
Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism



Abstract
1. Introduction
Aim
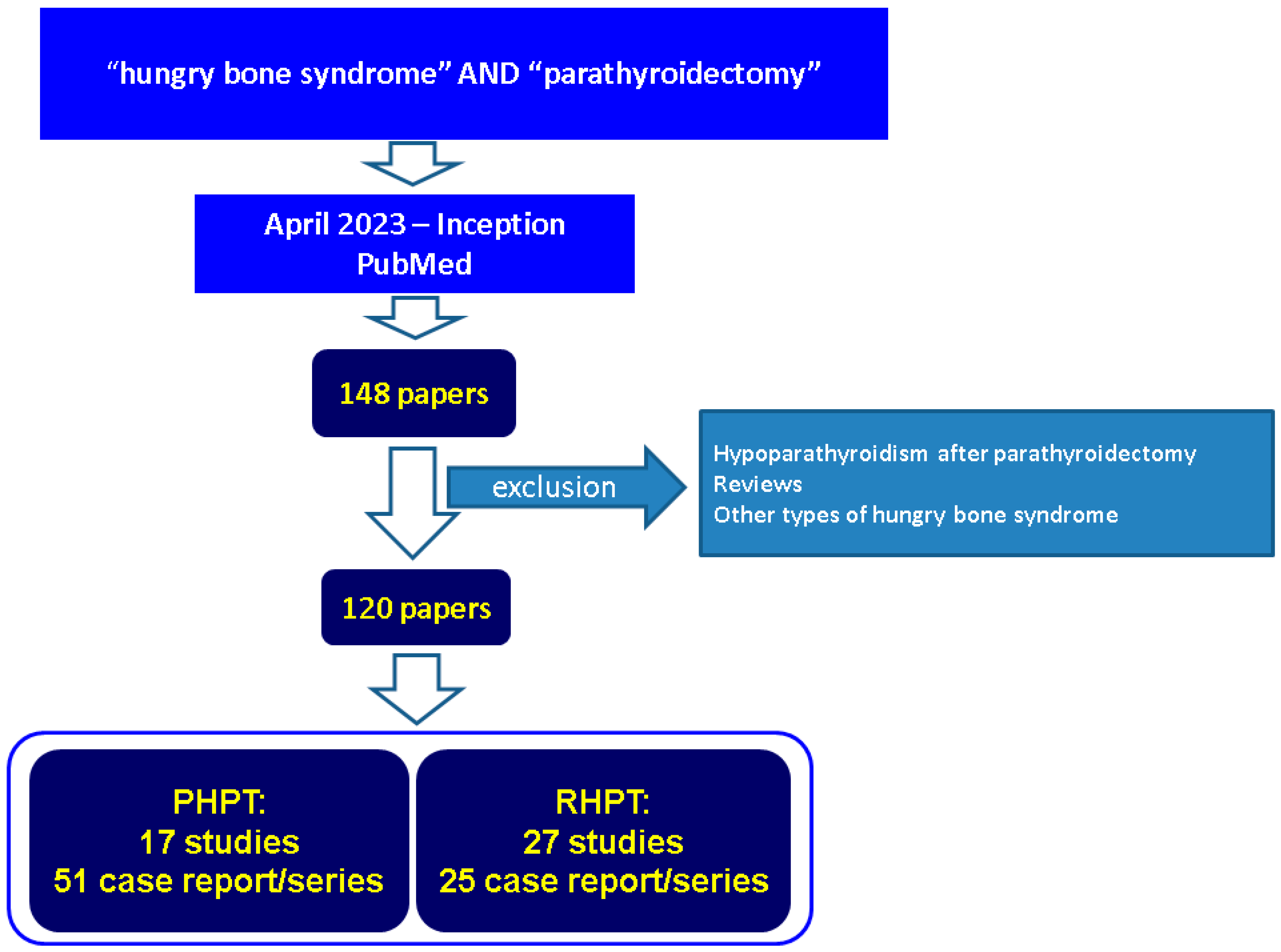
2. Methods
3. PTx-Related HBS
3.1. Pre-Operatory Predictors of HBS in PHPT
3.2. Pediatric PHPT and HBS
3.3. Pre-Operatory HBS Predictors in Subjects with RPHT
3.4. Post-Operatory Findings in RHPT: Focus on HBS
3.5. Outcome and Management in RHPT-Related HBS
4. Discussion
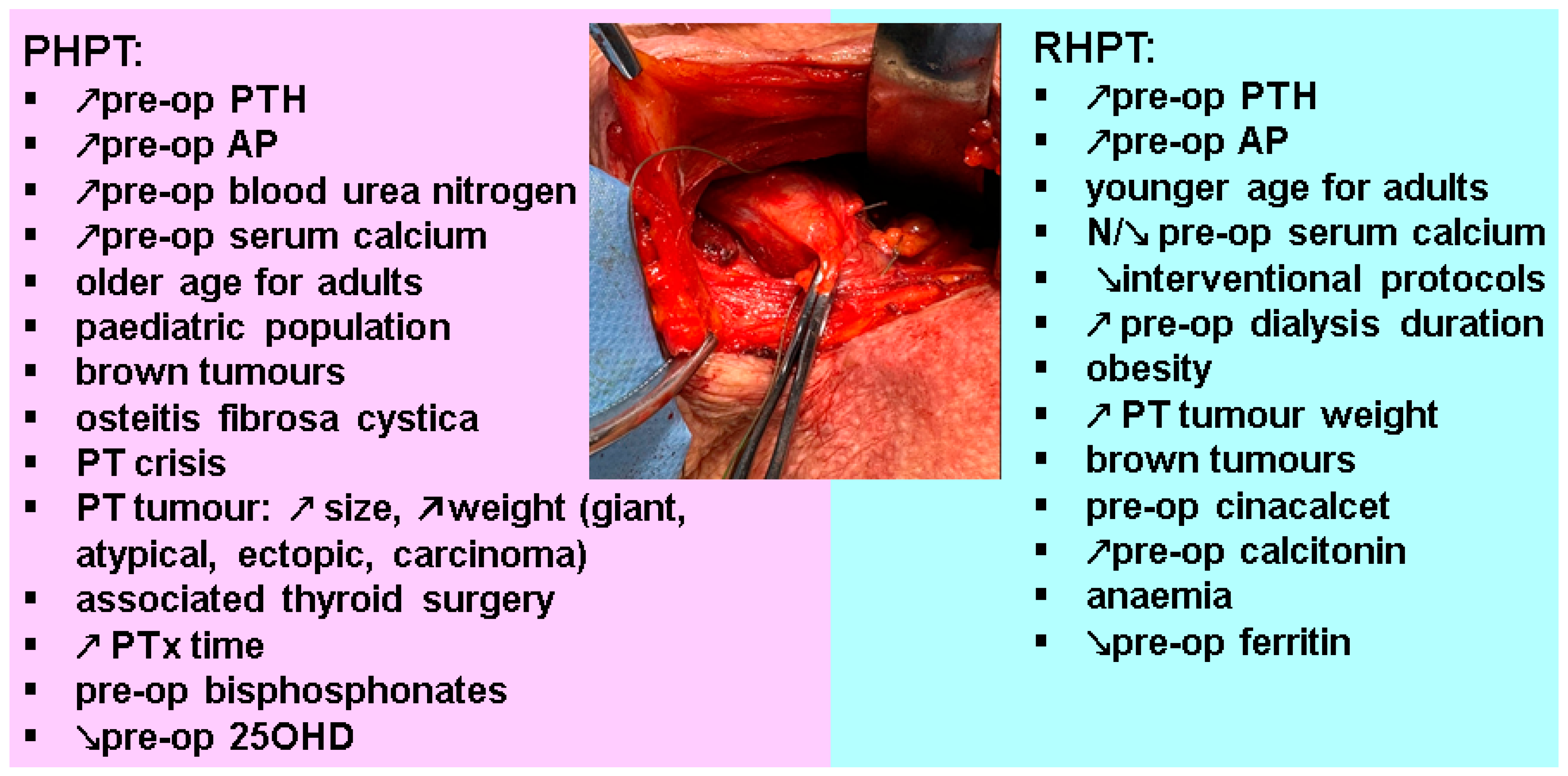
4.1. Panel of Investigations in PHPT and RHPT as Clues for HBS
4.2. Surgical Procedures
4.3. Individual Decision or Protocol-Based Management in HBS
4.4. Differential Diagnostic of Post-PTx Hypocalcemia
4.5. Integrating PTx-Related HBS to Non-PTx Causes of HBS
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AP | alkaline phosphatase |
| ERAS | enhanced recovery after surgery |
| FGF-23 | Fibroblast Growth Factor-23 |
| m-TOEPVA | transoral endoscopic parathyroidectomy vestibular approach |
| PT | parathyroid |
| PTH | parathormone (parathyroid hormone) |
| PTx | parathyroidectomy |
| RHPT | renal hyperparathyroidism |
| PHPT | primary hyperparathyroidism |
References
- Stefanova, D.; Ullmann, T.M.; Limberg, J.; Moore, M.; Beninato, T.; Zarnegar, R.; Fahey, T.J.; Finnerty, B.M. Risk Factors for Prolonged Length of Stay and Readmission After Parathyroidectomy for Renal Secondary Hyperparathyroidism. World J. Surg. 2020, 44, 3751–3760. [Google Scholar] [CrossRef] [PubMed]
- Lau, W.L.; Obi, Y.; Kalantar-Zadeh, K. Parathyroidectomy in the Management of Secondary Hyperparathyroidism. Clin. J. Am. Soc. Nephrol. 2018, 13, 952–961. [Google Scholar] [CrossRef] [PubMed]
- Jain, N.; Reilly, R.F. Hungry bone syndrome. Curr. Opin. Nephrol. Hypertens. 2017, 26, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Tai, Y.L.; Shen, H.Y.; Nai, W.H.; Fu, J.F.; Wang, I.K.; Huang, C.C.; Weng, C.H.; Lee, C.C.; Huang, W.H.; Yang, H.Y.; et al. Hungry bone syndrome after parathyroid surgery. Hemodial. Int. 2023, 27, 134–145. [Google Scholar] [CrossRef] [PubMed]
- Nistor, C.E.; Stanciu-Găvan, C.; Vasilescu, F.; Dumitru, A.V.; Ciuche, A. Attitude of the surgical approach in hyperparathyroidism: A retrospective study. Exp. Ther. Med. 2021, 22, 959. [Google Scholar] [CrossRef]
- Prasarttong-Osoth, P.; Wathanaoran, P.; Imruetaicharoenchoke, W.; Rojananin, S. Primary hyperparathyroidism: 11-year experience in a single institute in Thailand. Int. J. Endocrinol. 2012, 2012, 952426. [Google Scholar] [CrossRef]
- Alvarez-Payares, J.C.; Ribero, M.E.; Ramírez-Urrea, S.; Fragozo-Ramos, M.C.; Agámez-Gómez, J.E.; Román-González, A.; Arias, L.F.; Arenas, R.B.; López-Urbano, F. Giant Parathyroid Adenoma-Associated Fracture, Not All Lytic Bone Lesions are Cancer: A Case-Based Review. Case Rep. Med. 2022, 2022, 3969542. [Google Scholar] [CrossRef]
- Hernandez, P.M.; Enos, B.D.; Labarca, T.G.; Vanderstelt, A.G. From the Old, the Best: Parathyroidectomy in the Management of Soft-Tissue and Vascular Calcification in Patients with Chronic Renal Disease. Case Rep. Nephrol. 2021, 2021, 9985308. [Google Scholar] [CrossRef]
- Shavit, L.; Lifschitz, M.; Slotki, I. Prolonged hypophosphatemia following parathyroidectomy in chronic hemodialysis patients. Clin. Nephrol. 2012, 78, 399–405. [Google Scholar] [CrossRef]
- Florakis, D.; Karakozis, S.; Tseleni-Balafouta, S.; Makras, P. Lessons learned from the management of Hungry Bone Syndrome following the removal of an Atypical Parathyroid Adenoma. J. Musculoskelet. Neuronal Interact. 2019, 19, 379–384. [Google Scholar]
- Sandoval, M.A.; Paz-Pacheco, E. Primary hyperparathyroidism with classic and severe skeletal involvement. BMJ Case Rep. 2010, 2010, bcr0420102929. [Google Scholar] [CrossRef] [PubMed]
- Valea, A.; Ghemigian, A.; Radoi, V.; Carsote, M. Persistent post-operative hypoparathyroidism: Cardiac and psychiatric co-morbidities need to be correlated with vitamin D and calcium replacement. Arch. Balk. Med. Union 2016, 51, 425–428. [Google Scholar]
- Fackelmayer, O.J.; Wu, J.X.; Yeh, M.W. Endocrine Surgery: Management of Postoperative Complications Following Endocrine Surgery of the Neck. Surg. Clin. N. Am. 2021, 101, 767–784. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Fujikawa, P.; Brand, K.; Munshi, V.; Patel, K. Giant Parathyroid Adenoma: A Case Report. Cureus 2023, 15, e34140. [Google Scholar] [CrossRef] [PubMed]
- Morrone, L.F.; Tampoia, M.; Pansini, N.; Gesualdo, L. Kinetics of the circulating levels of bone alkaline phosphatase in a case of hungry bone disease following total parathyroidectomy. Ann. Ital. Med. Int. 2004, 19, 189–192. [Google Scholar] [PubMed]
- Pal, R.; Gautam, A.; Bhadada, S.K. Role of Bisphosphonates in The Prevention of Postoperative Hungry Bone Syndrome in Primary Hyperparathyroidism: A Meta-Analysis and Need for Randomized Controlled Trials. Drug Res. 2021, 71, 108–109. [Google Scholar] [CrossRef]
- Davenport, A.; Stearns, M.P. Administration of pamidronate helps prevent immediate postparathyroidectomy hungry bone syndrome. Nephrology 2007, 12, 386–390. [Google Scholar] [CrossRef]
- Carsote, M.; Paduraru, D.N.; Nica, A.E.; Valea, A. Parathyroidectomy: Is vitamin D a player for a good outcome? J. Med. Life 2016, 9, 348–352. [Google Scholar]
- Corsello, S.M.; Paragliola, R.M.; Locantore, P.; Ingraudo, F.; Ricciato, M.P.; Rota, C.A.; Senes, P.; Pontecorvi, A. Post-surgery severe hypocalcemia in primary hyperparathyroidism preoperatively treated with zoledronic acid. Hormones 2010, 9, 338–342. [Google Scholar] [CrossRef]
- Schnyder, M.A.; Stolzmann, P.; Huber, G.F.; Schmid, C. A patient with a history of breast cancer and multiple bone lesions: A case report. J. Med. Case Rep. 2017, 11, 127. [Google Scholar] [CrossRef][Green Version]
- Stanciu, M.; Boicean, L.C.; Popa, F.L. The role of combined techniques of scintigraphy and SPECT/CT in the diagnosis of primary hyperparathyroidism: A case report. Medicine 2019, 98, 14154. [Google Scholar] [CrossRef] [PubMed]
- Habas, E.S.; Eledrisi, M.; Khan, F.; Elzouki, A.Y. Secondary Hyperparathyroidism in Chronic Kidney Disease: Pathophysiology and Management. Cureus 2021, 13, e16388. [Google Scholar] [CrossRef] [PubMed]
- Steinl, G.K.; Kuo, J.H. Surgical Management of Secondary Hyperparathyroidism. Kidney Int. Rep. 2020, 6, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ortiz, M.E.; Pendón-Ruiz de Mier, M.V.; Rodríguez, M. Parathyroidectomy in dialysis patients: Indications, methods, and consequences. Semin. Dial. 2019, 32, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Hassanein, M.; Laird-Fick, H.; Tikaria, R.; Aldasouqi, S. Removing the problem: Parathyroidectomy for calciphylaxis. BMJ Case Rep. 2018, 11, e226696. [Google Scholar] [CrossRef]
- Anwar, F.; Abraham, J.; Nakshabandi, A.; Lee, E. Treatment of hypocalcemia in hungry bone syndrome: A case report. Int. J. Surg. Case Rep. 2018, 51, 335–339. [Google Scholar] [CrossRef]
- Headley, C.M. Hungry bone syndrome following parathyroidectomy. ANNA J. 1998, 25, 283–289. [Google Scholar]
- Graal, M.B.; Wolffenbuttel, B.H. Consequences of long-term hyperparathyroidism. Neth. J. Med. 1998, 53, 37–42. [Google Scholar] [CrossRef]
- Kaye, M. Hungry bone syndrome after surgical parathyroidectomy. Am. J. Kidney Dis. 1997, 30, 730–731. [Google Scholar] [CrossRef]
- Tanweer, F.; Liu, P.Z.; Vakharia, N.; Whitcroft, K. Prospective Audit and Review of Parathyroid Surgery in Rural Setting. Indian J. Otolaryngol. Head Neck Surg. 2022, 74 (Suppl. S2), 2513–2519. [Google Scholar] [CrossRef]
- Radu, C.P.; Daniealopol, V.; Santini, A.; Darie, R.; Sala, D.T. Fatal Hypocalcaemia Due to Hungry Bone Syndrome with Secondary Refractory HyperParathyroidism After Parathyroidectomy: A Case Report. J. Crit. Care Med. 2019, 5, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Pappachan, J.M.; Lahart, I.M.; Viswanath, A.K.; Borumandi, F.; Sodi, R.; Metzendorf, M.I.; Bongaerts, B. Parathyroidectomy for adults with primary hyperparathyroidism. Cochrane Database Syst. Rev. 2023, 3, CD013035. [Google Scholar] [CrossRef] [PubMed]
- das Neves, M.C.; Santos, R.O.; Ohe, M.N. Surgery for primary hyperparathyroidism. Arch. Endocrinol. Metab. 2022, 66, 678–688. [Google Scholar] [CrossRef]
- Tang, A.L.; Aunins, B.; Chang, K.; Wang, J.C.; Hagen, M.; Jiang, L.; Lee, C.Y.; Randle, R.W.; Houlton, J.J.; Sloan, D.; et al. A multi-institutional study evaluating and describing atypical parathyroid tumors discovered after parathyroidectomy. Laryngoscope Investig. Otolaryngol. 2022, 7, 901–905. [Google Scholar] [CrossRef]
- Chandran, M.; Bilezikian, J.P.; Salleh, N.M.; Ying, H.; Lau, J.; Lee, J.; deJong, M.C.; Chan Maung, A.; Parameswaran, R. Hungry bone syndrome following parathyroidectomy for primary hyperparathyroidism in a developed country in the Asia Pacific. A cohort study. Osteoporos. Sarcopenia 2022, 8, 11–16. [Google Scholar] [CrossRef]
- Nouikes Zitouni, S. Monocentric experience of primary hyperparathyroidism surgery in Algeria. Surg. Open Sci. 2021, 4, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Salman, M.A.; Rabiee, A.; Salman, A.A.; Youssef, A.; Shaaban, H.E.; Ftohy, T.; Maurice, K.K.; Balamoun, H. Role of vitamin D supplements in prevention of hungry bone syndrome after successful parathyroidectomy for primary hyperparathyroidism: A prospective study. Scand. J. Surg. 2021, 110, 329–334. [Google Scholar] [CrossRef]
- Guillén Martínez, A.J.; Smilg Nicolás, C.; Moraleda Deleito, J.; Guillén Martínez, S.; García-Purriños García, F. Risk factors and evolution of calcium and parathyroid hormone levels in hungry bone syndrome after parthyroidectomy for primary hyperparathyroidism. Endocrinol. Diabetes Nutr. 2020, 67, 310–316. [Google Scholar] [CrossRef]
- Jakubauskas, M.; Beiša, V.; Strupas, K. Risk factors of developing the hungry bone syndrome after parathyroidectomy for primary hyperparathyroidism. Acta Med. Litu. 2018, 25, 45–51. [Google Scholar] [CrossRef]
- Kaderli, R.M.; Riss, P.; Dunkler, D.; Pietschmann, P.; Selberherr, A.; Scheuba, C.; Niederle, B. The impact of vitamin D status on hungry bone syndrome after surgery for primary hyperparathyroidism. Eur. J. Endocrinol. 2018, 178, 1–9. [Google Scholar] [CrossRef]
- Kaderli, R.M.; Riss, P.; Geroldinger, A.; Selberherr, A.; Scheuba, C.; Niederle, B. Primary hyperparathyroidism: Dynamic postoperative metabolic changes. Clin. Endocrinol. 2018, 88, 129–138. [Google Scholar] [CrossRef]
- Mayilvaganan, S.; Vijaya Sarathi, H.A.; Shivaprasad, C. Indian Preoperative zoledronic acid therapy prevent hungry bone syndrome in patients with primary hyperparathyroidism. J. Endocrinol. Metab. 2017, 21, 76–79. [Google Scholar] [CrossRef]
- Kaya, C.; Tam, A.A.; Dirikoç, A.; Kılıçyazgan, A.; Kılıç, M.; Türkölmez, Ş.; Ersoy, R.; Çakır, B. Hypocalcemia development in patients operated for primary hyperparathyroidism: Can it be predicted preoperatively? Arch. Endocrinol. Metab. 2016, 60, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Malabu, U.H.; Founda, M.A. Primary hyperparathyroidism in Saudi Arabia: A review of 46 cases. Med. J. Malays. 2007, 62, 394–397. [Google Scholar]
- Lee, I.T.; Sheu, W.H.; Tu, S.T.; Kuo, S.W.; Pei, D. Bisphosphonate pretreatment attenuates hungry bone syndrome postoperatively in subjects with primary hyperparathyroidism. J. Bone Miner. Metab. 2006, 24, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Brasier, A.R.; Nussbaum, S.R. Hungry bone syndrome: Clinical and biochemical predictors of its occurrence after parathyroid surgery. Am. J. Med. 1988, 84, 654–660. [Google Scholar] [CrossRef] [PubMed]
- Erickson, L.A.; Mete, O.; Juhlin, C.C.; Perren, A.; Gill, A.J. Overview of the 2022 WHO Classification of Parathyroid Tumors. Endocr. Pathol. 2022, 33, 64–89. [Google Scholar] [CrossRef] [PubMed]
- Landeta, G.A.S.; Montes, A.T.; Jimenéz, T.I.G.; Guadalupe, V.O.; Baldomero, G.V.; Lourdes, B.H. Parathyroid Crisis as Presentation of Atypical Parathyroid Adenoma: Two Diagnostically Challenging Cases. J. Bone Metab. 2022, 29, 133–140. [Google Scholar] [CrossRef]
- Akin, R.D.; Pinheiro, A.D. Hypercalcemic Crisis Secondary to a Superior Mediastinal Parathyroid Adenoma: A Case Report. Ear Nose Throat J. 2022, 101, NP1–NP3. [Google Scholar] [CrossRef]
- Rutledge, S.; Harrison, M.; O’Connell, M.; O’Dwyer, T.; Byrne, M.M. Acute presentation of a giant intrathyroidal parathyroid adenoma: A case report. J. Med. Case Rep. 2016, 10, 286. [Google Scholar] [CrossRef]
- Raj, R.; Amine, A.; Herodotou, D. Postoperative Hypocalcemia Following Parathyroidectomy for Giant Parathyroid Adenoma. AACE Clin. Case Rep. 2020, 6, e352–e356. [Google Scholar] [CrossRef]
- Ohe, M.N.; Santos, R.O.; Hojaij, F.; Neves, M.C.; Kunii, I.S.; Orlandi, D.; Valle, L.; Martins, C.; Janovsky, C.; Ferreira, R.; et al. Parathyroid carcinoma and hungry bone syndrome. Arq. Bras. Endocrinol. Metabol. 2013, 57, 79–86. [Google Scholar] [CrossRef][Green Version]
- Kim, K.M.; Park, J.B.; Bae, K.S.; Kang, S.J. Hungry bone syndrome after parathyroidectomy of a minimally invasive parathyroid carcinoma. J. Korean Surg. Soc. 2011, 81, 344–349. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Buisset, C.; Demarquet, L.; Raynal, M.; Busby, H.; Nominé-Criqui, C.; Brunaud, L. When a Pathological Forearm Fracture Led to Explore the Neck: About a Case. Head Neck Pathol. 2020, 14, 828–832. [Google Scholar] [CrossRef]
- Yong, T.Y.; Li, J.Y. Mediastinal parathyroid carcinoma presenting with severe skeletal manifestations. J. Bone Miner. Metab. 2010, 28, 591–594. [Google Scholar] [CrossRef] [PubMed]
- Irie, T.; Mawatari, T.; Ikemura, S.; Matsui, G.; Iguchi, T.; Mitsuyasu, H. Brown tumor of the patella caused by primary hyperparathyroidism: A case report. Korean J. Radiol. 2015, 16, 613–616. [Google Scholar] [CrossRef]
- Ajmi, S.; Sfar, R.; Trimeche, S.; Ben Ali, K.; Nouira, M. Scintigraphic findings in hungry bone syndrome following parathyroidectomy. Rev. Esp. Med. Nucl. 2010, 29, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Parikh, P.; Shetty, S.; Rodrigues, G.; Bhat, S.N. Brown tumour mimicking skeletal metastasis. BMJ Case Rep. 2021, 14, e243478. [Google Scholar] [CrossRef] [PubMed]
- Witteveen, J.E.; van Thiel, S.; Romijn, J.A.; Hamdy, N.A. Hungry bone syndrome: Still a challenge in the post-operative management of primary hyperparathyroidism: A systematic review of the literature. Eur. J. Endocrinol. 2013, 168, R45–R53. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Yang, H.; Tan, H.; Song, R.; Zhang, Y.; Zhao, L. Brown tumor of the cervical spine with primary hyperparathyroidism: A case report and literature review. Medicine 2023, 102, e32768. [Google Scholar] [CrossRef]
- De La Flor Merino, J.C.; Justo, P.; Domínguez, J.J.; Gómez-Berrocal, A.; Seva, A.E.; Marschall, A.; Rodeles, M. Multiple brown tumors-Forgotten pathology in times of calcimimetics: A case report and literature review. SAGE Open Med. Case Rep. 2021, 9, 2050313X211039383. [Google Scholar] [CrossRef]
- Loh, H.H.; Lim, L.L.; Yee, A.; Loh, H.S.; Vethakkan, S.R. Effect of vitamin D replacement in primary hyperparathyroidism with concurrent vitamin D deficiency: A systematic review and meta-analysis. Minerva Endocrinol. 2019, 44, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Song, A.; Zhao, H.; Yang, Y.; Liu, S.; Nie, M.; Wang, O.; Xing, X. Safety and efficacy of common vitamin D supplementation in primary hyperparathyroidism and coexistent vitamin D deficiency and insufficiency: A systematic review and meta-analysis. J. Endocrinol. Investig. 2021, 44, 1667–1677. [Google Scholar] [CrossRef]
- Rolighed, L.; Rejnmark, L.; Sikjaer, T.; Heickendorff, L.; Vestergaard, P.; Mosekilde, L.; Christiansen, P. Vitamin D treatment in primary hyperparathyroidism: A randomized placebo controlled trial. J. Clin. Endocrinol. Metab. 2014, 99, 1072–1080. [Google Scholar] [CrossRef] [PubMed]
- Zelano, L.; Locantore, P.; Rota, C.A.; Policola, C.; Corsello, A.; Rossi, E.D.; Rufini, V.; Zagaria, L.; Raffaelli, M.; Pontecorvi, A. Parathyroid Carcinoma All-in-One, a Rare Life-Threatening Case with Multiple Systemic Manifestations: Case Report and Review of the Literature. Front. Endocrinol. 2022, 13, 881225. [Google Scholar] [CrossRef]
- Paepegaey, A.C.; Velayoudom, F.L.; Housni, S.; Gauthé, M.; Groussin, L. A Hungry Bone Syndrome Predicted by 18F-Fluorocholine PET/CT. Clin. Nucl. Med. 2019, 44, 903–904. [Google Scholar] [CrossRef] [PubMed]
- Tai, C.H.; Oh, H.B.; Seet, J.E.; Ngiam, K.Y. Pseudogout—A rare manifestation of hungry bone syndrome after focused parathyroidectomy. Ann. R. Coll. Surg. Engl. 2018, 100, e106–e108. [Google Scholar] [CrossRef]
- Zhou, W.; Chen, M. A case report of mediastinal ectopic parathyroid adenoma presented as parathyroid crisis localized by SPECT/CT. Medicine 2016, 95, e5157. [Google Scholar] [CrossRef]
- Sridhar, P.; Steenkamp, D.W.; Lee, S.L.; Ebright, M.I.; Litle, V.R.; Fernando, H.C. Mediastinal parathyroid adenoma with osteitis fibrosis cystica: Robot-assisted thoracic surgical resection. Innovations 2014, 9, 445–447. [Google Scholar] [CrossRef]
- Varma, R.; Kim, Y.J.; Garjian, K.; Barank, D. Hyperparathyroidism and hungry bone syndrome revisited. Clin. Nucl. Med. 2014, 39, 704–706. [Google Scholar] [CrossRef]
- Gratian, L.F.; Hyland, K.A.; Scheri, R.P. Hyperparathyroid crisis due to asymmetric parathyroid hyperplasia with a massive ectopic parathyroid gland. Endocr. Pract. 2014, 20, e180–e182. [Google Scholar] [CrossRef] [PubMed]
- Rastogi, A.; Bhadada, S.K.; Bhansali, A. Pseudoarthrosis and fracture: Interaction between severe vitamin D deficiency and primary hyperparathyroidism. Singap. Med. J. 2013, 54, e224–e227. [Google Scholar] [CrossRef] [PubMed]
- Wang, G.; Xiao, H.; Gu, Z.; Zhao, T. A case of primary hyperparathyroidism due to ectopic parathyroid adenoma in the thymus, accompanied with vitamin D deficiency. J. Clin. Endocrinol. Metab. 2013, 98, 2218–2222. [Google Scholar] [CrossRef][Green Version]
- Tachibana, S.; Sato, S.; Yokoi, T.; Nagaishi, R.; Akehi, Y.; Yanase, T.; Yamashita, H. Severe hypocalcemia complicated by postsurgical hypoparathyroidism and hungry bone syndrome in a patient with primary hyperparathyroidism, Graves’ disease, and acromegaly. Intern. Med. 2012, 51, 1869–1873. [Google Scholar] [CrossRef] [PubMed]
- Silaghi, H.; Valea, A.; Ghervan, C.; Silaghi, A.C. Ectopic intrathyroid parathyroid adenoma: Diagnostic and therapeutic challenges due to multiple osteolytic lesions. Case Rep. Med. Ultrason. 2011, 13, 241–244. [Google Scholar]
- Rathi, M.S.; Ajjan, R.; Orme, S.M. A case of parathyroid carcinoma with severe hungry bone syndrome and review of literature. Exp. Clin. Endocrinol. Diabetes 2008, 116, 487–490. [Google Scholar] [CrossRef]
- Meydan, N.; Barutca, S.; Guney, E.; Boylu, S.; Savk, O.; Culhaci, N.; Ayhan, M. Brown tumors mimicking bone metastases. J. Natl. Med. Assoc. 2006, 98, 950–953. [Google Scholar]
- Kuzucu, A.; Soysal, O.; Savli, H. Giant mediastinal parathyroid adenoma presenting with a hyperparathyroid crisis and leading to postoperative hungry bone syndrome. Eur. J. Surg. 2002, 168, 747–749. [Google Scholar] [CrossRef]
- Chandran, M.; Deftos, L.J.; Stuenkel, C.A.; Haghighi, P.; Orloff, L.A. Thymic parathyroid carcinoma and postoperative hungry bone syndrome. Endocr. Pract. 2003, 9, 152–156. [Google Scholar] [CrossRef]
- Chen, C.H.; Wang, P.W.; Liu, R.T.; Tung, S.C.; Jean, W.Y.; Lu, Y.C.; Kao, C.L.; Chen, L. Ectopic parathyroid adenoma with severe hungry bone syndrome: A case report. Changgeng Yi Xue Za Zhi 1996, 19, 196–202. [Google Scholar]
- Liou, M.J.; Lin, J.D.; Huang, M.J.; Huang, J.Y.; Hsueh, C.; Jeng, L.B. Parathyroid carcinoma with postoperative prolonged hypocalcemia in a patient with chronic renal failure. J. Formos Med. Assoc. 1996, 95, 337–341. [Google Scholar] [PubMed]
- Natsui, K.; Tanaka, K.; Suda, M.; Yasoda, A.; Shigeno, C.; Konishi, J.; Nakao, K. Oxyphil parathyroid adenoma associated with primary hyperparathyroidism and marked post-operative hungry bone syndrome. Intern. Med. 1996, 35, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Falko, J.M.; Bush, C.A.; Tzagournis, M.; Thomas, F.B. Case report. Congestive heart failure complicating the hungry bone syndrome. Am. J. Med. Sci. 1976, 271, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Williams-Karnesky, R.L.; Krumeich, L.; Wachtel, H.; Fraker, D.L.; Wirtalla, C.; Venuto, F.A.; Sellers, P.; Kelz, R.R. Data to inform counseling on parathyroidectomy for secondary hyperparathyroidism of renal origin. Surgery 2022, 171, 63–68. [Google Scholar] [CrossRef]
- Kritmetapak, K.; Kongpetch, S.; Chotmongkol, W.; Raruenrom, Y.; Sangkhamanon, S.; Pongchaiyakul, C. Incidence of and risk factors for post-parathyroidectomy hungry bone syndrome in patients with secondary hyperparathyroidism. Ren. Fail. 2020, 42, 1118–1126. [Google Scholar] [CrossRef]
- Yeşilkaya, E.; Cinaz, P.; Bideci, A.; Camurdan, O.; Demirel, F.; Demircan, S. Hungry bone syndrome after parathyroidectomy caused by an ectopic parathyroid adenoma. J. Bone Miner. Metab. 2009, 27, 101–104. [Google Scholar] [CrossRef]
- Tuli, G.; Munarin, J.; Tessaris, D.; Buganza, R.; Matarazzo, P.; De Sanctis, L. Primary Hyperparathyroidism (PHPT) in Children: Two Case Reports and Review of the Literature. Case Rep. Endocrinol. 2021, 2021, 5539349. [Google Scholar] [CrossRef]
- Lenherr-Taube, N.; Lam, C.K.; Vali, R.; Shammas, A.; Campisi, P.; Zawawi, F.; Somers, G.R.; Stimec, J.; Mete, O.; Wong, A.K.; et al. Severe Primary Hyperparathyroidism Caused by Parathyroid Carcinoma in a 13-Year-Old Child; Novel Findings from HRpQCT. JBMR Plus 2020, 4, e10324. [Google Scholar] [CrossRef]
- Hendarto, H.; Pramono, L.A.; Harbuwono, D.S.; Yunir, E.; Subekti, I. Parathyroid Adenoma in a Young Female Presenting Multiple Fractures and Postoperative Hungry Bone Syndrome. Acta Med. Indones 2017, 49, 69–73. [Google Scholar]
- Damiani, D.; Aguiar, C.H.; Bueno, V.S.; Montenegro, F.L.; Koch, V.H.; Cocozza, A.M.; Cordeiro, A.C.; Dichtchekenian, V.; Setian, N. Primary hyperparathyroidism in children: Patient report and review of the literature. J. Pediatr. Endocrinol. Metab. 1998, 11, 83–86. [Google Scholar] [CrossRef]
- Sharanappa, V.; Mishra, A.; Bhatia, V.; Mayilvagnan, S.; Chand, G.; Agarwal, G.; Agarwal, A.; Mishra, S.K. Pediatric Primary Hyperparathyroidism: Experience in a Tertiary Care Referral Center in a Developing Country over Three Decades. World J. Surg. 2021, 45, 488–495. [Google Scholar] [CrossRef] [PubMed]
- Hanba, C.; Bobian, M.; Svider, P.F.; Sheyn, A.; Siegel, B.; Lin, H.S.; Raza, S.N. Perioperative considerations and complications in pediatric parathyroidectomy. Int. J. Pediatr. Otorhinolaryngol. 2016, 91, 94–99. [Google Scholar] [CrossRef] [PubMed]
- George, J.; Acharya, S.V.; Bandgar, T.R.; Menon, P.S.; Shah, N.S. Primary hyperparathyroidism in children and adolescents. Indian J. Pediatr. 2010, 77, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Boro, H.; Khatiwada, S.; Alam, S.; Kubihal, S.; Dogra, V.; Malla, S.; Kumar, C. The spectrum of manifestations of primary hyperparathyroidism in children and adolescents. Pediatr. Endocrinol. Diabetes Metab. 2022, 28, 178–187. [Google Scholar] [CrossRef]
- Legault, O.; Inman, M.; Moolman, N.; Wiebe, S.; Poulin, A.; Nour, M.A. Severe hypercalcemia and a pelvic brown tumor in an adolescent with primary hyperparathyroidism: A case report. BMC Pediatr. 2020, 20, 547. [Google Scholar] [CrossRef]
- Juárez-León, Ó.A.; Gómez-Sámano, M.Á.; Cuevas-Ramos, D.; Almeda-Valdés, P.; López-Flores, A.; La Torre, M.A.; Reza-Albarrán, A.A.; Gómez-Pérez, F.J. Atypical Parathyroid Adenoma Complicated with Protracted Hungry Bone Syndrome after Surgery: A Case Report and Literature Review. Case Rep. Endocrinol. 2015, 2015, 757951. [Google Scholar] [CrossRef]
- Vitale, R.J.; Shieh, H.F.; Modi, B.P.; Gordon, R.J. Primary Hyperparathyroidism from Ectopic Parathyroid Adenoma in a 12-Year-Old with Slipped Capital Femoral Epiphysis. J. Endocr. Soc. 2022, 6, bvac071. [Google Scholar] [CrossRef]
- Saif, A. Primary hyperparathyroidism presenting with acute pancreatitis and asymptomatic bone involvement. Clin. Cases Miner. Bone Metab. 2015, 12, 199–201. [Google Scholar] [CrossRef]
- Ebina, K.; Miyoshi, Y.; Izumi, S.; Hashimoto, J.; Naka, N.; Tsukamoto, Y.; Kashii, M.; Kaito, T.; Yoshikawa, H. A case of adolescent giant parathyroid adenoma presenting multiple osteolytic fractures and postoperative hungry bone syndrome. Clin. Case Rep. 2015, 3, 835–840. [Google Scholar] [CrossRef]
- Çelik, A.; Divarcı, E.; Dökümcü, Z.; Ergün, O.; Özen, S.; Gökşen, D.; Darcan, Ş.; Ertan, Y. Intraoperative parathyroid hormone monitoring corroborates the success of parathyroidectomy in children. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 158–162. [Google Scholar] [CrossRef]
- Simsek, E.; Arikan, Y.; Dallar, Y.; Akkus, M.A. Prolonged hungry bone syndrome in a 10-year-old child with parathyroid adenoma. Indian Pediatr. 2009, 46, 178–180. [Google Scholar] [PubMed]
- Boechat, M.I.; Westra, S.J.; Van Dop, C.; Kaufman, F.; Gilsanz, V.; Roe, T.F. Decreased cortical and increased cancellous bone in two children with primary hyperparathyroidism. Metabolism 1996, 45, 76–81. [Google Scholar] [CrossRef] [PubMed]
- Kale, N.; Basaklar, A.C.; Sonmez, K.; Uluoglu, O.; Demirsoy, S. Hungry bone syndrome in a child following parathyroid surgery. J. Pediatr. Surg. 1992, 27, 1502–1503. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Xia, X.; Li, Z.; Cheng, F.; Zhu, X. Factors influencing the development of bone starvation syndrome after total parathyroidectomy in patients with renal hyperparathyroidism. Front. Surg. 2022, 9, 963231. [Google Scholar] [CrossRef]
- Ge, Y.; Yang, G.; Wang, N.; Zha, X.; Yu, X.; Mao, H.; Sun, B.; Zeng, M.; Zhang, B.; Xing, C. Bone metabolism markers and hungry bone syndrome after parathyroidectomy in dialysis patients with secondary hyperparathyroidism. Int. Urol. Nephrol. 2019, 51, 1443–1449. [Google Scholar] [CrossRef]
- Fülöp, T.; Koch, C.A.; Farah Musa, A.R.; Clark, C.M.; Gharaibeh, K.A.; Lengvársky, Z.; Hamrahian, M.; Pitman, K.T.; Dixit, M.P. Targeted surgical parathyroidectomy in end-stage renal disease patients and long-term metabolic control: A single-center experience in the current era. Hemodial. Int. 2018, 22, 394–404. [Google Scholar] [CrossRef]
- Latus, J.; Roesel, M.; Fritz, P.; Braun, N.; Ulmer, C.; Steurer, W.; Biegger, D.; Alscher, M.D.; Kimmel, M. Incidence of and risk factors for hungry bone syndrome in 84 patients with secondary hyperparathyroidism. Int. J. Nephrol. Renovasc. Dis. 2013, 6, 131–137. [Google Scholar] [CrossRef]
- Wang, M.; Chen, B.; Zou, X.; Wei, T.; Gong, R.; Zhu, J.; Li, Z. A Nomogram to Predict Hungry Bone Syndrome after Parathyroidectomy in Patients with Secondary Hyperparathyroidism. J. Surg. Res. 2020, 255, 33–41. [Google Scholar] [CrossRef]
- Yang, G.; Zha, X.; Mao, H.; Yu, X.; Wang, N.; Xing, C. Hypocalcemia-based prediction of hungry bone syndrome after parathyroidectomy in hemodialysis patients with refractory secondary hyperparathyroidism. J. Int. Med. Res. 2018, 46, 4985–4994. [Google Scholar] [CrossRef]
- Ho, L.Y.; Wong, P.N.; Sin, H.K.; Wong, Y.Y.; Lo, K.C.; Chan, S.F.; Lo, M.W.; Lo, K.Y.; Mak, S.K.; Wong, A.K. Risk factors and clinical course of hungry bone syndrome after total parathyroidectomy in dialysis patients with secondary hyperparathyroidism. BMC Nephrol. 2017, 18, 12. [Google Scholar] [CrossRef]
- Hamrahian, M.; Pitman, K.T.; Csongrádi, É.; Bain, J.H.; Kanyicska, B.; Fülöp, T. Symmetrical craniofacial hypertrophy in patients with tertiary hyperparathyroidism and high-dose cinacalcet exposure. Hemodial. Int. 2012, 16, 571–576. [Google Scholar] [CrossRef] [PubMed]
- Ko, W.C.; Liu, C.L.; Lee, J.J.; Liu, T.P.; Wu, C.J.; Cheng, S.P. Osteocalcin is an Independent Predictor for Hungry Bone Syndrome after Parathyroidectomy. World J. Surg. 2020, 44, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Schneider, R.; Steinmetz, C.; Karakas, E.; Bartsch, D.K.; Schlosser, K. Influence of Parathyroidectomy on Bone Metabolism and Bone Pain in Patients with Secondary Hyperparathyroidism. Eur. Surg. Res. 2018, 59, 35–47. [Google Scholar] [CrossRef]
- Lederer, E. Understanding renal phosphate handling: Unfinished business. Curr. Opin. Nephrol. Hypertens. 2023. ahead of print. [Google Scholar] [CrossRef]
- Portales-Castillo, I.; Rieg, T.; Khalid, S.B.; Nigwekar, S.U.; Neyra, J.A. Physiopathology of Phosphate Disorders. Adv. Kidney Dis. Health 2023, 30, 177–188. [Google Scholar] [CrossRef]
- Kravietz, A.M.; Buicko, J.L.; Parreco, J.P.; Lopez, M.A.; Kozol, R.A. Thirty-day readmissions following parathyroidectomy: Evidence from the National Readmissions Database, 2013–2014. Am. J. Otolaryngol. 2018, 39, 82–87. [Google Scholar] [CrossRef]
- Goldfarb, M.; Gondek, S.S.; Lim, S.M.; Farra, J.C.; Nose, V.; Lew, J.I. Postoperative hungry bone syndrome in patients with secondary hyperparathyroidism of renal origin. World J. Surg. 2012, 36, 1314–1319. [Google Scholar] [CrossRef]
- Neary, N.M.; El-Maouche, D.; Hopkins, R.; Libutti, S.K.; Moses, A.M.; Weinstein, L.S. Development and treatment of tertiary hyperparathyroidism in patients with pseudohypoparathyroidism type 1B. J. Clin. Endocrinol. Metab. 2012, 97, 3025–3030. [Google Scholar] [CrossRef] [PubMed]
- Itoh, M.; Okajima, M.; Kittaka, Y.; Yachie, A.; Wada, T.; Saikawa, Y. Tertiary hyperparathyroidism in patients with pseudohypoparathyroidism type 1a. Bone Rep. 2022, 16, 101569. [Google Scholar] [CrossRef]
- Collins, M.T.; Lindsay, J.R.; Jain, A.; Kelly, M.H.; Cutler, C.M.; Weinstein, L.S.; Liu, J.; Fedarko, N.S.; Winer, K.K. Fibroblast growth factor-23 is regulated by 1alpha,25-dihydroxyvitamin D. J. Bone Miner. Res. 2005, 20, 1944–1950. [Google Scholar] [CrossRef]
- Crowley, R.K.; Kilbane, M.; King, T.F.; Morrin, M.; O’Keane, M.; McKenna, M.J. Hungry bone syndrome and normalisation of renal phosphorus threshold after total parathyroidectomy for tertiary hyperparathyroidism in X-linked hypophosphataemia: A case report. J. Med. Case Rep. 2014, 8, 84. [Google Scholar] [CrossRef]
- Savio, R.M.; Gosnell, J.E.; Posen, S.; Reeve, T.S.; Delbridge, L.W. Parathyroidectomy for tertiary hyperparathyroidism associated with X-linked dominant hypophosphatemic rickets. Arch. Surg. 2004, 139, 218–222. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wang, L.; Zhang, X.; Hu, F.; Yuan, H.; Gao, Z.; He, L.; Zou, S. Impact of enhanced recovery after surgery program for hungry bone syndrome in patients on maintenance hemodialysis undergoing parathyroidectomy for secondary hyperparathyroidism. Ann. Surg. Treat. Res. 2022, 103, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.L.; de Brito Marques, F.; Freire, L.; Soares, V.; Guerreiro, L.; Silva, S.; Guedes, C. Intensive calcium monitoring improves outcomes on hungry bone syndrome in hyperparathyroidism. Endocr. Regul. 2021, 55, 30–41. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Fu, W.H.; Lim, E.L.A.; Ng, C.F.J.; Choong, H.L. Hungry bone syndrome after parathyroidectomy in end-stage renal disease patients: Review of an alkaline phosphatase-based treatment protocol. Int. Urol. Nephrol. 2020, 52, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Ge, Y.; Zha, X.; Mao, H.; Wang, N.; Xing, C. Peritoneal dialysis can alleviate the clinical course of hungry bone syndrome after parathyroidectomy in dialysis patients with secondary hyperparathyroidism. Int. Urol. Nephrol. 2019, 51, 535–542. [Google Scholar] [CrossRef]
- Ferreira, D.; Vilayur, E.; Gao, M.; Sankoorikal, C.; Bendinelli, C. Calcitriol loading before total parathyroidectomy with autotransplant in patients with end-stage kidney disease: Does it prevent postoperative hypocalcaemia? Intern. Med. J. 2019, 49, 886–893. [Google Scholar] [CrossRef] [PubMed]
- Hernandes, F.R.; Canziani, M.E.; Barreto, F.C.; Santos, R.O.; Moreira, V.M.; Rochitte, C.E.; Carvalho, A.B. The shift from high to low turnover bone disease after parathyroidectomy is associated with the progression of vascular calcification in hemodialysis patients: A 12-month follow-up study. PLoS ONE 2017, 12, e0174811. [Google Scholar] [CrossRef]
- Konturek, A.; Barczyński, M.; Stopa, M.; Nowak, W. Subtotal parathyroidectomy for secondary renal hyperparathyroidism: A 20-year surgical outcome study. Langenbecks Arch. Surg. 2016, 401, 965–974. [Google Scholar] [CrossRef]
- Florescu, M.C.; Islam, K.M.; Plumb, T.J.; Smith-Shull, S.; Nieman, J.; Mandalapu, P. Calcium supplementation after parathyroidectomy in dialysis and renal transplant patients. Int. J. Nephrol. Renovasc. Dis. 2014, 7, 183–190. [Google Scholar] [CrossRef]
- Jofré, R.; López Gómez, J.M.; Menárguez, J.; Polo, J.R.; Guinsburg, M.; Villaverde, T.; Pérez Flores, I.; Carretero, D.; Rodríguez Benitez, P.; Pérez García, R. Parathyroidectomy: Whom and when? Kidney Int. Suppl. 2003, 63, S97–S100. [Google Scholar] [CrossRef][Green Version]
- Zhong, A.; Billa, V.; Rotstein, L.E.; Wong, P.Y.; Bargman, J.M.; Vas, S.I.; Oreopoulos, D.G. Recurrence of hyperparathyroidism after total parathyroidectomy and autotransplantation in peritoneal dialysis patients. Perit. Dial. Int. 2000, 20, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Brotzer, L.; Nickler, M.; Kim, M.J.; Mueller, B.; Blum, C.A. Adrenal function testing in dialysis patients—A review of the literature. BMC Nephrol. 2021, 22, 360. [Google Scholar] [CrossRef]
- Narasaki, Y.; Sohn, P.; Rhee, C.M. The Interplay between Thyroid Dysfunction and Kidney Disease. Semin. Nephrol. 2021, 41, 133–143. [Google Scholar] [CrossRef]
- Garibotto, G.; Esposito, P.; Picciotto, D.; Verzola, D. Testosterone Disorders and Male Hypogonadism in Kidney Disease. Semin. Nephrol. 2021, 41, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Bransky, N.; Iyer, N.R.; Cannon, S.M.; Tyan, A.H.; Mylavarapu, P.; Orosco, R.; Hom, D.B.; Moazzam, A.A. Three Rare Concurrent Complications of Tertiary Hyperparathyroidism: Maxillary Brown Tumor, Uremic Leontiasis Ossea, and Hungry Bone Syndrome. J. Bone Metab. 2020, 27, 217–226. [Google Scholar] [CrossRef]
- Ahmed, C.; Kendi, F.; Gebran, N.; Barcebal, C.; Dahmani, K.; El Houni, A.; Budruddin, M. Use of Recombinant Human Parathyroid Hormone to Treat Hungry Bone Syndrome in Hemodialysis Patient. Oman Med. J. 2020, 35, e164. [Google Scholar] [CrossRef] [PubMed]
- Nogueira, E.L.; Costa, A.C.; Santana, A.; Guerra, J.O.; Silva, S.; Mil-Homens, C.; Costa, A.G. Teriparatide efficacy in the treatment of severe hypocalcemia after kidney transplantation in parathyroidectomized patients: A series of five case reports. Transplantation 2011, 92, 316–320. [Google Scholar] [CrossRef]
- Marcucci, G.; Masi, L.; Cianferotti, L.; Giusti, F.; Fossi, C.; Parri, S.; Gronchi, G.; Brandi, M.L. Chronic hypoparathyroidism and treatment with teriparatide. Endocrine 2021, 72, 249–259. [Google Scholar] [CrossRef]
- Cusano, N.E.; Rubin, M.R.; Bilezikian, J.P. Parathyroid hormone therapy for hypoparathyroidism. Best Pract. Res. Clin. Endocrinol. Metab. 2015, 29, 47–55. [Google Scholar] [CrossRef][Green Version]
- Bashir, S.O.; Aamer, M.A.; Omer, H.A.; Morsy, M.D. Penile calcific uremic arteriolopathy occurring postparathyroidectomy in a hemodialysis patient. Saudi J. Kidney Dis. Transpl. 2016, 27, 1265–1269. [Google Scholar] [CrossRef]
- Fritschi, B.C.; Trachsler, J.; Varga, Z.; Binet, I.; Fehr, T. Iatrogenic nephrocalcinosis with acute renal failure: An underestimated complication after parathyroidectomy? NDT Plus 2010, 3, 551–554. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lin, R.; Vucak-Dzumhur, M.; Elder, G.J. Changes to bone mineral density, the trabecular bone score and hip structural analysis following parathyroidectomy: A case report. BMC Nephrol. 2020, 21, 513. [Google Scholar] [CrossRef]
- Wu, Y.J.; Cheng, B.C.; Chiu, C.H.; Huang, S.C.; Li, L.C.; Chung, S.Y.; Den Chen, K.; Pan, C.C.; Li, J.Y.; Lin, H.W.; et al. Successful Modified Transoral Endoscopic Parathyroidectomy Vestibular Approach for Secondary Hyperparathyroidism with Ectopic Mediastinal Glands. Surg. Laparosc. Endosc. Percutan. Tech. 2019, 29, e88–e93. [Google Scholar] [CrossRef] [PubMed]
- Tai, T.S.; Hsu, Y.H.; Chang, J.M.; Chen, C.C. Recurrent tertiary hyperparathyroidism due to supernumerary parathyroid glands in a patient receiving long-term hemodialysis: A case report. BMC Endocr. Disord. 2019, 19, 16. [Google Scholar] [CrossRef] [PubMed]
- Tayyebi-Khosroshahi, H.; Farnood, F.; Ghorbanian, M.; Karkon-Shayan, F.; Naghavi-Behzad, M. Persistent hypocalcemia and hungry bone syndrome after parathyroidectomy and renal transplantation in a patient with end-stage renal disease. Niger. Med. J. 2017, 58, 50–52. [Google Scholar] [CrossRef]
- Altun, E.; Paydas, S.; Kaya, B.; Balal, M. Prolonged hypophosphatemia following parathyroidectomy in chronic hemodialysis patients. Saudi J. Kidney Dis. Transpl. 2015, 26, 976–979. [Google Scholar] [CrossRef] [PubMed]
- Park-Sigal, J.; Don, B.R.; Porzig, A.; Recker, R.; Griswold, V.; Sebastian, A.; Duh, Q.Y.; Portale, A.A.; Shoback, D.; Schambelan, M. Severe hypercalcemic hyperparathyroidism developing in a patient with hyperaldosteronism and renal resistance to parathyroid hormone. J. Bone Miner. Res. 2013, 28, 700–708. [Google Scholar] [CrossRef]
- Chu, H.Y.; Chu, P.; Lin, Y.F.; Chou, H.K.; Lin, S.H. Uremic tumoral calcinosis in patients on peritoneal dialysis: Clinical, radiologic, and laboratory features. Perit. Dial. Int. 2011, 31, 430–439. [Google Scholar] [CrossRef]
- Goto, S.; Fujii, H.; Matsui, Y.; Fukagawa, M. Marked increase in bone formation markers after cinacalcet treatment by mechanisms distinct from hungry bone syndrome in a haemodialysis patient. NDT Plus 2010, 3, 71–73. [Google Scholar] [CrossRef][Green Version]
- Ohlrich, H.; Barco, K.; Silver, M.R. The use of parenteral nutrition in a severely malnourished hemodialysis patient with hypercalcemia. Nutr. Clin. Pract. 2005, 20, 559–568. [Google Scholar] [CrossRef]
- Miles, A.M.; Markell, M.S.; Sumrani, N.; Hong, J.; Friedman, E.A. Severe hyperparathyroidism associated with prolonged hungry bone syndrome in a renal transplant recipient. J. Am. Soc. Nephrol. 1997, 8, 1626–1631. [Google Scholar] [CrossRef]
- Hardoff, R.; Frajewicki, V. Bone scintigraphy in hungry bone syndrome following parathyroidectomy. J. Nucl. Med. 1996, 37, 1371–1373. [Google Scholar] [PubMed]
- Frajewicki, V.; Kohan, R.; Abu-Ata, M.; Leiba, M.; Cohen, O.; Ben-Ari, J. Intraperitoneal phosphate administration in hungry bone syndrome. Clin. Nephrol. 1990, 34, 223–224. [Google Scholar] [PubMed]
- Benz, R.L.; Schleifer, C.R.; Teehan, B.P.; Sigler, M.H.; Gilgore, G.S. Successful treatment of postparathyroidectomy hypocalcemia using continuous ambulatory intraperitoneal calcium (CAIC) therapy. Perit. Dial. Int. 1989, 9, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Albright, F.; Baird, P.C.; Cope, O.; Bloomberg, E. Studies on the physiology of the parathyroid glands. IV. Renal complications of hyperparathyroidism. Am. J. Med. Sci. 1934, 187, 49–65. [Google Scholar] [CrossRef]
- Albright, F.; Aub, J.C.; Bauer, W. Hyperparathyroidism: A common and polymorphic condition as illustrated by seventeen proved cases from one clinic. JAMA 1934, 102, 1276–1287. [Google Scholar] [CrossRef]
- Albright, F.; Sulkowitch, H.W.; Bloomberg, E. Hyperparathyroidism due to idiopathic hypertrophy (hyperplasia?) of parathyroid tissue. Arch. Intern. Med. 1938, 62, 199–215. [Google Scholar] [CrossRef]
- Felsenfeld, A.J.; Levine, B.S.; Kleeman, C.R. Fuller Albright and our current understanding of calcium and phosphorus regulation and primary hyperparathyroidism. Nefrologia 2011, 31, 346–357. [Google Scholar] [CrossRef]
- Iacobone, M.; Scerrino, G.; Palazzo, F.F. Parathyroid surgery: An evidence-based volume-outcomes analysis: European Society of Endocrine Surgeons (ESES) positional statement. Langenbecks Arch. Surg. 2019, 404, 919–927. [Google Scholar] [CrossRef]
- Yao, L.; Guyatt, G.; Ye, Z.; Bilezikian, J.P.; Brandi, M.L.; Clarke, B.L.; Mannstadt, M.; Khan, A.A. Methodology for the Guidelines on Evaluation and Management of Hypoparathyroidism and Primary Hyperparathyroidism. J. Bone Miner. Res. 2022, 37, 2404–2410. [Google Scholar] [CrossRef]
- Silverberg, S.J. Vitamin D deficiency and primary hyperparathyroidism. J. Bone Miner. Res. 2007, 22 (Suppl. S2), V100–V104. [Google Scholar] [CrossRef] [PubMed]
- Dumitru, N.; Ghemigian, A.; Carsote, M.; Albu, S.E.; Terzea, D.; Valea, A. Thyroid nodules after initial evaluation by primary health care practitioners: An ultrasound pictorial essay. Arch. Balk Med. Union 2016, 51, 434–438. [Google Scholar]
- Perrier, N.; Lang, B.H.; Farias, L.C.B.; Poch, L.L.; Sywak, M.; Almquist, M.; Vriens, M.R.; Yeh, M.W.; Shariq, O.; Duh, Q.Y.; et al. Surgical Aspects of Primary Hyperparathyroidism. J. Bone Miner. Res. 2022, 37, 2373–2390. [Google Scholar] [CrossRef] [PubMed]
- Lui, M.S.; Shirali, A.S.; Huang, B.L.; Fisher, S.B.; Perrier, N.D. Advances in Endocrine Surgery. Surg. Oncol. Clin. N. Am. 2023, 32, 199–220. [Google Scholar] [CrossRef] [PubMed]
- Asmar, A.; Ross, E.A. Post-parathyroidectomy thyrotoxicosis and atrial flutter: A case for caution. NDT Plus 2011, 4, 117–119. [Google Scholar] [CrossRef]
- Guo, Z.; Zhao, L.; Xie, Y.; Yan, Y.; Mo, Z. Hungry Bone Syndrome Secondary to Subtotal Thyroidectomy in A Patient with Thyrotoxicosis. Am. J. Med. Sci. 2021, 362, 314–320. [Google Scholar] [CrossRef]
- Hagdorn, Q.A.J.; Loh, P.; Velthuis, S. Recurrent hypocalcaemic torsades de pointes due to hungry bone syndrome: A rare complication of thyroidectomy. Neth. Heart J. 2021, 29, 415–416. [Google Scholar] [CrossRef]
- Kusuki, K.; Mizuno, Y. Hungry bone syndrome after thyroidectomy for thyroid storm. BMJ Case Rep. 2019, 12, e231411. [Google Scholar] [CrossRef]
- Karunakaran, P.; Maharajan, C.; Ramalingam, S.; Rachmadugu, S.V. Is hungry bone syndrome a cause of postoperative hypocalcemia after total thyroidectomy in thyrotoxicosis? A prospective study with bone mineral density correlation. Surgery 2018, 163, 367–372. [Google Scholar] [CrossRef]
- Lazareva, O.; Panayiotopoulos, A.; Kazachkova, I.; Jacobson-Dickman, E. A teenage boy with hypocalcemia after radioablation for Graves’ disease. J. Pediatr. Endocrinol. Metab. 2014, 27, 379–382. [Google Scholar] [CrossRef]
- Edafe, O.; Balasubramanian, S.P. Incidence, prevalence and risk factors for post-surgical hypocalcaemia and hypoparathyroidism. Gland Surg. 2017, 6 (Suppl. S1), S59–S68. [Google Scholar] [CrossRef] [PubMed]
- Koubar, S.H.; Qannus, A.A.; Medawar, W.; Abu-Alfa, A.K. Hungry bone syndrome two weeks after starting cinacalcet: A call for caution. CEN Case Rep. 2018, 7, 21–23. [Google Scholar] [CrossRef] [PubMed]
- Yano, S.; Suzuki, K.; Sumi, M.; Tokumoto, A.; Shigeno, K.; Himeno, Y.; Sugimoto, T. Bone metabolism after cinacalcet administration in patients with secondary hyperparathyroidism. J. Bone Miner. Metab. 2010, 28, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, T.; Akizawa, T.; Uchida, E.; Tsukamoto, Y.; Iwasaki, M.; Koshikawa, S.; KRN1493 Study Group. Long-term cinacalcet HCl treatment improved bone metabolism in Japanese hemodialysis patients with secondary hyperparathyroidism. Am. J. Nephrol. 2009, 29, 230–236. [Google Scholar] [CrossRef]
- Lazar, E.S.; Stankus, N. Cinacalcet-induced hungry bone syndrome. Semin. Dial. 2007, 20, 83–85. [Google Scholar] [CrossRef]
- Nowack, R.; Wachtler, P. Hypophosphatemia and hungry bone syndrome in a dialysis patient with secondary hyperparathyroidism treated with cinacalcet--proposal for an improved monitoring. Clin. Lab. 2006, 52, 583–587. [Google Scholar]
- Nachankar, A.; Katyal, A.; Bansal, N.; Bishnoi, A. Hungry bone syndrome like presentation following single-dose denosumab for hypercalcaemia secondary to sarcoidosis with IgA nephropathy. BMJ Case Rep. 2022, 15, e250647. [Google Scholar] [CrossRef]
- Honda, M.; Shimata, K.; Sambommatsu, Y.; Ibuki, S.; Isono, K.; Yamamoto, H.; Sugawara, Y.; Sakamoto, S.; Inomata, Y.; Hibi, T. Hungry Bone Syndrome after Living Donor Liver Transplant for Biliary Atresia. Exp. Clin. Transplant. 2021, 19, 386–389. [Google Scholar] [CrossRef]
- Kumar, S.; Diamond, T. Lessons learnt from delayed diagnosis of FGF-23-producing tumour-induced osteomalacia and post-operative hungry bone syndrome. Bone Rep. 2020, 12, 100276. [Google Scholar] [CrossRef]
- Rendina, D.; De Filippo, G.; Tauchmanovà, L.; Insabato, L.; Muscariello, R.; Gianfrancesco, F.; Esposito, T.; Cioffi, M.; Colao, A.; Strazzullo, P.; et al. Bone turnover and the osteoprotegerin-RANKL pathway in tumor-induced osteomalacia: A longitudinal study of five cases. Calcif. Tissue Int. 2009, 85, 293–300. [Google Scholar] [CrossRef]
- Garla, V.V.; Salim, S.; Kovvuru, K.R.; Subauste, A. Hungry bone syndrome secondary to prostate cancer successfully treated with radium therapy. BMJ Case Rep. 2018, 2018, bcr2018225039. [Google Scholar] [CrossRef] [PubMed]
- Riveros, H.A.; Almodóvar, L.O.; Danés, C.F.; Domingo, J.P. Hungry bone syndrome: Persistent hypocalcemia related to osteoblastic bone metastases of prostate cancer. J. Palliat. Med. 2013, 16, 1496–1497. [Google Scholar] [CrossRef]
- Berruti, A.; Sperone, P.; Fasolis, G.; Torta, M.; Fontana, D.; Dogliotti, L.; Angeli, A. Pamidronate administration improves the secondary hyperparathyroidism due to “Bone Hunger Syndrome” in a patient with osteoblastic metastases from prostate cancer. Prostate 1997, 33, 252–255. [Google Scholar] [CrossRef]
- Sakai, K.; Tomoda, Y.; Saito, H.; Tanaka, K. Hungry bone syndrome and osteoblastic bone metastasis from gastric cancer. QJM 2020, 113, 903–904. [Google Scholar] [CrossRef] [PubMed]
- Eller-Vainicher, C.; Ossola, M.W.; Beck-Peccoz, P.; Chiodini, I. PTHrP-associated hypercalcemia of pregnancy resolved after delivery: A case report. Eur. J. Endocrinol. 2012, 166, 753–756. [Google Scholar] [CrossRef]
- Whitson, H.E.; Lobaugh, B.; Lyles, K.W. Severe hypocalcemia following bisphosphonate treatment in a patient with Paget’s disease of bone. Bone 2006, 39, 954–958. [Google Scholar] [CrossRef]




| First Author Year of Publication Reference Number | Study Design Studied Population | Post-Operatory Outcome (HBS) |
|---|---|---|
| Tang 2022 [34] | Retrospective study (between 2000 and 2018) N = 28 adults with atypical PT adenoma + PHPT mean age: 56 y 1/3 with renal dysfunction and stones 1/5 with bone loss | HBS prevalence: 7% |
| Chandran 2022 [35] | Retrospective study (between 2012 and 2019) N = 164 adults with PHPT | HBS prevalence: 2.4% Pre-operatory predictors of HBS: iPTH and AP |
| Nouikes Zitouni 2021 [36] | Retrospective study (between 2002 and 2013) N = 62 adults with PHPT mean age: 47 y | HBS prevalence: 19.3% |
| Salman 2021 [37] | Interventional study N = 102 p with PHPT N1 = 52 p without VD replacements N2 = 25 p with VD replacements + 25OHD > 20 ng/mL N3 = 25 p with VD replacements + 25OHD > 20 ng/mL | HBS prevalence: 8%, 16%, 23% (p = NS) Pre-operatory 25OHD is not an independent predictor of HBS. |
| Guillén Martínez 2020 [38] | Case-control, observational, analytical study (between 2007 and 2016) N = 82 p with PHPT | HBS prevalence: 12.2% HBS correlated with:
|
| Jakubauskas 2018 [39] |
Retrospective study (between 2005 and 2016) N = 94 p with PHPT | HBS prevalence: 28.7% HBS correlated with:
|
| Kaderli 2018 [40] |
Retrospective study N = 385 p with PHPT | HBS prevalence: 8.6% Pre-operatory predictor: PTH (not 25OHD) |
| Kaderli (bis) 2018 [41] |
Retrospective study N = 425 p with PHPT | PTH in post-operatory day 1: discriminative for transitory hypoPT, not for HBS PTH in post-operatory day 5–7: diagnostic of HBS |
| Mayilvaganan 2017 [42] |
Retrospective study (between 2013 and 2015) N = 19 p with PHPT N1 = 11 p with pre-PTx ZOL N2 = 8 p without pre-PTx ZOL | HBS prevalence: N1 = 0/11 N2 = 3/8 |
| Kaya 2016 [43] |
Retrospective study N = 62 p with PHPT | HBS prevalence: 13.4% HBS correlated with:
|
| Prasarttong-Osoth 2012 [6] |
Retrospective study (between 1997 and 2007) N = 45 p with PHPT | HBS prevalence: 22% |
| Malabu 2007 [44] |
Retrospective study (between 200 and 2006) N = 46 p with PHPT | HBS prevalence (+recurrent HPT): 4% |
| Lee 2006 [45] |
Retrospective study (between 1997 and 2002) N = 23 p with PHPT | HBS: 9/23 (BP exposure: 0/9) HBS-free: 14/23 (BP exposure: 6/14) |
| Brasier 1988 [46] |
Retrospective study N = 219 p with PHPT | HBS prevalence: 12.6% HBS correlated with:
|

{kind=link}
{kind=link}
{kind=link}
| First Author Year of Publication Reference Number | Presentation | Post-Operatory Outcome (HBS) |
|---|---|---|
| Shah 2023 [14] |
| Pre-operatory: 2 rounds of hemodialysis + calcitonin + ZOL |
| Zelano 2022 [65] |
| HBS (IV therapy for 4 days, oral therapy for 8 months) |
| Landeta 2022 [48] |
| HBS for 6 months after en bloc resection |
| Alvarez-Payares 2022 [7] |
| Post-operatory HBS since first 72 h (complicated with pulmonary embolism) |
| Parikh 2021 [58] |
| Total PTX followed by HBS |
| Raj 2020 [51] |
| HBS (IV therapy for 4 weeks) |
| Buisset 2019 [54] |
| HBS (+right thyroid lobectomy) |
| Florakis 2019 [10] |
| HBS: 2-day hospitalization 6-month post-PTx HBS |
| Paepegaey 2019 [66] |
| HBS (as indicated by PET/CT) |
| Tai 2018 [67] |
| HBS complicated with pseudogout flare |
| Schnyder 2017 [20] |
| HBS as clue for OFC, not bone metastasis |
| Rutledge 2016 [50] |
| HBS since post-operatory day 3 |
| Zhou 2016 [68] |
| HBS |
| Irie 2015 [56] |
| HBS (IV therapy for 30 days) Patellar pain resolution 1 month since PTx. |
| Sridhar 2014 [69] |
| HBS (the patient had severe obesity) |
| Varma 2014 [70] |
| HBS |
| Gratian 2014 [71] |
| HBS |
| Rastogi 2013 [72] |
| HBS |
| Ohe 2013 [52] |
| HBS |
| Wang G 2013 [73] |
| HBS |
| Tachibana 2012 [74] |
| PTx and thyroidectomy → HBS |
| Kim 2012 [53] |
| HBS |
| Silaghi 2011 [75] |
| HBS |
| Corsello 2010 [19] |
| HBS (ZOL before PTx) |
| Yong 2010 [55] |
| HBS |
| Sandoval 2010 [11] |
| HBS (IV therapy since day 7 to day 15) |
| Ajmi 2010 [57] |
| HBS |
| Rathi 2008 [76] |
| HBS |
| Meydan 2006 [77] |
| HBS |
| Morrone 2005 [15] |
| HBS (AP dynamics reflects calcium changes) |
| Kuzucu 2002 [78] |
| HBS |
| Chandran 2003 [79] |
| HBS |
| Chen 1996 [80] |
| HBS |
| Liou 1996 [81] |
| Post-PTx → early asymptomatic hypocalcemia → symptomatic HBS since month 8 (+↗PTH) |
| Natsui 1996 [82] |
| HBS |
| Falko 1976 [83] |
| HBS complicated with congestive heart failure |
| First Author Year of Publication Reference Number | Study Design Studied Population | Post-Operatory Outcome (HBS) |
|---|---|---|
| Sharanappa 2021 [91] | Retrospective study (between 1989 and 2019) N = 35 p with PHPT (<18 y) mean age: 15.2 y | HBS prevalence: 35% |
| Hanba 2016 [92] |
Retrospective pediatric study (between 2009 and 2012) N = 182 p with N’ = 262 PTx | Post-operatory prolonged hospital stat correlated with:
|
| George 2010 [93] |
Retrospective pediatric study (between 1993 and 2006) N = 15 p with PHPT | HBS prevalence: 33.3% |
| First Author Year of Publication Reference Number | Presentation | Post-Operatory Outcome (HBS) |
|---|---|---|
| Boro 2022 [94] |
| HBS prevalence: 40% (N = 4) |
| Vitale 2022 [97] |
| HBS (pediatric thoracoscopic resection) |
| Tuli 2021 [87] |
| HBS (non-cinalcet case) |
| Legault 2020 [95] |
| HBS (IV therapy of 6 days) |
| Lenherr-Taube 2020 [88] |
| HBS (IV therapy for 3 weeks) |
| Hendarto 2017 [89] |
| HBS |
| Juárez-León 2015 [96] |
| prolonged HBS (for 42 months: calcium supplements) |
| Saif 2015 [98] |
| HBS (IV therapy for 5 days) |
| Ebina 2015 [99] |
| HBS (IV therapy from day 4 to 28 after PTx) |
| Çelik 2014 [100] |
| 1/5 developed HBS |
| Yeşilkaya 2009 [86] |
| HBS |
| Simsek 2009 [101] |
| HBS (IV therapy for 4 weeks) |
| Damiani 1998 [90] |
| HBS |
| Boechat 1996 [102] |
| HBS |
| Kale 1992 [103] |
| HBS |
| First Author Year of Publication Reference Number | Study Design Studied Population | Post-Operatory Outcome (HBS) |
|---|---|---|
| Tai 2023 [4] | Single-center, retrospective study (between 2009–2019) N = 120 p with RHPT + PTx N1 = 100 p + ve HBS N2 = 20 p HBS free | Pre-operative predictor for HBS: serum ferritin (p = 0.038) Post-operative parameters: N1 < N2 (p < 0.001)
|
| Tanweer 2023 [30] | Single-surgeon experience (between 2016 and 2020) N = 53 p with PTx mean age: 75 y | 3.7% with post-operative HBS (among RHPT) |
| Wang L 2022 [123] | Single-center, retrospective study (between 2020 and 2021) N = 108 p with RHPT N1 = 52 p (no ERAS program) N2 = 56 p (ERAS program) | Pre-operatory predictor for HBS:
Post-operatory HBS correlated with:
|
| Peng 2022 [104] | Single-center, retrospective study (between 2015 and 2021) N = 141 p with RHPT + successful PTx N1 = 46 p with HBS (32%) N2 = 95 p HBS free | Pre-operatory predictor for HBS: N1 > N2 (p < 0.05)
|
| Williams-Karnesky 2022 [84] | Retrospective study N = 796 p with RHPT + PTx N1 = 164 p with HBS (20.6%) N2 = 632 p HBS free | Pre-operatory predictor for HBS:
|
| Ferreira 2021 [124] | Retrospective study N = 77 p with PHPT and RHPT | Active monitoring and electrolytes replacement consequences:
|
| Kritmetapak 2021 [85] | Retrospective study (between 2014 and 2020) N = 130 p with RHPT + PTx N1 = 85.4% with HBS | Pre-operatory predictor for HBS:
|
| Stefanova 2020 [1] | Retrospective study (between 2011 and 2016) N = 1846 p with RHPT + PTx | HBS and hypocalcemia caused 47% of post-PTX readmissions. |
| Wang M 2020 [108] | Prospective—retrospective study (between 2016 and 2018) N = 131 p with RHPT + PTx | HBS prevalence: 76.3% Pre-operatory independent predictors:
|
| Wong 2020 [125] | Retrospective study (between 2008 and 2013) N = 167 p with RHPT + PTx | Hypocalcemia (including HBS) rate: 10.9% Pre-operatory AP-based calcium supplementation for HBS |
| Ko 2020 [112] | Retrospective study (between 2010 and 2017) N = 260 p with RHPT + PTx | Pre-operatory predictors for HBS:
|
| Ge 2020 [105] | Retrospective study (between 2015 and 2017) N = 115 p with RHPT + PTx | HBS prevalence: 87.8% Pre-operatory predictors for HBS occurrence:
|
| Yang 2019 [126] | Retrospective study N1 = 169 p with RHPT + PTx + HD N2 = 29 p with RHPT + PTx + PD | HBS prevalence: N1 = 92.9% N2 = 75.86% (p = 0.004) |
| Ferreira 2019 [127] | Retrospective study N = 45 p with RHPT + PTx + 10-day calcitriol protocol before PTX | HBS prevalence: 28.3% Pre-operatory predictors for HBS:
|
| Yang 2018 [109] |
Retrospective study N = 252 p with RHPT + PTx + hemodialysis | HBS prevalence: 71.4% Pre-operatory predictors for HBS:
|
| Fülöp 2018 [106] |
Retrospective study (between 2005 and 2016) N = 37 p with RHPT + PTx | Younger age correlated with:
|
| Kravietz 2018 [116] |
National database study (between 2013 and 2014) N = 7171 p with PTx N1 = 58.89% with PHPT N2 = 21.99% with RHPT | 30-day readmission rate due to: N1: sepsis (13%), hypocalcemia (12%) N2: hypocalcemia (22%), HBS (14%) |
| Schneider 2018 [40] |
Prospective observational pilot study (between 2010 and 2012) N = 35 p with RHPT | HBS-associated bone pain correlated with:
|
| Hernandes 2017 [128] |
Follow-up study N = 19 p with RHPT | After 6-month HBS → at 12 months: low bone turnover associated with vascular calcifications progression |
| Ho 2017 [110] |
Retrospective study N = 62 p with RHPT | HBS prevalence: 27.4% Pre-operatory predictors for HBS:
|
| Konturek 2016 [129] |
Retrospective study (between 1995 and 2014) N = 297 p with RHPT | HBS prevalence: 31.3% (subtotal PTx) vs. 6.9% (incomplete PTx) |
| Florescu 2014 [130] |
Retrospective study N = 41 p with RHPT N1 = 73% under dialysis N2 = 27% renal transplant | Pre-operatory predictors for HBS:
|
| Latus 2013 [107] |
Retrospective study N = 84 p with RHPT | HBS prevalence: 51.2% Pre-operatory predictors for HBS:
|
| Goldfarb 2012 [117] |
Retrospective study N = 79 p with RHPT | HBS prevalence: 27.8%Pre-operatory predictor for HBS: young age |
| Davenport 2009 [17] |
Retrospective study N = 37 p with RHPT | Pre-operatory use of pamidronate 24–48 h before PTx (27/37) → HBS (2/27) |
| Jofré 2003 [131] |
Retrospective study N = 148 p with RHPT | HBS prevalence: 20% |
| Zhong 2000 [132] | Retrospective study (between 1994 and 1998) N = 19 p with RHPT | HBS prevalence: 15.78% |
| First Author Year of Publication Reference Number | Presentation | Post-Operatory Outcome (HBS) |
|---|---|---|
| Itoh 2022 [119] |
| Post-operatory HBS: high dose calcium + alphacalcidol |
| Hernandez 2021 [8] |
| Subtotal PTx → HBS (PTH ↘ to 205 pg/mL): high dose calcium + calcitriol |
| Lin 2020 [143] |
| HBS (IV therapy of 17 days) |
| Bransky 2020 [136] |
| TPT for severe hypocalcemia amid HBS |
| Ahmed 2020 [137] |
| TPT for persistent hypocalcemia amid HBS |
| Radu 2020 [31] |
| HBS with severe hypocalcemia (2.2–3.1 mg/dL) with cardiac arrest |
| Wu 2019 [144] |
| 1/10 p with HBS (11-day hospitalization) |
| Tai 2019 [145] |
| HBS after both interventions |
| Hassanein 2019 [25] |
| HBS initially aggravated calciphylaxis which completely remitted in 1 y |
| Anwar 2018 [26] |
| HBS requiring extremely high doses of calcium (maximum of 35.9 g. day) |
| Tayyebi-Khosroshahi 2017 [146] |
| HBS following renal transplant after both PTx |
| Bashir 2016 [141] |
| calciphylaxis after therapy for HBS |
| Altun 2015 [147] |
| Persistent HBS-related hypophosphatemia (8–10 months) |
| Crowley 2014 [121] |
| HBS → normalization of renal phosphorus threshold |
| Hamrahian 2013 [111] |
| HBS |
| Park-Sigal 2013 [148] |
| HBS |
| Chu 2011 [149] |
| HBS: 1 out of 3 patients |
| Goto 2010 [150] |
| HBS (cinacalcet before PTx) |
| Collins 2005 [120] |
| HBS: 1 out of 3 patients (pseudohypoparathyroidism type 1b) |
| Ohlrich 2005 [151] |
| HBS |
| Savio 2004 [122] |
| PTx: 3/6 and HBS |
| Miles 1997 [152] |
| Prolonged HBS (20 months) |
| Hardoff 1996 [153] |
| HBS |
| Frajewicki 1990 [154] |
| HBS with resistant hypophosphatemia → intraperitoneal phosphate therapy |
| Benz 1989 [155] |
| HBS with severe hypocalcemia (1 p with malabsorption) → intraperitoneal calcium therapy |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carsote, M.; Nistor, C. Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism. Diagnostics 2023, 13, 1953. https://doi.org/10.3390/diagnostics13111953
Carsote M, Nistor C. Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism. Diagnostics. 2023; 13(11):1953. https://doi.org/10.3390/diagnostics13111953
Chicago/Turabian StyleCarsote, Mara, and Claudiu Nistor. 2023. "Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism" Diagnostics 13, no. 11: 1953. https://doi.org/10.3390/diagnostics13111953
APA StyleCarsote, M., & Nistor, C. (2023). Forestalling Hungry Bone Syndrome after Parathyroidectomy in Patients with Primary and Renal Hyperparathyroidism. Diagnostics, 13(11), 1953. https://doi.org/10.3390/diagnostics13111953