

Therapeutic Management and Prognostic Factors for Ovarian Malignant Tumours in Adolescents: A Comprehensive Review of Current Guidelines

 ,
,
Abstract
1. Introduction
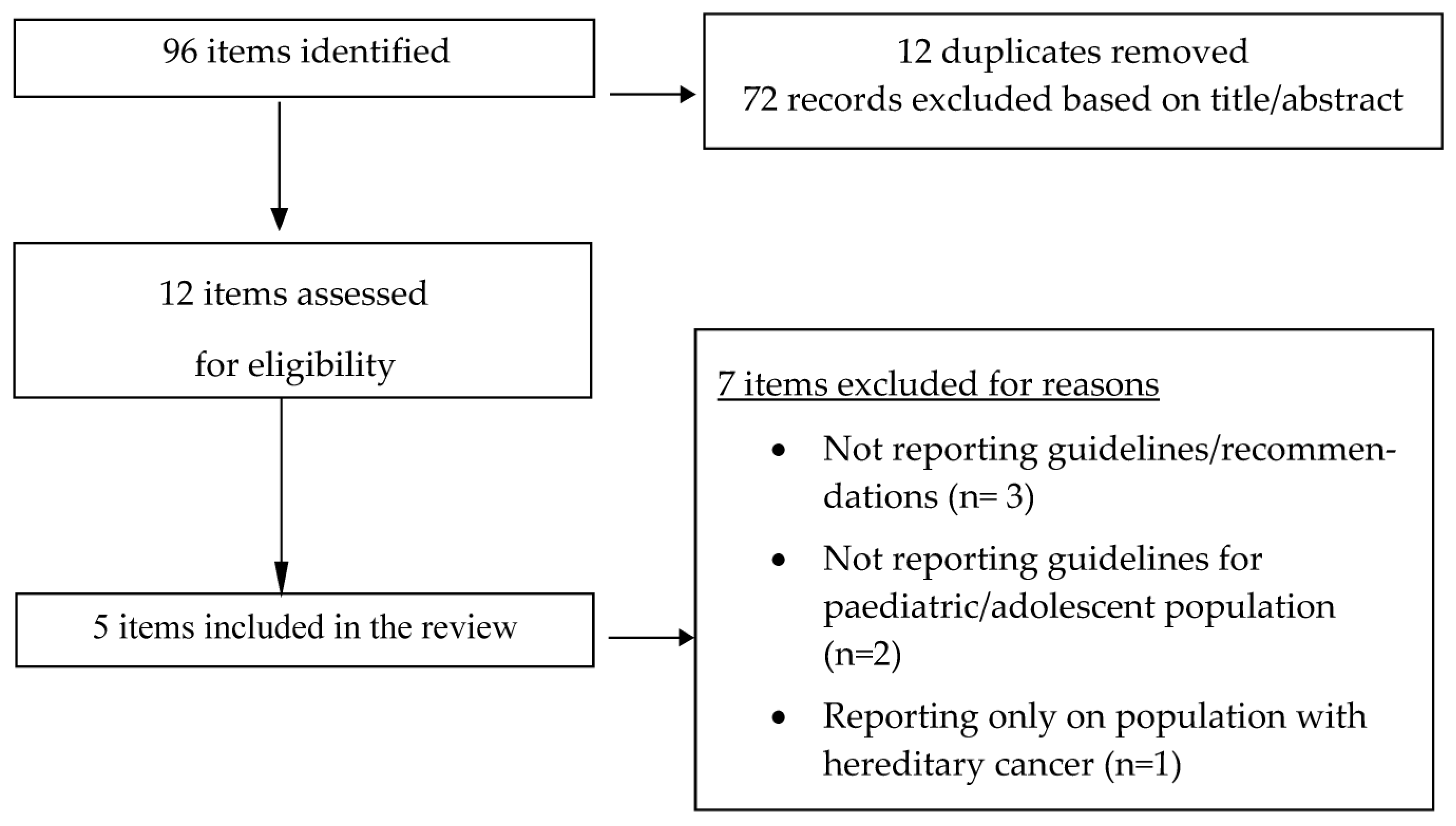
2. Methods
3. Diagnostic Evaluation
4. Pathology and Molecular Biology
5. Assessment of Prognostic Factors
6. Surgical Staging
7. General Principles of Therapeutic Management
8. Germ Cell Tumours (GCTs)
8.1. Early Stages
8.2. Advanced Stages
8.3. Refractory or Recurrent Disease
9. Sex Cord Stromal Tumours (SCSTs)
9.1. Early Stages
9.2. Advanced Stages
9.3. Refractory or Recurrent Disease
10. Small Cell Carcinoma of the Ovary Hypercalcemic Type (SCCOHT)
10.1. Early Stages
10.2. Advanced Stages
10.3. Refractory or Recurrent Disease
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Liu, H.; Wang, X.; Lu, D.; Liu, Z.; Shi, G. Ovarian Masses in Children and Adolescents in China: Analysis of 203 Cases. J. Ovarian Res. 2013, 6, 47. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Jiang, W.; Li, G.; Xu, C. Ovarian Masses in Children and Adolescents—An Analysis of 521 Clinical Cases. J. Pediatr. Adolesc. Gynecol. 2014, 27, e73–e77. [Google Scholar] [CrossRef] [PubMed]
- Rathore, R.; Sharma, S.; Arora, D. Spectrum of Childhood and Adolescent Ovarian Tumors in India: 25 Years Experience at a Single Institution. Open Access Maced. J. Med. Sci. 2016, 4, 551. [Google Scholar] [CrossRef]
- Mahadik, K.; Ghorpade, K. Childhood Ovarian Malignancy. J. Obstet. Gynaecol. India 2014, 64, 91. [Google Scholar] [CrossRef] [PubMed]
- Banlı-Cesur, I.; Tanrıdan-Okcu, N.; Özçelik, Z. Ovarian Masses in Children and Adolescents: Analysis on 146 Patients. J. Gynecol. Obstet. Hum. Reprod. 2021, 50, 101901. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.H.; Kim, J.W.; Shin, S.S.; Jeong, S.I.; Lim, H.S.; Choi, Y.D.; Lee, K.H.; Kang, W.D.; Jeong, Y.Y.; Kang, H.K. Review of Ovarian Tumors in Children and Adolescents: Radiologic-Pathologic Correlation. Radiographics 2014, 34, 2039–2055. [Google Scholar] [CrossRef]
- Shaaban, A.M.; Rezvani, M.; Elsayes, K.M.; Baskin, H.; Mourad, A.; Foster, B.R.; Jarboe, E.A.; Menias, C.O. Ovarian Malignant Germ Cell Tumors: Cellular Classification and Clinical and Imaging Features. Radiographics 2014, 34, 777–801. [Google Scholar] [CrossRef] [PubMed]
- Grigore, M.; Murarasu, M.; Himiniuc, L.M.; Toma, B.F.; Duma, O.; Popovici, R. Large Ovarian Tumors in Adolescents, a Systematic Review of Reported Cases, Diagnostic Findings and Surgical Management. Taiwan. J. Obstet. Gynecol. 2021, 60, 602–608. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Morice, P.; Lorusso, D.; Prat, J.; Oaknin, A.; Pautier, P.; Colombo, N. Non-Epithelial Ovarian Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, iv1–iv18. [Google Scholar] [CrossRef]
- Fonseca, A.; Lindsay Frazier, A.; Shaikh, F. Germ Cell Tumors in Adolescents and Young Adults. J. Oncol. Pract. 2019, 15, 433–441. [Google Scholar] [CrossRef]
- Pierce, J.L.; Frazier, A.L.; Amatruda, J.F. Pediatric Germ Cell Tumors: A Developmental Perspective. Adv. Urol. 2018, 2018, 9059382. [Google Scholar] [CrossRef] [PubMed]
- Gupta, B.; Guleria, K.; Suneja, A.; Vaid, N.B.; Rajaram, S.; Wadhwa, N. Adolescent Ovarian Masses: A Retrospective Analysis. J. Obstet. Gynaecol. 2016, 36, 515–517. [Google Scholar] [CrossRef] [PubMed]
- Herrington, C.S.; Editorial Board. WHO Classification of Tumours. Tumours of the Ovary (Chapter 1). In WHO Classification of Tumours of Female Reproductive Organs, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2020; pp. 93–143. [Google Scholar]
- Alaggio, R.; Hill, D.A.; Jacques, T.S.; Jarzembowski, J.A.; López-Terrada, D.H.; Pfister, S.M. WHO Classification of Tumors: Pediatric Tumors, 1st ed.; International Agency for Research on Cancer: Lyon, France, 2021. [Google Scholar]
- Baert, T.; Storme, N.; Van Nieuwenhuysen, E.; Uyttebroeck, A.; Van Damme, N.; Vergote, I.; Coosemans, A. Ovarian Cancer in Children and Adolescents: A Rare Disease That Needs More Attention. Maturitas 2016, 88, 3–8. [Google Scholar] [CrossRef] [PubMed]
- Tarca, E.; Trandafir, L.M.; Cojocaru, E.; Costea, C.F.; Rosu, S.T.; Butnariu, L.I.; Iordache, A.C.; Munteanu, V.; Luca, A.C. Diagnosis Difficulties and Minimally Invasive Treatment for Ovarian Masses in Adolescents. Int. J. Women’s Health 2022, 14, 1047. [Google Scholar] [CrossRef]
- Takayasu, H.; Masumoto, K.; Tanaka, N.; Aiyoshi, T.; Sasaki, T.; Ono, K.; Chiba, F.; Urita, Y.; Shinkai, T. A Clinical Review of Ovarian Tumors in Children and Adolescents. Pediatr. Surg. Int. 2020, 36, 701–709. [Google Scholar] [CrossRef]
- Cartault, A.; Caula-Legriel, S.; Baunin, C.; Le Mandat, A.; Lemasson, F.; Galinier, P.; Pienkowski, C. Ovarian Masses in Adolescent Girls. Endocr. Dev. 2012, 22, 194–207. [Google Scholar] [CrossRef]
- Zhang, B.; Zhang, L.; Meng, G. Clinical Analysis of 52 Adolescent Patients with Ovarian Masses ≥10 Cm in Diameter. J. Int. Med. Res. 2021, 49, 1–13. [Google Scholar] [CrossRef]
- Marginean, C.O.; Marginean, C.; Chinceşan, M.; Marginean, M.O.; Melit, L.E.; Sasaran, V.; Marginean, C.D. Pediatric Ovarian Tumors, a Challenge for Pediatrician and Gynecologist: Three Case Reports (CARE Compliant). Medicine 2019, 98, e15242. [Google Scholar] [CrossRef]
- Sadeghian, N.; Sadeghian, I.; Mirshemirani, A.; Tabari, A.K.; Ghoroubi, J.; Gorji, F.A.; Roushanzamir, F. Types and Frequency of Ovarian Masses in Children over a 10-Year Period. Casp. J. Intern. Med. 2015, 6, 220. [Google Scholar]
- van Heerden, J.; Tjalma, W.A. The Multidisciplinary Approach to Ovarian Tumours in Children and Adolescents. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 243, 103–110. [Google Scholar] [CrossRef]
- AlDakhil, L.; Aljuhaimi, A.; AlKhattabi, M.; Alobaid, S.; Mattar, R.E.; Alobaid, A. Ovarian Neoplasia in Adolescence: A Retrospective Chart Review of Girls with Neoplastic Ovarian Tumors in Saudi Arabia. J. Ovarian Res. 2022, 15, 105. [Google Scholar] [CrossRef] [PubMed]
- L’Observatoire des Tumeurs Malignes Rares Gynécologiques. Référentiels, Version Février 2022. Available online: https://www.ovaire-rare.org/ (accessed on 12 October 2022).
- Ritchie, J.; O’Mahony, F.; Garden, A. Guideline for the Management of Ovarian Cysts in Children and Adolescents. Br. Soc. Paediatr. Adolesc. Gynaecol. 2018, 11, 2–11. [Google Scholar]
- Sessa, C.; Schneider, D.T.; Planchamp, F.; Baust, K.; Braicu, E.I.; Concin, N.; Godzinski, J.; McCluggage, W.G.; Orbach, D.; Pautier, P.; et al. ESGO–SIOPE Guidelines for the Management of Adolescents and Young Adults with Non-Epithelial Ovarian Cancers. Lancet Oncol. 2020, 21, e360–e368. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.T.; Orbach, D.; Ben-Ami, T.; Bien, E.; Bisogno, G.; Brecht, I.B.; Cecchetto, G.; Ferrari, A.; Godzinski, J.; Janic, D.; et al. Consensus recommendations from the EXPeRT/PARTNER groups for the diagnosis and therapy of sex cord stromal tumors in children and adolescents. Pediatr Blood Cancer. 2021, 68 (Suppl. S4), e29017. [Google Scholar] [CrossRef]
- de Faria, F.W.; Valera, E.T.; Macedo, C.R.P.D.; Azevedo, E.F.; Vieira, A.G.S.; Martins, G.E.; Júnior, A.G.D.C.; dos Reis, M.B.F.; Foulkes, W.D.; Lopes, L.F. Comment on: Consensus recommendations from the EXPeRT/PARTNER groups for the diagnosis and therapy of sex cord stromal tumors in children and adolescents. Pediatr. Blood Cancer 2022, 69, e29650. [Google Scholar] [CrossRef]
- Lockley, M.; Stoneham, S.J.; Olson, T.A. Ovarian Cancer in Adolescents and Young Adults. Pediatr. Blood Cancer 2019, 66, e27512. [Google Scholar] [CrossRef]
- Solheim, O.; Kærn, J.; Tropé, C.G.; Rokkones, E.; Dahl, A.A.; Nesland, J.M.; Fosså, S.D. Malignant Ovarian Germ Cell Tumors: Presentation, Survival and Second Cancer in a Population Based Norwegian Cohort (1953–2009). Gynecol. Oncol. 2013, 131, 330–335. [Google Scholar] [CrossRef]
- Chaopotong, P.; Therasakvichya, S.; Leelapatanadit, C.; Jaishuen, A.; Kuljarusnont, S. Ovarian Cancer in Children and Adolescents: Treatment and Reproductive Outcomes. Asian Pac. J. Cancer Prev. 2015, 16, 4787–4790. [Google Scholar] [CrossRef]
- Yeap, S.T.; Hsiao, C.C.; Hsieh, C.S.; Yu, H.R.; Chen, Y.C.; Chuang, J.H.; Sheen, J.M. Pediatric Malignant Ovarian Tumors: 15 Years of Experience at a Single Institution. Pediatr. Neonatol. 2011, 52, 140–144. [Google Scholar] [CrossRef]
- Janssen, C.L.; Littooij, A.S.; Fiocco, M.; Huige, J.C.B.; de Krijger, R.R.; Hulsker, C.C.C.; Goverde, A.J.; Zsiros, J.; Mavinkurve-Groothuis, A.M.C. The Diagnostic Value of Magnetic Resonance Imaging in Differentiating Benign and Malignant Pediatric Ovarian Tumors. Pediatr. Radiol. 2021, 51, 427. [Google Scholar] [CrossRef]
- van Nimwegen, L.W.E.; Mavinkurve-Groothuis, A.M.C.; de Krijger, R.R.; Hulsker, C.C.C.; Goverde, A.J.; Zsiros, J.; Littooij, A.S. MR Imaging in Discriminating between Benign and Malignant Paediatric Ovarian Masses: A Systematic Review. Eur. Radiol. 2020, 30, 1166. [Google Scholar] [CrossRef] [PubMed]
- Gershenson, D.M. Current Advances in the Management of Malignant Germ Cell and Sex Cord-Stromal Tumors of the Ovary. Gynecol. Oncol. 2012, 125, 515–517. [Google Scholar] [CrossRef] [PubMed]
- Akakpo, P.K.; Derkyi-Kwarteng, L.; Quayson, S.E.; Gyasi, R.K.; Anim, J.T. Ovarian Tumors in Children and Adolescents: A 10-Yr Histopathologic Review in Korle-Bu Teaching Hospital, Ghana. Int. J. Gynecol. Pathol. 2016, 35, 479–507. [Google Scholar] [CrossRef]
- Al-Agha, O.M.; Huwait, H.F.; Chow, C.; Yang, W.; Senz, J.; Kalloger, S.E.; Huntsman, D.G.; Young, R.H.; Gilks, C.B. FOXL2 Is a Sensitive and Specific Marker for Sex Cord-Stromal Tumors of the Ovary. Am. J. Surg. Pathol. 2011, 35, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Ramos, P.; Karnezis, A.N.; Craig, D.W.; Sekulic, A.; Russell, M.L.; Hendricks, W.P.D.; Corneveaux, J.J.; Barrett, M.T.; Shumansky, K.; Yang, Y.; et al. Small Cell Carcinoma of the Ovary, Hypercalcemic Type, Displays Frequent Inactivating Germline and Somatic Mutations in SMARCA4. Nat. Genet. 2014, 46, 427–429. [Google Scholar] [CrossRef]
- Karnezis, A.N.; Wang, Y.; Ramos, P.; Hendricks, W.P.D.; Oliva, E.; D’Angelo, E.; Prat, J.; Nucci, M.R.; Nielsen, T.O.; Chow, C.; et al. Dual Loss of the SWI/SNF Complex ATPases SMARCA4/BRG1 and SMARCA2/BRM Is Highly Sensitive and Specific for Small Cell Carcinoma of the Ovary, Hypercalcaemic Type. J. Pathol. 2016, 238, 389–400. [Google Scholar] [CrossRef]
- Jelinic, P.; Mueller, J.J.; Olvera, N.; Dao, F.; Scott, S.N.; Shah, R.; Gao, J.; Schultz, N.; Gonen, M.; Soslow, R.A.; et al. Recurrent SMARCA4 Mutations in Small Cell Carcinoma of the Ovary. Nat. Genet. 2014, 46, 424–426. [Google Scholar] [CrossRef]
- Mangili, G.; Sigismondi, C.; Gadducci, A.; Cormio, G.; Scollo, P.; Tateo, S.; Ferrandina, G.; Greggi, S.; Candiani, M.; Lorusso, D. Outcome and Risk Factors for Recurrence in Malignant Ovarian Germ Cell Tumors: A MITO-9 Retrospective Study. Int. J. Gynecol. Cancer 2011, 21, 1414–1421. [Google Scholar] [CrossRef]
- de la Motte Rouge, T.; Pautier, P.; Genestie, C.; Rey, A.; Gouy, S.; Leary, A.; Haie-Meder, C.; Kerbrat, P.; Culine, S.; Fizazi, K.; et al. Prognostic Significance of an Early Decline in Serum Alpha-Fetoprotein during Chemotherapy for Ovarian Yolk Sac Tumors. Gynecol. Oncol. 2016, 142, 452–457. [Google Scholar] [CrossRef]
- Reed, N.S.; Pautier, P.; Åvall-Lundqvist, E.; Choi, C.H.; Du Bois, A.; Friedlander, M.; Fyles, A.; Kichenadasse, G.; Provencher, D.M.; Ray-Coquard, I. Gynecologic Cancer InterGroup (GCIG) Consensus Review for Ovarian Small Cell Cancers. Int. J. Gynecol. Cancer 2014, 24 (Suppl. S3), S30–S34. [Google Scholar] [CrossRef]
- Brown, J.; Friedlander, M.; Backes, F.J.; Harter, P.; O’Connor, D.M.; De La Motte Rouge, T.; Lorusso, D.; Maenpaa, J.; Kim, J.W.; Tenney, M.E.; et al. Gynecologic Cancer Intergroup (GCIG) Consensus Review for Ovarian Germ Cell Tumors. Int. J. Gynecol. Cancer 2014, 24 (Suppl. S3), S48–S54. [Google Scholar] [CrossRef]
- Mangili, G.; Sigismondi, C.; Lorusso, D.; Cormio, G.; Candiani, M.; Scarfone, G.; Mascilini, F.; Gadducci, A.; Mosconi, A.M.; Scollo, P.; et al. The Role of Staging and Adjuvant Chemotherapy in Stage I Malignant Ovarian Germ Cell Tumors (MOGTs): The MITO-9 Study. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2017, 28, 333–338. [Google Scholar] [CrossRef]
- Billmire, D.F.; Vinocur, C.; Rescorla, F.; Cushing, B.; London, W.; Schlatter, M.; Davis, M.; Giller, R.; Lauer, S.; Olson, T.; et al. Outcome and Staging Evaluation in Malignant Germ Cell Tumors of the Ovary in Children and Adolescents: An Intergroup Study. J. Pediatr. Surg. 2004, 39, 424–429. [Google Scholar] [CrossRef]
- Young, R.H.; Oliva, E.; Scully, R.E. Small Cell Carcinoma of the Ovary, Hypercalcemic Type. A Clinicopathological Analysis of 150 Cases. Am. J. Surg. Pathol. 1994, 18, 1102–1116. [Google Scholar] [CrossRef]
- Nasioudis, D.; Kanninen, T.T.; Holcomb, K.; Sisti, G.; Witkin, S.S. Prevalence of Lymph Node Metastasis and Prognostic Significance of Lymphadenectomy in Apparent Early-Stage Malignant Ovarian Sex Cord-Stromal Tumors. Gynecol. Oncol. 2017, 145, 243–247. [Google Scholar] [CrossRef]
- Park, J.Y.; Kim, D.Y.; Suh, D.S.; Kim, J.H.; Kim, Y.M.; Kim, Y.T.; Nam, J.H. Outcomes of Pediatric and Adolescent Girls with Malignant Ovarian Germ Cell Tumors. Gynecol. Oncol. 2015, 137, 418–422. [Google Scholar] [CrossRef]
- Braungart, S.; Craigie, R.J.; Farrelly, P.; Losty, P.D. Operative Management of Pediatric Ovarian Tumors and the Challenge of Fertility-Preservation: Results from the UK CCLG Surgeons Cancer Group Nationwide Study. J. Pediatr. Surg. 2020, 55, 2425–2429. [Google Scholar] [CrossRef]
- Gershenson, D.M. Treatment of Ovarian Cancer in Young Women. Clin. Obstet. Gynecol. 2012, 55, 65–74. [Google Scholar] [CrossRef]
- Tomao, F.; Peccatori, F.; del Pup, L.; Franchi, D.; Zanagnolo, V.; Panici, P.B.; Colombo, N. Special Issues in Fertility Preservation for Gynecologic Malignancies. Crit. Rev. Oncol. Hematol. 2016, 97, 206–219. [Google Scholar] [CrossRef]
- Arapaki, A.; Christopoulos, P.; Kalampokas, E.; Triantafyllidou, O.; Matsas, A.; Vlahos, N.F. Ovarian Tissue Cryopreservation in Children and Adolescents. Children 2022, 9, 1256. [Google Scholar] [CrossRef]
- McKenzie, N.D.; Kennard, J.A.; Ahmad, S. Fertility Preserving Options for Gynecologic Malignancies: A Review of Current Understanding and Future Directions. Crit. Rev. Oncol. Hematol. 2018, 132, 116–124. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| SEX CORD-STROMAL TUMOURS | GERM CELL TUMOURS |
|---|---|
| Pure stromal tumours | Teratoma, benign |
| Fibroma, NOS | Immature teratoma, NOS |
| Cellular fibroma | Extra-gonadal teratoma |
| Thecoma | Post-pubertal type teratoma |
| Luteinised thecoma associated with sclerosing peritonitis | Dysgerminoma |
| Sclerosing stromal tumour | Yolk sac tumour |
| Microcystic stromal tumour | Embryonal carcinoma |
| Signet ring stromal tumour | Choriocarcinoma, NOS |
| Leydig cell tumour | Fetus in fetu |
| Steroid cell tumour | Mixed germ cell tumour |
| Malignant steroid cell tumour | Monodermal teratomas and somatic type tumours arising from a dermoid cyst |
| Fibrosarcoma | Struma ovarii, NOS |
| Pure sex cord tumours | Struma ovarii, malignant |
| Adult granulosa cell tumour | Struma carcinoid |
| Juvenile granulosa cell tumour | Teratoma with malignant transformation |
| Sertoli cell tumour, NOS | Cystic teratoma, NOS |
| Sex cord tumour with annular tubules | Germ cell sex cord stromal tumours |
| Mixed sex cord stromal tumours | Gonadoblastoma |
| Sertoli–Leydig cell tumour | Dissecting gonadoblastoma |
| Well differentiated | Undifferentiated gonadal tissue |
| Moderately differentiated | Mixed germ cell-sec cord stromal tumour, unclassified |
| Poorly differentiated | |
| Retiform | |
| Sex cord stromal tumour, NOS | |
| Gynandroblastoma | |
| Other | |
| Papillary cystadenoma |
| L’Observatoire des Tumeurs Malignes Rares Gynécologiques (Centres Experts TRMG) | ESGO-SIOPE | ESMO | BritSPAG | EXPeRT/ PARTNER Consensus | |
|---|---|---|---|---|---|
| Country | France | International/ European | International/ European | United Kingdom | International/ European |
| Issued | 2022 | 2020 | 2018 | 2018 | 2021 |
| Title | Les tumeurs malignes rares gynécologiques—Référentiels | Non-epithelial ovarian cancers in adolescents and young adults | Non-epithelial ovarian cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up | Guideline for the management of ovarian cysts in children and adolescents | Consensus recommendations from the EXPeRT/PARTNER groups for the diagnosis and therapy of sex cord stromal tumours in children and adolescents |
| Diagnostic evaluation | |||||
| Reference to specialised centre with multidisciplinary board | Not discussed | Recommended | Not discussed | Recommended | Not discussed |
| Abdominal–pelvic ultrasound | Recommended as initial imaging | Not discussed | Recommended | Recommended as initial imaging | Recommended |
| Evaluation of endometrial thickness | Recommended for suspected hormone-producing tumours | Recommended for suspected hormone-producing tumours | Endometrial curettage recommended for adults | Not discussed | Not discussed |
| Chest X-ray | Not discussed | Not discussed | Recommended | Not discussed | Recommended |
| CT scan | Not discussed | Recommended thoracic CT scan | Recommended abdominal–pelvic CT scan | Not discussed | Low-dose chest CT as an alternative to chest X-ray |
| Abdominal–pelvic MRI | Recommended for suspected GCTs | Recommended | Not discussed | Not discussed | Recommended |
| PET scan | Recommended in selected cases | Not recommended | Recommended in selected cases | Not discussed | Not discussed |
| Serum tumour markers (basic panel: β-hCG, AFP, LDH, CA125) | Recommended, pre- and post-operative measurement | Recommended, pre- and post-operative measurement | Recommended, pre- and post-operative measurement | Recommended | Recommended |
| Hormonal profile | Not discussed | Recommended if signs of hormonal production/precocious puberty | Not discussed | Recommended if signs of hormonal production/precocious puberty | Recommended |
| Post-operative imaging if omitted preoperatively | Not discussed | Recommended | Not discussed | Recommended | Not discussed |
| Pathology and molecular biology | |||||
| Preoperative biopsy | Not discussed | Recommended if extraovarian spread, avoided if cystic component | Not discussed | Not discussed | Ovarian biopsy strongly discouraged at diagnosis |
| Opinion of expert pathologist | Not discussed | Recommended | Recommended | Not discussed | Recommended |
| Use of immunohistochemical markers | Recommended | Recommended | Recommended | Not discussed | Recommended, FOXL2 for granulosa cell tumours to distinguish adult and juvenile types |
| Karyotyping | Recommended for suspected gonadoblastoma | Recommended for suspected gonadoblastoma | Recommended for suspected gonadoblastoma | Not discussed | Not discussed |
| Mutational analysis | Recommended, DICER1 mutations for suspect SCSTs, SMARCA4 mutations for SCCOHT | Recommended, DICER1 mutations for suspect SCSTs, SMARCA4 mutations for SCCOHT, Germline mutation analysis for bilateral GCTs, unilateral GCTs with pubertal retardation, Sertoli–Leydig cell tumours and SCCOHT | Recommended, DICER1 mutations for suspect SCSTs, SMARCA4 mutations for SCCOHT | Not discussed | Recommended, DICER1 mutations for suspected SLCTs or gynandroblastoma |
| Assessment of prognostic factors | |||||
| GCTs | Not discussed | Recommended, based on age at diagnosis, FIGO stage, tumour histology, residual disease after surgical resection | Not discussed | Not discussed | Not discussed |
| SCSTs | Not discussed | Recommended, based on FIGO stage, size of tumour, intraoperative tumour rupture | Not discussed | Not discussed | Not discussed |
| SCCOHT | Not discussed | Recommended based on FIGO stage, size of tumour, preoperative calcium levels, presence of large cells, residual disease after surgical resection | Not discussed | Not discussed | Not discussed |
| Surgical staging | |||||
| Surgical approach | Not discussed | Open route recommended | Not discussed | Not discussed | Open route recommended |
| Complete surgical staging (peritoneal fluid cytology, complete examination of peritoneal cavity, biopsies of diaphragmatic–paracolic–pelvic peritoneum and abnormal areas, biopsy of omentum, inspection of pelvic–paraaortic lymph nodes and excision of enlarged ones) | Recommended | Recommended | Recommended | Not discussed | Recommended |
| Biopsy of contralateral ovary | Not discussed | Not recommended if macroscopically normal | Not recommended if macroscopically normal | Not discussed | Not recommended if unsuspicious in palpation and by ultrasound |
| Systematic pelvic–paraaortic lymphadenectomy | Not discussed | Not routinely recommended | Not routinely recommended, highly indicated for SCCOHT | Not discussed | Not routinely recommended |
| General principles of therapeutic management | |||||
| Surgical approach | Not discussed | Median laparotomy recommended when high suspicion of malignancy | Open route recommended | Not discussed | Median laparotomy recommended, sub-umbilical transverse Incision or pfannenstiel laparotomy can be accepted |
| Tumour resection | Not discussed | Oophorectomy recommended, tumourectomy–cystectomy to be avoided | Unilateral salpingo-oophorectomy recommended | Not discussed | Oophorectomy or adnexectomy is recommended |
| Fertility-sparing surgery | Not discussed | Recommended if oncologically safe | Recommended if oncologically safe | Recommended if oncologically safe | Recommended for FIGO stage IA SCSTs |
| Fertility preservation | Ovarian stimulation recommended for GCTs and stage IA granulosa SCSTs | Oncofertility counselling recommended | Oocyte cryopreservation with ovarian stimulation recommended | Not discussed | Not discussed |
| Hormone replacement therapy | Recommended for GCTs and SCCOHT, to be discussed for IA and IB granulosa SCSTs, not recommended for other SCSTs | Not discussed | Recommended for GCTs and SCCOHT, not recommended for SCSTs | Not discussed | Not discussed |
| Hormonal contraception (if desired) | Recommended for GCTs, recommended for SCSTs with oestrogen-free products | Not discussed | Recommended for GCTs | Not discussed | Not discussed |
| Follow-up | Recommended with serum tumour markers, tailored depending on histological type of tumour | Recommended with serum tumour markers, tailored depending on histological type of tumour | Recommended with serum tumour markers, ultrasound and CT scan of abdomen, pelvis ± chest, tailored depending on histological type of tumour | Not discussed | Recommended with serum tumour markers, ultrasound, chest X-ray and abdominal MRI in case of equivocal findings and poor visibility on ultrasound |
| Supportive care and psycho–oncological support | Not discussed | Recommended | Not discussed | Not discussed | Not discussed |
| Treatment of GCTs | Not discussed | Not discussed | |||
| Early stage | |||||
| Unilateral oophorectomy recommended | Open unilateral oophorectomy recommended | Unilateral salpingo-oophorectomy recommended | ||
| For bilateral disease, recommendation for preservation of ovarian tissue if possible | For bilateral disease, recommendation for genetic analysis and preservation of ovarian tissue if possible (bilateral salpingo-oophorectomy recommended if gonadoblastoma or dysgerminoma) Lymphadenectomy only if preoperative/intraoperative evidence of nodal involvement | ||||
| BEP is most used regimen | Not recommended for stage IA GCTs with complete surgical resection (only active surveillance needed). Potentially recommended for stage IB GCTs—to be discussed. For stage IC1 GCTs, either ChT or active surveillance recommended For stage IC2-IC3 GCTs, ChT is recommended | BEP is most used regimen | ||
| Stage IA+IB: active surveillance recommended. Stage IC: active surveillance (if complete surgical resection) or ChT recommended | Stage IA: active surveillance recommended. Stage IB+IC: active surveillance (if complete surgical resection) or ChT recommended. | Stage IA: active surveillance recommended. Stage IB+IC: active surveillance (if complete surgical resection) or ChT recommended. | ||
| Stage IA-IC2 grade 1–2: active surveillance recommended. Stage IA-IC2 grade 3: active surveillance (if complete surgical resection) or ChT recommended. Stage IC3 grade 1: active surveillance recommended. Stage IC3 grade 2–3: active surveillance (if complete surgical resection) or ChT recommended. | Not discussed | Stage IA: active surveillance recommended. Stage IB+IC: active surveillance (if complete surgical resection) or ChT recommended. | ||
| Stage IA: active surveillance (if complete surgical resection) or ChT recommended. Stage IB+ IC: ChT recommended. | Stage IA: active surveillance (if complete surgical resection) or ChT recommended. Stage IB+ IC: ChT recommended. | Stage IA+IB: active surveillance (if complete surgical resection) or ChT recommended. Stage IC: ChT recommended. | ||
| Advanced stage | |||||
| Fertility sparing surgery to be considered. Second surgery recommended in case of residual disease, immature teratomas, embryonal carcinomas, non-secreting mixed germ-cell tumours with post-chemotherapy residual lesions | Fertility sparing surgery to be considered. Second surgery recommended in case of residual disease and immature teratomas (exception: immature teratoma and gliomatosis peritonei, where large biopsies can instead be taken). | Fertility sparing surgery to be considered. Second surgery recommended in case of residual disease and immature teratomas. | ||
| BEP regimen is recommended. | BEP regimen for three–four cycles (bleomycin omitted after cycle three) is recommended. Alternative regimens: cisplatine-etoposide-ifosfamide, cisplatin-etoposide-dose-reduced bleomycin, carboplatin-etoposide-bleomycin. | BEP regimen for three–four cycles (bleomycin omitted after cycle three) is recommended. Platinum-sensitive relapse: use of combinations with platinum to be considered. | ||
| Refractory or recurrent disease | Role of surgery unclear, mostly treated with chemotherapy. Prior administration of ChT: BEP (three–four cycles) are recommended. No prior administration of ChT: VelP (vinblastine, ifosfamide, cisplatin) or TIP (paclitaxel, ifosfamide, platine) for three–four cycles to be considered. | Role of surgery unclear, mostly treated with chemotherapy. Prior administration of ChT: previous regimens and the time interval between initial diagnosis and relapse to be considered. | Not discussed | ||
| Intensified chemotherapy ± stem cell support to be considered in case of incomplete response. | Intensified chemotherapy ± stem cell support to be considered in case of incomplete response. Growing teratoma syndrome with only mature tissues in histology: extensive surgical resection is recommended. Recurrent pure dysgerminoma: radiotherapy to be discussed. | ||||
| Treatment of SCSTs | Not discussed | ||||
| Early stage | |||||
| Complete surgical staging (±endometrial curettage) recommended. | Complete surgical staging is recommended. | Complete surgical staging is recommended. | ||
| Total hysterectomy as part only recommended in stage II+. | If adhesions to the omentum, omentectomy is recommended; routine omentectomy not required if unsuspicious | ||||
| Lymphadenectomy only if preoperative or intraoperative evidence of nodal involvement. | Lymphadenectomy only if preoperative or intraoperative evidence of nodal involvement. | Routine retroperitoneal lymph node dissection is not recommended if unsuspicious | |||
| Stage IA: only surgery is recommended, fertility preservation acceptable if macroscopic lesions are excised. | Stage IA: only surgery is recommended. Stage IA+: chemotherapy to be considered. | Stage IA: only surgery is recommended. | Stage IA: only surgery is rec-ommended, fertility preservation is acceptable. Stage IA/IB tumours do not require adjuvant ChT if histology shows good to intermediate differentiation. | ||
| BEP (three–four cycles) is recommended, carboplatin-paclitaxel is alternative option. | BEP (three–four cycles) is recommended, carboplatin-paclitaxel is alternative option. | BEP (three–four cycles) is recommended, carboplatin-paclitaxel is alternative option. | ChT protocols include cisplatin-based regimen (e.g., bleomycin–etoposide-cisplatin or etoposide-ifosfamide–cisplatin). | |
| Stage IA-IC1: ChT may be avoided if complete surgical resection. Stage IC2-IC3: ChT is recommended. | Stage IA-IC1: ChT may be avoided if complete surgical resection. Stage IC2-IC3: ChT is recommended. | Stage IC: ChT is recommended. | In stage IC tumours, three–four cycles of ChT are recommended. | |
| Stage IA-IC2: may be avoided if complete surgical resection. Stage IC3: ChT is recommended. | Stage IC2-IC3: ChT is recommended. | Stage IC: ChT is certainly recommended if preoperative spontaneous tumour rupture and/or malignant ascites | ||
| Stage IA-IC2 well or moderately differentiated Sertoli–Leydig cell tumours: omission of chemotherapy is acceptable. | Stage IC: ChT is recommended. | Stage IA poorly differentiated tumours or with heterologous elements/retiform patterns and Stage >IA: ChT is recommended. | Stage IC: adjuvant ChT is recommended, irrespective of the time of the tumour rupture | |
| Advanced stage | |||||
| Debulking surgery: recommended for advanced stages. | Stage III with incomplete initial macroscopic resection and residual disease after chemotherapy: second surgery to be discussed. | Debulking surgery: recommended for advanced stage granulosa cell tumours. | There is no role for debulking surgery (apart from palliative surgery)—inoperable tumours should be biopsied and upfront ChT should be initiated followed by delayed tumour resection. | |
| Recommended. | Recommended. | Recommended. | In stages II–IV tumours, four cycles of ChT are recommended, with second-look surgery if initial macroscopic incomplete resection or residual disease | |
| BEP regimen for three–four cycles (alternative option: carboplatine-paclitaxel for six cycles). | BEP regimen for at least four cycles (alternative options: cisplatin-etoposide-ifosfamide for at least four cycles or carboplatine-paclitaxel). | BEP regimen for three cycles (alternative option: carboplatine-paclitaxel for six cycles). | Adjuvant ChT is recommended in all tumours with locoregional spread, distant metastases or unresectable tumours | ||
| Refractory/recurrent disease | Platinum-based chemotherapy is recommended. | Treatment plan to be discussed in multidisciplinary board. | Platinum-based chemotherapy is recommended. | ||
| Cytoreductive surgery recommended treatment of choice for relapsed patients. | |||||
| Additional treatment options to be considered. | Additional treatment options to be considered. | Additional treatment options to be considered. | |||
| Treatment of SCCOHT | |||||
| Early stage | Not discussed | Not discussed | |||
| Fertility-sparing surgery is not recommended | Fertility-sparing surgery is not recommended. | Fertility-sparing surgery is not recommended. | ||
| Radical surgery is recommended (including total abdominal hysterectomy, bilateral salpingo-oophorectomy, full pelvic and para-aortic lympadenectomy) | Radical surgery is recommended (including total abdominal hysterectomy, bilateral salpingo-oophorectomy, full pelvic and para-aortic lympadenectomy). | Radical surgery is recommended (including total abdominal hysterectomy, bilateral salpingo-oophorectomy, full pelvic and para-aortic lympadenectomy) | |||
| ChT is recommended. | ChT with platinum and etoposide combinations is recommended. Complete remission after initial chemotherapy: dose-intensive chemotherapy with stem cell support to be discussed. | ChT with platinum and etoposide (and potentially paclitaxel) combinations is recommended. | ||
| Pelvic radiotherapy to be discussed. | Pelvic radiotherapy to be discussed. | Pelvic radiotherapy to be discussed. | |||
| Advanced stage | |||||
| Debulking surgery, either initial or interval after three–six cycles of chemotherapy (including systematic pelvic and para-aortic lymphadenectomy) Is recommended. | Debulking surgery, either initial or interval after three–six cycles of chemotherapy (including systematic pelvic and para-aortic lymphadenectomy) is recommended. | Debulking surgery, either initial or interval after three–six cycles of chemotherapy (including systematic pelvic and para-aortic lymphadenectomy) is recommended. | ||
| ChT is recommended. | ChT with platinum and etoposide combinations is recommended. | ChT with platinum and etoposide combinations is recommended. | ||
| Complete remission after initial surgery and ChT: dose-intensive regimen, followed by high-dose chemotherapy with stem cell support and pelvic radiotherapy to be considered. | |||||
| Refractory/recurrent disease | Not discussed | No suggested treatment. | Not discussed |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Margioula-Siarkou, C.; Petousis, S.; Margioula-Siarkou, G.; Mavromatidis, G.; Chatzinikolaou, F.; Hatzipantelis, E.; Guyon, F.; Dinas, K. Therapeutic Management and Prognostic Factors for Ovarian Malignant Tumours in Adolescents: A Comprehensive Review of Current Guidelines. Diagnostics 2023, 13, 1080. https://doi.org/10.3390/diagnostics13061080
Margioula-Siarkou C, Petousis S, Margioula-Siarkou G, Mavromatidis G, Chatzinikolaou F, Hatzipantelis E, Guyon F, Dinas K. Therapeutic Management and Prognostic Factors for Ovarian Malignant Tumours in Adolescents: A Comprehensive Review of Current Guidelines. Diagnostics. 2023; 13(6):1080. https://doi.org/10.3390/diagnostics13061080
Chicago/Turabian StyleMargioula-Siarkou, Chrysoula, Stamatios Petousis, Georgia Margioula-Siarkou, George Mavromatidis, Fotios Chatzinikolaou, Emmanouel Hatzipantelis, Frédéric Guyon, and Konstantinos Dinas. 2023. "Therapeutic Management and Prognostic Factors for Ovarian Malignant Tumours in Adolescents: A Comprehensive Review of Current Guidelines" Diagnostics 13, no. 6: 1080. https://doi.org/10.3390/diagnostics13061080
APA StyleMargioula-Siarkou, C., Petousis, S., Margioula-Siarkou, G., Mavromatidis, G., Chatzinikolaou, F., Hatzipantelis, E., Guyon, F., & Dinas, K. (2023). Therapeutic Management and Prognostic Factors for Ovarian Malignant Tumours in Adolescents: A Comprehensive Review of Current Guidelines. Diagnostics, 13(6), 1080. https://doi.org/10.3390/diagnostics13061080