
Exploring Extended White Blood Cell Parameters for the Evaluation of Sepsis among Patients Admitted to Intensive Care Units

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Collection and Analysis
2.3. Research Cell Population Data Derived from the XN-1000 Haematology Analyzer
2.4. Statistical Analysis
3. Results
3.1. Demographics Data
3.2. Blood Investigation Profiles among Study Participants
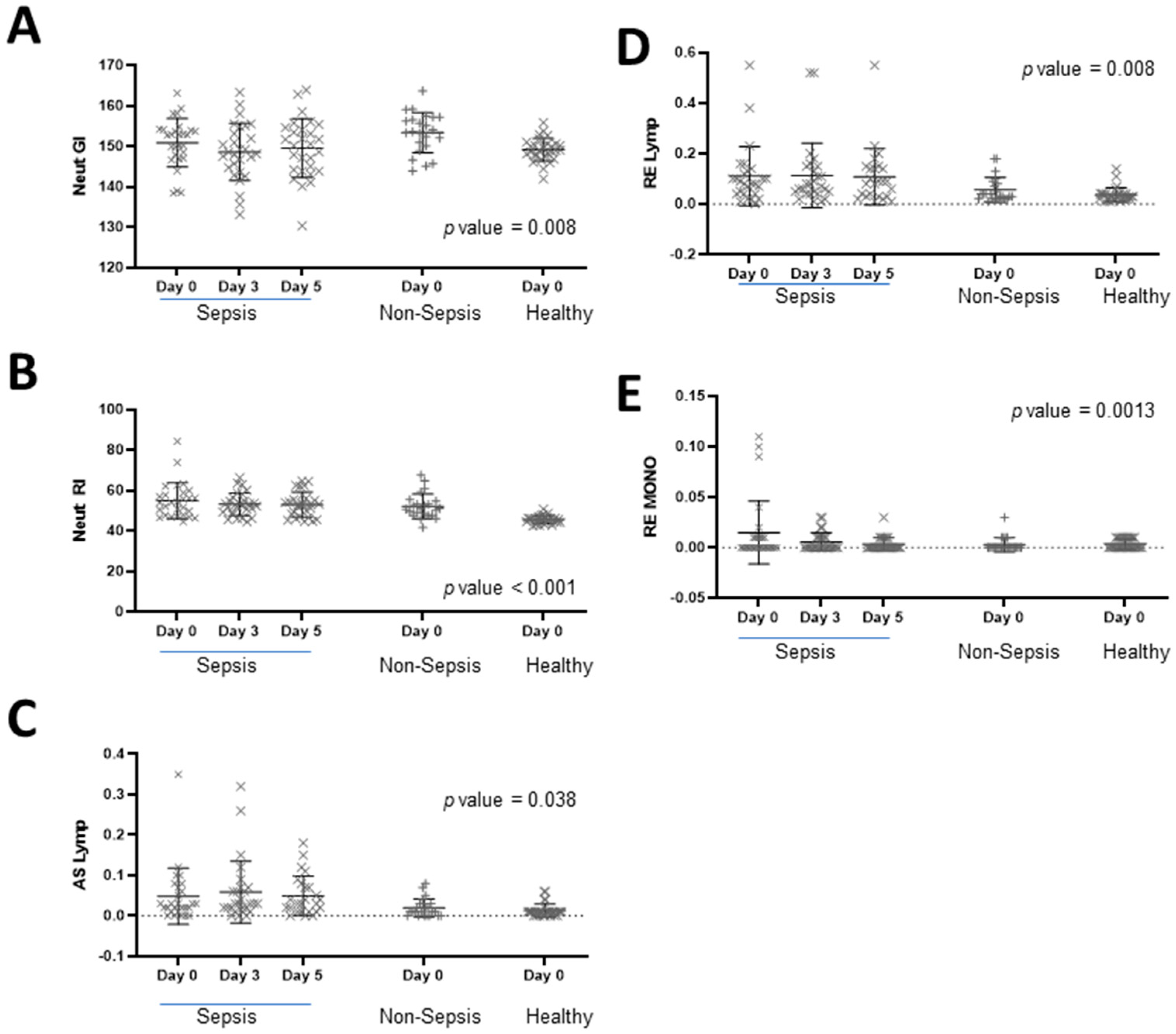
3.3. Haematological Extended Inflammatory Parameters in Culture Negative Septic Patients
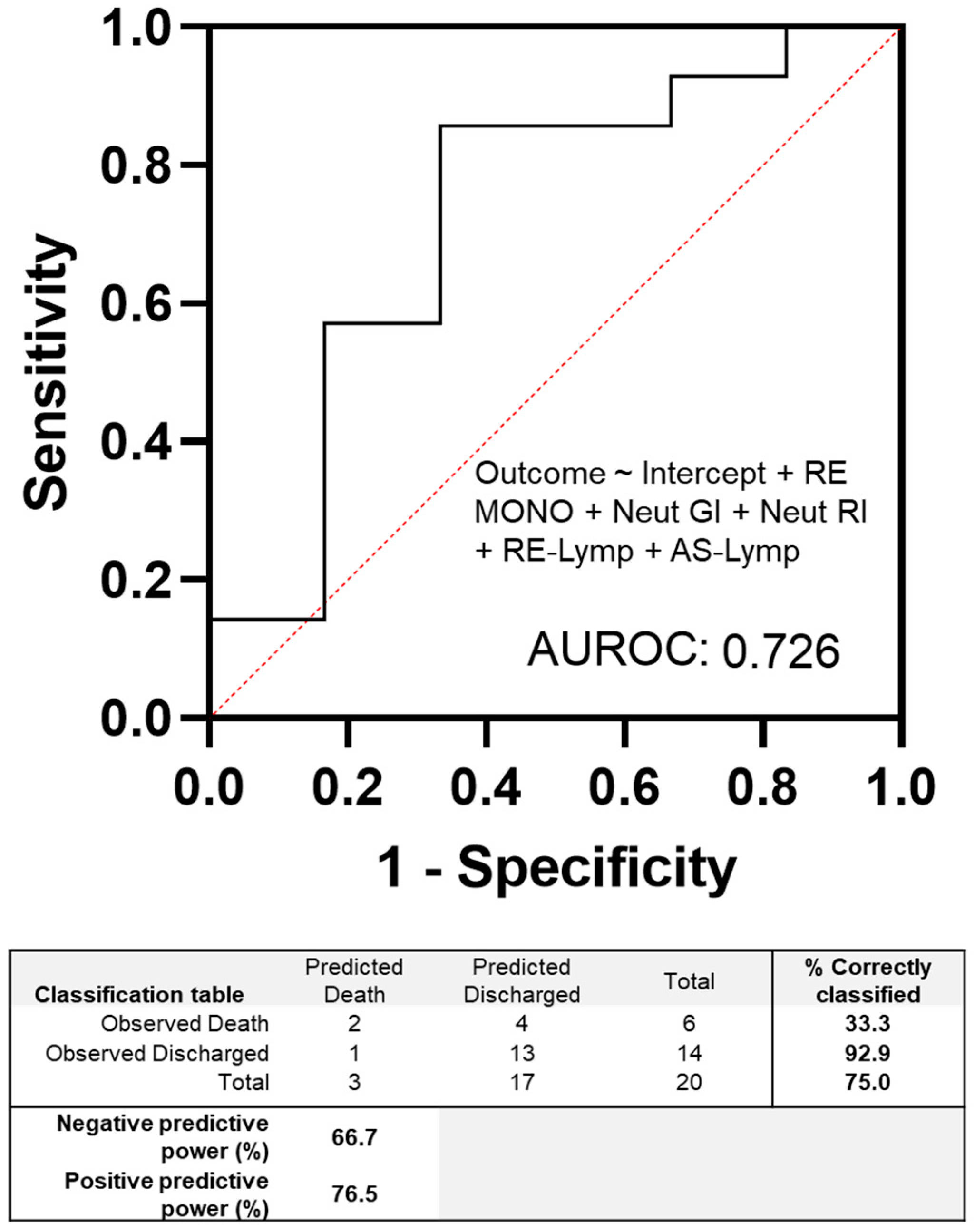
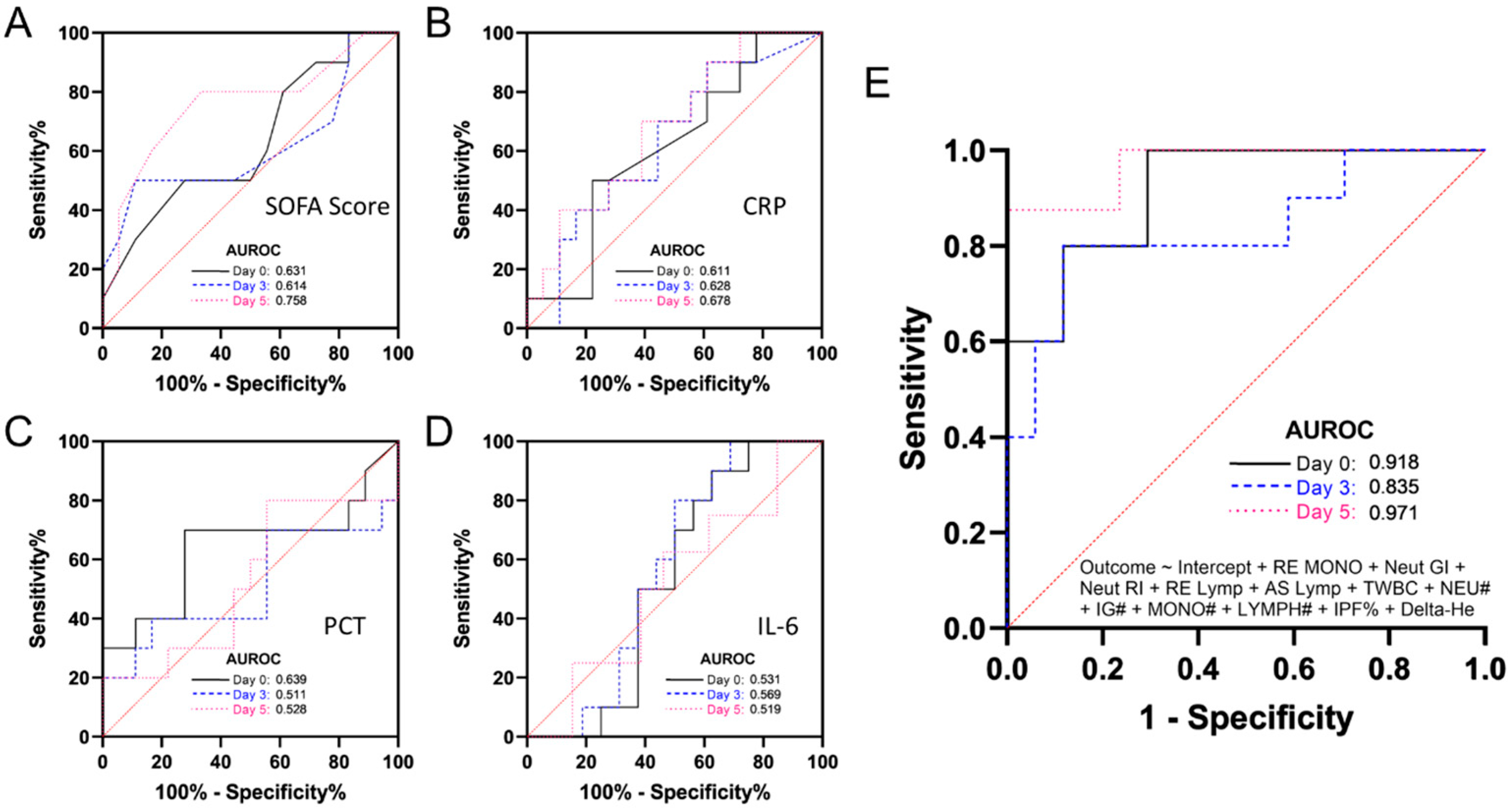
3.4. Evaluating the Discriminatory Power of Haematological Parameters in Comparison to Classical Sepsis Markers
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Developing a new definition and assessing new clinical criteria for septic shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). J. Am. Med. Assoc. 2016, 315, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Marshall, J.C. Sepsis-3: What is the meaning of a definition? Crit. Care Med. 2016, 44, 1459–1460. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Jaschinski, U.; Wittebole, X.; Szakmany, T.; Lipman, J.; Ñamendys-Silva, S.A.; Martin-Loeches, I.; Leone, M.; Lupu, M.-N.; Vincent, J.-L. Sepsis in intensive care unit patients: Worldwide data from the intensive care over nations audit. Open Forum Infect. Dis. 2018, 5, ofy313. [Google Scholar] [CrossRef] [PubMed]
- Marik, P.E.; Taeb, A.M. SIRS, qSOFA and new sepsis definition. J. Thorac. Dis. 2017, 9, 943. [Google Scholar] [CrossRef] [PubMed]
- Lambden, S.; Laterre, P.F.; Levy, M.M.; Francois, B.J.C.C. The SOFA score—Development, utility and challenges of accurate assessment in clinical trials. Crit. Care 2019, 23, 374. [Google Scholar] [CrossRef]
- Lie, K.C.; Lau, C.-Y.; Van Vinh Chau, N.; West, T.E.; Limmathurotsakul, D. Utility of SOFA score, management and outcomes of sepsis in Southeast Asia: A multinational multicenter prospective observational study. J. Intensiv. Care 2018, 6, 9. [Google Scholar] [CrossRef]
- Castelli, G.; Pognani, C.; Cita, M.; Stuani, A.; Sgarbi, L.; Paladini, R. Procalcitonin, C-reactive protein, white blood cells and SOFA score in ICU: Diagnosis and monitoring of sepsis. Minerva Anestesiol. 2006, 72, 69. [Google Scholar]
- Guido, M.; Quattrocchi, M.; Zizza, A.; Pasanisi, G.; Pavone, V.; Lobreglio, G.; Gabutti, G.; De Donno, M.A. Molecular approaches in the diagnosis of sepsis in neutropenic patients with haematological malignances. J. Prev. Med. Hyg. 2012, 53, 104–108. [Google Scholar]
- Long, Y.; Zhang, Y.; Gong, Y.; Sun, R.; Su, L.; Lin, X.; Shen, A.; Zhou, J.; Caiji, Z.; Wang, X. Diagnosis of sepsis with cell-free DNA by next-generation sequencing technology in ICU patients. Arch. Med. Res. 2016, 47, 365–371. [Google Scholar] [CrossRef]
- Lee, K.; Chang, J.-P.; Huang, W.-C.; Tai, C.-H.; Wu, H.-T.; Chi, C.-H. Immunology; Infection. Comparative of clinical performance between next-generation sequencing and standard blood culture diagnostic method in patients suffering from sepsis. J. Microbiol. Immunol. Infect. 2022, 55, 845–852. [Google Scholar] [CrossRef]
- Henriquez-Camacho, C.; Losa, J. Biomarkers for sepsis. BioMed Res. Int. 2014, 2014, 547818. [Google Scholar] [CrossRef]
- Tsalik, E.L.; Jaggers, L.B.; Glickman, S.W.; Langley, R.J.; van Velkinburgh, J.C.; Park, L.P.; Fowler, V.G.; Cairns, C.B.; Kingsmore, S.F.; Woods, C.W. Discriminative value of inflammatory biomarkers for suspected sepsis. J. Emerg. Med. 2012, 43, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Gaieski, D.F.; Drumheller, B.C.; Goyal, M.; Fuchs, B.D.; Shofer, F.S.; Zogby, K. Accuracy of handheld point-of-care fingertip lactate measurement in the emergency department. West. J. Emerg. Med. 2013, 14, 58. [Google Scholar] [CrossRef] [PubMed]
- Haydar, S.A.; Moore, E.T.; Higgins III, G.L.; Irish, C.B.; Owens, W.B.; Strout, T.D. Effect of bedside ultrasonography on the certainty of physician clinical decisionmaking for septic patients in the emergency department. Ann. Emerg. Med. 2012, 60, 346–358.e344. [Google Scholar] [CrossRef] [PubMed]
- Barati, M.; Alinejad, F.; Bahar, M.A.; Tabrisi, M.S.; Shamshiri, A.R.; Karimi, H. Comparison of WBC, ESR, CRP and PCT serum levels in septic and non-septic burn cases. Burns 2008, 34, 770–774. [Google Scholar] [CrossRef]
- Lee, C.-C.; Chen, S.-Y.; Tsai, C.-L.; Wu, S.-C.; Chiang, W.-C.; Wang, J.-L.; Sun, H.-Y.; Chen, S.-C.; Chen, W.-J.; Hsueh, P.-R. Prognostic value of mortality in emergency department sepsis score, procalcitonin, and C-reactive protein in patients with sepsis at the emergency department. Shock 2008, 29, 322–327. [Google Scholar] [CrossRef] [PubMed]
- Streeton, J.; Desem, N.; Jones, S. Sensitivity and specificity of a gamma interferon blood test for tuberculosis infection. Int. J. Tuberc. Lung Dis. 1998, 2, 443–450. [Google Scholar]
- Tan, S.J.; Yeo, T.; Sukhatme, S.A.; Kong, S.L.; Lim, W.-T.; Lim, C.T. Personalized treatment through detection and monitoring of genetic aberrations in single circulating tumor cells. In Isolation and Molecular Characterization of Circulating Tumor Cells; Springer: Cham, Switzerland, 2017; pp. 255–273. [Google Scholar]
- Maecker, H.T.; Lindstrom, T.M.; Robinson, W.H.; Utz, P.J.; Hale, M.; Boyd, S.D.; Shen-Orr, S.S.; Fathman, C.G.J.N.R.R. New tools for classification and monitoring of autoimmune diseases. Nat. Rev. Rheumatol. 2012, 8, 317–328. [Google Scholar] [CrossRef]
- Guerrero, R.B.; Salazar, D.; Tanpaiboon, P. Laboratory diagnostic approaches in metabolic disorders. Ann. Transl. Med. 2018, 6, 470. [Google Scholar] [CrossRef]
- Briggs, C.; Longair, I.; Kumar, P.; Singh, D.; Machin, S.J. Performance evaluation of the Sysmex haematology XN modular system. J. Clin. Pathol. 2012, 65, 1024–1030. [Google Scholar] [CrossRef]
- Roshan, T.; Rosline, H.; Ahmed, S.; Rapiaah, M.; Wan Zaidah, A.; Khattak, M. Hematological reference values of healthy Malaysian population. Int. J. Lab. Hematol. 2009, 31, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Ehram, J.; Kamaliah, M.; Shukeri, M.; Rosline, H.; Marini, R. Detection of Iron Deficiency Anaemia by Reticulocyte Haemoglobin (RET-He) in Haemodialysis Patients on Recombinant Human Erythropoietin (rHuEPO). Int. Med. J. 2020, 27, 308–311. [Google Scholar]
- Urrechaga, E.; Bóveda, O.; Aguirre, U. Role of leucocytes cell population data in the early detection of sepsis. J. Clin. Pathol. 2017, 71, 259–266. [Google Scholar] [CrossRef] [PubMed]
- Cornet, E.; Boubaya, M.; Troussard, X. Contribution of the new XN-1000 parameters NEUT-RI and NEUT-WY for managing patients with immature granulocytes. Int. J. Lab. Hematol. 2015, 37, e123–e126. [Google Scholar] [CrossRef] [PubMed]
- Dugar, S.; Choudhary, C.; Duggal, A. Sepsis and septic shock: Guideline-based management. Clevel. Clin. J. Med. 2020, 87, 53–64. [Google Scholar] [CrossRef]
- Clifford, K.M.; Dy-Boarman, E.A.; Haase, K.K.; Maxvill, K.; Pass, S.E.; Alvarez, C.A. Challenges with diagnosing and managing sepsis in older adults. Expert Rev. Anti-Infect. Ther. 2016, 14, 231–241. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Zubert, S.; Funk, D.J.; Kumar, A. Antibiotics in sepsis and septic shock: Like everything else in life, timing is everything. Crit. Care Med. 2010, 38, 1211–1212. [Google Scholar] [CrossRef]
- Goyette, R.E.; Key, N.S.; Ely, E.W. Hematologic changes in sepsis and their therapeutic implications. Semin. Respir. Crit. Care Med. 2004, 25, 645–659. [Google Scholar] [CrossRef]
- van der Geest, P.J.; Mohseni, M.; Linssen, J.; Duran, S.; de Jonge, R.; Groeneveld, A. The intensive care infection score–a novel marker for the prediction of infection and its severity. Crit. Care 2016, 20, 180. [Google Scholar] [CrossRef] [PubMed]
- Kaeslin, M.; Brunner-Agten, S.; Raths, J.; Huber, A. Improvement in detecting bacterial infection in lower respiratory tract infections using the Intensive Care Infection Score (ICIS). J. Lab. Med. 2016, 40, 175–182. [Google Scholar] [CrossRef]
- Jha, B.; Goel, S.; Singh, M.K.; Sethi, M.; Deswal, V.; Kataria, S.; Mehta, Y.; Saxena, R. Value of new advanced hematological parameters in early prediction of severity of COVID-19. Int. J. Lab. Hematol. 2023, 45, 282–288. [Google Scholar] [CrossRef] [PubMed]
- Khodaiji, S.; Jacob, B.; Mansukhani, D. Hematology parameters aid to differentiate Indian SARS-CoV-2 positive patients from suspected cases. Acad. Lett. 2021, 2, 1552. [Google Scholar] [CrossRef]
- Meisner, M.; Tschaikowsky, K.; Palmaers, T.; Schmidt, J. Comparison of procalcitonin (PCT) and C-reactive protein (CRP) plasma concentrations at different SOFA scores during the course of sepsis and MODS. Crit. Care 1999, 3, 1–6. [Google Scholar] [CrossRef]
- Nierhaus, A.; Linssen, J.; Wichmann, D.; Braune, S.; Kluge, S. Use of a Weighted, Automated Analysis of the Differential Blood Count to Differentiate Sepsis from Non-Infectious Systemic Inflammation: The Intensive Care Infection Score (ICIS). Inflamm. Allergy-Drug Targets 2012, 11, 109–115. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Sepsis (n = 30) | Control Arm | p Value | |
|---|---|---|---|---|
| Non-Sepsis (n = 23) | Healthy (n = 30) | |||
| Age(year) | 58 (13) | 49 (16) | 34 (13) | |
| Gender | ||||
| Female | 14 (46.7%) | 9 (39.1%) | 10 (33.3%) | |
| Male | 16 (53.3%) | 14 (60.9%) | 20 (66.7%) | |
| Blood Culture | ||||
| Positive | 7 (23.3%) | 0 | NA | |
| Negative | 23 (76.7%) | 23 (100%) | NA | |
| Clinical Outcome | ||||
| Death | 10 (33.3%) | 0 | NA | |
| Discharged | 20 (66.7%) | 23 (100%) | NA | |
| Laboratory Results | ||||
| SOFA | 7.10 (3.02) | 0.96 (0.21) | 0.00 (0.00) | <0.001 |
| CRP (mg/L) | 142.60 (47.85) | 75.84 (57.69) | 0.50 (0.00) | <0.001 |
| PCT (ng/mL) | 26.45 (36.63) | 0.25 (0.11) | 0.10 (0.00) | <0.001 |
| IL-6 (pg/mL) | 59.02 (42.07) | 28.34 (37.17) | 1.56 (0.00) | <0.001 |
| TWBC (103/μL) | 13.82 (5.50) | 13.00 (4.99) | 7.05 (1.87) | <0.001 |
| NEUT# (103/μL) | 12.26 (5.71) | 10.88 (4.56) | 3.85 (1.37) | <0.001 |
| NEUT-GI (SI) | 150.80 (5.97) | 153.33 (4.98) | 149.13 (2.80) | 0.008 |
| NEUT-RI (FI) | 56.49 (10.36) | 52.20 (6.15) | 45.61 (1.89) | <0.001 |
| IG# (103/μL) | 0.47 (0.77) | 0.17 (0.22) | 0.05 (0.03) | 0.004 |
| MONO# (103/μL) | 0.73 (0.31) | 0.85 (0.53) | 0.53 (0.17) | 0.004 |
| LYMPH# (103/μL) | 1.04 (0.52) | 1.18 (0.54) | 2.30 (0.57) | <0.001 |
| RE-LYMP (103/μL) | 0.11 (0.11) | 0.06 (0.05) | 0.04 (0.03) | 0.001 |
| AS-LYMP (cells/μL) | 0.05 (0.07) | 0.02 (0.02) | 0.01 (0.02) | 0.014 |
| PLT# (103/μL) | 197.77 (109.92) | 282.65 (123.12) | 292.83 (78.68) | 0.001 |
| IPF % | 5.69 (4.32) | 3.27 (2.06) | 4.09 (2.45) | 0.021 |
| Delta-He (pg) | 0.14 (3.62) | 2.01 (2.19) | 2.85 (1.73) | 0.001 |
| NE-WX (ch) | 338.57 (33.96) | 314.65 (17.00) | 314.77 (10.94) | <0.001 |
| NE-WY (ch) | 750.87 (175.04) | 673.78 (91.44) | 601.30 (24.55) | <0.001 |
| NE-WZ (ch) | 659.67 (48.42) | 606.22 (26.48) | 634.93 (27.51) | <0.001 |
| RE-MONO# (103/μL) | 0.015 (0.030) | 0.003 (0.007) | 0.004 (0.005) | 0.037 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, S.F.; Tan, S.J.; Mazlan, M.Z.; Iberahim, S.; Lee, Y.X.; Hassan, R. Exploring Extended White Blood Cell Parameters for the Evaluation of Sepsis among Patients Admitted to Intensive Care Units. Diagnostics 2023, 13, 2445. https://doi.org/10.3390/diagnostics13142445
Ho SF, Tan SJ, Mazlan MZ, Iberahim S, Lee YX, Hassan R. Exploring Extended White Blood Cell Parameters for the Evaluation of Sepsis among Patients Admitted to Intensive Care Units. Diagnostics. 2023; 13(14):2445. https://doi.org/10.3390/diagnostics13142445
Chicago/Turabian StyleHo, Sook Fong, Swee Jin Tan, Mohd Zulfakar Mazlan, Salfarina Iberahim, Ying Xian Lee, and Rosline Hassan. 2023. "Exploring Extended White Blood Cell Parameters for the Evaluation of Sepsis among Patients Admitted to Intensive Care Units" Diagnostics 13, no. 14: 2445. https://doi.org/10.3390/diagnostics13142445
APA StyleHo, S. F., Tan, S. J., Mazlan, M. Z., Iberahim, S., Lee, Y. X., & Hassan, R. (2023). Exploring Extended White Blood Cell Parameters for the Evaluation of Sepsis among Patients Admitted to Intensive Care Units. Diagnostics, 13(14), 2445. https://doi.org/10.3390/diagnostics13142445