
Clinical Efficacy of Adjuvant Chemotherapy in Advanced Upper Tract Urothelial Carcinoma (pT3-T4): Real-World Data from the Taiwan Upper Tract Urothelial Carcinoma Collaboration Group

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
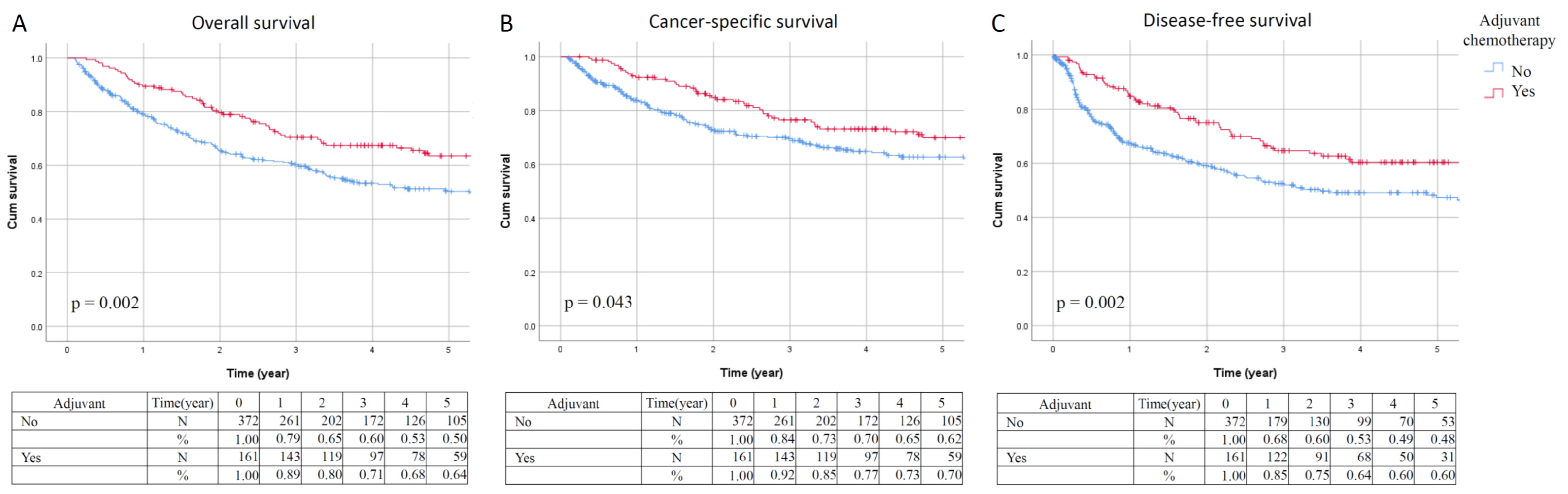
3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soria, F.; Shariat, S.F.; Lerner, S.P.; Fritsche, H.-M.; Rink, M.; Kassouf, W.; Spiess, P.E.; Lotan, Y.; Ye, D.; Fernandez, I.M.; et al. Epidemiology, diagnosis, preoperative evaluation and prognostic assessment of upper-tract urothelial carcinoma (UTUC). World J. Urol. 2017, 35, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Rouprêt, M.; Babjuk, M.; Burger, M.; Capoun, O.; Cohen, D.; Compérat, E.M.; Cowan, N.C.; Dominguez-Escrig, J.L.; Gontero, P.; Mostafid, A.H.; et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2020 Update. Eur. Urol. 2020, 79, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Chou, Y.H.; Huang, C.H. Unusual clinical presentation of upper urothelial carcinoma in Taiwan. Cancer 1999, 85, 1342–1344. [Google Scholar] [CrossRef]
- Li, C.-C.; Chang, T.-H.; Wu, W.-J.; Ke, H.-L.; Huang, S.-P.; Tsai, P.-C.; Chang, S.-J.; Shen, J.-T.; Chou, Y.-H.; Huang, C.-H. Significant Predictive Factors for Prognosis of Primary Upper Urinary Tract Cancer after Radical Nephroureterectomy in Taiwanese Patients. Eur. Urol. 2008, 54, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Li, W.-M.; Shen, J.-T.; Li, C.-C.; Ke, H.-L.; Wei, Y.-C.; Wu, W.J.; Chou, Y.-H.; Huang, C.-H. Oncologic Outcomes Following Three Different Approaches to the Distal Ureter and Bladder Cuff in Nephroureterectomy for Primary Upper Urinary Tract Urothelial Carcinoma. Eur. Urol. 2010, 57, 963–969. [Google Scholar] [CrossRef] [PubMed]
- Colin, P.; Koenig, P.; Ouzzane, A.; Berthon, N.; Villers, A.; Biserte, J.; Rouprêt, M. Environmental factors involved in carcinogenesis of urothelial cell carcinomas of the upper urinary tract. Br. J. Urol. 2009, 104, 1436–1440. [Google Scholar] [CrossRef]
- Wang, Y.-H.; Yeh, S.-D.; Shen, K.-H.; Shen, C.-H.; Juang, G.-D.; Hsu, L.-I.; Chiou, H.-Y.; Chen, C.-J. A significantly joint effect between arsenic and occupational exposures and risk genotypes/diplotypes of CYP2E1, GSTO1 and GSTO2 on risk of urothelial carcinoma. Toxicol. Appl. Pharmacol. 2009, 241, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Margulis, V.; Shariat, S.F.; Matin, S.F.; Kamat, A.M.; Zigeuner, R.; Kikuchi, E.; Lotan, Y.; Weizer, A.; Raman, J.; Wood, C.G.; et al. Outcomes of radical nephroureterectomy: A series from the Upper Tract Urothelial Carcinoma Collaboration. Cancer 2009, 115, 1224–1233. [Google Scholar] [CrossRef]
- Abouassaly, R.; Alibhai, S.; Shah, N.; Timilshina, N.; Fleshner, N.; Finelli, A. Troubling Outcomes From Population-level Analysis of Surgery for Upper Tract Urothelial Carcinoma. Urology 2010, 76, 895–901. [Google Scholar] [CrossRef]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Espinós, E.L.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Flaig, T.W.; Spiess, P.E.; Agarwal, N.; Bangs, R.; Boorjian, S.A.; Buyyounouski, M.K.; Chang, S.; Downs, T.M.; Efstathiou, J.A.; Friedlander, T.; et al. Bladder Cancer, Version 3.2020, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2020, 18, 329–354. [Google Scholar] [CrossRef] [Green Version]
- Birtle, A.; Johnson, M.; Chester, J.; Jones, R.; Dolling, D.; Bryan, R.; Harris, C.; Winterbottom, A.; Blacker, A.; Catto, J.W.F.; et al. Adjuvant chemotherapy in upper tract urothelial carcinoma (the POUT trial): A phase 3, open-label, randomised controlled trial. Lancet 2020, 395, 1268–1277. [Google Scholar] [CrossRef]
- Nakagawa, T.; Komemushi, Y.; Kawai, T.; Otsuka, M.; Miyakawa, J.; Uemura, Y.; Kanatani, A.; Taguchi, S.; Naito, A.; Suzuki, M.; et al. Efficacy of post-nephroureterectomy cisplatin-based adjuvant chemotherapy for locally advanced upper tract urothelial carcinoma: A multi-institutional retrospective study. World J. Urol. 2017, 35, 1569–1575. [Google Scholar] [CrossRef]
- Chang, Y.; Hsiao, P.; Chen, G.; Lin, C.; Chang, C.; Wu, H.; Huang, C.; Yang, C.; Yeh, S. Outcomes of stage II-IV upper-tract urothelial carcinoma and adjuvant chemotherapy for locally advanced cancer. Oncol. Lett. 2018, 17, 1341–1348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Necchi, A.; Vullo, S.L.; Mariani, L.; Moschini, M.; Hendricksen, K.; Rink, M.; Sosnowski, R.; Dobruch, J.; Raman, J.D.; Wood, C.G.; et al. Adjuvant chemotherapy after radical nephroureterectomy does not improve survival in patients with upper tract urothelial carcinoma: A joint study by the European Association of Urology-Young Academic Urologists and the Upper Tract Urothelial Carcinoma Col. Br. J. Urol. 2018, 121, 252–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vassilakopoulou, M.; Rouge, T.D.L.M.; Colin, P.; Ouzzane, A.; Khayat, D.; Dimopoulos, M.; Papadimitriou, C.A.; Bamias, A.; Pignot, G.; Nouhaud, F.X.; et al. Outcomes after adjuvant chemotherapy in the treatment of high-risk urothelial carcinoma of the upper urinary tract (UUT-UC). Cancer 2011, 117, 5500–5508. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Matsumoto, K.; Hirayama, T.; Koguchi, D.; Murakami, Y.; Matsuda, D.; Okuno, N.; Utsunomiya, T.; Taoka, Y.; Irie, A.; et al. Oncologic Outcomes of Salvage Chemotherapy in Patients with Recurrent or Metastatic Lesions after Radical Nephroureterectomy: A Multi-Institutional Retrospective Study. Chemotherapy 2020, 65, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Ho, G.Y.; Woodward, N.; Coward, J.I. Cisplatin versus carboplatin: Comparative review of therapeutic management in solid malignancies. Crit. Rev. Oncol. 2016, 102, 37–46. [Google Scholar] [CrossRef] [Green Version]
- Leow, J.J.; Martin-Doyle, W.; Fay, A.P.; Choueiri, T.K.; Chang, S.L.; Bellmunt, J. A Systematic Review and Meta-analysis of Adjuvant and Neoadjuvant Chemotherapy for Upper Tract Urothelial Carcinoma. Eur. Urol. 2014, 66, 529–541. [Google Scholar] [CrossRef]
- Miller, R.P.; Tadagavadi, R.K.; Ramesh, G.; Reeves, W.B. Mechanisms of Cisplatin Nephrotoxicity. Toxins 2010, 2, 2490–2518. [Google Scholar] [CrossRef] [Green Version]
- Seisen, T.; Shariat, S.F.; Cussenot, O.; Peyronnet, B.; Renard-Penna, R.; Colin, P.; Rouprêt, M. Contemporary role of lymph node dissection at the time of radical nephroureterectomy for upper tract urothelial carcinoma. World J. Urol. 2017, 35, 535–548. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Escrig, J.L.; Peyronnet, B.; Seisen, T.; Bruins, H.M.; Yuan, Y.; Babjuk, M.; Böhle, A.; Burger, M.; Compérat, E.M.; Gontero, P.; et al. Potential Benefit of Lymph Node Dissection During Radical Nephroureterectomy for Upper Tract Urothelial Carcinoma: A Systematic Review by the European Association of Urology Guidelines Panel on Non–muscle-invasive Bladder Cancer. Eur. Urol. Focus 2019, 5, 224–241. [Google Scholar] [CrossRef] [PubMed]
- Dong, F.; Xu, T.; Wang, X.; Shen, Y.; Zhang, X.; Chen, S.; Zhong, S.; Zhang, M.; Ding, Q. Lymph node dissection could bring survival benefits to patients diagnosed with clinically node-negative upper urinary tract urothelial cancer: A population-based, propensity score-matched study. Int. J. Clin. Oncol. 2018, 24, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Zhai, T.-S.; Jin, L.; Zhou, Z.; Liu, X.; Liu, H.; Chen, W.; Lu, J.-Y.; Yao, X.-D.; Feng, L.-M.; Ye, L. Effect of lymph node dissection on stage-specific survival in patients with upper urinary tract urothelial carcinoma treated with nephroureterectomy. BMC Cancer 2019, 19, 1207. [Google Scholar] [CrossRef] [Green Version]
- Guo, R.; Zhu, Y.; Xiong, G.; Li, X.; Zhang, K.; Zhou, L. Role of lymph node dissection in the management of upper tract urothelial carcinomas: A meta-analysis. BMC Urol. 2018, 18, 24. [Google Scholar] [CrossRef] [Green Version]
- Novara, G.; Matsumoto, K.; Kassouf, W.; Walton, T.J.; Fritsche, H.-M.; Bastian, P.J.; Martínez-Salamanca, J.I.; Seitz, C.; Lemberger, R.J.; Burger, M.; et al. Prognostic Role of Lymphovascular Invasion in Patients with Urothelial Carcinoma of the Upper Urinary Tract: An International Validation Study. Eur. Urol. 2010, 57, 1064–1071. [Google Scholar] [CrossRef]
- Liu, W.; Zhou, Z.; Dong, D.; Sun, L.; Zhang, G. Prognostic Value of Lymphovascular Invasion in Node-Negative Upper Urinary Tract Urothelial Carcinoma Patients Undergoing Radical Nephroureterectomy. Yonsei Med. J. 2019, 60, 174–181. [Google Scholar] [CrossRef]
- Fan, E.W.; Li, C.-C.; Wu, W.J.; Huang, C.-N.; Li, W.-M.; Ke, H.-L.; Yeh, H.-C.; Wu, T.-F.; Liang, P.-I.; Ma, L.-J.; et al. FGF7 Over Expression is an Independent Prognosticator in Patients with Urothelial Carcinoma of the Upper Urinary Tract and Bladder. J. Urol. 2015, 194, 223–229. [Google Scholar] [CrossRef]
- Chen, C.-S.; Lin, C.-Y.; Wang, C.-L.; Wang, S.-S.; Li, J.-R.; Yang, C.-K.; Cheng, C.-L.; Chiu, K.-Y.; Yang, S.-F. Association between lymphovascular invasion and oncological outcome in node-negative upper tract urothelial carcinoma with different stage. Urol. Oncol. Semin. Orig. Investig. 2021, 39, 132.e13–132.e26. [Google Scholar] [CrossRef]
- Galsky, M.D.; Chen, G.J.; Oh, W.; Bellmunt, J.; Roth, B.J.; Petrioli, R.; Dogliotti, L.; Dreicer, R.; Sonpavde, G. Comparative effectiveness of cisplatin-based and carboplatin-based chemotherapy for treatment of advanced urothelial carcinoma. Ann. Oncol. 2012, 23, 406–410. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Variables | Adjuvant Chemotherapy (n = 161) | No Adjuvant Chemotherapy (n = 372) | p-Value | ||
|---|---|---|---|---|---|
| n | (%) | n | (%) | ||
| Sex | |||||
| Male | 80 | (49.7) | 167 | (44.9) | 0.308 |
| Female | 81 | (50.3) | 205 | (55.1) | |
| Age (years) | |||||
| Mean ± SD | 64.3 ± 9.9 | 70.5 ± 11.2 | <0.001 * | ||
| Median | 65.9 | 726 | |||
| BMI (kg/m2) | |||||
| Mean ± SD | 24.5 ± 4.0 | 23.9 ± 3.8 | 0.386 | ||
| Median | 24.1 | 23.8 | |||
| Follow-up (months) | |||||
| Mean ± SE | 60.1 ± 7.6 | 51.2 ± 7.8 | <0.001 * | ||
| Median | 46.8 | 29.0 | |||
| ASA | |||||
| 1 | 2 | (2.0) | 4 | (2.4) | 0.009 * |
| 2 | 51 | (50.0) | 50 | (29.8) | |
| 3 | 49 | (48.0) | 113 | (67.3) | |
| 4 | 0 | (0.0) | 1 | (0.6) | |
| ECOG | |||||
| 0 | 58 | (46.8) | 98 | (41.0) | 0.293 |
| 1 | 55 | (44.4) | 102 | (42.7) | |
| 2 | 10 | (8.1) | 31 | (13.0) | |
| 3 | 1 | (0.8) | 4 | (1.7) | |
| 4 | 0 | (0.0) | 4 | (1.7) | |
| Smoking | |||||
| No | 85 | (72.0) | 182 | (71.7) | 0.940 |
| Yes | 33 | (28.0) | 72 | (28.3) | |
| Tumor location | |||||
| Renal pelvis | 80 | (49.7) | 202 | (54.3) | 0.317 |
| Ureter | 50 | (31.1) | 92 | (24.7) | |
| Renal pelvis + ureter | 31 | (19.3) | 78 | (21.0) | |
| Tumor size | |||||
| <1 cm | 3 | (2.3) | 10 | (3.2) | 0.760 |
| ≥1 and <2 cm | 22 | (16.5) | 39 | (12.7) | |
| ≥2 and <3 cm | 26 | (19.5) | 56 | (18.2) | |
| ≥3 cm | 82 | (61.7) | 203 | (65.9) | |
| Histological variant | |||||
| No | 135 | (83.9) | 322 | (86.6) | 0.412 |
| Yes | 26 | (16.1) | 50 | (13.4) | |
| Tumor grade | |||||
| Low grade | 12 | (7.5) | 15 | (4.1) | 0.098 |
| High grade | 148 | (92.5) | 355 | (95.9) | |
| Multifocality | |||||
| No | 102 | (63.4) | 234 | (62.9) | 0.921 |
| Yes | 59 | (36.6) | 138 | (37.1) | |
| Concurrent CIS | |||||
| No | 141 | (87.6) | 325 | (87.4) | 0.946 |
| Yes | 20 | (12.4) | 47 | (12.6) | |
| Lymphovascular invasion | |||||
| No | 99 | (61.5) | 245 | (65.9) | 0.333 |
| Yes | 62 | (38.5) | 127 | (34.1) | |
| Pathological stage | |||||
| Stage III | 128 | (79.5) | 308 | (83.2) | 0.301 |
| Stage IV | 33 | (83.2) | 62 | (16.7) | |
| Pathological T stage | |||||
| pT3 | 146 | (90.7) | 326 | (87.6) | 0.310 |
| pT4 | 15 | (9.3) | 46 | (12.4) | |
| Pathological N stage | |||||
| pN0 | 38 | (23.6) | 74 | (19.9) | 0.011 * |
| pN1 | 10 | (6.2) | 10 | (2.7) | |
| pN2 | 12 | (7.5) | 10 | (2.7) | |
| pNx | 98 | (60.9) | 272 | (73.1) | |
| Overall Survival | Cancer-Specific Survival | Disease-Free Survival | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Adjuvant chemotherapy | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 0.636 | 0.478–0.847 | 0.002 * | 0.700 | 0.495–0.990 | 0.044 * | 0.624 | 0.459–0.850 | 0.003 * |
| Chemotherapy regimens | |||||||||
| Gemcitabine and cisplatin | 1 | 1 | 1 | ||||||
| MVAC | 1.014 | 0.598–1.718 | 0.960 | 0.847 | 0.475–1.511 | 0.574 | 0.794 | 0.480–1.316 | 0.371 |
| Carboplatin-based | 0.529 | 0.127–2.204 | 0.382 | 0.314 | 0.043–2.296 | 0.254 | 0.482 | 0.116–1.998 | 0.315 |
| Others | 1.215 | 0.774–1.905 | 0.397 | 1.048 | 0.640–1.714 | 0.853 | 1.057 | 0.689–1.624 | 0.799 |
| Sex | |||||||||
| Male | 1 | 1 | 1 | ||||||
| Female | 1.011 | 0.788–1.296 | 0.932 | 1.110 | 0.814–1.515 | 0.509 | 1.119 | 0.851–1.472 | 0.421 |
| Age | |||||||||
| <70 | 1 | 1 | 1 | ||||||
| ≥70 | 1.750 | 1.360–2.253 | <0.001 * | 1.407 | 1.031–1.921 | 0.031 * | 1.280 | 0.971–1.686 | 0.080 |
| BMI | |||||||||
| <24 | 1 | 1 | 1 | ||||||
| ≥24 | 0.896 | 0.647–1.241 | 0.509 | 0.989 | 0.678–1.444 | 0.956 | 0.990 | 0.698–1.402 | 0.953 |
| ASA | |||||||||
| 1 | 1 | 1 | 1 | ||||||
| >1 | 2.527 | 0.352–18.131 | 0.357 | 1.833 | 0.254–13.201 | 0.548 | 1.202 | 0.296–4.885 | 0.797 |
| ECOG | |||||||||
| 0 | 1 | 1 | 1 | ||||||
| ≥1 | 1.115 | 0.805–1.544 | 0.513 | 0.978 | 0.672–1.423 | 0.906 | 1.028 | 0.729–1.449 | 0.876 |
| Smoking | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 1.181 | 0.849–1.643 | 0.323 | 1.482 | 1.005–2.186 | 0.047 * | 1.368 | 0.968–1.934 | 0.076 |
| Hospitals | |||||||||
| Medical centers | 1 | 1 | 1 | ||||||
| Regional hospitals | 1.111 | 0.880–1.403 | 0.376 | 1.166 | 0.882–1.541 | 0.280 | 1.105 | 0.855–1.429 | 0.446 |
| Tumor location | |||||||||
| Renal pelvis | 1 | 1 | 1 | ||||||
| Ureter | 1.134 | 0.848–1.517 | 0.395 | 1.358 | 0.952–1.937 | 0.091 | 1.349 | 0.979–1.858 | 0.067 |
| Renal pelvis + ureter | 1.200 | 0.869–1.657 | 0.267 | 1.214 | 0.808–1.824 | 0.351 | 1.289 | 0.910–1.826 | 0.153 |
| Tumor size | |||||||||
| <3 cm | 1 | 1 | 1 | ||||||
| ≥3 cm | 1.478 | 1.082–2.018 | 0.014 * | 1.898 | 1.281–2.810 | 0.001 * | 1.607 | 1.154–2.240 | 0.005 * |
| Histological variants | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 1.185 | 0.828–1.694 | 0.353 | 1.355 | 0.890–2.063 | 0.156 | 1.105 | 0.754–1.620 | 0.609 |
| Tumor grade | |||||||||
| Low grade | 1 | 1 | 1 | ||||||
| High grade | 2.854 | 1.269–6.421 | 0.011 * | 5.804 | 1.438–23.414 | 0.013 * | 4.212 | 1.565–11.339 | 0.004 * |
| Multifocality | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 1.367 | 1.062–1.758 | 0.015 * | 1.407 | 1.029–1.924 | 0.033 * | 1.390 | 1.053–1.836 | 0.020 * |
| Concurrent CIS | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 1.122 | 0.751–1.676 | 0.575 | 1.125 | 0.696–1.817 | 0.632 | 0.959 | 0.626–1.469 | 0.847 |
| Lymphovascular invasion | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 1.476 | 1.139–1.914 | 0.003 * | 1.672 | 1.223–2.285 | 0.001 * | 1.305 | 0.988–1.725 | 0.061 |
| Pathological T stage | |||||||||
| pT3 | 1 | 1 | 1 | ||||||
| pT4 | 2.723 | 1.980–3.746 | <0.001 * | 3.120 | 2.124–4.583 | <0.001 * | 2.294 | 1.567–3.357 | <0.001 * |
| Pathological N stage | |||||||||
| pN0 + pNx | 1 | 1 | 1 | ||||||
| pN1 + pN2 | 0.474 | 0.313–0.718 | <0.001 * | 0.389 | 0.246–0.617 | <0.001 | 0.410 | 0.269–0.625 | <0.001 * |
| Overall Survival | Cancer-Specific Survival | Disease-Free Survival | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value |
| Adjuvant chemotherapy | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 0.599 | 0.419–0.857 | 0.005 * | 0.598 | 0.391–0.914 | 0.018 * | 0.456 | 0.310–0.673 | <0.001 * |
| Age | |||||||||
| <70 | 1 | 1 | 1 | ||||||
| ≥70 | 1.727 | 1.272–2.346 | <0.001 * | 1.321 | 0.917–1.902 | 0.134 | 1.176 | 0.856–1.616 | 0.317 |
| Tumor size | |||||||||
| <3 cm | 1 | 1 | 1 | ||||||
| ≥3 cm | 1.188 | 0.859–1.643 | 0.299 | 1.473 | 0.974–2.226 | 0.066 | 1.377 | 0.978–1.939 | 0.067 |
| Tumor grade | |||||||||
| Low grade | 1 | 1 | 1 | ||||||
| High grade | 2.526 | 1.033–6.181 | 0.042 * | 8.184 | 1.139–58.824 | 0.037 * | 3.772 | 1.197–11.885 | 0.023 * |
| Multifocality | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 1.274 | 0.951–1.707 | 0.104 | 1.375 | 0.966–1.957 | 0.077 | 1.415 | 1.043–1.920 | 0.026 * |
| Lymphovascular invasion | |||||||||
| No | 1 | 1 | 1 | ||||||
| Yes | 1.258 | 0.935–1.693 | 0.129 | 1.395 | 0.970–2.006 | 0.073 | 1.193 | 0.870–1.635 | 0.274 |
| Pathological T stage | |||||||||
| pT3 | 1 | 1 | 1 | ||||||
| pT4 | 2.390 | 1.588–3.596 | <0.001 * | 2.234 | 1.377–3.627 | 0.001 * | 1.654 | 1.033–2.650 | 0.036 * |
| Pathological N stage | |||||||||
| pN0 + pNx | 1 | 1 | 1 | ||||||
| pN1 + pN2 | 2.234 | 1.397–3.572 | 0.001 * | 2.323 | 1.361–3.963 | 0.002 * | 2.888 | 1.755–4.752 | <0.001 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-Y.; Weng, H.-Y.; Tai, T.-Y.; Wu, H.-C.; Chen, W.-C.; Chen, C.-H.; Huang, C.-Y.; Lo, C.-W.; Yu, C.-C.; Tsai, C.-Y.; et al. Clinical Efficacy of Adjuvant Chemotherapy in Advanced Upper Tract Urothelial Carcinoma (pT3-T4): Real-World Data from the Taiwan Upper Tract Urothelial Carcinoma Collaboration Group. J. Pers. Med. 2022, 12, 226. https://doi.org/10.3390/jpm12020226
Lin C-Y, Weng H-Y, Tai T-Y, Wu H-C, Chen W-C, Chen C-H, Huang C-Y, Lo C-W, Yu C-C, Tsai C-Y, et al. Clinical Efficacy of Adjuvant Chemotherapy in Advanced Upper Tract Urothelial Carcinoma (pT3-T4): Real-World Data from the Taiwan Upper Tract Urothelial Carcinoma Collaboration Group. Journal of Personalized Medicine. 2022; 12(2):226. https://doi.org/10.3390/jpm12020226
Chicago/Turabian StyleLin, Chung-Yu, Han-Yu Weng, Ta-Yao Tai, Hsi-Chin Wu, Wen-Chi Chen, Chung-Hsin Chen, Chao-Yuan Huang, Chi-Wen Lo, Chih-Chin Yu, Chung-You Tsai, and et al. 2022. "Clinical Efficacy of Adjuvant Chemotherapy in Advanced Upper Tract Urothelial Carcinoma (pT3-T4): Real-World Data from the Taiwan Upper Tract Urothelial Carcinoma Collaboration Group" Journal of Personalized Medicine 12, no. 2: 226. https://doi.org/10.3390/jpm12020226
APA StyleLin, C.-Y., Weng, H.-Y., Tai, T.-Y., Wu, H.-C., Chen, W.-C., Chen, C.-H., Huang, C.-Y., Lo, C.-W., Yu, C.-C., Tsai, C.-Y., Wu, W.-C., Jiang, Y.-H., Lee, Y.-K., Hsueh, T. Y., Chiu, A. W., Chiang, B.-J., Huang, H.-C., Chen, I.-H. A., Chen, Y.-T., ... Li, W.-M. (2022). Clinical Efficacy of Adjuvant Chemotherapy in Advanced Upper Tract Urothelial Carcinoma (pT3-T4): Real-World Data from the Taiwan Upper Tract Urothelial Carcinoma Collaboration Group. Journal of Personalized Medicine, 12(2), 226. https://doi.org/10.3390/jpm12020226