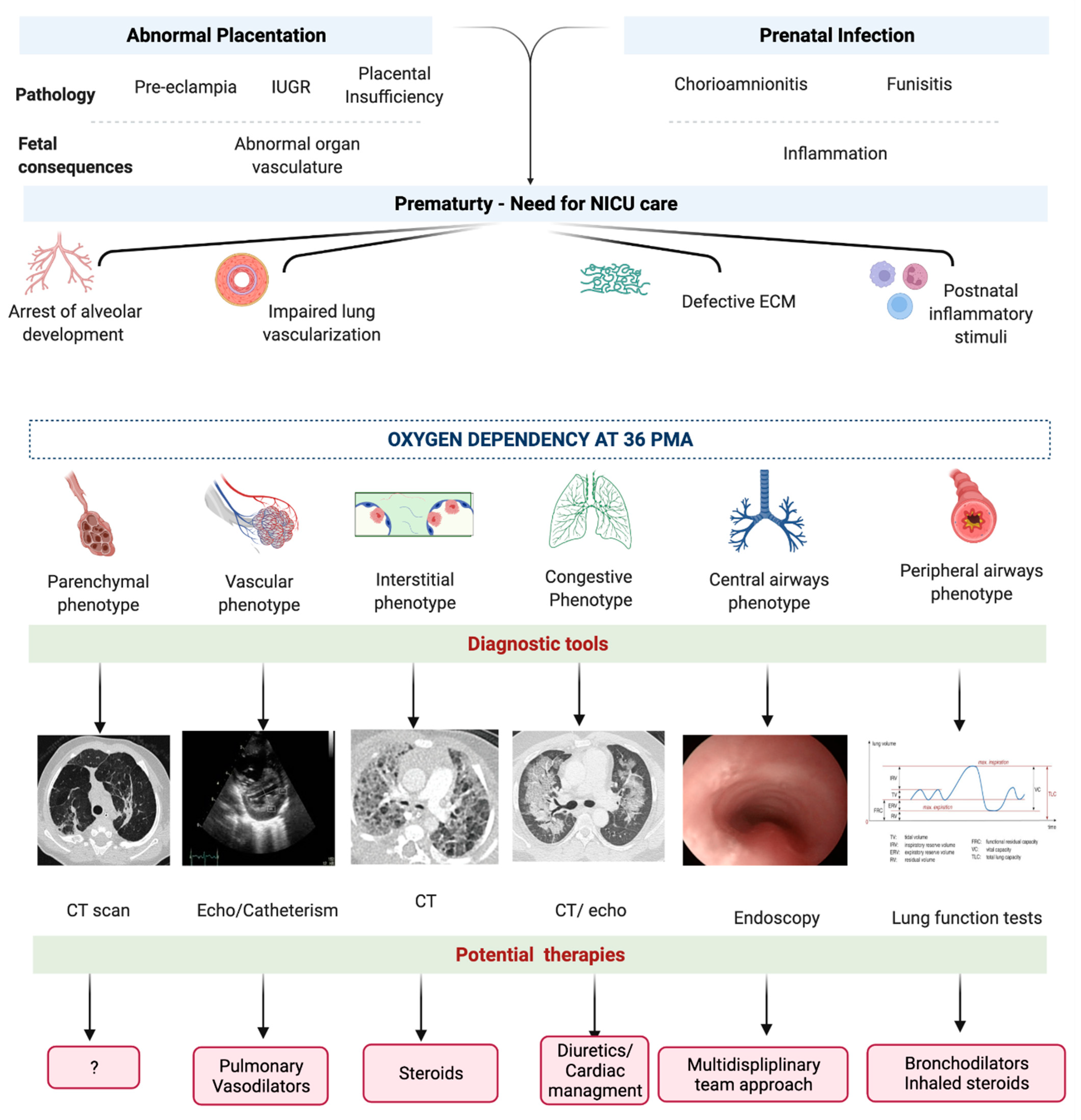
6. Phenotypes of BPD
6.1. Parenchymal Phenotype
6.2. Peripheral Airway Phenotype
6.3. Central Airway Phenotype
6.4. Interstitial Phenotype
6.5. Congestive Phenotype
6.6. Vascular Phenotype
6.7. Mixed Phenotype
7. Prematurity Endotypes and BPD Phenotypes: Implications for Personalized Clinical Management and Research
7.1. Personalized Diagnosis and Follow-Up
7.2. Toward a Personalized Therapy for BPD
7.3. Research
7.4. New Challenges: BPD and COVID-19 Pandemic
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stoll, B.J.; Hansen, N.I.; Bell, E.F.; Walsh, M.C.; Carlo, W.A.; Shankaran, S.; Laptook, A.R.; Sánchez, P.J.; Van Meurs, K.P.; Wyckoff, M.; et al. Trends in Care Practices, Morbidity, and Mortality of Extremely Preterm Neonates, 1993–2012. JAMA J. Am. Med. Assoc. 2015, 314, 1039–1051. [Google Scholar] [CrossRef] [PubMed]
- Horbar, J.D.; Edwards, E.M.; Greenberg, L.T.; Morrow, K.A.; Soll, R.F.; Buus-Frank, M.E.; Buzas, J.S. Variation in Performance of Neonatal Intensive Care Units in the United States. JAMA Pediatr. 2017, 171, e164396. [Google Scholar] [CrossRef] [PubMed]
- Thébaud, B.; Goss, K.N.; Laughon, M.; Whitsett, J.A.; Abman, S.H.; Steinhorn, R.H.; Aschner, J.L.; Davis, P.G.; McGrath-Morrow, S.A.; Soll, R.F. Bronchopulmonary dysplasia. Nat. Rev. Dis. Primers 2019, 5, 78. [Google Scholar] [CrossRef]
- Abman, S.H.; Bancalari, E.; Jobe, A. The evolution of bronchopulmonary dysplasia after 50 years. Am. J. Respir. Crit. Care Med. 2017, 195, 421–424. [Google Scholar] [CrossRef]
- McEvoy, C.T.; Jain, L.; Schmidt, B.; Abman, S.; Bancalari, E.; Aschner, J.L. Bronchopulmonary dysplasia: NHLBI workshop on the primary prevention of chronic lung diseases. Ann. Am. Thorac. Soc. 2014, 11, S146–S153. [Google Scholar] [CrossRef]
- Maitre, N.L.; Ballard, R.A.; Ellenberg, J.H.; Davis, S.D.; Greenberg, J.M.; Hamvas, A.; Pryhuber, G.S. Respiratory consequences of prematurity: Evolution of a diagnosis and development of a comprehensive approach. J. Perinatol. 2015, 35, 313–321. [Google Scholar] [CrossRef]
- Sriram, S.; Schreiber, M.D.; Msall, M.E.; Kuban, K.C.K.; Joseph, R.M.; TM, O.S.; Allred, E.N.; Leviton, A. Cognitive Development and Quality of Life Associated with BPD in 10-Year-Olds Born Preterm. Pediatrics 2018, 141, e20172719. [Google Scholar] [CrossRef]
- Álvarez-Fuente, M.; Arruza, L.; Muro, M.; Zozaya, C.; Avila, A.; López-Ortego, P.; González-Armengod, C.; Torrent, A.; Gavilán, J.L.; Del Cerro, M.J. The economic impact of prematurity and bronchopulmonary dysplasia. Eur. J. Pediatr. 2017, 176, 1587–1593. [Google Scholar] [CrossRef]
- Wang, S.-H.; Tsao, P.-N. Phenotypes of bronchopulmonary dysplasia. Int. J. Mol. Sci. 2020, 21, 6112. [Google Scholar] [CrossRef]
- Northway, W.H., Jr.; Rosan, R.C.; Porter, D.Y. Pulmonary disease following respirator therapy of hyaline-membrane disease. Bronchopulmonary dysplasia. N. Engl. J. Med. 1967, 276, 357–368. [Google Scholar] [CrossRef]
- McGoldrick, E.; Stewart, F.; Parker, R.; Dalziel, S.R. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst. Rev. 2020, 12, CD004454. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, T.; Maeta, H.; Chida, S.; Morita, T.; Watabe, Y.; Abe, T. Artificial surfactant therapy in hyaline-membrane disease. Lancet 1980, 1, 55–59. [Google Scholar] [CrossRef]
- Sreenan, C.; Lemke, R.P.; Hudson-Mason, A.; Osiovich, H. High-flow nasal cannulae in the management of apnea of prematurity: A comparison with conventional nasal continuous positive airway pressure. Pediatrics 2001, 107, 1081–1083. [Google Scholar] [CrossRef] [PubMed]
- Shennan, A.T.; Dunn, M.S.; Ohlsson, A.; Lennox, K.; Hoskins, E.M. Abnormal pulmonary outcomes in premature infants: Prediction from oxygen requirement in the neonatal period. Pediatrics 1988, 82, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Jobe, A.J. The new BPD: An arrest of lung development. Pediatric Res. 1999, 46, 641–643. [Google Scholar] [CrossRef]
- Jobe, A.H.; Bancalari, E. Bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 163, 1723–1729. [Google Scholar] [CrossRef]
- Walsh, M.C.; Yao, Q.; Gettner, P.; Hale, E.; Collins, M.; Hensman, A.; Everette, R.; Peters, N.; Miller, N.; Muran, G.; et al. Impact of a physiologic definition on bronchopulmonary dysplasia rates. Pediatrics 2004, 114, 1305–1311. [Google Scholar] [CrossRef]
- Higgins, R.D.; Jobe, A.H.; Koso-Thomas, M.; Bancalari, E.; Viscardi, R.M.; Hartert, T.V.; Ryan, R.M.; Kallapur, S.G.; Steinhorn, R.H.; Konduri, G.G.; et al. Bronchopulmonary Dysplasia: Executive Summary of a Workshop. J. Pediatr. 2018, 197, 300–308. [Google Scholar] [CrossRef]
- Huizing, M.J.; Villamor-Martínez, E.; Vento, M.; Villamor, E. Pulse oximeter saturation target limits for preterm infants: A survey among European neonatal intensive care units. Eur. J. Pediatr. 2017, 176, 51–56. [Google Scholar] [CrossRef]
- Manja, V.; Lakshminrusimha, S.; Cook, D.J. Oxygen saturation target range for extremely preterm infants: A systematic review and meta-analysis. JAMA Pediatr. 2015, 169, 332–340. [Google Scholar] [CrossRef]
- Mahle, W.T.; Martin, G.R.; Beekman, R.H., 3rd; Morrow, W.R. Endorsement of Health and Human Services recommendation for pulse oximetry screening for critical congenital heart disease. Pediatrics 2012, 129, 190–192. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.J.; Di Fiore, J.M.; Walsh, M.C. Hypoxic Episodes in Bronchopulmonary Dysplasia. Clin. Perinatol. 2015, 42, 825–838. [Google Scholar] [CrossRef] [PubMed]
- Hagadorn, J.I.; Sink, D.W.; Buus-Frank, M.E.; Edwards, E.M.; Morrow, K.A.; Horbar, J.D.; Ferrelli, K.; Soll, R.F. Alarm safety and oxygen saturation targets in the Vermont Oxford Network iNICQ 2015 collaborative. J. Perinatol. 2017, 37, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Manja, V.; Saugstad, O.D.; Lakshminrusimha, S. Oxygen Saturation Targets in Preterm Infants and Outcomes at 18-24 Months: A Systematic Review. Pediatrics 2017, 139, e20161609. [Google Scholar] [CrossRef]
- Huizing, M.J.; Villamor-Martínez, E.; Meus, S.; de Jonge, F.M.; Villamor, E. Dutch Neonatal Intensive Care Nurses’ Perceptions of Pulse Oximeter Saturation Target Limits for Preterm Infants. J. Pediatric Nurs. 2019, 49, e36–e41. [Google Scholar] [CrossRef]
- Alshehri, M.A. Are preterm infants at high altitude at greater risk for the development of bronchopulmonary dysplasia? J. Trop. Pediatr. 2014, 60, 68–73. [Google Scholar] [CrossRef]
- Buendía, J.A.; Ramírez Velasquez, C.; Benjumea-Bedoya, D. Bronchopulmonary dysplasia: Incidence and severity in premature infants born at high altitude. Pediatr. Pulmonol. 2021, 57, 470–475. [Google Scholar] [CrossRef]
- Jensen, E.A.; Dysart, K.; Gantz, M.G.; McDonald, S.; Bamat, N.A.; Keszler, M.; Kirpalani, H.; Laughon, M.M.; Poindexter, B.B.; Duncan, A.F.; et al. The Diagnosis of Bronchopulmonary Dysplasia in Very Preterm Infants. An Evidence-based Approach. Am. J. Respir. Crit. Care Med. 2019, 200, 751–759. [Google Scholar] [CrossRef]
- Guaman, M.C.; Pishevar, N.; Abman, S.H.; Keszler, M.; Truog, W.E.; Panitch, H.; Nelin, L.D. Invasive mechanical ventilation at 36 weeks post-menstrual age, adverse outcomes with a comparison of recent definitions of bronchopulmonary dysplasia. J. Perinatol. 2021, 41, 1936–1942. [Google Scholar] [CrossRef]
- Isayama, T.; Lee, S.K.; Yang, J.; Lee, D.; Daspal, S.; Dunn, M.; Shah, P.S. Revisiting the Definition of Bronchopulmonary Dysplasia: Effect of Changing Panoply of Respiratory Support for Preterm Neonates. JAMA Pediatr. 2017, 171, 271–279. [Google Scholar] [CrossRef]
- Lötvall, J.; Akdis, C.A.; Bacharier, L.B.; Bjermer, L.; Casale, T.B.; Custovic, A.; Lemanske Jr, R.F.; Wardlaw, A.J.; Wenzel, S.E.; Greenberger, P.A. Asthma endotypes: A new approach to classification of disease entities within the asthma syndrome. J. Allergy Clin. Immunol. 2011, 127, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Hamilos, D.L. Chronic rhinosinusitis endotyping: Sharpening the focus on inflammation. J. Allergy Clin. Immunol. 2016, 137, 1457–1459. [Google Scholar] [CrossRef] [PubMed]
- McElrath, T.F.; Hecht, J.L.; Dammann, O.; Boggess, K.; Onderdonk, A.; Markenson, G.; Harper, M.; Delpapa, E.; Allred, E.N.; Leviton, A. Pregnancy disorders that lead to delivery before the 28th week of gestation: An epidemiologic approach to classification. Am. J. Epidemiol. 2008, 168, 980–989. [Google Scholar] [CrossRef]
- Kramer, B.W.; Kallapur, S.; Newnham, J.; Jobe, A.H. Prenatal inflammation and lung development. Semin. Fetal Neonatal Med. 2009, 14, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Taglauer, E.; Abman, S.H.; Keller, R.L. Recent advances in antenatal factors predisposing to bronchopulmonary dysplasia. Semin. Perinatol. 2018, 42, 413–424. [Google Scholar] [CrossRef] [PubMed]
- Bancalari, E. Antenatal Infections and Respiratory Outcome in Preterm Infants. Am. J. Perinatol. 2020, 37, S39–S41. [Google Scholar] [CrossRef]
- Willet, K.E.; Jobe, A.H.; Ikegami, M.; Newnham, J.; Brennan, S.; Sly, P.D. Antenatal endotoxin and glucocorticoid effects on lung morphometry in preterm lambs. Pediatric Res. 2000, 48, 782–788. [Google Scholar] [CrossRef]
- Kallapur, S.G.; Bachurski, C.J.; Cras, T.D.L.; Joshi, S.N.; Ikegami, M.; Jobe, A.H. Vascular changes after intra-amniotic endotoxin in preterm lamb lungs. Am. J. Physiol. Lung Cell Mol. Physiol. 2004, 287, L1178–L1185. [Google Scholar] [CrossRef]
- Wallace, B.; Peisl, A.; Seedorf, G.; Nowlin, T.; Kim, C.; Bosco, J.; Kenniston, J.; Keefe, D.; Abman, S.H. Anti–sFlt-1 therapy preserves lung alveolar and vascular growth in antenatal models of bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2018, 197, 776–787. [Google Scholar] [CrossRef]
- Hirsch, K.; Taglauer, E.; Seedorf, G.; Callahan, C.; Mandell, E.; White, C.W.; Kourembanas, S.; Abman, S.H. Perinatal hypoxia-inducible factor stabilization preserves lung alveolar and vascular growth in experimental bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2020, 202, 1146–1158. [Google Scholar] [CrossRef]
- Abele, A.N.; Taglauer, E.S.; Almeda, M.; Wilson, N.; Abikoye, A.; Seedorf, G.J.; Mitsialis, S.A.; Kourembanas, S.; Abman, S. Antenatal Mesenchymal Stromal Cell Extracellular Vesicle Treatment Preserves Lung Development in a Model of Bronchopulmonary Dysplasia Due to Chorioamnionitis. Am. J. Physiol. Lung Cell Mol. Physiol. 2022, 322, L179–L190. [Google Scholar] [CrossRef] [PubMed]
- Yoder, B.A.; Coalson, J.J.; Winter, V.T.; Siler-Khodr, T.; Duffy, L.B.; Cassell, G.H. Effects of antenatal colonization with Ureaplasma urealyticum on pulmonary disease in the immature baboon. Pediatric Res. 2003, 54, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Collins, J.J.; Kallapur, S.G.; Knox, C.L.; Nitsos, I.; Polglase, G.R.; Pillow, J.J.; Kuypers, E.; Newnham, J.P.; Jobe, A.H.; Kramer, B.W. Inflammation in fetal sheep from intra-amniotic injection of Ureaplasma parvum. Am. J. Physiol. Lung Cell Mol. Physiol. 2010, 299, L852–L860. [Google Scholar] [CrossRef] [PubMed]
- Kallapur, S.G.; Kramer, B.W.; Jobe, A.H. Ureaplasma and BPD. Semin. Perinatol. 2013, 37, 94–101. [Google Scholar] [CrossRef] [PubMed]
- Thébaud, B. Preempting Bronchopulmonary Dysplasia: Time to Focus on the Placenta? Am. J. Respir. Cell Mol. Biol. 2022, 66, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Baker, C.D.; Abman, S.H. Impaired pulmonary vascular development in bronchopulmonary dysplasia. Neonatology 2015, 107, 344–351. [Google Scholar] [CrossRef]
- Villamor-Martinez, E.; Álvarez-Fuente, M.; Ghazi, A.M.; Degraeuwe, P.; Zimmermann, L.J.; Kramer, B.W.; Villamor, E. Association of chorioamnionitis with bronchopulmonary dysplasia among preterm infants: A systematic review, meta-analysis, and metaregression. JAMA Netw. Open 2019, 2, e1914611. [Google Scholar] [CrossRef] [PubMed]
- Pierro, M.; Villamor-Martinez, E.; van Westering-Kroon, E.; Alvarez-Fuente, M.; Abman, S.H.; Villamor, E. Association of the dysfunctional placentation endotype of prematurity with bronchopulmonary dysplasia: A systematic review, meta-analysis and meta-regression. Thorax 2022, 77, 268–275. [Google Scholar] [CrossRef]
- Travers, C.P.; Carlo, W.A.; McDonald, S.A.; Das, A.; Bell, E.F.; Ambalavanan, N.; Jobe, A.H.; Goldberg, R.N.; D’Angio, C.T.; Stoll, B.J. Mortality and pulmonary outcomes of extremely preterm infants exposed to antenatal corticosteroids. Am. J. Obstet. Gynecol. 2018, 218, 130.e1–130.e13. [Google Scholar] [CrossRef]
- Lee, R.; Williams, E.E.; Dassios, T.; Greenough, A. Influence of antenatal corticosteroids and sex on the mortality and morbidity of extremely prematurely born infants. J. Matern. Fetal Neonat. Med. 2021, 1–4. [Google Scholar] [CrossRef]
- Van Westering-Kroon, E.; Huizing, M.J.; Villamor-Martínez, E.; Villamor, E. Male Disadvantage in Oxidative Stress-Associated Complications of Prematurity: A Systematic Review, Meta-Analysis and Meta-Regression. Antioxidants 2021, 10, 1490. [Google Scholar] [CrossRef] [PubMed]
- Logan, J.W.; Lynch, S.K.; Curtiss, J.; Shepherd, E.G. Clinical phenotypes and management concepts for severe, established bronchopulmonary dysplasia. Paediatr. Respir. Rev. 2019, 31, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, E.G.; Clouse, B.J.; Hasenstab, K.A.; Sitaram, S.; Malleske, D.T.; Nelin, L.D.; Jadcherla, S.R. Infant pulmonary function testing and phenotypes in severe bronchopulmonary dysplasia. Pediatrics 2018, 141, e20173350. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.Y.; Jensen, E.A.; White, A.M.; Wang, Y.; Biko, D.M.; Nilan, K.; Fraga, M.V.; Mercer-Rosa, L.; Zhang, H.; Kirpalani, H. Characterization of Disease Phenotype in Very Preterm Infants with Severe Bronchopulmonary Dysplasia. Am. J. Respir. Crit. Care Med. 2020, 201, 1398–1406. [Google Scholar] [CrossRef]
- Arjaans, S.; Zwart, E.A.H.; Ploegstra, M.J.; Bos, A.F.; Kooi, E.M.W.; Hillege, H.L.; Berger, R.M.F. Identification of gaps in the current knowledge on pulmonary hypertension in extremely preterm infants: A systematic review and meta-analysis. Paediatr. Perinat. Epidemiol. 2018, 32, 258–267. [Google Scholar] [CrossRef]
- Lagatta, J.M.; Hysinger, E.B.; Zaniletti, I.; Wymore, E.M.; Vyas-Read, S.; Yallapragada, S.; Nelin, L.D.; Truog, W.E.; Padula, M.A.; Porta, N.F.M.; et al. The Impact of Pulmonary Hypertension in Preterm Infants with Severe Bronchopulmonary Dysplasia through 1 Year. J. Pediatr. 2018, 203, 218–224. [Google Scholar] [CrossRef]
- Coalson, J.J. Pathology of bronchopulmonary dysplasia. Semin. Perinatol. 2006, 30, 179–184. [Google Scholar] [CrossRef]
- Thunqvist, P.; Tufvesson, E.; Bjermer, L.; Winberg, A.; Fellman, V.; Domellöf, M.; Melén, E.; Norman, M.; Hallberg, J. Lung function after extremely preterm birth-A population-based cohort study (EXPRESS). Pediatric Pulmonol. 2018, 53, 64–72. [Google Scholar] [CrossRef]
- Bourbon, J.R.; Boucherat, O.; Boczkowski, J.; Crestani, B.; Delacourt, C. Bronchopulmonary dysplasia and emphysema: In search of common therapeutic targets. Trends Mol. Med. 2009, 15, 169–179. [Google Scholar] [CrossRef]
- McGrath-Morrow, S.A.; Collaco, J.M. Bronchopulmonary dysplasia: What are its links to COPD? Ther. Adv. Respir. Dis. 2019, 13, 1753466619892492. [Google Scholar] [CrossRef]
- Ochiai, M.; Hikino, S.; Yabuuchi, H.; Nakayama, H.; Sato, K.; Ohga, S.; Hara, T. A new scoring system for computed tomography of the chest for assessing the clinical status of bronchopulmonary dysplasia. J. Pediatr. 2008, 152, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Oppenheim, C.; Mamou-Mani, T.; Sayegh, N.; de Blic, J.; Scheinmann, P.; Lallemand, D. Bronchopulmonary dysplasia: Value of CT in identifying pulmonary sequelae. AJR Am. J. Roentgenol. 1994, 163, 169–172. [Google Scholar] [CrossRef] [PubMed]
- Mahut, B.; De Blic, J.; Emond, S.; Benoist, M.R.; Jarreau, P.H.; Lacaze-Masmonteil, T.; Magny, J.F.; Delacourt, C. Chest computed tomography findings in bronchopulmonary dysplasia and correlation with lung function. Arch. Dis. Child. Fetal Neonatal Ed. 2007, 92, F459–F464. [Google Scholar] [CrossRef] [PubMed]
- Van Mastrigt, E.; Logie, K.; Ciet, P.; Reiss, I.K.; Duijts, L.; Pijnenburg, M.W.; Tiddens, H.A. Lung CT imaging in patients with bronchopulmonary dysplasia: A systematic review. Pediatric Pulmonol. 2016, 51, 975–986. [Google Scholar] [CrossRef]
- Henningfeld, J.K.; Maletta, K.; Ren, B.; Richards, K.L.; Wegner, C.; D’Andrea, L.A. Liberation from home mechanical ventilation and decannulation in children. Pediatric Pulmonol. 2016, 51, 838–849. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.; McGrath-Morrow, S.A.; Collaco, J.M. Oxygen weaning after hospital discharge in children with bronchopulmonary dysplasia. Pediatric Pulmonol. 2016, 51, 1206–1211. [Google Scholar] [CrossRef] [PubMed]
- Clemm, H.H.; Vollsæter, M.; Røksund, O.D.; Eide, G.E.; Markestad, T.; Halvorsen, T. Exercise capacity after extremely preterm birth. Development from adolescence to adulthood. Ann. Am. Thorac. Soc. 2014, 11, 537–545. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E. Adult survivors of preterm birth. What spirometry conceals, exercise tests reveal. Ann. Am. Thorac. Soc. 2014, 11, 1606–1607. [Google Scholar] [CrossRef]
- MacLean, J.E.; DeHaan, K.; Fuhr, D.; Hariharan, S.; Kamstra, B.; Hendson, L.; Adatia, I.; Majaesic, C.; Lovering, A.T.; Thompson, R.B.; et al. Altered breathing mechanics and ventilatory response during exercise in children born extremely preterm. Thorax 2016, 71, 1012–1019. [Google Scholar] [CrossRef]
- Collaco, J.M.; McGrath-Morrow, S.A. Respiratory Phenotypes for Preterm Infants, Children, and Adults: Bronchopulmonary Dysplasia and More. Ann. Am. Thorac. Soc. 2018, 15, 530–538. [Google Scholar] [CrossRef]
- Baraldi, E.; Bonetto, G.; Zacchello, F.; Filippone, M. Low exhaled nitric oxide in school-age children with bronchopulmonary dysplasia and airflow limitation. Am. J. Respir. Crit. Care Med. 2005, 171, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Martinez, F.D. Early-Life Origins of Chronic Obstructive Pulmonary Disease. N. Engl. J. Med. 2016, 375, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Fabbri, L.M.; Hurd, S.S. Global Strategy for the Diagnosis, Management and Prevention of COPD: 2003 update. Eur. Respir. J. 2003, 22, 1–2. [Google Scholar] [CrossRef]
- Friedlander, A.L.; Lynch, D.; Dyar, L.A.; Bowler, R.P. Phenotypes of chronic obstructive pulmonary disease. COPD 2007, 4, 355–384. [Google Scholar] [CrossRef] [PubMed]
- Semple, T.; Akhtar, M.R.; Owens, C.M. Imaging Bronchopulmonary Dysplasia-A Multimodality Update. Front. Med. 2017, 4, 88. [Google Scholar] [CrossRef] [PubMed]
- Su, Y.T.; Chiu, C.C.; Lai, S.H.; Hsia, S.H.; Lin, J.J.; Chan, O.W.; Chiu, C.Y.; Tseng, P.L.; Lee, E.P. Risk Factors for Tracheobronchomalacia in Preterm Infants with Bronchopulmonary Dysplasia. Front. Pediatr. 2021, 9, 697470. [Google Scholar] [CrossRef]
- Hysinger, E.B.; Panitch, H.B. Paediatric Tracheomalacia. Paediatric Respir. Rev. 2016, 17, 9–15. [Google Scholar] [CrossRef]
- Deoras, K.S.; Wolfson, M.R.; Searls, R.L.; Hilfer, S.R.; Shaffer, T.H. Developmental changes in tracheal structure. Pediatric Res. 1991, 30, 170–175. [Google Scholar] [CrossRef]
- Tan, J.Z.; Ditchfield, M.; Freezer, N. Tracheobronchomalacia in children: Review of diagnosis and definition. Pediatr. Radiol. 2012, 42, 906–915; quiz 1027–1028. [Google Scholar] [CrossRef] [PubMed]
- Austin, J.; Ali, T. Tracheomalacia and bronchomalacia in children: Pathophysiology, assessment, treatment and anaesthesia management. Paediatr. Anaesth. 2003, 13, 3–11. [Google Scholar] [CrossRef]
- Napolitano, N.; Jalal, K.; McDonough, J.M.; Monk, H.M.; Zhang, H.; Jensen, E.; Dysart, K.C.; Kirpalani, H.M.; Panitch, H.B. Identifying and treating intrinsic PEEP in infants with severe bronchopulmonary dysplasia. Pediatric Pulmonol. 2019, 54, 1045–1051. [Google Scholar] [CrossRef]
- Greenholz, S.K.; Hall, R.J.; Lilly, J.R.; Shikes, R.H. Surgical implications of bronchopulmonary dysplasia. J. Pediatric Surg. 1987, 22, 1132–1136. [Google Scholar] [CrossRef]
- Carden, K.A.; Boiselle, P.M.; Waltz, D.A.; Ernst, A. Tracheomalacia and tracheobronchomalacia in children and adults: An in-depth review. Chest 2005, 127, 984–1005. [Google Scholar] [CrossRef]
- Mok, Q.; Negus, S.; McLaren, C.A.; Rajka, T.; Elliott, M.J.; Roebuck, D.J.; McHugh, K. Computed tomography versus bronchography in the diagnosis and management of tracheobronchomalacia in ventilator dependent infants. Arch. Dis. Child. Fetal Neonatal Ed. 2005, 90, F290–F293. [Google Scholar] [CrossRef]
- Hysinger, E.B.; Friedman, N.L.; Padula, M.A.; Shinohara, R.T.; Zhang, H.; Panitch, H.B.; Kawut, S.M. Tracheobronchomalacia Is Associated with Increased Morbidity in Bronchopulmonary Dysplasia. Ann. Am. Thorac. Soc. 2017, 14, 1428–1435. [Google Scholar] [CrossRef]
- Kamran, A.; Zendejas, B.; Jennings, R.W. Current concepts in tracheobronchomalacia: Diagnosis and treatment. Semin. Pediatric Surg. 2021, 30, 151062. [Google Scholar] [CrossRef]
- Deutsch, G.H. Chapter 2—Histologic Phenotypes of Bronchopulmonary Dysplasia and Childhood Interstitial and Diffuse Lung Disease. In Updates on Neonatal Chronic Lung Disease; Kallapur, S.G., Pryhuber, G.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 13–31. [Google Scholar]
- Nogee, L.M. Interstitial lung disease in newborns. Semin. Fetal. Neonatal. Med. 2017, 22, 227–233. [Google Scholar] [CrossRef]
- Thacker, P.G.; Vargas, S.O.; Fishman, M.P.; Casey, A.M.; Lee, E.Y. Current Update on Interstitial Lung Disease of Infancy: New Classification System, Diagnostic Evaluation, Imaging Algorithms, Imaging Findings, and Prognosis. Radiol. Clin. N. Am. 2016, 54, 1065–1076. [Google Scholar] [CrossRef] [PubMed]
- Dishop, M.K. Diagnostic Pathology of Diffuse Lung Disease in Children. Pediatric Allergy Immunol. Pulmonol. 2010, 23, 69–85. [Google Scholar] [CrossRef]
- Semple, T.R.; Ashworth, M.T.; Owens, C.M. Interstitial Lung Disease in Children Made Easier…Well, Almost. Radiographics 2017, 37, 1679–1703. [Google Scholar] [CrossRef]
- Jang, H.J.; Yong, S.H.; Leem, A.Y.; Lee, S.H.; Kim, S.Y.; Lee, S.H.; Kim, E.Y.; Chung, K.S.; Jung, J.Y.; Kang, Y.A.; et al. Corticosteroid responsiveness in patients with acute exacerbation of interstitial lung disease admitted to the emergency department. Sci. Rep. 2021, 11, 5762. [Google Scholar] [CrossRef]
- Connors, J.; Gibbs, K. Bronchopulmonary Dysplasia: A Multidisciplinary Approach to Management. Curr. Pediatr. Rep. 2019, 7, 83–89. [Google Scholar] [CrossRef]
- Nugent, K.; Dobbe, L.; Rahman, R.; Elmassry, M.; Paz, P. Lung morphology and surfactant function in cardiogenic pulmonary edema: A narrative review. J. Thorac. Dis. 2019, 11, 4031–4038. [Google Scholar] [CrossRef]
- Shah, A.B.; Hashmi, S.S.; Sahulee, R.; Pannu, H.; Gupta-Malhotra, M. Characteristics of systemic hypertension in preterm children. J. Clin. Hypertens. 2015, 17, 364–370. [Google Scholar] [CrossRef]
- Stewart, A.; Brion, L.P. Intravenous or enteral loop diuretics for preterm infants with (or developing) chronic lung disease. Cochrane Database Syst. Rev. 2011, 2011, CD001453. [Google Scholar] [CrossRef]
- Bhatt, A.J.; Pryhuber, G.S.; Huyck, H.; Watkins, R.H.; Metlay, L.A.; Maniscalco, W.M. Disrupted pulmonary vasculature and decreased vascular endothelial growth factor, Flt-1, and TIE-2 in human infants dying with bronchopulmonary dysplasia. Am. J. Respir. Crit. Care Med. 2001, 164, 1971–1980. [Google Scholar] [CrossRef]
- Stenmark, K.R.; Abman, S.H. Lung vascular development: Implications for the pathogenesis of bronchopulmonary dysplasia. Annu. Rev. Physiol. 2005, 67, 623–661. [Google Scholar] [CrossRef]
- Alvira, C.M. Aberrant Pulmonary Vascular Growth and Remodeling in Bronchopulmonary Dysplasia. Front. Med. 2016, 3, 21. [Google Scholar] [CrossRef]
- Sheth, S.; Goto, L.; Bhandari, V.; Abraham, B.; Mowes, A. Factors associated with development of early and late pulmonary hypertension in preterm infants with bronchopulmonary dysplasia. J. Perinatol. 2020, 40, 138–148. [Google Scholar] [CrossRef]
- Kim, H.H.; Sung, S.I.; Yang, M.S.; Han, Y.S.; Kim, H.S.; Ahn, S.Y.; Jeon, G.W.; Chang, Y.S.; Park, W.S. Early pulmonary hypertension is a risk factor for bronchopulmonary dysplasia-associated late pulmonary hypertension in extremely preterm infants. Sci. Rep. 2021, 11, 11206. [Google Scholar] [CrossRef]
- An, H.S.; Bae, E.J.; Kim, G.B.; Kwon, B.S.; Beak, J.S.; Kim, E.K.; Kim, H.S.; Choi, J.H.; Noh, C.I.; Yun, Y.S. Pulmonary hypertension in preterm infants with bronchopulmonary dysplasia. Korean Circ. J. 2010, 40, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, J.L.; Pakrashi, T.; Jones, D.E.; South, A.P.; Shah, T.A. Echocardiographic detection of pulmonary hypertension in extremely low birth weight infants with bronchopulmonary dysplasia requiring prolonged positive pressure ventilation. J. Perinatol. 2011, 31, 635–640. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.H.; Kim, H.S.; Choi, C.W.; Kim, E.K.; Kim, B.I.; Choi, J.H. Risk factors for pulmonary artery hypertension in preterm infants with moderate or severe bronchopulmonary dysplasia. Neonatology 2012, 101, 40–46. [Google Scholar] [CrossRef] [PubMed]
- Arattu Thodika, F.M.S.; Nanjundappa, M.; Dassios, T.; Bell, A.; Greenough, A. Pulmonary hypertension in infants with bronchopulmonary dysplasia: Risk factors, mortality and duration of hospitalisation. J. Perinat. Med. 2021, 50, 327–333. [Google Scholar] [CrossRef] [PubMed]
- Hansmann, G.; Sallmon, H.; Roehr, C.C.; Kourembanas, S.; Austin, E.D.; Koestenberger, M. Pulmonary hypertension in bronchopulmonary dysplasia. Pediatric Res. 2021, 89, 446–455. [Google Scholar] [CrossRef]
- Swier, N.L.; Richards, B.; Cua, C.L.; Lynch, S.K.; Yin, H.; Nelin, L.D.; Smith, C.V.; Backes, C.H. Pulmonary vein stenosis in neonates with severe bronchopulmonary dysplasia. Am. J. Perinatol. 2016, 33, 671–677. [Google Scholar] [CrossRef]
- Mahgoub, L.; Kaddoura, T.; Kameny, A.R.; Lopez Ortego, P.; Vanderlaan, R.D.; Kakadekar, A.; Dicke, F.; Rebeyka, I.; Calderone, C.A.; Redington, A. Pulmonary vein stenosis of ex-premature infants with pulmonary hypertension and bronchopulmonary dysplasia, epidemiology, and survival from a multicenter cohort. Pediatric Pulmonol. 2017, 52, 1063–1070. [Google Scholar] [CrossRef]
- Del Cerro, M.J.; Sabaté Rotés, A.; Cartón, A.; Deiros, L.; Bret, M.; Cordeiro, M.; Verdú, C.; Barrios, M.I.; Albajara, L.; Gutierrez-Larraya, F. Pulmonary hypertension in bronchopulmonary dysplasia: Clinical findings, cardiovascular anomalies and outcomes. Pediatric Pulmonol. 2014, 49, 49–59. [Google Scholar] [CrossRef]
- Collaco, J.M.; Romer, L.H.; Stuart, B.D.; Coulson, J.D.; Everett, A.D.; Lawson, E.E.; Brenner, J.I.; Brown, A.T.; Nies, M.K.; Sekar, P.; et al. Frontiers in pulmonary hypertension in infants and children with bronchopulmonary dysplasia. Pediatr. Pulmonol. 2012, 47, 1042–1053. [Google Scholar] [CrossRef]
- Abman, S.H. Bronchopulmonary Dysplasia: “A Vascular Hypothesis”. Am. J. Respir. Crit. Care Med. 2001, 164, 1755–1756. [Google Scholar] [CrossRef]
- Thébaud, B.; Abman, S.H. Bronchopulmonary dysplasia: Where have all the vessels gone? Roles of angiogenic growth factors in chronic lung disease. Am. J. Respir. Crit. Care Med. 2007, 175, 978–985. [Google Scholar] [CrossRef] [PubMed]
- Soldati, G.; Demi, M.; Demi, L. Ultrasound patterns of pulmonary edema. Ann. Transl. Med. 2019, 7, S16. [Google Scholar] [CrossRef] [PubMed]
- Abiramalatha, T.; Ramaswamy, V.V.; Bandyopadhyay, T.; Somanath, S.H.; Shaik, N.B.; Pullattayil, A.K.; Weiner, G.M. Interventions to Prevent Bronchopulmonary Dysplasia in Preterm Neonates: An Umbrella Review of Systematic Reviews and Meta-analyses. JAMA Pediatr. 2022. [Google Scholar] [CrossRef]
- Morty, R.E. Using experimental models to identify pathogenic pathways and putative disease management targets in bronchopulmonary dysplasia. Neonatology 2020, 117, 233–239. [Google Scholar] [CrossRef]
- Buczynski, B.W.; Maduekwe, E.T.; O’Reilly, M.A. The role of hyperoxia in the pathogenesis of experimental BPD. Semin. Perinatol. 2013, 37, 69–78. [Google Scholar] [CrossRef]
- Kinsella, J.P.; Cutter, G.R.; Steinhorn, R.H.; Nelin, L.D.; Walsh, W.F.; Finer, N.N.; Abman, S.H. Noninvasive inhaled nitric oxide does not prevent bronchopulmonary dysplasia in premature newborns. J. Pediatr. 2014, 165, 1104–1108.e1. [Google Scholar] [CrossRef]
- Taglauer, E.S.; Fernandez-Gonzalez, A.; Willis, G.R.; Reis, M.; Yeung, V.; Liu, X.; Prince, L.S.; Mitsialis, S.A.; Kourembanas, S. Antenatal mesenchymal stromal cell extracellular vesicle therapy prevents preeclamptic lung injury in mice. Am. J. Respir. Cell Mol. Biol. 2022, 66, 86–95. [Google Scholar] [CrossRef]
- Di Cicco, M.; Tozzi, M.G.; Ragazzo, V.; Peroni, D.; Kantar, A. Chronic respiratory diseases other than asthma in children: The COVID-19 tsunami. Ital. J. Pediatr. 2021, 47, 220. [Google Scholar] [CrossRef]
- Woodruff, R.C.; Campbell, A.P.; Taylor, C.A.; Chai, S.J.; Kawasaki, B.; Meek, J.; Anderson, E.J.; Weigel, A.; Monroe, M.L.; Reeg, L. Risk factors for severe COVID-19 in children. Pediatrics 2022, 149, e137–e145. [Google Scholar] [CrossRef]
- Sotgiu, G.; Dobler, C.C. Social stigma in the time of coronavirus disease 2019. Eur. Resp. J. 2020, 56, 2002461. [Google Scholar] [CrossRef]
- Cahal, M.; Amirav, I.; Diamant, N.; Be’er, M.; Besor, O.; Lavie, M. Real-time effects of COVID-19 pandemic lockdown on pediatric respiratory patients. Pediatric Pulmonol. 2021, 56, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Peroni, D.G.; Trambusti, I.; Di Cicco, M.E.; Nuzzi, G. Vitamin D in pediatric health and disease. Pediatric Allergy Immunol. 2020, 31, 54–57. [Google Scholar] [CrossRef] [PubMed]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pierro, M.; Van Mechelen, K.; van Westering-Kroon, E.; Villamor-Martínez, E.; Villamor, E. Endotypes of Prematurity and Phenotypes of Bronchopulmonary Dysplasia: Toward Personalized Neonatology. J. Pers. Med. 2022, 12, 687. https://doi.org/10.3390/jpm12050687
Pierro M, Van Mechelen K, van Westering-Kroon E, Villamor-Martínez E, Villamor E. Endotypes of Prematurity and Phenotypes of Bronchopulmonary Dysplasia: Toward Personalized Neonatology. Journal of Personalized Medicine. 2022; 12(5):687. https://doi.org/10.3390/jpm12050687
Chicago/Turabian StylePierro, Maria, Karen Van Mechelen, Elke van Westering-Kroon, Eduardo Villamor-Martínez, and Eduardo Villamor. 2022. "Endotypes of Prematurity and Phenotypes of Bronchopulmonary Dysplasia: Toward Personalized Neonatology" Journal of Personalized Medicine 12, no. 5: 687. https://doi.org/10.3390/jpm12050687
APA StylePierro, M., Van Mechelen, K., van Westering-Kroon, E., Villamor-Martínez, E., & Villamor, E. (2022). Endotypes of Prematurity and Phenotypes of Bronchopulmonary Dysplasia: Toward Personalized Neonatology. Journal of Personalized Medicine, 12(5), 687. https://doi.org/10.3390/jpm12050687