
Current Perspectives on Periodontitis in Systemic Sclerosis: Associative Relationships, Pathogenic Links, and Best Practices


 , ,
, , 
 ,
, {kind=link}
{kind=link}
Abstract
1. Introduction
2. Oral Manifestations in Systemic Sclerosis
3. Oral Hygiene in SSc Patients
4. Association between SSc and Periodontitis Supported by Clinical Observational Studies
5. Diagnosis and Evolution of Periodontitis in SSc
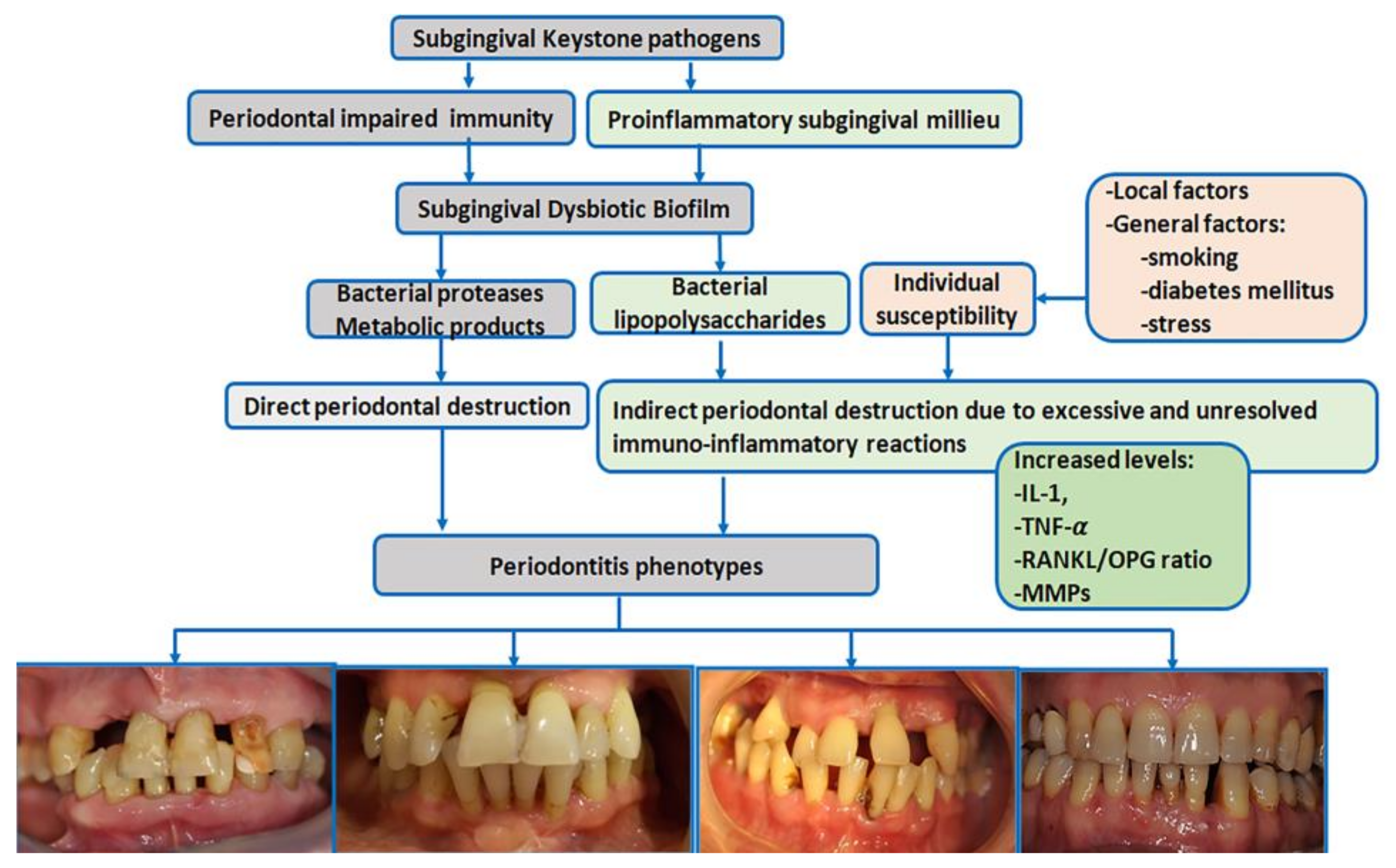
6. A Brief Overview of the Pathogenesis of Periodontitis
7. The Biological Pathogenic Links in Periodontitis and SSc
7.1. Increased Plaque Formation in SSc Patients
7.2. The Role of Vasculopathy in Periodontitis Development
7.3. Proinflammatory Milieu in Both SSc and Periodontitis
7.4. Autoimmunity
7.5. Vitamin D Involvement in SSc and Periodontitis
8. Periodontal Therapy in SSc
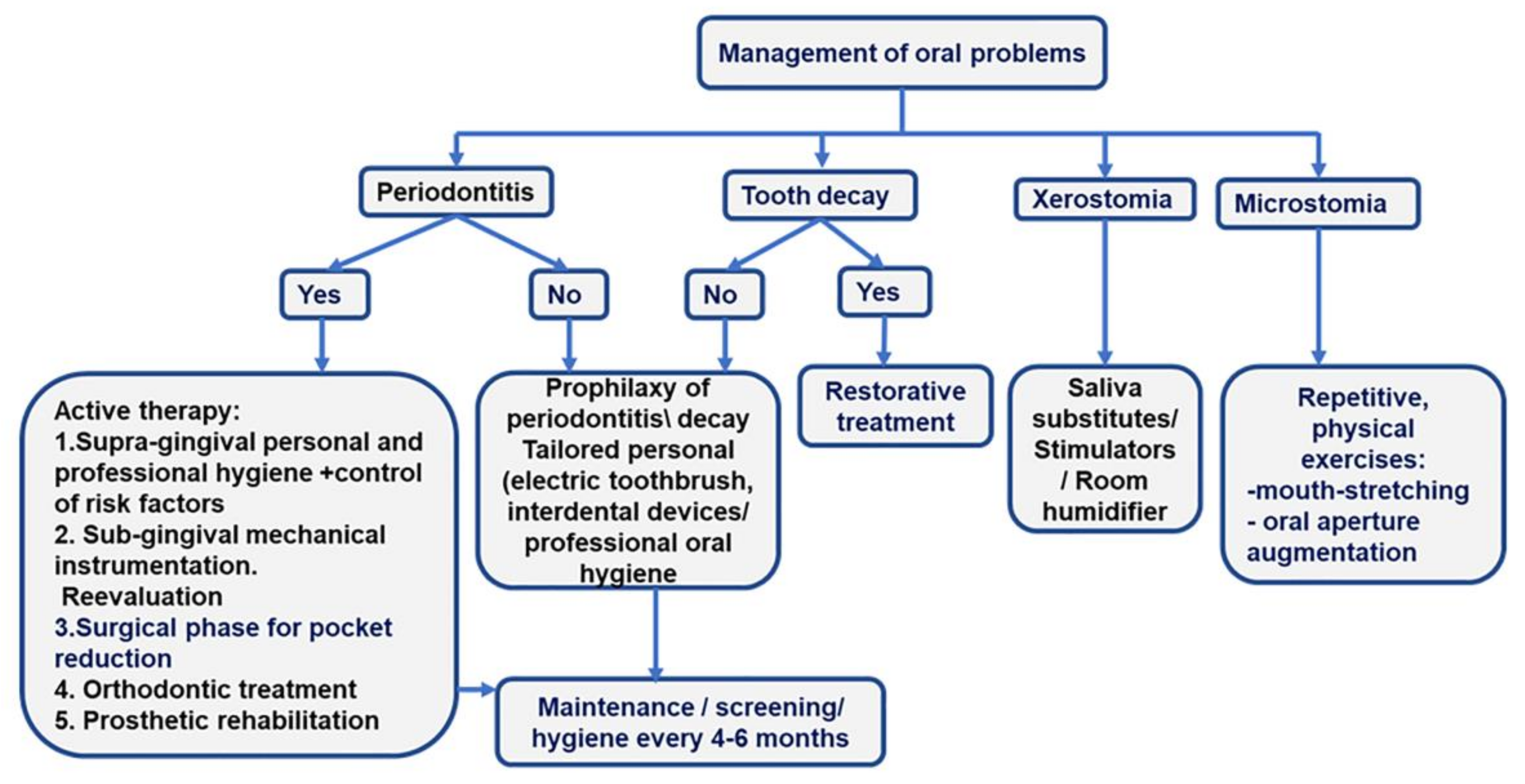
- Preventive therapy. The management of hyposialia should be carried out by prescribing saliva substitutes and stimulators (pilocarpine hydrochloride if Sjogren’s syndrome is associated) to diminish the risk of periodontitis, oral ulcers, and caries. Daily baking soda mouthwash should also be prescribed.
- Prevention and management of microstomia. In patients with microstomia, mouth-opening exercises can improve the inter-incisor distance with severe limitations and the ability to chew, phonation, and dental hygiene [28]. Two times per day, five repetitions of each orofacial physical exercise, holding each for 10 s, should be included in the rehabilitation program of SSc patients: stretching lips with fingers, inflating checks, maximal mouth opening, biting a wood stick with left and right molars, pushing chins to left and right sides with the hand [42].
- Personal oral hygiene or “patient package”. The “patient package” can be used to implement a tailored-oral hygiene protocol for efficiently removing tooth biofilm. The “patient package” represents a complex repetitive approach that implies information, motivation, and teaching the use of personalized oral devices (toothbrush and interdental cleaning aids -dental floss and interdental brushes). The oral-cleaning devices are prescribed to accommodate microstomia and decreased manual dexterity. A small-head oscillating-rotating electric toothbrush or a manual toothbrush with a child-sized brush head, used twice daily, are suitable options for SSc patients [48].
- Management of risk factors. Cessation of smoking is mandatory.
- Prevention of tooth caries. A complex prophylactic package must be implemented to interfere with the cariogenic risk. The package consists of alimentary advice addressing pH modifications, proper specialist-supervised dental hygiene for combating microbial aggression, and systematic fluoridation through fluoride-containing toothpaste associated with fluoride-carrying devices or professional applications of fluoride varnishes [28].
- Bi-annual dental visits for screening of oral lesions (complete periodontal, dental, and oral mucosal examination) and maintenance by providing professional hygienic care and, eventually, treatments.
- Tooth caries should be treated according to current clinical guidelines.
- If diagnosed, periodontitis treatment should follow current clinical guides [31,32]. Briefly, the first phase of therapy is supragingival hygiene and the control of risk factors; the second phase involves subgingival instrumentation and reevaluation. Surgical approaches, orthodontic treatment, and prosthetic rehabilitation drive patients to the end of active therapy and inclusion in the maintenance phase [Figure 2].
- The use of dental implants is case-dependent, according to the ability to perform oral hygiene, the degree of microstomia, and the insertion of posterior implants [28]. Ideally, anterior implants are recommended, particularly at the canine levels of the jaw, to stabilize a removable metal prosthesis [28]. The implant treatment plan should be tailored with regard to disease severity, the presence of sicca syndrome, limitations in performing oral hygiene, and/or the treatment of an oral cancer. Marked gingival fibrosis and severe microvascular impairment contraindicate dental implants. However, the risk-benefit ratio of implant rehabilitation should be appraised.
- Oral ulcers should be combated by local applications of topical antiseptics and anesthetics (such as chlorhexidine and lidocaine 2%) between meals to limit the risk of aspiration.
- Soft resins may be used to manufacture the base of the removable prostheses to overcome oral lesions induced by rigid materials and microstomia [28].
- Anaesthetics without vasoconstrictors should be used in these patients.
9. Conclusions
10. Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denton, C.P.; Khanna, D. Systemic sclerosis. Lancet 2017, 390, 1685–1699. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Zhu, J.; Zhu, Y.; Zhang, X.; Wu, R.; Li, S.; Su, Y. Oral manifestations of patients with systemic sclerosis: A meta-analysis for case-controlled studies. BMC Oral Health 2021, 21, 250. [Google Scholar] [CrossRef]
- Perelas, A.; Silver, R.M.; Arrossi, A.V.; Highland, K.B. Systemic sclerosis-associated interstitial lung disease. Lancet Respir. Med. 2020, 8, 304–320. [Google Scholar] [CrossRef] [PubMed]
- Di Battista, M.; Barsotti, S.; Orlandi, M.; Lepri, G.; Codullo, V.; Della Rossa, A.; Guiducci, S.; Del Galdo, F. One year in review 2021: Systemic sclerosis. Clin. Exp. Rheumatol. 2021, 39, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Østbø, N.; Jimenez, E.Y.; Harb, S.; Bourgeault, A.; Carrier, M.; Thombs, B.D.; the Scleroderma Patient-Centered Intervention Network (SPIN) Diet and Nutrition Education Patient Advisory Team. Nutrition Information Resources Used by People with Systemic Sclerosis and Perceived Advantages and Disadvantages: A Nominal Group Technique Study. ACR Open Rheumatol. 2021, 3, 540–549. [Google Scholar] [CrossRef]
- Shionoya, D.Y.; Kamiga, D.H.; Tsujimoto, D.G.; Nakamura, E.; Nakamura, K.; Sunada, D.K. Anesthetic Management of a Patient With Systemic Sclerosis and Microstomia. Anesthesia Prog. 2020, 67, 28–34. [Google Scholar] [CrossRef]
- Denton, C.P.; Hughes, M.; Gak, N.; Vila, J.; Buch, M.; Chakravarty, K.; Fligelstone, K.; Gompels, L.L.; Griffiths, B.; Herrick, A.L.; et al. BSR and BHPR guideline for the treatment of systemic sclerosis. Rheumatology 2016, 55, 1906–1910. [Google Scholar] [CrossRef]
- De Vries-Bouwstra, J.K.; Allanore, Y.; Matucci-Cerinic, M.; Balbir-Gurman, A. Worldwide Expert Agreement on Updated Recommendations for the Treatment of Systemic Sclerosis. J. Rheumatol. 2019, 47, 249–254. [Google Scholar] [CrossRef]
- Eke, P.I.; Page, R.C.; Wei, L.; Thornton-Evans, G.; Genco, R.J. Update of the Case Definitions for Population-Based Surveillance of Periodontitis. J. Periodontol. 2012, 83, 1449–1454. [Google Scholar] [CrossRef]
- Nazir, M.; Al-Ansari, A.; Al-Khalifa, K.; Alhareky, M.; Gaffar, B.; Almas, K. Global Prevalence of Periodontal Disease and Lack of Its Surveillance. Sci. World J. 2020, 2020, 2146160. [Google Scholar] [CrossRef]
- Eke, P.I.; Thornton-Evans, G.O.; Wei, L.; Borgnakke, W.S.; Dye, B.A.; Genco, R.J. Periodontitis in US Adults. J. Am. Dent. Assoc. 2018, 149, 576–588.e6. [Google Scholar] [CrossRef]
- Stødle, I.H.; Verket, A.; Høvik, H.; Sen, A.; Koldsland, O.C. Prevalence of periodontitis based on the 2017 classification in a Norwegian population: The HUNT study. J. Clin. Periodontol. 2021, 48, 1189–1199. [Google Scholar] [CrossRef]
- Sødal, A.T.T.; Hove, L.H.; Diep, M.T.; Skudutyte-Rysstad, R.; Koldsland, O.C. Periodontal conditions in a 65-year-old population and prevalence of periodontitis according to three different bone level thresholds. BMC Oral Health 2022, 22, 246. [Google Scholar] [CrossRef]
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Guo, H.; Chang, S.; Pi, X.; Hua, F.; Jiang, H.; Liu, C.; Du, M. The Effect of Periodontitis on Dementia and Cognitive Impairment: A Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 6823. [Google Scholar] [CrossRef]
- Priyamvara, A.; Dey, A.K.; Bandyopadhyay, D.; Katikineni, V.; Zaghlol, R.; Basyal, B.; Barssoum, K.; Amarin, R.; Bhatt, D.L.; Lavie, C.J. Periodontal Inflammation and the Risk of Cardiovascular Disease. Curr. Atheroscler. Rep. 2020, 22, 28. [Google Scholar] [CrossRef]
- Nwizu, N.; Wactawski-Wende, J.; Genco, R.J. Periodontal disease and cancer: Epidemiologic studies and possible mechanisms. Periodontology 2000 2020, 83, 213–233. [Google Scholar] [CrossRef]
- Ziukaite, L.; Slot, D.; Cobb, C.; Coucke, W.; Van Der Weijden, G. Prevalence of diabetes among patients diagnosed with periodontitis: A retrospective cross-sectional study. Int. J. Dent. Hyg. 2017, 16, 305–311. [Google Scholar] [CrossRef]
- Gil, L.; Mínguez, I.; Caffesse, R.; Llambés, F. Periodontal Disease in Pregnancy: The Influence of General Factors and Inflammatory Mediators. Oral Health Prev. Dent. 2019, 17, 69–73. [Google Scholar] [CrossRef]
- Pischon, N.; Hoedke, D.; Kurth, S.; Lee, P.; Dommisch, H.; Steinbrecher, A.; Pischon, T.; Burmester, G.R.; Buttgereit, F.; Detert, J.; et al. Increased Periodontal Attachment Loss in Systemic Sclerosis Patients. J. Periodontol. 2016, 87, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Oral Health and Systemic Health—The Great Disconnect. Aust. Dent. J. 2012, 57, 403. [CrossRef] [PubMed]
- Pischon, N.; Pischon, T.; Gülmez, E.; Kröger, J.; Purucker, P.; Kleber, B.-M.; Landau, H.; Jost-Brinkmann, P.-G.; Schlattmann, P.; Zernicke, J.; et al. Periodontal disease in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2010, 69, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Firestein, G.S.; McInnes, I.B. Immunopathogenesis of Rheumatoid Arthritis. Immunity 2017, 46, 183–196. [Google Scholar] [CrossRef] [PubMed]
- De Molon, R.S.; Rossa, C., Jr.; Thurlings, R.M.; Cirelli, J.A.; Koenders, M.I. Linkage of Periodontitis and Rheumatoid Arthritis: Current Evidence and Potential Biological Interactions. Int. J. Mol. Sci. 2019, 20, 4541. [Google Scholar] [CrossRef]
- Krutyhołowa, A.; Strzelec, K.; Dziedzic, A.; Bereta, G.P.; Łazarz-Bartyzel, K.; Potempa, J.; Gawron, K. Host and bacterial factors linking periodontitis and rheumatoid arthritis. Front. Immunol. 2022, 13, 980805. [Google Scholar] [CrossRef]
- Möller, B.; Kollert, F.; Sculean, A.; Villiger, P.M. Infectious Triggers in Periodontitis and the Gut in Rheumatoid Arthritis (RA): A Complex Story about Association and Causality. Front. Immunol. 2020, 11, 1108. [Google Scholar] [CrossRef]
- González-Febles, J.; Sanz, M. Periodontitis and rheumatoid arthritis: What have we learned about their connection and their treatment? Periodontol. 2000 2021, 87, 181–203. [Google Scholar] [CrossRef]
- Alantar, A.; Cabane, J.; Hachulla, E.; Princ, G.; Ginisty, D.; Hassin, M.; Sorel, M.; Maman, L.; Pilat, A.; Mouthon, L. Recommendations for the care of oral involvement in patients with systemic sclerosis. Arthritis Care Res. 2011, 63, 1126–1133. [Google Scholar] [CrossRef]
- Laforgia, A.; Corsalini, M.; Stefanachi, G.; Tafuri, S.; Ballini, A.; Pettini, F.; Di Venere, D. Non-surgical periodontal management in scleroderma disease patients. J. Biol. Regul. Homeost. Agents 2016, 30, 847–851. [Google Scholar]
- Poole, J.; Conte, C.; Brewer, C.; Good, C.C.; Perella, D.; Rossie, K.M.; Steen, V. Oral hygiene in scleroderma: The effectiveness of a multi-disciplinary intervention program. Disabil. Rehabil. 2009, 32, 379–384. [Google Scholar] [CrossRef]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Berglundh, T.; Sculean, A.; Tonetti, M.S.; Aass, A.M.; Aimetti, M.; et al. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2020, 47, 4–60. [Google Scholar] [CrossRef]
- Herrera, D.; Sanz, M.; Kebschull, M.; Jepsen, S.; Sculean, A.; Berglundh, T.; Papapanou, P.N.; Chapple, I.; Tonetti, M.S.; Aimetti, M.; et al. Treatment of stage IV periodontitis: The EFP S3 level clinical practice guideline. J. Clin. Periodontol. 2022, 49, 4–71. [Google Scholar] [CrossRef]
- Smirani, R.; Truchetet, M.; Poursac, N.; Naveau, A.; Schaeverbeke, T.; Devillard, R. Impact of systemic sclerosis oral manifestations on patients’ health-related quality of life: A systematic review. J. Oral Pathol. Med. 2018, 47, 808–815. [Google Scholar] [CrossRef]
- Parat, K.; Radić, M.; Perković, D.; Lukenda, D.B.; Kaliterna, D.M. Reduced salivary flow and caries status are correlated with disease activity and severity in patients with diffuse cutaneous systemic sclerosis. J. Int. Med. Res. 2020, 48, 030006052094137. [Google Scholar] [CrossRef]
- Mohamed, A.A.; Lu, X.-L.; Mounmin, F.A. Diagnosis and Treatment of Esophageal Candidiasis: Current Updates. Can. J. Gastroenterol. Hepatol. 2019, 2019, 3585136. [Google Scholar] [CrossRef]
- Jagadish, R.; Mehta, D.S.; Jagadish, P. Oral and periodontal manifestations associated with systemic sclerosis: A case series and review. J. Indian Soc. Periodontol. 2012, 16, 271–274. [Google Scholar] [CrossRef]
- Balanescu, P.; Balanescu, E.; Baicus, C.; Balanescu, A. S100A6, Calumenin and Cytohesin 2 as Biomarkers for Cutaneous Involvement in Systemic Sclerosis Patients: A Case Control Study. J. Pers. Med. 2021, 11, 368. [Google Scholar] [CrossRef]
- Taveras, J.M. The interpretation of radiographs. In Disorders of the Temporomandibular Joint; Schwartz, L., Ed.; W.B. Saunders: Philadelphia, PA, USA, 1959; pp. 154–162. [Google Scholar]
- Haers, P.; Sailer, H. Mandibular resorption due to systemic sclerosis. Case Report of Surgical Correction of a Secondary Open Bite Deformity. Int. J. Oral Maxillofac. Surg. 1995, 24, 261–267. [Google Scholar] [CrossRef]
- Aliko, A.; Ciancaglini, R.; Alushi, A.; Tafaj, A.; Ruci, D. Temporomandibular joint involvement in rheumatoid arthritis, systemic lupus erythematosus and systemic sclerosis. Int. J. Oral Maxillofac. Surg. 2011, 40, 704–709. [Google Scholar] [CrossRef]
- Ferreira, E.L.A.; Christmann, R.B.; Borba, E.F.; Borges, C.T.L.; Siqueira, J.T.T.; Bonfa, E. Mandibular function is severely impaired in systemic sclerosis patients. J. Orofac. Pain 2010, 24, 197–202. [Google Scholar]
- Cüzdan, N.; Türk, I.; Çiftçi, V.; Arslan, D.; Doğan, M.C.; Ünal, I. The effect of a home-based orofacial exercise program on oral aperture of patients with systemic sclerosis: A single-blind prospective randomized controlled trial. Arch. Rheumatol. 2021, 36, 176–184. [Google Scholar] [CrossRef]
- Sydow, E.; Van der Elst, K.; Verschueren, P.; Lenaerts, J.; Westhovens, R.; De Langhe, E. A mixed method study exploring patient satisfaction and feasibility of two exercise programmes in systemic sclerosis-associated microstomia. Rheumatol. Adv. Pract. 2021, 5, rkab017. [Google Scholar] [CrossRef] [PubMed]
- Mouthon, L.; Rannou, F.; Berezne, A.; Pagnoux, C.; Arene, J.; Fois, E.; Cabane, J.; Guillevin, L.; Revel, M.; Fermanian, J.; et al. Development and validation of a scale for mouth handicap in systemic sclerosis: The Mouth Handicap in Systemic Sclerosis scale. Ann. Rheum. Dis. 2007, 66, 1651–1655. [Google Scholar] [CrossRef] [PubMed]
- Maddali-Bongi, S.; Del Rosso, A.; Mikhaylova, S.; Francini, B.; Branchi, A.; Baccini, M.; Matucci-Cerinic, M. Impact of hand and face disabilities on global disability and quality of life in systemic sclerosis patients. Clin. Exp. Rheumatol. 2014, 32, 15–20. [Google Scholar]
- Klasser, G.D.; Balasubramaniam, R.; Epstein, J. Topical review-connective tissue diseases: Orofacial manifestations including pain. J. Orofac. Pain 2007, 21, 171–184. [Google Scholar]
- Matarese, G.; Isola, G.; Alibrandi, A.; Gullo, A.L.; Bagnato, G.; Cordasco, G.; Perillo, L. Occlusal and MRI characterizations in systemic sclerosis patients: A prospective study from Southern Italian cohort. Jt. Bone Spine 2016, 83, 57–62. [Google Scholar] [CrossRef]
- Yuen, H.; Hant, F.; Hatfield, C.; Summerlin, L.; Smith, E.; Silver, R. Factors associated with oral hygiene practices among adults with systemic sclerosis. Int. J. Dent. Hyg. 2013, 12, 180–186. [Google Scholar] [CrossRef]
- Garaiman, A.; Mihai, C.; Dobrota, R.; Jordan, S.; Maurer, B.; Flemming, J.; Distler, O.; Becker, M.O. The Hospital Anxiety and Depression Scale in patients with systemic sclerosis: A psychometric and factor analysis in a monocentric cohort. Clin. Exp. Rheumatol. 2021, 39, 34–42. [Google Scholar] [CrossRef]
- Yuen, H.K.; Weng, Y.; Bandyopadhyay, D.; Reed, S.G.; Leite, R.S.; Silver, R.M. Effect of a multi-faceted intervention on gingival health among adults with systemic sclerosis. Clin. Exp. Rheumatol. 2011, 29, S26–S32. [Google Scholar]
- Kleber, C.J.; Putt, M.S. Formation of flossing habit using a floss-holding device. J. Dent. Hyg. JDH 1990, 64, 140–143. [Google Scholar]
- Leung, W.K.; Chu, C.H.; Mok, M.Y.; Yeung, K.S.; Ng, S.K. Periodontal Status of Adults With Systemic Sclerosis: Case-Control Study. J. Periodontol. 2011, 82, 1140–1145. [Google Scholar] [CrossRef]
- Mayer, Y.; Elimelech, R.; Balbir-Gurman, A.; Braun-Moscovici, Y.; Machtei, E.E. Periodontal condition of patients with autoimmune diseases and the effect of anti-tumor necrosis factor—A therapy. J. Periodontol. 2013, 84, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Elimelech, R.; Mayer, Y.; Braun-Moscovici, Y.; Machtei, E.E.; Balbir-Gurman, A. Periodontal Conditions and Tumor Necrosis Factor-Alpha Level in Gingival Crevicular Fluid of Scleroderma Patients. Isr. Med. Assoc. J. IMAJ 2015, 17, 549–553. [Google Scholar]
- Baron, M.; Hudson, M.; Tatibouet, S.; Steele, R.; Lo, E.; Gravel, S.; Gyger, G.; Sayegh, T.E.; Pope, J.; Fontaine, A.; et al. The Canadian systemic sclerosis oral health study: Orofacial manifestations and oral health-related quality of life in systemic sclerosis compared with the general population. Rheumatology 2014, 53, 1386–1394. [Google Scholar] [CrossRef] [PubMed]
- Isola, G.; Williams, R.C.; Gullo, A.L.; Ramaglia, L.; Matarese, M.; Iorio-Siciliano, V.; Cosio, C.; Matarese, G. Risk association between scleroderma disease characteristics, periodontitis, and tooth loss. Clin. Rheumatol. 2017, 36, 2733–2741. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, G.S.G.; de Melo, M.L.M.; Leão, J.C.; Carvalho, A.T.; Porter, S.; Duarte, A.L.B.P.; Dantas, A.T.; Gueiros, L.A. Oral features of systemic sclerosis: A case–control study. Oral Dis. 2019, 25, 1995–2002. [Google Scholar] [CrossRef]
- Iordache, C.; Antohe, M.-E.; Chirieac, R.; Ancuța, E.; Țănculescu, O.; Ancuța, C. Volumetric Cone Beam Computed Tomography for the Assessment of Oral Manifestations in Systemic Sclerosis: Data from an EUSTAR Cohort. J. Clin. Med. 2019, 8, 1620. [Google Scholar] [CrossRef]
- Geurs, N.; Iacono, V.; Krayer, J.; Mealey, B.L.; Paquette, D.; Pearson, B.; Schweinebraten, M. American Academy of Periodontology Task Force Report on the Update to the 1999 Classification of Periodontal Diseases and Conditions. J. Periodontol. 2015, 86, 835–838. [Google Scholar] [CrossRef]
- Dagenais, M.; MacDonald, D.; Baron, M.; Hudson, M.; Tatibouet, S.; Steele, R.; Gravel, S.; Mohit, S.; El Sayegh, T.; Pope, J.; et al. The Canadian Systemic Sclerosis Oral Health Study IV: Oral radiographic manifestations in systemic sclerosis compared with the general population. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 104–111. [Google Scholar] [CrossRef]
- White, S.C.; Frey, N.W.; Blaschke, D.D.; Ross, M.D.; Clements, P.J.; Furst, D.E.; Paulus, H.E. Oral radiographic changes in patients with progressive systemic sclerosis (scleroderma). J. Am. Dent. Assoc. 1977, 94, 1178–1182. [Google Scholar] [CrossRef]
- Said, M.H.; Foletti, J.; Graillon, N.; Guyot, L.; Chossegros, C. Orofacial manifestations of scleroderma. A literature review. Rev. Stomatol. Chir. Maxillofac. Chir. Orale 2016, 117, 322–326. [Google Scholar] [CrossRef]
- Baron, M.; Hudson, M.; Tatibouet, S.; Steele, R.; Lo, E.; Gravel, S.; Gyger, G.; El Sayegh, T.; Pope, J.; Fontaine, A.; et al. The Canadian Systemic Sclerosis Oral Health Study III: Relationship between disease characteristics and oro-facial manifestations in systemic sclerosis. Arthritis Care Res. 2014, 12, 180–186. [Google Scholar]
- Page, R.C.; Eke, P.I. Case Definitions for Use in Population-Based Surveillance of Periodontitis. J. Periodontol. 2007, 78, 1387–1399. [Google Scholar] [CrossRef]
- Isola, G.; Palazzo, G.; Polizzi, A.; Murabito, P.; Giuffrida, C.; Gullo, A.L. Association of Systemic Sclerosis and Periodontitis with Vitamin D Levels. Nutrients 2021, 13, 705. [Google Scholar] [CrossRef]
- Rosen, Y.; Daich, J.; Soliman, I.; Brathwaite, E.; Shoenfeld, Y. Vitamin D and autoimmunity. Scand. J. Rheumatol. 2016, 45, 439–447. [Google Scholar] [CrossRef]
- Gullo, A.L.; Mandraffino, G.; Bagnato, G.; Aragona, C.O.; Imbalzano, E.; D’Ascola, A.; Rotondo, F.; Cinquegrani, A.; Mormina, E.; Saitta, C.; et al. Vitamin D Status in Rheumatoid Arthritis: Inflammation, Arterial Stiffness and Circulating Progenitor Cell Number. PLoS ONE 2015, 10, e0134602. [Google Scholar] [CrossRef]
- Zerr, P.; Vollath, S.; Palumbo-Zerr, K.; Tomcik, M.; Huang, J.; Distler, A.; Beyer, C.; Dees, C.; Gela, K.; Distler, O.; et al. Vitamin D receptor regulates TGF-β signalling in systemic sclerosis. Ann. Rheum. Dis. 2014, 74, e20. [Google Scholar] [CrossRef]
- Meghil, M.M.; Hutchens, L.; Raed, A.; Multani, N.A.; Rajendran, M.; Zhu, H.; Looney, S.; Elashiry, M.; Arce, R.M.; Peacock, M.E.; et al. The influence of vitamin D supplementation on local and systemic inflammatory markers in periodontitis patients: A pilot study. Oral Dis. 2019, 25, 1403–1413. [Google Scholar] [CrossRef]
- Chu, C.H.; Yeung, C.M.K.; Lai, I.A.; Leung, W.K.; Mok, M.Y. Oral health of Chinese people with systemic sclerosis. Clin. Oral Investig. 2010, 15, 931–939. [Google Scholar] [CrossRef]
- Papapanou, P.N. Systemic effects of periodontitis: Lessons learned from research on atherosclerotic vascular disease and adverse pregnancy outcomes. Int. Dent. J. 2015, 65, 283–291. [Google Scholar] [CrossRef]
- Jepsen, S.; Caton, J.G.; Albandar, J.M.; Bissada, N.F.; Bouchard, P.; Cortellini, P.; Demirel, K.; de Sanctis, M.; Ercoli, C.; Fan, J.; et al. Periodontal Manifestations of Systemic Diseases and Developmental and Acquired Conditions: Consensus Report of Workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions: Classification and Case Definitions for Periodontal Manifestations of Systemic Diseases and Developmental and Acquired Conditions. J. Periodontol. 2018, 89, S237–S248. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions: Classification and Case Definitions for Periodontitis. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed]
- Needleman, I.; Garcia, R.; Gkranias, N.; Kirkwood, K.L.; Kocher, T.; Di Iorio, A.; Moreno, F.; Petrie, A. Mean annual attachment, bone level, and tooth loss: A systematic review. J. Periodontol. 2018, 89, S120–S139. [Google Scholar] [CrossRef] [PubMed]
- Lamont, R.J.; Koo, H.; Hajishengallis, G. The oral microbiota: Dynamic communities and host interactions. Nat. Rev. Microbiol. 2018, 16, 745–759. [Google Scholar] [CrossRef]
- Abusleme, L.; Hoare, A.; Hong, B.; Diaz, P.I. Microbial signatures of health, gingivitis, and periodontitis. Periodontology 2000 2021, 86, 57–78. [Google Scholar] [CrossRef]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef]
- Abusleme, L.; Dupuy, A.K.; Dutzan, N.; Silva, N.; Burleson, J.A.; Strausbaugh, L.D.; Gamonal, J.; Diaz, P.I. The subgingival microbiome in health and periodontitis and its relationship with community biomass and inflammation. ISME J. 2013, 7, 1016–1025. [Google Scholar] [CrossRef]
- Hajishengallis, G. Immunomicrobial pathogenesis of periodontitis: Keystones, pathobionts, and host response. Trends Immunol. 2013, 35, 3–11. [Google Scholar] [CrossRef]
- Plemmenos, G.; Evangeliou, E.; Polizogopoulos, N.; Chalazias, A.; Deligianni, M.; Piperi, C. Central Regulatory Role of Cytokines in Periodontitis and Targeting Options. Curr. Med. Chem. 2021, 28, 3032–3058. [Google Scholar] [CrossRef]
- Pan, W.; Wang, Q.; Chen, Q. The cytokine network involved in the host immune response to periodontitis. Int. J. Oral Sci. 2019, 11, 30. [Google Scholar] [CrossRef]
- Tsukasaki, M. RANKL and osteoimmunology in periodontitis. J. Bone Miner. Metab. 2020, 39, 82–90. [Google Scholar] [CrossRef]
- Di Benedetto, A.; Gigante, I.; Colucci, S.; Grano, M. Periodontal Disease: Linking the Primary Inflammation to Bone Loss. Clin. Dev. Immunol. 2013, 2013, 503754. [Google Scholar] [CrossRef]
- Niklander, S.; Bordagaray, M.; Fernández, A.; Hernández, M. Vascular Endothelial Growth Factor: A Translational View in Oral Non-Communicable Diseases. Biomolecules 2021, 11, 85. [Google Scholar] [CrossRef]
- Huang, J.; Cai, X.; Ou, Y.; Zhou, Y.; Wang, Y. Resolution of inflammation in periodontitis: A review. Int. J. Clin. Exp. Pathol. 2018, 11, 4283–4295. [Google Scholar]
- Scala, E.; Pallotta, S.; Frezzolini, A.; Abeni, D.; Barbieri, C.; Sampogna, F.; DE Pità, O.; Puddu, P.; Paganelli, R.; Russo, G. Cytokine and chemokine levels in systemic sclerosis: Relationship with cutaneous and internal organ involvement. Clin. Exp. Immunol. 2004, 138, 540–546. [Google Scholar] [CrossRef]
- Scardina, G.; Pizzigatti, M.; Messina, P. Periodontal Microcirculatory Abnormalities in Patients with Systemic Sclerosis. J. Periodontol. 2005, 76, 1991–1995. [Google Scholar] [CrossRef]
- Maurer, B.; Distler, A.; Suliman, Y.A.; Gay, R.E.; Michel, B.A.; Gay, S.; Distler, J.H.W.; Distler, O. Vascular endothelial growth factor aggravates fibrosis and vasculopathy in experimental models of systemic sclerosis. Ann. Rheum. Dis. 2013, 73, 1880–1887. [Google Scholar] [CrossRef]
- Manetti, M.; Guiducci, S.; Romano, E.; Bellando-Randone, S.; Lepri, G.; Bruni, C.; Conforti, M.L.; Ibba-Manneschi, L.; Matucci-Cerinic, M. Increased plasma levels of the VEGF165b splice variant are associated with the severity of nailfold capillary loss in systemic sclerosis. Ann. Rheum. Dis. 2013, 72, 1425–1427. [Google Scholar] [CrossRef]
- Ozcelik, O.; Haytac, M.C.; Ergin, M.; Antmen, B.; Seydaoglu, G. The immunohistochemical analysis of vascular endothelial growth factors A and C and microvessel density in gingival tissues of systemic sclerosis patients: Their possible effects on gingival inflammation. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2008, 105, 481–485. [Google Scholar] [CrossRef]
- Koch, A.E.; Distler, O. Vasculopathy and disordered angiogenesis in selected rheumatic diseases: Rheumatoid arthritis and systemic sclerosis. Arthritis Res. Ther. 2007, 9, S3. [Google Scholar] [CrossRef]
- Luzina, I.G.; Atamas, S.P.; Wise, R.; Wigley, F.M.; Choi, J.; Xiao, H.Q.; White, B. Occurrence of an activated, profibrotic pattern of gene expression in lung CD8+ T cells from scleroderma patients. Arthritis Rheum. 2003, 48, 2262–2274. [Google Scholar] [CrossRef] [PubMed]
- Gyftaki-Venieri, D.A.; Abraham, D.J.; Ponticos, M. Insights into myofibroblasts and their activation in scleroderma: Opportunities for therapy? Curr. Opin. Rheumatol. 2018, 30, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Korman, B. Evolving insights into the cellular and molecular pathogenesis of fibrosis in systemic sclerosis. Transl. Res. 2019, 209, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Fang, F.; Jiang, D. IL-1β/HMGB1 signalling promotes the inflammatory cytokines release via TLR signalling in human intervertebral disc cells. Biosci. Rep. 2016, 36, e00379. [Google Scholar] [CrossRef]
- Gamal, R.M.; Gamal, W.M.; Ghandour, A.M.; Abozaid, H.S.M.; Mohamed, M.E.; Emad, Y.; Galeel, A.A. Study of the osteoprotegerin/receptor activator of nuclear factor-kB ligand system association with inflammation and atherosclerosis in systemic sclerosis. Immunol. Investig. 2018, 47, 241–250. [Google Scholar] [CrossRef]
- Taylan, A.; Birlik, M.; Kenar, G.; Toprak, B.; Gundogdu, B.; Gurler, O.; Karakas, B.; Akıncı, B.; Sisman, A.R. Osteoprotegrin interacts with biomarkers and cytokines that have roles in osteoporosis, skin fibrosis, and vasculopathy in systemic sclerosis: A potential multifaceted relationship between OPG/RANKL/TRAIL and Wnt inhibitors. Mod. Rheumatol. 2018, 29, 619–624. [Google Scholar] [CrossRef]
- Tilvawala, R.; Nguyen, S.H.; Maurais, A.J.; Nemmara, V.V.; Nagar, M.; Salinger, A.J.; Nagpal, S.; Weerapana, E.; Thompson, P.R. The Rheumatoid Arthritis-Associated Citrullinome. Cell Chem. Biol. 2018, 25, 691–704. [Google Scholar] [CrossRef]
- Darrah, E.; Andrade, F. Rheumatoid arthritis and citrullination. Curr. Opin. Rheumatol. 2018, 30, 72–78. [Google Scholar] [CrossRef]
- Nguyen, H.; James, E.A. Immune recognition of citrullinated epitopes. Immunology 2016, 149, 131–138. [Google Scholar] [CrossRef]
- Wielosz, E.; Majdan, M.; Dryglewska, M.; Zwolak, R. Anti-CCP antibodies and rheumatoid factor in systemic sclerosis: Prevalence and relationships with joint manifestations. Adv. Clin. Exp. Med. 2018, 27, 1253–1257. [Google Scholar] [CrossRef]
- Ciesielski, O.; Biesiekierska, M.; Panthu, B.; Soszyński, M.; Pirola, L.; Balcerczyk, A. Citrullination in the pathology of inflammatory and autoimmune disorders: Recent advances and future perspectives. Cell. Mol. Life Sci. 2022, 79, 94. [Google Scholar] [CrossRef]
- Olsen, I.; Yamazaki, K. Can oral bacteria affect the microbiome of the gut? J. Oral Microbiol. 2019, 11, 1586422. [Google Scholar] [CrossRef]
- Laustriat, G.; Ruyssen-Witrand, A.; Constantin, A.; Barnetche, T.; Adoue, D.; Cantagrel, A.; Degboé, Y. Anti-citrullinated peptides antibodies in systemic sclerosis: Meta-analysis of frequency and meaning. Jt. Bone Spine 2018, 85, 147–153. [Google Scholar] [CrossRef]
- Van Venrooij, W.J.; Van Beers, J.J.; Pruijn, G.J. Anti-CCP Antibody, a Marker for the Early Detection of Rheumatoid Arthritis. Ann. N. Y. Acad. Sci. 2008, 1143, 268–285. [Google Scholar] [CrossRef]
- Siebuhr, A.S.; Kjelgaard-Petersen, C.F.; Sun, S.; Byrjalsen, I.; Christiansen, C.; Karsdal, M.A.; Bay-Jensen, A.-C. Suppression of active, but not total MMP-3, is associated with treatment response in a phase III clinical study of rheumatoid arthritis. Clin. Exp. Rheumatol. 2017, 36, 94–101. [Google Scholar]
- Gullo, A.L.; Mandraffino, G.; Rodríguez-Carrio, J.; Scuruchi, M.; Sinicropi, D.; Postorino, M.; Morace, C.; Giuffrida, C.; Sciortino, D.; Gallizzi, R.; et al. Endocan and Circulating Progenitor Cells in Women with Systemic Sclerosis: Association with Inflammation and Pulmonary Hypertension. Biomedicines 2021, 9, 533. [Google Scholar] [CrossRef]
- Arnson, Y.; Amital, H.; Agmon-Levin, N.; Alon, D.; Sánchez-Castañón, M.; López-Hoyos, M.; Matucci-Cerinic, M.; Szücs, G.; Shapira, Y.; Szekanecz, Z.; et al. Serum 25-OH vitamin D concentrations are linked with various clinical aspects in patients with systemic sclerosis: A retrospective cohort study and review of the literature. Autoimmun. Rev. 2011, 10, 490–494. [Google Scholar] [CrossRef]
- Hiremath, V.P.; Rao, C.B.; Naik, V.; Prasad, K.V. Anti-inflammatory Effect of Vitamin D on Gingivitis: A Dose-Response Randomised Control Trial. Oral Health Prev. Dent. 2013, 11, 61–69. [Google Scholar] [CrossRef]
- Grenier, D.; Morin, M.-P.; Fournier-Larente, J.; Chen, H. Vitamin D inhibits the growth of and virulence factor gene expression by Porphyromonas gingivalis and blocks activation of the nuclear factor kappa B transcription factor in monocytes. J. Periodontal Res. 2015, 51, 359–365. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ciurea, A.; Rednic, N.V.; Soancă, A.; Micu, I.C.; Stanomir, A.; Oneț, D.; Șurlin, P.; Filipescu, I.; Roman, A.; Stratul, Ș.I.; et al. Current Perspectives on Periodontitis in Systemic Sclerosis: Associative Relationships, Pathogenic Links, and Best Practices. Diagnostics 2023, 13, 841. https://doi.org/10.3390/diagnostics13050841
Ciurea A, Rednic NV, Soancă A, Micu IC, Stanomir A, Oneț D, Șurlin P, Filipescu I, Roman A, Stratul ȘI, et al. Current Perspectives on Periodontitis in Systemic Sclerosis: Associative Relationships, Pathogenic Links, and Best Practices. Diagnostics. 2023; 13(5):841. https://doi.org/10.3390/diagnostics13050841
Chicago/Turabian StyleCiurea, Andreea, Nicolae Voicu Rednic, Andrada Soancă, Iulia Cristina Micu, Alina Stanomir, Diana Oneț, Petra Șurlin, Ileana Filipescu, Alexandra Roman, Ștefan Ioan Stratul, and et al. 2023. "Current Perspectives on Periodontitis in Systemic Sclerosis: Associative Relationships, Pathogenic Links, and Best Practices" Diagnostics 13, no. 5: 841. https://doi.org/10.3390/diagnostics13050841
APA StyleCiurea, A., Rednic, N. V., Soancă, A., Micu, I. C., Stanomir, A., Oneț, D., Șurlin, P., Filipescu, I., Roman, A., Stratul, Ș. I., & Pamfil, C. (2023). Current Perspectives on Periodontitis in Systemic Sclerosis: Associative Relationships, Pathogenic Links, and Best Practices. Diagnostics, 13(5), 841. https://doi.org/10.3390/diagnostics13050841