
Prognostic Significance of Programmed Cell Death Ligand 1 Expression in High-Grade Serous Ovarian Carcinoma: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Materials and Methods
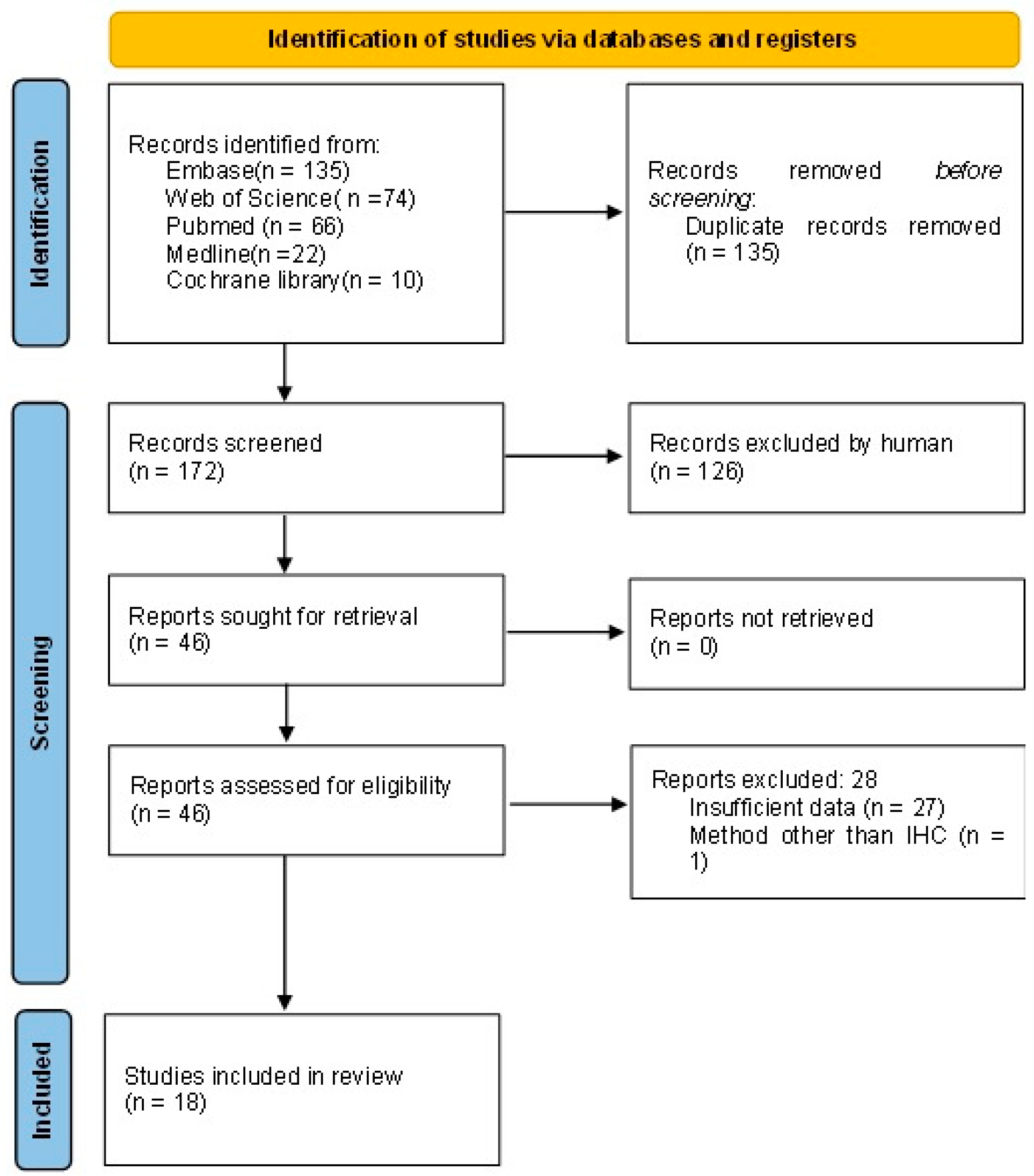
2.1. Literature Search and Study Design
2.2. Literature Selection
2.3. Extraction of Data
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Included Studies
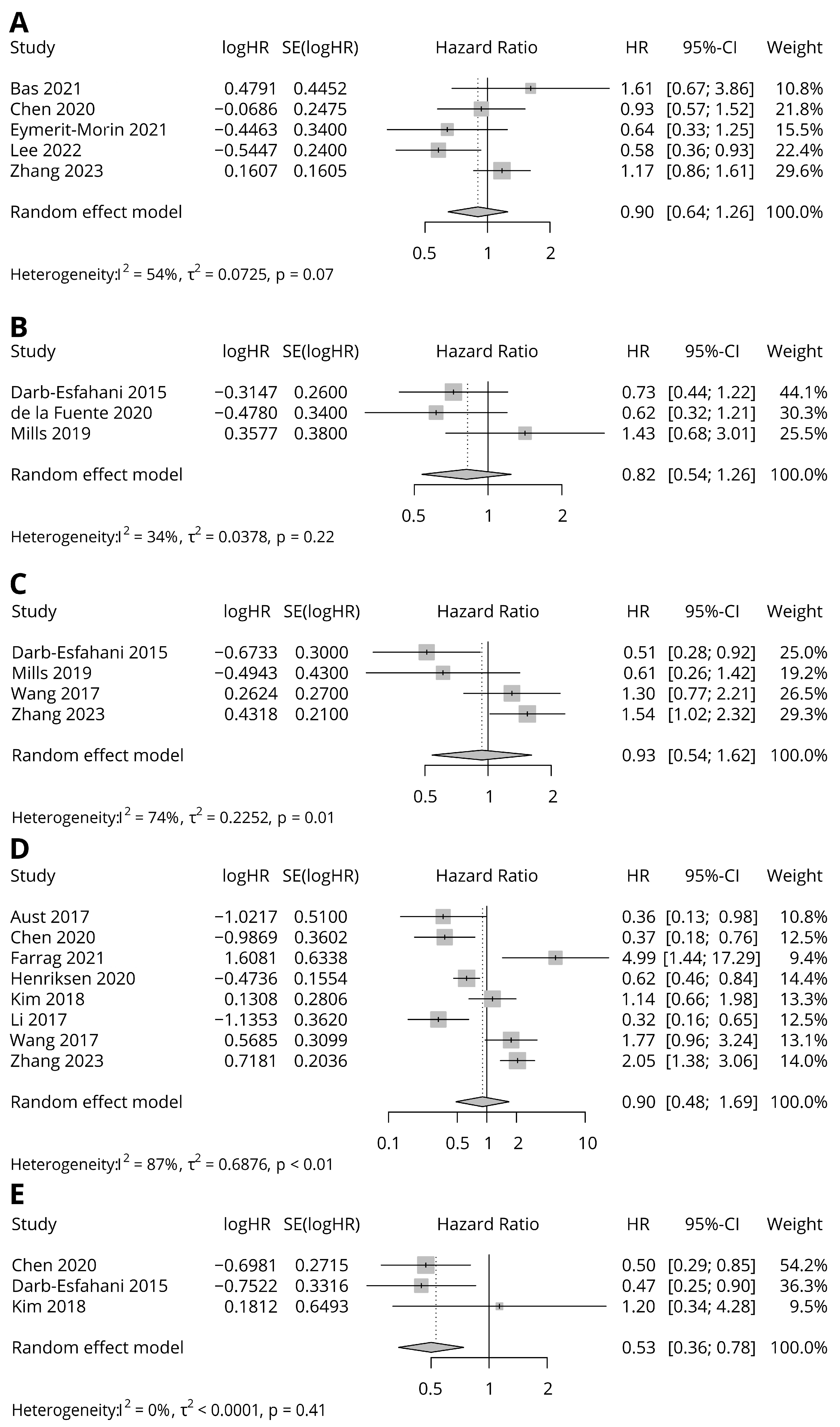
3.2. Prognostic Significance of PD-L1 Expression
3.3. Subgroup Analysis
3.4. Subgroup Analysis of Data from Studies with FDA-Approved Antibodies
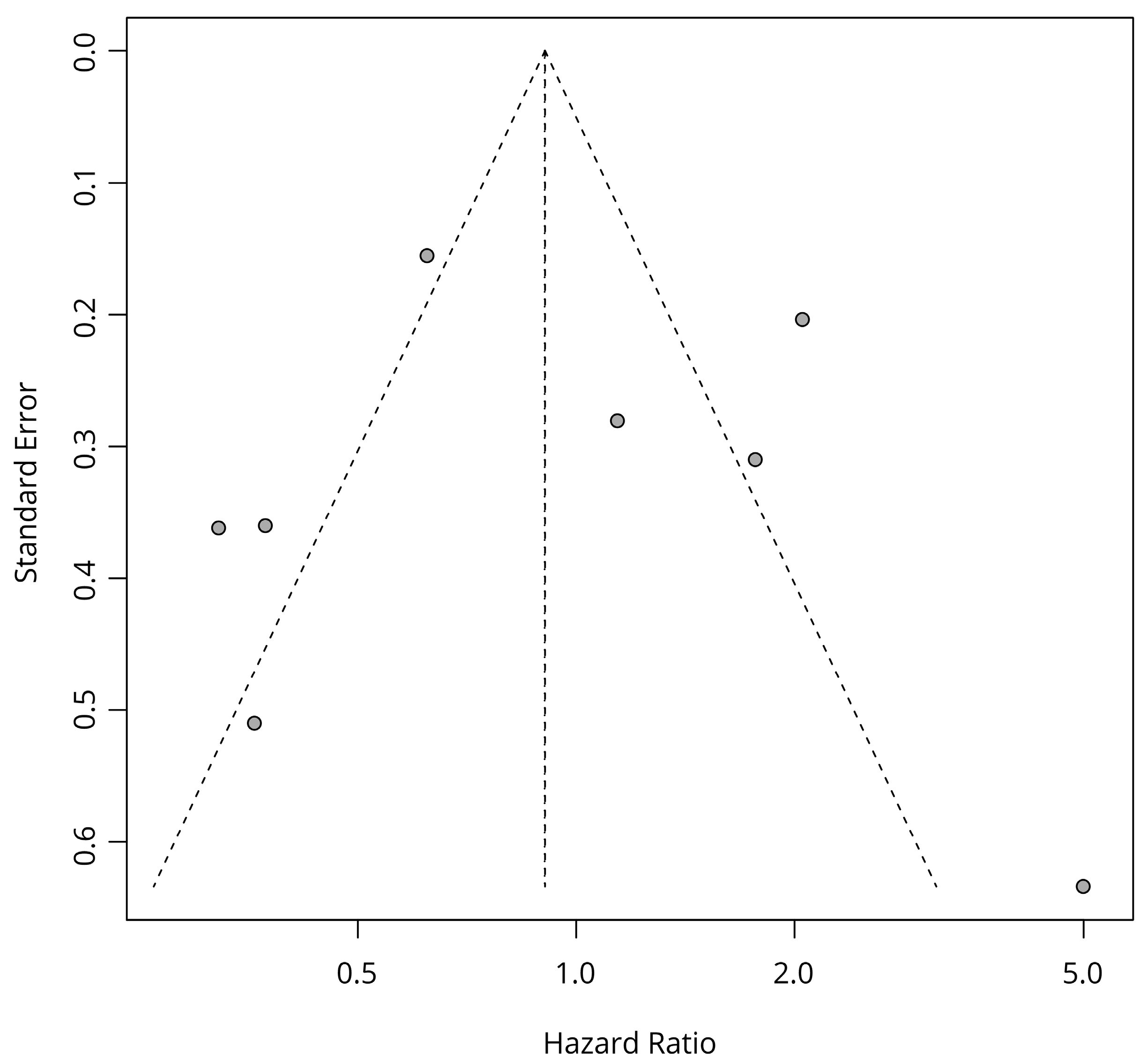
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peres, L.C.; Cushing-Haugen, K.L.; Anglesio, M.; Wicklund, K.; Bentley, R.; Berchuck, A.; Kelemen, L.E.; Nazeran, T.M.; Gilks, C.B.; Harris, H.R.; et al. Histotype classification of ovarian carcinoma: A comparison of approaches. Gynecol. Oncol. 2018, 151, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.L.; Brady, M.F.; Wenzel, L.; Fleming, G.F.; Huang, H.Q.; DiSilvestro, P.A.; Fujiwara, K.; Alberts, D.S.; Zheng, W.; Tewari, K.S.; et al. Randomized Trial of Intravenous Versus Intraperitoneal Chemotherapy Plus Bevacizumab in Advanced Ovarian Carcinoma: An NRG Oncology/Gynecologic Oncology Group Study. J. Clin. Oncol. 2019, 37, 1380–1390. [Google Scholar] [CrossRef]
- Bolton, K.L.; Chenevix-Trench, G.; Goh, C.; Sadetzki, S.; Ramus, S.J.; Karlan, B.Y.; Lambrechts, D.; Despierre, E.; Barrowdale, D.; McGuffog, L.; et al. Association between BRCA1 and BRCA2 mutations and survival in women with invasive epithelial ovarian cancer. JAMA 2012, 307, 382–390. [Google Scholar] [CrossRef] [PubMed]
- Pennington, K.P.; Walsh, T.; Harrell, M.I.; Lee, M.K.; Pennil, C.C.; Rendi, M.H.; Thornton, A.; Norquist, B.M.; Casadei, S.; Nord, A.S.; et al. Germline and somatic mutations in homologous recombination genes predict platinum response and survival in ovarian, fallopian tube, and peritoneal carcinomas. Clin. Cancer Res. 2014, 20, 764–775. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Martin, A.; Pothuri, B.; Vergote, I.; DePont Christensen, R.; Graybill, W.; Mirza, M.R.; McCormick, C.; Lorusso, D.; Hoskins, P.; Freyer, G.; et al. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019, 381, 2391–2402. [Google Scholar] [CrossRef]
- Moore, K.; Colombo, N.; Scambia, G.; Kim, B.G.; Oaknin, A.; Friedlander, M.; Lisyanskaya, A.; Floquet, A.; Leary, A.; Sonke, G.S.; et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2018, 379, 2495–2505. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.; Wu, D.; Li, L.; Chai, Y.; Huang, J. PD-L1 and Survival in Solid Tumors: A Meta-Analysis. PLoS ONE 2015, 10, e0131403. [Google Scholar] [CrossRef]
- Sanmamed, M.F.; Chen, L. Inducible expression of B7-H1 (PD-L1) and its selective role in tumor site immune modulation. Cancer J. 2014, 20, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, Z.; Li, Y.; Zhao, W.; Wu, J.; Zhang, Z. PD-1/PD-L1 Checkpoint Inhibitors in Tumor Immunotherapy. Front. Pharmacol. 2021, 12, 731798. [Google Scholar] [CrossRef] [PubMed]
- Aust, S.; Felix, S.; Auer, K.; Bachmayr-Heyda, A.; Kenner, L.; Dekan, S.; Meier, S.M.; Gerner, C.; Grimm, C.; Pils, D. Absence of PD-L1 on tumor cells is associated with reduced MHC I expression and PD-L1 expression increases in recurrent serous ovarian cancer. Sci. Rep. 2017, 7, 42929. [Google Scholar] [CrossRef]
- Bansal, A.; Srinivasan, R.; Rohilla, M.; Rai, B.; Rajwanshi, A.; Suri, V.; Chandra Saha, S. Immunotyping in tubo-ovarian high-grade serous carcinoma by PD-L1 and CD8+ T-lymphocytes predicts disease-free survival. APMIS 2021, 129, 254–264. [Google Scholar] [CrossRef]
- Bas, Y.; Koc, N.; Helvaci, K.; Kocak, C.; Akdeniz, R.; Sahin, H.H.K. Clinical and pathological significance of programmed cell death 1 (PD-1)/programmed cell death ligand 1 (PD-L1) expression in high grade serous ovarian cancer. Transl. Oncol. 2021, 14, 100994. [Google Scholar] [CrossRef]
- Chen, H.; Molberg, K.; Strickland, A.L.; Castrillon, D.H.; Carrick, K.; Jiang, Q.; Niu, S.; Rivera-Colon, G.; Gwin, K.; Hinson, S.; et al. PD-L1 Expression and CD8+ Tumor-infiltrating Lymphocytes in Different Types of Tubo-ovarian Carcinoma and Their Prognostic Value in High-grade Serous Carcinoma. Am. J. Surg. Pathol. 2020, 44, 1050–1060. [Google Scholar] [CrossRef] [PubMed]
- Darb-Esfahani, S.; Kunze, C.A.; Kulbe, H.; Sehouli, J.; Wienert, S.; Lindner, J.; Budczies, J.; Bockmayr, M.; Dietel, M.; Denkert, C.; et al. Prognostic impact of programmed cell death-1 (PD-1) and PD-ligand 1 (PD-L1) expression in cancer cells and tumor-infiltrating lymphocytes in ovarian high grade serous carcinoma. Oncotarget 2016, 7, 1486–1499. [Google Scholar] [CrossRef]
- Eymerit-Morin, C.; Ilenko, A.; Gaillard, T.; Varinot, J.; Comperat, E.; Bendifallah, S.; Darai, E. PD-L1 expression with QR1 and E1L3N antibodies according to histological ovarian cancer subtype: A series of 232 cases. Eur. J. Histochem. 2021, 65, 1. [Google Scholar] [CrossRef]
- Farrag, M.S.; Abdelwahab, K.; Farrag, N.S.; Elrefaie, W.E.; Emarah, Z. Programmed death ligand-1 and CD8 tumor-infiltrating lymphocytes (TILs) as prognostic predictors in ovarian high-grade serous carcinoma (HGSC). J. Egypt. Natl. Cancer Inst. 2021, 33, 16. [Google Scholar] [CrossRef] [PubMed]
- Fucikova, J.; Rakova, J.; Hensler, M.; Kasikova, L.; Belicova, L.; Hladikova, K.; Truxova, I.; Skapa, P.; Laco, J.; Pecen, L.; et al. TIM-3 Dictates Functional Orientation of the Immune Infiltrate in Ovarian Cancer. Clin. Cancer Res. 2019, 25, 4820–4831. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, J.R.; Donskov, F.; Waldstrom, M.; Jakobsen, A.; Hjortkjaer, M.; Petersen, C.B.; Dahl Steffensen, K. Favorable prognostic impact of Natural Killer cells and T cells in high-grade serous ovarian carcinoma. Acta Oncol. 2020, 59, 652–659. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Kim, J.Y.; Lee, Y.J.; Kim, S.H.; Lee, J.Y.; Nam, E.J.; Kim, S.; Kim, S.W.; Kim, Y.T. Expression of programmed cell death ligand 1 and immune checkpoint markers in residual tumors after neoadjuvant chemotherapy for advanced high-grade serous ovarian cancer. Gynecol. Oncol. 2018, 151, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.J.; Woo, H.Y.; Kim, Y.N.; Park, J.; Nam, E.J.; Kim, S.W.; Kim, S.; Kim, Y.T.; Park, E.; Joung, J.G.; et al. Dynamics of the Tumor Immune Microenvironment during Neoadjuvant Chemotherapy of High-Grade Serous Ovarian Cancer. Cancers 2022, 14, 2308. [Google Scholar] [CrossRef]
- Li, M.; Li, H.; Liu, F.; Bi, R.; Tu, X.; Chen, L.; Ye, S.; Cheng, X. Characterization of ovarian clear cell carcinoma using target drug-based molecular biomarkers: Implications for personalized cancer therapy. J. Ovarian Res. 2017, 10, 9. [Google Scholar] [CrossRef] [PubMed]
- Martin de la Fuente, L.; Westbom-Fremer, S.; Arildsen, N.S.; Hartman, L.; Malander, S.; Kannisto, P.; Masback, A.; Hedenfalk, I. PD-1/PD-L1 expression and tumor-infiltrating lymphocytes are prognostically favorable in advanced high-grade serous ovarian carcinoma. Virchows Arch. 2020, 477, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Mills, A.M.; Peres, L.C.; Meiss, A.; Ring, K.L.; Modesitt, S.C.; Abbott, S.E.; Alberg, A.J.; Bandera, E.V.; Barnholtz-Sloan, J.; Bondy, M.L.; et al. Targetable Immune Regulatory Molecule Expression in High-Grade Serous Ovarian Carcinomas in African American Women: A Study of PD-L1 and IDO in 112 Cases From the African American Cancer Epidemiology Study (AACES). Int. J. Gynecol. Pathol. 2019, 38, 157–170. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Lou, W.; Di, W.; Wu, X. Prognostic value of tumor PD-L1 expression combined with CD8(+) tumor infiltrating lymphocytes in high grade serous ovarian cancer. Int. Immunopharmacol. 2017, 52, 7–14. [Google Scholar] [CrossRef]
- Zhang, T.; Zhou, X.; Zhang, X.; Niu, S.; Chen, H.; Zhou, F. Discordance of PD-L1 expression in primary and metastatic ovarian high-grade serous carcinoma and its correlation with CD8+ tumor-infiltrating lymphocytes and patient prognosis. Virchows Arch. 2023, 482, 755–766. [Google Scholar] [CrossRef]
- Huang, L.J.; Deng, X.F.; Chang, F.; Wu, X.L.; Wu, Y.; Diao, Q.Z. Prognostic significance of programmed cell death ligand 1 expression in patients with ovarian carcinoma: A systematic review and meta-analysis. Medicine 2018, 97, e12858. [Google Scholar] [CrossRef]
- Piao, J.; Lim, H.J.; Lee, M. Prognostic value of programmed cell death ligand-1 expression in ovarian cancer: An updated meta-analysis. Obstet. Gynecol. Sci. 2020, 63, 346–356. [Google Scholar] [CrossRef]
- Wang, L. Prognostic effect of programmed death-ligand 1 (PD-L1) in ovarian cancer: A systematic review, meta-analysis and bioinformatics study. J. Ovarian Res. 2019, 12, 37. [Google Scholar] [CrossRef]
- Cheng, B.; Liang, H.; Jiang, T.; Chen, J.; Wang, G. Characterization of PD-L1 expression and its prognostic value in patients with ovarian cancer. Transl. Cancer Res. 2018, 7, 1271–1281. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef]
- Irvine, A.F.; Waise, S.; Green, E.W.; Stuart, B. A non-linear optimisation method to extract summary statistics from Kaplan-Meier survival plots using the published P value. BMC Med. Res. Methodol. 2020, 20, 269. [Google Scholar] [CrossRef]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; Version 4.3.0; R Foundation for Statistical Computing: Vienna, Austria, 2023. [Google Scholar]
- Balduzzi, S.; Rucker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Yang, Y.; Chen, Y.; Lin, W.; Chen, X.; Liu, J.; Huang, Y.; Wang, H.; Teng, L. PD-L1: Biological mechanism, function, and immunotherapy in gastric cancer. Front. Immunol. 2022, 13, 1060497. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Han, J.; Yang, Y.; Chen, Y. PD-1/PD-L1 checkpoint inhibitors in advanced hepatocellular carcinoma immunotherapy. Front. Immunol. 2022, 13, 1070961. [Google Scholar] [CrossRef]
- Kim, H.; Chung, J.H. PD-L1 Testing in Non-small Cell Lung Cancer: Past, Present, and Future. J. Pathol. Transl. Med. 2019, 53, 199–206. [Google Scholar] [CrossRef]
- Yaghoubi, N.; Soltani, A.; Ghazvini, K.; Hassanian, S.M.; Hashemy, S.I. PD-1/PD-L1 blockade as a novel treatment for colorectal cancer. Biomed. Pharmacother. 2019, 110, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Vranic, S.; Cyprian, F.S.; Gatalica, Z.; Palazzo, J. PD-L1 status in breast cancer: Current view and perspectives. Semin. Cancer Biol. 2021, 72, 146–154. [Google Scholar] [CrossRef]
- Bellmunt, J.; Powles, T.; Vogelzang, N.J. A review on the evolution of PD-1/PD-L1 immunotherapy for bladder cancer: The future is now. Cancer Treat. Rev. 2017, 54, 58–67. [Google Scholar] [CrossRef]
- Shalhout, S.Z.; Emerick, K.S.; Kaufman, H.L.; Miller, D.M. Immunotherapy for Non-melanoma Skin Cancer. Curr. Oncol. Rep. 2021, 23, 125. [Google Scholar] [CrossRef] [PubMed]
- Yi, M.; Niu, M.; Xu, L.; Luo, S.; Wu, K. Regulation of PD-L1 expression in the tumor microenvironment. J. Hematol. Oncol. 2021, 14, 10. [Google Scholar] [CrossRef]
- Lipson, E.J.; Vincent, J.G.; Loyo, M.; Kagohara, L.T.; Luber, B.S.; Wang, H.; Xu, H.; Nayar, S.K.; Wang, T.S.; Sidransky, D.; et al. PD-L1 expression in the Merkel cell carcinoma microenvironment: Association with inflammation, Merkel cell polyomavirus and overall survival. Cancer Immunol. Res. 2013, 1, 54–63. [Google Scholar] [CrossRef]
- Droeser, R.A.; Hirt, C.; Viehl, C.T.; Frey, D.M.; Nebiker, C.; Huber, X.; Zlobec, I.; Eppenberger-Castori, S.; Tzankov, A.; Rosso, R.; et al. Clinical impact of programmed cell death ligand 1 expression in colorectal cancer. Eur. J. Cancer 2013, 49, 2233–2242. [Google Scholar] [CrossRef]
- Velcheti, V.; Schalper, K.A.; Carvajal, D.E.; Anagnostou, V.K.; Syrigos, K.N.; Sznol, M.; Herbst, R.S.; Gettinger, S.N.; Chen, L.; Rimm, D.L. Programmed death ligand-1 expression in non-small cell lung cancer. Lab. Investig. 2014, 94, 107–116. [Google Scholar] [CrossRef]
- Madore, J.; Vilain, R.E.; Menzies, A.M.; Kakavand, H.; Wilmott, J.S.; Hyman, J.; Yearley, J.H.; Kefford, R.F.; Thompson, J.F.; Long, G.V.; et al. PD-L1 expression in melanoma shows marked heterogeneity within and between patients: Implications for anti-PD-1/PD-L1 clinical trials. Pigment. Cell Melanoma Res. 2015, 28, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Boger, C.; Behrens, H.M.; Mathiak, M.; Kruger, S.; Kalthoff, H.; Rocken, C. PD-L1 is an independent prognostic predictor in gastric cancer of Western patients. Oncotarget 2016, 7, 24269–24283. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Chen, R.; Zhang, X.; Fu, R.; Tao, L.; Jia, W. Combined PD-1/PD-L1 and tumor-infiltrating immune cells redefined a unique molecular subtype of high-grade serous ovarian carcinoma. BMC Genom. 2022, 23, 51. [Google Scholar] [CrossRef] [PubMed]
- Wieser, V.; Gaugg, I.; Fleischer, M.; Shivalingaiah, G.; Wenzel, S.; Sprung, S.; Lax, S.F.; Zeimet, A.G.; Fiegl, H.; Marth, C. BRCA1/2 and TP53 mutation status associates with PD-1 and PD-L1 expression in ovarian cancer. Oncotarget 2018, 9, 17501–17511. [Google Scholar] [CrossRef] [PubMed]
- Abiko, K.; Matsumura, N.; Hamanishi, J.; Horikawa, N.; Murakami, R.; Yamaguchi, K.; Yoshioka, Y.; Baba, T.; Konishi, I.; Mandai, M. IFN-gamma from lymphocytes induces PD-L1 expression and promotes progression of ovarian cancer. Br. J. Cancer 2015, 112, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Parra, E.R.; Villalobos, P.; Mino, B.; Rodriguez-Canales, J. Comparison of Different Antibody Clones for Immunohistochemistry Detection of Programmed Cell Death Ligand 1 (PD-L1) on Non-Small Cell Lung Carcinoma. Appl. Immunohistochem. Mol. Morphol. 2018, 26, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Mesnage, S.J.L.; Auguste, A.; Genestie, C.; Dunant, A.; Pain, E.; Drusch, F.; Gouy, S.; Morice, P.; Bentivegna, E.; Lhomme, C.; et al. Neoadjuvant chemotherapy (NACT) increases immune infiltration and programmed death-ligand 1 (PD-L1) expression in epithelial ovarian cancer (EOC). Ann. Oncol. 2017, 28, 651–657. [Google Scholar] [CrossRef] [PubMed]
- Grabosch, S.; Bulatovic, M.; Zeng, F.; Ma, T.; Zhang, L.; Ross, M.; Brozick, J.; Fang, Y.; Tseng, G.; Kim, E.; et al. Cisplatin-induced immune modulation in ovarian cancer mouse models with distinct inflammation profiles. Oncogene 2019, 38, 2380–2393. [Google Scholar] [CrossRef] [PubMed]
- Xue, C.; Xu, Y.; Ye, W.; Xie, Q.; Gao, H.; Xu, B.; Zhang, D.; Jiang, J. Expression of PD-L1 in ovarian cancer and its synergistic antitumor effect with PARP inhibitor. Gynecol. Oncol. 2020, 157, 222–233. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Study | Region | Slide Type | Ab 1 Clone | Ab 1 Manufacturer | Ab Species | Ab Clonality | Scoring Method | Survival Analysis Type | Endpoint |
|---|---|---|---|---|---|---|---|---|---|
| Aust 2017 [10] | Europe | Whole section | E1L3N | Cell Signaling | Rabbit | monoclonal | TC 3 | KM 6 | OS |
| Bansal 2021 [11] | Asia | TMA 2 | SP263 | Ventana (Roche) | Rabbit | monoclonal | CPS 4 | KM 6 | DFS |
| Bas 2021 [12] | Europe | TMA 2 | 22C3 | Dako | Mouse | monoclonal | CPS 4 | KM 6 | OS |
| Chen 2020 [13] | America | Whole section | 22C3 | Dako | Mouse | monoclonal | TC 3 | KM 6 | OS, PFS |
| CPS 4 | KM 6 | OS, PFS | |||||||
| Darb-Esfahani 2015 [14] | Europe | TMA 2 | EPR1161 | Abcam | Rabbit | monoclonal | TC 3 | KM 6 | PFS |
| Cox 7 (multi 9) | OS, PFS | ||||||||
| IC 5 | Cox 7 (multi 9) | OS, PFS | |||||||
| de la Fuente 2020 [22] | Europe | TMA 2 | 22C3 | Dako | Mouse | monoclonal | IC 5 | KM 6 | OS |
| Eymerit-Morin 2021 [15] | Europe | TMA 2 | QR1 | Diagomics | Rabbit | monoclonal | CPS 4 | Cox 7 (uni 8, multi 9) | OS, DFS |
| Farrag 2021 [16] | Africa | N/A | GB11339 | Servicebio | Rabbit | polyclonal | TC 3 | KM 6 | OS, DFS |
| Fucikova 2019 [17] | Europe | Whole section | N/A | N/A | N/A | N/A | TC 3 | KM 6 | RFS |
| Henriksen 2020 [18] | Europe | N/A 2 | SP263 | Ventana (Roche) | Rabbit | monoclonal | TC 3 | KM6 | OS |
| Kim 2018 [19] | Asia | TMA 2 | SP263 | Ventana (Roche) | Rabbit | monoclonal | TC 3 | KM 6 | OS, PFS |
| Lee 2022 [20] | Asia | TMA 2 | 22C3 | Dako | Mouse | monoclonal | CPS 4 | KM 6 | OS, PFS |
| Li 2017 [21] | Asia | TMA 2 | SP263 | Ventana (Roche) | Rabbit | monoclonal | TC 3 | KM 6 | OS |
| Mills 2019 [23] | America | Whole section | SP142 | Spring Bioscience | Rabbit | monoclonal | TC 3, IC 5 | KM 6 | OS |
| Wang 2017 [24] | Asia | Whole section | E1L3N | Cell Signaling | Rabbit | monoclonal | TC 3 | Cox 7 (multi 9) | OS |
| TC 3, IC 5 | KM 6, Cox (multi 9) | OS | |||||||
| Zhang 2023 [25] | Asia | Whole section | 22C3 | Dako | Mouse | monoclonal | TC 3 | Cox 7 (uni 8) | OS |
| TC 3 | KM 6 | RFS | |||||||
| CPS 4 | Cox 7 (uni 8, multi 9) | OS, RFS |
| Study | Scoring Method | Cut-Off | Survival Analysis Type | Survival Endpoint | PD-L1 Positive Rate | HR 1 | SE 2 of ln(HR) | CI 3 | High Stage Only | High Stage Proportion | NACT 4 Included | Slide Type | FDA Approval | Ab Species |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aust 2017 [10] | TC | 1% | KM | OS | 14/20 | 0.36 | 0.51 | 0.13~0.98 | No | N/A | No | Whole section | Not approved | Rabbit |
| Chen 2020 [13] | TC | 1% | KM | OS | 21/100 | 0.37 | 0.36 | 0.18~0.76 | No | 91% | N/A | Whole section | Approved | Mouse |
| Farrag 2021 [16] | TC | 1% | KM | OS | 29/45 | 4.99 | 0.63 | 1.44~17.29 | No | 74% | Yes | N/A | Not approved | Rabbit |
| Henriksen 2020 [18] | TC | 1% | KM | OS | 164/283 | 0.62 | 0.16 | 0.46~0.84 | No | 83% | No | N/A | Approved | Rabbit |
| Kim 2018 [19] | TC | 5% | KM | OS | 36/108 | 1.14 | 0.28 | 0.65~1.98 | Yes | N/A | Yes | TMA | Approved | Rabbit |
| Li 2017 [21] | TC | Custom method | KM | OS | 13/112 | 0.32 | 0.36 | 0.16~0.65 | No | 85% | No | TMA | Approved | Rabbit |
| Wang 2017 [24] | TC | 5% | KM | OS | 26/81 | 1.77 | 0.31 | 0.96~3.24 | No | 76% | No | Whole section | Not approved | Rabbit |
| Zhang 2023 [25] | TC | 1% | KM | OS | 81/212 | 2.05 | 0.2 | 1.37~3.06 | Yes | N/A | No | Whole section | Approved | Mouse |
| Darb-Esfahani 2015 [14] | TC | 0 (any) | Cox (multi) | OS | 178/202 | 0.51 | 0.3 | 0.28~0.91 | No | N/A | No | TMA | Not approved | Rabbit |
| Mills 2019 [23] | TC | 1% | Cox (multi) | OS | 27/93 | 0.61 | 0.43 | 0.26~1.41 | No | 83% | No | Whole section | Not approved | Rabbit |
| Wang 2017 [24] | TC | 5% | Cox (multi) | OS | 26/81 | 1.3 | 0.27 | 0.76~2.21 | No | 76% | No | Whole section | Not approved | Rabbit |
| Zhang 2023 [25] | TC | 1% | Cox (multi) | OS | 81/212 | 1.54 | 0.21 | 1.03~2.32 | Yes | N/A | No | Whole section | Approved | Mouse |
| Chen 2020 [13] | TC | 1% | KM | PFS | 21/100 | 0.5 | 0.27 | 0.29~0.84 | No | 91% | N/A | Whole section | Approved | Mouse |
| Darb-Esfahani 2015 [14] | TC | 0 (any) | KM | PFS | 153/177 | 0.47 | 0.33 | 0.24~0.9 | No | N/A | No | TMA | Not approved | Rabbit |
| Kim 2018 [19] | TC | 5% | KM | PFS | 36/108 | 1.2 | 0.65 | 0.34~4.28 | Yes | N/A | Yes | TMA | Approved | Rabbit |
| Bas 2021 [12] | CPS | 5% | KM | OS | 9/94 | 1.61 | 0.45 | 0.67~3.86 | No | 65% | N/A | TMA | Approved | Mouse |
| Chen 2020 [13] | CPS | 1 | KM | OS | 48/100 | 0.93 | 0.25 | 0.57~1.52 | No | 91% | N/A | Whole section | Approved | Mouse |
| Eymerit-Morin 2021 [15] | CPS | 1 | KM | OS | 22/59 | 0.64 | 0.34 | 0.32~1.25 | No | 60% | Yes | TMA | Not approved | Rabbit |
| Lee 2022 [20] | CPS | 10 | KM | OS | 21/139 | 0.58 | 0.24 | 0.37~0.93 | Yes | N/A | Yes | TMA | Approved | Mouse |
| Zhang 2023 [25] | CPS | 1 | KM | OS | 127/212 | 1.17 | 0.16 | 0.85~1.60 | Yes | N/A | No | Whole section | Approved | Mouse |
| Darb-Esfahani 2015 [14] | IC | 20/mm2 | Cox (multi) | OS | 60/200 | 0.73 | 0.26 | 0.44~1.2 | No | N/A | No | TMA | Not approved | Rabbit |
| de la Fuente 2020 [22] | IC | 1% | Cox (multi) | OS | 26/130 | 0.62 | 0.34 | 0.32~1.2 | Yes | N/A | Yes | TMA | Approved | Mouse |
| Mills 2019 [23] | IC | 1% | Cox (multi) | OS | 70/93 | 1.43 | 0.38 | 0.68~3.0 | No | 83% | No | Whole section | Not approved | Rabbit |
| Survival Type | Scoring | Data Type | Number of Studies | HR 1 | CI 2 | p-Value | I 2 | p-Value |
|---|---|---|---|---|---|---|---|---|
| OS 3 | CPS 5 | KM 8 | 5 | 0.9 | 0.64–1.26 | 0.53 | 54.1 | 0.07 |
| OS 3 | IC 6 | Multi Cox 9 | 3 | 0.82 | 0.54–1.26 | 0.37 | 33.7 | 0.22 |
| OS 3 | TC 7 | Multi Cox 9 | 4 | 0.93 | 0.54–1.62 | 0.81 | 73.5 | 0.01 |
| OS 3 | TC 7 | KM 8 | 8 | 0.9 | 0.48–1.69 | 0.75 | 86.5 | <0.0001 |
| PFS 4 | TC 7 | KM 8 | 3 | 0.53 | 0.35–0.78 | 0.0015 | 0.0 | 0.42 |
| Survival Type | Scoring | Data Type | Subgroup | Number of Studies | HR 1 | CI 2 | p-Value | I 2 | |
|---|---|---|---|---|---|---|---|---|---|
| OS 3 | CPS 4 | KM 6 | FDA approval | Approved | 4 | 0.96 | 0.65–1.40 | 0.82 | 59.1 |
| Not approved | 1 | 0.64 | 0.33–1.25 | 0.19 | |||||
| Stage | High stage only | 2 | 0.84 | 0.42–1.68 | 0.63 | 83.2 | |||
| High and low stage | 3 | 0.92 | 0.64–1.32 | 0.65 | 27.0 | ||||
| NACT | Included | 2 | 0.6 | 0.40–0.88 | 0.009 | 0.0 | |||
| Not included | 1 | 1.17 | 0.86–1.60 | 0.32 | |||||
| Ab species | Mouse | 4 | 0.96 | 0.65–1.40 | 0.82 | 59.1 | |||
| Rabbit | 1 | 0.64 | 0.33–1.25 | 0.19 | |||||
| OS 3 | TC 5 | KM 6 | FDA approval | Approved | 5 | 0.73 | 0.37–1.44 | 0.36 | 89.0 |
| Not approved | 3 | 1.43 | 0.34–6.02 | 0.62 | 82.9 | ||||
| Stage | High stage only | 2 | 1.58 | 0.89–2.80 | 0.12 | 65.2 | |||
| High and low stage | 6 | 0.75 | 0.34–1.65 | 0.47 | 82.3 | ||||
| NACT | Included | 2 | 2.14 | 0.51–8.95 | 0.3 | 78.0 | |||
| Not included | 5 | 0.8 | 0.38–1.71 | 0.57 | 89.5 | ||||
| Ab species | Mouse | 2 | 0.9 | 0.17–4.77 | 0.9 | 94.1 | |||
| Rabbit | 6 | 0.9 | 0.43–1.89 | 0.78 | 82.0 | ||||
| Region | Asia | 4 | 1.1 | 0.49–2.45 | 0.81 | 85.8 | |||
| Europe | 2 | 0.59 | 0.42–0.82 | 0.0017 | 5.4 | ||||
| Africa | 1 | 4.99 | 1.44–17.29 | 0.01 | |||||
| America | 1 | 0.37 | 0.18–0.76 | 0.006 | |||||
| Slide type | Whole slide | 4 | 0.88 | 0.35–2.25 | 0.8 | 87.7 | |||
| TMA | 2 | 0.62 | 0.18–2.14 | 0.45 | 86.9 | ||||
| Survival Type | Scoring | Data Type | Subgroup | Number of Studies | HR 1 | CI 2 | p-Value | I 2 | p-Value | |
|---|---|---|---|---|---|---|---|---|---|---|
| OS | CPS | KM | Stage | High stage only | 2 | 0.84 | 0.42–1.68 | 0.63 | 83.2 | 0.01 |
| High and low stage | 2 | 1.08 | 0.67–1.75 | 0.74 | 13.5 | 0.28 | ||||
| OS | TC | KM | Stage | High stage only | 2 | 1.58 | 0.89–2.80 | 0.12 | 65.2 | 0.09 |
| High and low stage | 3 | 0.46 | 0.30–0.73 | 0.0009 | 49.3 | 0.13 | ||||
| NACT | Included | 1 | 1.14 | 0.66–1.98 | 0.64 | |||||
| Not included | 3 | 0.86 | 0.68–1.08 | 0.61 | 93.3 | <0.0001 | ||||
| Ab species | Mouse | 2 | 1.36 | 0.96–1.92 | 0.9 | 94.1 | <0.0001 | |||
| Rabbit | 3 | 0.65 | 0.32–1.21 | 0.16 | 74.6 | 0.02 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, J.; Han, K.M.; Jung, H.; Kim, H. Prognostic Significance of Programmed Cell Death Ligand 1 Expression in High-Grade Serous Ovarian Carcinoma: A Systematic Review and Meta-Analysis. Diagnostics 2023, 13, 3258. https://doi.org/10.3390/diagnostics13203258
Kang J, Han KM, Jung H, Kim H. Prognostic Significance of Programmed Cell Death Ligand 1 Expression in High-Grade Serous Ovarian Carcinoma: A Systematic Review and Meta-Analysis. Diagnostics. 2023; 13(20):3258. https://doi.org/10.3390/diagnostics13203258
Chicago/Turabian StyleKang, Jeongwan, Kang Min Han, Hera Jung, and Hyunchul Kim. 2023. "Prognostic Significance of Programmed Cell Death Ligand 1 Expression in High-Grade Serous Ovarian Carcinoma: A Systematic Review and Meta-Analysis" Diagnostics 13, no. 20: 3258. https://doi.org/10.3390/diagnostics13203258
APA StyleKang, J., Han, K. M., Jung, H., & Kim, H. (2023). Prognostic Significance of Programmed Cell Death Ligand 1 Expression in High-Grade Serous Ovarian Carcinoma: A Systematic Review and Meta-Analysis. Diagnostics, 13(20), 3258. https://doi.org/10.3390/diagnostics13203258